Electronic Health Records, Electronic Prescribing and Medication Errors: A Systematic Review of Literature, 2000-2014
33
0
0
Full text
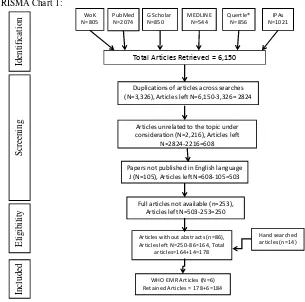
Figure

Related documents