\ /
>
\
Fetal
Ear Length
Jason
C. Birnholz,
MD,
and
Elaine
E. Farrell,
MD
From the Department of Diagnostic Radiology Rush-Presbyterian-St Luke’s Medical Center and Rush Medical College, Chicago, and the Department of Pediatrics, Division of Neonatology, Northwestern Medical Center and Evanston Hospital, Evanston, Illinois
ABSTRACT. A prenatal standard for ear length was
developed from ultrasonic images of 180 normal sub-jects. Length increased from about 6 mm at 15 weeks
to 33 mm at term and was well fit by linear regression (r2 = .96). Short ears (1.5 SD below gestational age
average) were associated strongly, and specifically,
with chromosomal disorders. Pediatrics 1988;81:555-558; ear length, chromosome, fetus.
Small ears are a feature ofthe Down syndrome’
and both small or long ears may occur with other aneuploid conditions.2 Postnatal standards for ear size (eg, length)3’4 are available from infant
stud-ies, but there do not appear to be comparable early
fetal data that can be applied to prenatal evalu-ation. We have previously reported ridge
pattern-ing with gestational age,5 which we now
supple-ment with observations of ear length.
MATERIALS
AND
METHODS
Maximal ear length from tip of helix to end of lobe was measured during ultrasonic examination of 180 second- and third-trimester fetuses. Only one determination was scored for patients having
multiple visits. Patients were entered
consecu-tively from our daily case load when gestational age (conceptual age plus 2 weeks) was known by a certain date of conception or by concordance of
menstrual dating and ultrasonic staging prior to
the 24th week; all cases with ultrasonically on
Received for publication April 18, 1986; accepted June 18, 1987.
Reprint requests to (J.C.B.) Department of Diagnostic Ra-diology, Rush-Presbyterian-St Luke’s Medical Center, 1753 W Congress Pkwy, Chicago, IL 60612.
PEDIATRICS (ISSN 0031 4005). Copyright © 1988 by the American Academy of Pediatrics.
postnatally detected structural abnormalities
(including the ear), macnosomia, or maternal alco-ho! or drug use were excluded, but there was
no
further distinction by fetal sex or position, or maternal age, cigarette smoking, on disease (ie, hypertension, diabetes, on collagen vasculardisease). The population was a socioeconomically
mixed, predominantly urban group with the fol-lowing approximate racial or ethnic composition: 55% white, 40% black, 3% Asian Indian, and 2%
Hispanic.
Ultrasonic images were obtained with a corn-mercial, large-aperture, dynamically focused array system operated at either 5.0 or 3.5 MHz (Acuson 128, Mountain View, CA).
Measure-ments were obtained parallel to the array,
ob-viating the need for any assumption about sound
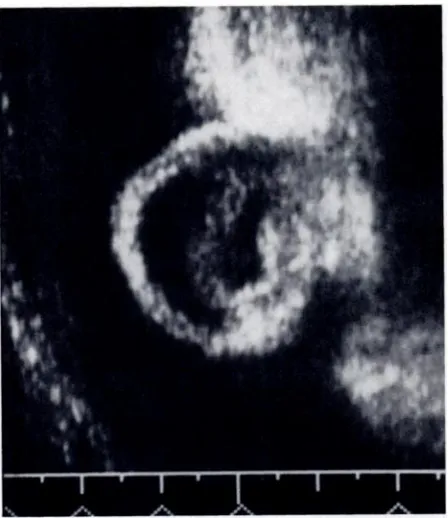
propagation velocity. The external ear was visu-alized along its length in coronal or frontal views
(Figs 1 and 2), respectively. A maximal length
section from edge of helix to tip of lobe was found
Fig 1. Lobe is prominent in this 34.9-mm long,
Fig 2. This 29-mm long ear has a rounded shape.
TABLE I. Four-Week Interval Samples
* Values are means ± SD.
556 FETAL EAR LENGTH
by continuous viewing with change in probe po-sition. Three separate length determinations were averaged per fetus.
OBSERVATIONS
Ear length and gestational age for the “normal” population sample are summarized in Table 1. In a linear fit of these data, ear length (mm) =
1.1011 x gestational age (wk) - 9.5089, r =
.962.
Eleven larger than gestational age fetuses with eventual birth weight greater than 3,800 g uni-fommly had prenatal ear length 1 SD greater than their age-adjusted norm. Most of these
fe-tuses were seen in the last month of pregnancy,
but one had ear length more than 2 SD greater than average when examined at 27 weeks. Eight
cases with growth retardation, attributed to
pla-No. of Fetuses Gestational Age (wk)* Ear Length (mm)*
12 14.808 ± 0.96043 5.775 ± 0.78009
40 18.075 ± 1.2405 9.9975 ± 1.5685 16 21.85 ± 1.2966 14.475 ± 2.151
18 26.15 ± 1.2868 19.811 ± 2.5117
33 30.015 ± 1.1035 25.273 ± 2.1915
32 33.944 ± 1.1937 27.781 ± 2.5734
29 37.866 ± 1.5352 30.99 ± 2.7894
cental vascular insufficiency, had ear length ap-propniate to the remainder of the population.
Findings in 35 cases with fetal abnormalities are shown in Table 2 and summarized in Table 3.
DISCUSSION
Ear length is an unambiguous, simple mea-surement that, in our experience, can be obtained in nearly all fetal ultrasonographic examinations.
We measure
the maximal
length,
combining
the
cartilaginous and lobe portions, because they have similar reflectivities. Theme is, however, a
di-morphic subdivision of the general population for
lobe types,68 and it is possible that failure to
dis-tinguish these parts contributes to the observed
variance, particularly in the third trimester when lobes become more obvious.
Ear length data were collected in a cross-sec-tional sample, but we believe they indicate a
rea-sonably linear pattern for length increment for
individual cases in the second and third tnimes-tens. A similar pattern is seen for other length growth features, such as the interosseous spacing
of the lumbar spine.9 The ultrasonic maximal ear length parallels but is less than the postnatal third-trimester physical length reported by Sivan et al.4 Further investigation will be necessary to determine whether this difference is related to ul-trasonic technique or to a primary genetic differ-ence between ethnically disparate study popula-tions. Physical ear length corresponded within 1 mm of the ultrasonic value in one patient with postmortem study shortly after fetal examination (Table 2, fetus 1).
Ear length distinguished cases with underlying chromosomal disorders with 100% specificity and 83% sensitivity (Table 3) in this study. Short ears were always found in our cases of trisomy 13 or
18 but only in about half of those with tnisomy
21. There is not sufficient information from these observations to identify when in the second trimester retarded ear length first becomes evi-dent, although we believe, for our prospective de-tection oftwo cases oftnisomy 21 at 16 weeks, that the sign may be applicable in
mid-second-trimes-ten studies.
We suggest that ear length be determined ul-trasonically whenever risk or suspicion of a chro-mosomal disorder is present or when a fetal anom-aly is detected. Short ears (ie, length 1 .5 SD less than the norm) can be taken as highly indicative
of an underlying systemic (eg, chromosomal) de-velopmental syndrome. Our findings suggest that normal ear length mitigates against that possibility.
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
TABLE 2. Findings in 35 Cases With Fetal Abnormalities
Fetus Major Prenatal U Itrasonic Findings Gestational Ear Difference
No. Age (wk) Length (mm) From Average (SD) Aneuploidy
1 Triploidy: multisystem 22.7 11.1 - 2.05
abnormalities
2 Trisomy 13, facial anomalies, 33.2 20.0 - 2.19
ambiguous genitalia
3 Tnisomy 13, umbilical hernia, 32.8 18.4 - 3.19
neural tube defects, ventricular septal defect
4 Tnisomy 13, umbilical hernia, 35.0 18.1 - 4.27
cleft lip
5 Trisomy 18, double outlet right 23.3 10.1 - 2.65
ventrical, cerebellar agenesis
6 Tnisomy 18, tetralogy of Fallot, 33.4 19.4 - 2.86
delayed gyration
7 Trisomy 18, cushion defect, hand 36.1 20.6 - 3.45
position
8 Tnisomy 21, hand and epiphyseal 21.2 11.2 - 1.21
findings
9 Tnisomy 21, delayed cerebellar 16.0 5.1 - 1.91
development
10 Trisomy 21, hydrocephalus 16.4 5.6 - 2.01
11 Trisomy 21, tetralogy of Fallot, 27.8 22.5 + 1.09
hydrocephalus
12 Tnisomy 21 19.4 11.4 -0.32
13 Tnisomy 21, ventriculomegaly 20.7 15.0 + 1.38
14 Turner syndrome, lymphedema 23.6 10.2 - 5.00
15 Translocation, lung hypoplasia 28.5 15.1 - 2.71
Normal chromosome complements
1 Chondroectodermal dysplasia 27.8 20.2 - 0.36
2 Thanatophoric dwarf 33.5 27.6 + 0.08
3 Thanatophoric dwarf 22.0 14.0 - 0.54
4 Short limb dwarf 25.5 19.7 + 0.88
5 Osteogenesis imperfecta (III) 22.4 14.2 - 0.46
6 Craniosynostosis 32.1 24.4 - 0.54
7 Microcephaly 33.0 28.7 + 0.81
8 Hydrocephalus 30.2 25.5 + 0.82
9 Lumbar neural tube defect 24.6 19.1 + 0.60
10 Sacral neural tube defect and 21.8 14.9 + 0.01
cerebellar agenesis
11 Cystic encephalocele, ambiguous 17.2 11.0 + 1.45
genitalia
12 Absent corpus callosum, 29.7 20.0 - 2.88
hydrocephalus
13 Fetal alcohol syndrome 34.0 30.0 + 1.10
14 Midgut volvulus 34.1 27.0 - 0.39
15 Duodenal atresia 32.5 26.0 -0.35
16 Duodenal atresia 27.3 25.0 + 2.17
17 Gastroschisis 21.6 15.0 + 0.54
18 Gastroschisis and imperforate 27.7 26.0 + 3.98
anus
19 Posterior urethral valves 28.1 24.0 + 2.02
20 Bilateral ureterovesical junction 31.6 29.8 + 4.08
obstruction
TABLE 3. Anomalies*
Ear Length Aneuploidy Euploidy
Normal or long 4 20
Short 11 0
* “Short” ears are defined as more than 1.5 SD less than
age-corrected mean. Results are numbers of ears.
REFERENCES
1. Aase JM, Wilson AC, Smith DW: Small ears in Down’s syndrome. J Pediatr 1973;82:845-884
2. Merlob P, Sivan Y, Reisner SH: Anthropometric mea-surements of the newborn infant. Birth Defects 1984;20:15-20
phys-558
FETAL EAR LENGTHical parameters: An aid to syndrome delineation. Birth Defects 1974;10:3-4
4. Sivan Y, Merlob P, Reisner SH: Assessment of ear length and low set in newborn infants. JMed Genet 1983;20:213-215
5. Birnholz JC: The fetal external ear. Radiology 1983;
147:819-821
6. Lai LYC. Walsh RI: Observations on ear lobe types. Acta
Genet 1966;16:250-257
7. Dutta P, Ganguly P: Further observations on ear lobe
at-tachment. Acta Genet 1965;15:77-82
8. Dronamraju KR: Ear lobe attachment in the Buffalo
re-gion. Acta Genet 1966;16:258-264
9. BirnholzJC: Fetallumbar spine. Radiology 1986;158:805-807
RUNNING
IN THE RAIN
If you are caught out in the rain, is it better to run for shelter, or would you still get just as wet as if you strolled casually for cover? Most of us don’t think in such a situation-we run. But there is a superficially appealing
argument, to do with the density of raindrops and the volume of air swept
out by a moving person, which suggests that instinct is wrong. Now, however,
Alessandro De Angelis, of the University of Udiine, Italy, has knocked that
argument on the head.
De Angelis
has gone
to the trouble
of calculating
the interaction
between
falling raindrops and a moving parallelepiped, representing a person. It turns out that for vertical rain someone moving at a brisk walk (three metres pen second) will get 10 per cent wetter than a world champion runner moving at 10 metres per second. The effort, says De Angelis, isn’t worth the bother (Eur J Phys, 8:201).
From New Scientist, Aug 27, 1987, p 27.
Submitted by Student
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
1988;81;555
Pediatrics
Jason C. Birnholz and Elaine E. Farrell
Fetal Ear Length
Services
Updated Information &
http://pediatrics.aappublications.org/content/81/4/555
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
1988;81;555
Pediatrics
Jason C. Birnholz and Elaine E. Farrell
Fetal Ear Length
http://pediatrics.aappublications.org/content/81/4/555
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 1988 by the
been published continuously since 1948. Pediatrics is owned, published, and trademarked by the
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news