Randomized, Controlled Trial of OROS Methylphenidate Once a Day in
Children With Attention-Deficit/Hyperactivity Disorder
Mark L. Wolraich, MD*; Laurence L. Greenhill, MD‡; William Pelham, PhD§; James Swanson, PhD
储
;
Timothy Wilens, MD¶; Donna Palumbo, PhD#; Marc Atkins, PhD**; Keith McBurnett, PhD‡‡;
Oscar Bukstein, MD§§; and Gerald August, PhD
储储
, on behalf of the Concerta Study Group
ABSTRACT. Objective. A new once-a-day methyl-phenidate (MPH) formulation, Concerta (methylpheni-date HCl) extended-release tablets (OROS MPH), has been developed. This study was conducted to determine the safety and efficacy of OROS MPH in a multicenter, randomized, clinical trial.
Methods. Children with attention-deficit/hyperactiv-ity disorder (ADHD;nⴝ282), all subtypes, ages 6 to 12 years, were randomized to placebo (nⴝ90), immediate-release methylphenidate (IR MPH) 3 times a day (tid; dosed every 4 hours;nⴝ97), or OROS MPH once a day (qd;nⴝ95) in a double-blind, 28-day trial. Outcomes in multiple domains were assessed, and data were analyzed using analysis of variance and Kaplan Meier product limit estimates for time to study cessation. The primary time point for analysis was the last available patient visit using last observation carried forward.
Results. Children in the OROS and IR MPH groups showed significantly greater reductions in core ADHD symptoms than did children on placebo. This was true both at the end of week 1 and at the end of treatment on the basis of mean teacher and parent IOWA Conners ratings. IR MPH tid and OROS MPH qd did not differ significantly on any direct comparisons. Forty-eight per-cent of the placebo group discontinued early compared with 14% and 16% in the IR MPH and OROS MPH groups, respectively.
Conclusions. For the treatment of core ADHD symp-toms, OROS MPH dosed qd and IR MPH dosed tid were superior to placebo and were not significantly different from each other. Pediatrics 2001;108:883– 892; attention-deficit/hyperactivity disorder, methylphenidate, OROS, Concerta.
ABBREVIATIONS. MPH, methylphenidate hydrochloride; ADHD, attention-deficit/hyperactivity disorder; IR, immediate release; SR, sustained release; tid, 3 times a day; qd, once a day; IRB, institutional review board; AE, adverse event; I/O, inattention/ overactivity; C-GAS, Children’s Global Assessment Scale; O/D, oppositional defiance; ODD, oppositional defiant disorder; LOCF, last observation carried forward.
M
ethylphenidate (MPH) was the most widely
dispensed stimulant medication used for
treating attention-deficit/hyperactivity
dis-order (ADHD) in 1999.
1ADHD is characterized by
developmentally inappropriate inattention,
hyperac-tivity, and impulsiveness and affects an estimated
3% to 5% of the school-age population.
2Because
MPH has a short half-life (2– 4 hours), the standard
immediate-release (IR) formulation typically must be
administered 2 or 3 times a day to maintain
thera-peutic efficacy.
3This often causes difficulties for
chil-dren who must be given a controlled substance
mid-day at school and for school officials who must
handle controlled medications. A sustained-release
(SR) MPH preparation, Ritalin-SR, is available;
how-ever, its duration of action is reported to be 8 hours.
4A study in children with ADHD revealed that a
slightly increasing plasma MPH concentration across
the day provided efficacy equivalent to IR MPH
dosed 3 times a day (tid).
5ALZA Corporation has
developed a once-a-day, osmotic, controlled-release,
oral dosage form of MPH, Concerta
(methylpheni-date HCl) extended-release tablets (OROS MPH),
that provides this slightly increasing plasma
concen-tration. OROS MPH was designed to maintain
effi-cacy through 12 hours with once-daily dosing (qd)
and to have a safety profile and efficacy comparable
to IR MPH given tid at 4-hour intervals.
6OROS MPH
eliminates the need for both in-school and
after-school dosing. The purpose of this study was to
determine the safety and efficacy of OROS MPH qd
compared with IR MPH tid and placebo in the
com-munity setting.
METHODS Patients
Boys and girls, ages 6 to 12 years, with a clinical diagnosis of any subtype of ADHD were recruited primarily through a cen-tralized recruitment service using radio and newspaper advertise-ments. Patients who were taking MPH or had taken it in the past had to have been on a total daily MPH dose (IR or IR/SR combi-nation) of at least 10 mg but not more than 60 mg. Patients were excluded from participation if they had an acute or serious chronic disease, were hypersensitive to methylphenidate, were having significant adverse experiences from methylphenidate, or were taking a medication that would interfere with the safe adminis-tration of methylphenidate. Patients with glaucoma, Tourette’s syndrome, an ongoing seizure disorder, or a psychotic disorder also were excluded, as were girls who had reached menarche.
More than 4000 parents of patients made initial contact in response to institutional review board (IRB)-approved postings and advertisements, and approximately 90% of these were ex-cluded from participation on the basis of a brief telephone screen.
From *Vanderbilt University, Nashville, Tennessee; ‡New York State Psy-chiatric Institute, New York; §State University of New York at Buffalo, Buffalo, New York;储University of California at Irvine, Irvine, California; ¶Massachusetts General Hospital, Boston, Massachusetts; #University of Rochester, Rochester, Minnesota; **University of Illinois at Chicago, Chi-cago, Illinois; ‡‡University of ChiChi-cago, ChiChi-cago, Illinois; §§Western Psychi-atric Institute and Clinic, University of Pittsburgh, Pittsburgh, Pennsylva-nia; and储储University of Minnesota, Rochester, Minnesota.
Received for publication Jun 5, 2000; accepted Mar 2, 2001.
Reprint requests to (M.L.W.) Child Study Center, 1100 NE 13th St, Okla-homa City, OK 73117. E-mail: [email protected]
Reasons for exclusion at this phase included unacceptable medical condition/medication, child’s age not within the range specified in the study inclusion criteria (6 –12 years), girls who had reached menarche, informational requests about ADHD without interest in study participation, and distance from the investigational site. Initially, acceptable respondents were invited to the clinics at each site for a day of screening procedures.
More than 500 patients were screened at 14 investigational sites; 405 of these enrolled into a screening study to confirm the diagnosis of ADHD. After the screening study, 210 of these pa-tients who previously had received MPH treatment within 4 weeks of entry into this study were enrolled directly into the current study, whereas 111 who had not received MPH before this study initially were enrolled into a dose-titration study. After the dose titration study, 102 patients entered the current study. One patient in the titration study did not receive treatment, and 4 terminated prematurely (1 for tics, 2 refused medication, and 1 because of possible drug diversion). An additional 4 patients did not enroll in the randomized study (because of timing of the study [n⫽3] or because the 54-mg dose was found to be ineffective [n⫽
1]). (Of the remaining patients enrolled in the screening study, 30 participated in a pharmacokinetic and pharmacodynamic study and later were enrolled into a separate long-term safety study, and 54 discontinued participation [52 patients did not meet the en-trance criteria, 1 was unable to swallow the medication, and 1 for unknown reasons].)
An effect size of 1.0 was considered in the sample size calcu-lation. Although a smaller number of patients would be required to demonstrate the treatment difference with such an anticipated effect size, the study was planned to enroll 300 patients to enhance the safety information available. A sample size of 300 would provide⬎99% power to detect a difference of 3 units between OROS MPH and placebo for the primary assessment (IOWA Con-ners Inattention/Overactivity [I/O] subscale; based on a Studentt
test with standard deviation of 3.0 and␣⫽0.05).
To be enrolled, the child’s ADHD diagnosis had to be con-firmed by the Diagnostic Interview Schedule for Children (Ver-sion 4)7administered by a trained interviewer. Severity of ADHD
symptoms was rated both at school by the community school teacher (teacher) and at home by the parent/caregiver (parent) using the SNAP-IV8and the IOWA Conners Rating Scale.9Parents
rated their child’s impairment using the Children’s Global Assess-ment Scale (C-GAS).10The study-site investigators reviewed all of
these assessments before making a final diagnosis on the basis of clinical judgment. Per the study protocol, patients had to agree to take the supplied study drug as the only medication for ADHD during the 4-week study period.
Each patient’s parent had to read, sign, and date an IRB-approved consent form that explained the nature, purpose, risks, and duration of the study. Each patient who was 7 years old or older and who could write his or her name read (or was read) and then signed an approved assent form or followed the IRB-approved standard practice for pediatric patients at each partici-pating study center.
Procedure
Patients were assigned to 1 of 3 treatment dose levels (18 mg OROS MPH qd/5 mg IR MPH tid, 36 mg OROS MPH qd/10 mg
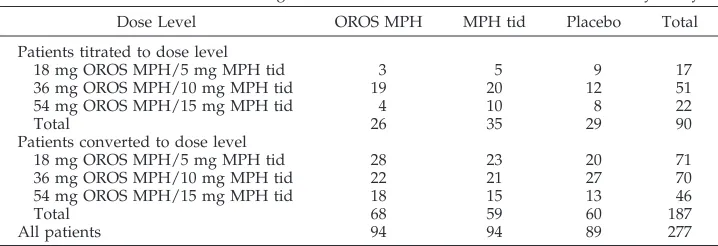
IR MPH tid, 54 mg OROS MPH qd/15 mg IR MPH tid), based either on titration (as described below) or conversion from previ-ous MPH treatment. Table 1 shows the numbers of patients as-signed to each dose level according to whether they underwent dose titration or dose conversion. Within each dose level, patients were randomized equally to OROS MPH qd, IR MPH (over-encapsulated Ritalin) tid, or placebo in a 3-group parallel design. A stratified randomization was conducted centrally at ALZA Cor-poration.
As described elsewhere in more detail,11patients who had not
received MPH for ADHD from their own practitioner in the 4 weeks before study entry first participated in an open-label, dose-ranging 1- to 4-week stepwise titration trial. Patients were titrated to an optimal dose based on investigator review of parent/teacher rating forms, presence of treatment-emergent adverse events (AEs), and clinical judgment. All patients were started on a dose of OROS MPH of 18 mg qd, and this was increased to 36 mg qd and then to 54 mg qd as necessary (ie, patients were titrated up to the higher doses only if deemed necessary by the investigators).
Patients who had taken MPH during the 4 weeks before study entry were assigned to a dose level based on their prestudy therapeutic dose and regimen. Their dose was determined by taking into account both their morning and total daily IR MPH doses. In general, IR MPH doses were converted to a total daily OROS MPH dose approximately equal to 3 times the usual morn-ing IR MPH dose.
Dosing was conducted in a double-blind and double-dummy manner. All patients received 3 OROS systems (active or placebo) and 1 IR capsule (active or placebo) at 0730 and an additional IR capsule (active or placebo) at 1130 and at 1530. Patients were dosed daily for 28 days.
During the course of the study, patients were allowed to receive behavioral interventions as long as the interventions had been initiated before the start of the study and did not change during the study. New behavioral therapy was not allowed during the course of the study.
Study Measures Behaviors
IOWA Conners Ratings Scale
The I/O subscale of the IOWA Conners Rating Scale9
com-pleted by the teacher on the Friday of week 4 (day 27) was defined as the primary efficacy measure before the study began. The IOWA Conners Rating Scale consists of 10 items divided into 2 subsets, I/O and Oppositional/Defiance (O/D). Items were scored on a 4-point scale (from 0⫽not at all to 3⫽very much), and the subsets were analyzed separately. Teachers and parents completed both subsets of the IOWA Conners scale on each Friday during the study to evaluate inattention and behavior in school and at home. Effect size also was determined for the primary efficacy parameter. The IOWA Conners scale has been used in treatment studies and has shown adequate discriminant validi-ty.12
SNAP-IV
The SNAP-IV8included 18 items that reflect ADHD symptoms
in the Diagnostic and Statistical Manual of Mental Disorders, 4th
TABLE 1. Number of Patients Assigned to Each Dose Level and Included in the Efficacy Analysis Dose Level OROS MPH MPH tid Placebo Total
Patients titrated to dose level
18 mg OROS MPH/5 mg MPH tid 3 5 9 17
36 mg OROS MPH/10 mg MPH tid 19 20 12 51
54 mg OROS MPH/15 mg MPH tid 4 10 8 22
Total 26 35 29 90
Patients converted to dose level
18 mg OROS MPH/5 mg MPH tid 28 23 20 71
36 mg OROS MPH/10 mg MPH tid 22 21 27 70
54 mg OROS MPH/15 mg MPH tid 18 15 13 46
Total 68 59 60 187
All patients 94 94 89 277
Edition(inattention and hyperactivity/impulsivity), and 8 items that reflect oppositional defiant disorder (ODD) symptoms. At the end of the study, teachers and parents completed the 26 SNAP-IV items, which were scored using the same 4-point scale as the IOWA Conners. The SNAP-IV has been used in large, multisite pediatric psychopharmacology clinical trials, showing medication effects for children who are treated with MPH.13
Function
The parent-scored C-GAS generates a global rating of the child’s impairment. The C-GAS has been found to demonstrate concurrent and discriminant validity.10
Change/Efficacy
Clinical Global Impressions-Improvement
At the end of the study, study-site investigators responded to the following question using a 7-point Likert scale (from 0⫽very much worse to 6⫽very much improved): Rate total improvement whether or not, in your judgment, it is due entirely to treatment. Compared with his/her condition the week before the start of the 4-week treatment, how much has he/she changed?14,15The rating
was based on a review of teacher and parent ratings and a parent interview. The Clinical Global Impressions-Improvement has been shown to be sensitive to medication effects in a trial with children and adolescents.16
Global Assessment of Efficacy
Parents and teachers completed a global assessment of efficacy at the end of the study rating the patient’s behavior and attention on a 4-point scale (0⫽poor; 1⫽fair; 2⫽good; 3⫽excellent) in response to the following question: What is your opinion of the effectiveness of treatment this week?
Peer Interaction
On day 27, teachers rated 6 items from the SNAP-IV Peer Interaction category using the same 4-point scale as the SNAP inattention and hyperactivity/impulsivity and ODD items. These 6 items from the SNAP and 1 item from the IOWA Conners Rating Scale were analyzed to give the Peer Interaction score.
Parent Satisfaction Questionnaire
A Parent Satisfaction Questionnaire was completed at the end of treatment, based on a questionnaire used in the National Insti-tute of Mental Health Multimodal Treatment Study of Children with ADHD (MTA).13At the end of the study, parents were asked
to rate their satisfaction with the study medication and its benefit to the patient symptom relief compared with previous medica-tions and whether they would recommend the treatment to other patients.
Safety Assessment
AEs were collected on days 7, 14, and 28 by asking parents whether any new development in the child’s health had occurred since the last clinic visit. Spontaneously reported AEs also were recorded. Reported events were assessed to determine whether any events were serious, life-threatening, or unexpected and to assign severity and relationship to study medication. In addition, parents rated the child’s sleep quality for the preceding 2 weeks on days 0, 14, and 28. Sleep quality was rated as excellent, good, fair, or poor. Parents also rated the child’s appetite for the previous 2 weeks on days 14 and 28. Food intake was rated as more than before, about the same amount as before, or less than before, relative to the child’s usual food intake before participating in any ALZA study. Parents were questioned at screening about the history or presence of motor and/or verbal tics and on days 0, 14, and 28 about the presence of tics and any changes in their severity or specificity. When a new occurrence or a clinically significant increase in tics was observed, it was recorded as an AE. Vital signs (blood pressure and pulse rate) were recorded at screening and on days 0, 14, and 28.
Statistical Analysis
The study protocol defined the time for conducting the primary analyses as the end of week 4 (day 27). The disparate dropout rates in the placebo and active treatment groups necessitated an amend-ment to this time point. The primary time point for analyses became the end of study, defined as the end of week 4 for patients
who completed the trial or the last available measurement for patients who dropped out early (ie, the last available patient visit, using a last observation carried forward [LOCF] approach). An analysis with all available data (without LOCF) also was con-ducted, and the results were consistent with those of the LOCF analysis.
Primary analyses were conducted using analysis of variance techniques. As a further measure of efficacy, treatment groups were compared in time with dropout using Kaplan Meier product limit estimates. Effect sizes were calculated by dividing the differ-ence of the mean scores (active vs placebo) by the standard devi-ation of the placebo group.
RESULTS Patients
Figure 1 presents the patient disposition. A total of
312 patients were enrolled at 14 centers in the United
States. A site audit at 1 site (30 patients) uncovered
irregularities that made it impossible to verify the
results reported, so before the study data were
ana-lyzed, a decision was made to exclude the efficacy
data from this site. This included 11 patients in the
dose-titration group and 19 patients who previously
had received MPH treatment. However, the data also
were analyzed with this site included, and the nature
of the results and conclusions did not change. Of the
282 patients who were enrolled at the remaining
sites, 5 were not treated (3 withdrew consent, 1 of
whom was in the dose-titration group, 1 did not
return, and 1 did not have the diagnosis confirmed).
Therefore, 277 patients were included in the efficacy
analyses (90 patients from the dose-titration group
and 187 patients who previously had received MPH
therapy; see Table 1). Within each dose level, patients
were distributed equally among the 3 treatments.
The number of patients enrolled at each of the 13
remaining sites ranged from 10 to 28.
Seventy-one patients discontinued treatment
pre-maturely (OROS MPH,
n
⫽
15; IR MPH,
n
⫽
13;
placebo,
n
⫽
43). Table 2 shows the cumulative
num-ber of dropouts by week. Fifty-nine patients
discon-tinued for lack of efficacy, 38 from the placebo group,
11 from the OROS MPH group, and 10 from the IR
MPH group. Three patients discontinued because of
noncompliance, 2 for AEs/intercurrent illnesses, and
2 because of protocol violations. In addition, 1
pa-tient discontinued for each of the following reasons:
AE requiring dose reduction, lost to follow-up, did
not return, could not swallow the pills, and took
supplemental MPH.
Dose of Drug
The average total daily dose for patients from the
13 sites was 29.5 mg per day (0.9
⫾
0.4 mg/kg/d) for
IR MPH and 34.3 mg per day (1.1
⫾
0.5 mg/kg/d)
for OROS MPH. These doses need to be considered
in the context of the approximate 90% bioavailability
of OROS MPH relative to IR MPH reported by Modi
et al.
17Patients remained on the predetermined
OROS MPH and IR MPH doses throughout the
study.
Demographic and Baseline Characteristics
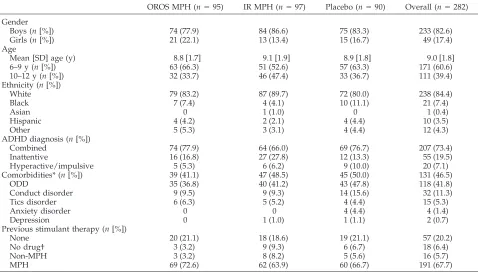
were white. More than two thirds (67.7%) of the
patients previously had received MPH treatment for
ADHD before entering the study, and 73.4% of their
diagnoses were the combined subtype of ADHD.
Comorbidities also were present in 46.5%; ODD
(41.8%) was the major comorbidity in all 3 treatment
groups. No statistically significant differences were
seen among treatment groups for these demographic
and baseline characteristics, except for the
comorbid-ity general anxiety disorder, present in 4 patients in
the placebo group but in no patients in the other
treatment groups.
Fig 1. Patient disposition.
TABLE 2. Number of Patients Enrolled and Treated and Cumulative Number of Dropouts by Week
Treatment Number of Patients Cumulative Dropout Rate (n[%])* Overall Site
Excluded
Treated Week 1 Week 2 Week 3 Week 4
OROS MPH qd 106 95 94
Dropouts 3 (3.2) 6 (6.4) 11 (11.7) 15 (16.0)
Remaining 91 (96.8) 88 (93.6) 83 (88.3) 79 (84.0)
IR MPH 107 97 94
Dropouts 6 (6.4) 12 (12.8) 13 (13.8) 13 (13.8)
Remaining 88 (93.6) 82 (87.2) 81 (86.2) 81 (86.2)
Placebo 99 90 89
Dropouts 20 (22.5) 37 (41.6) 42 (47.2) 43 (48.3)
Remaining 69 (77.5) 52 (58.4) 47 (52.8) 46 (51.7)
Total 312 282 277
Dropouts 29 (10.5) 55 (19.9) 66 (23.8) 71 (25.6)
Remaining 248 (89.5) 222 (80.1) 211 (76.2) 206 (74.4)
Average categorical ratings for the hyperactive/
impulsive and inattentive components of the
Diag-nostic Interview Schedule for Children and mean
scores for C-GAS at baseline were similar for patients
in the 3 treatment groups. Baseline values for the
IOWA Conners, Peer Interaction, and the SNAP-IV
are shown in Tables 4 and 5.
Outcome Measures and Efficacy
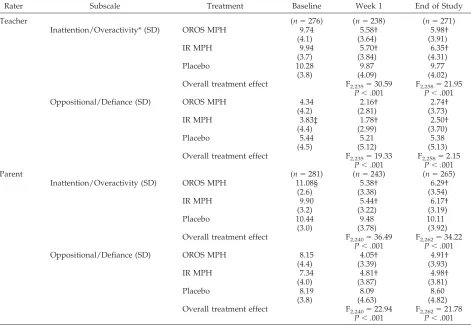
Table 4 shows the baseline, week 1, and
end-of-study results for the teacher and parent IOWA
Con-ners I/O and O/D subscales. The teacher IOWA
Conners I/O scores at the end of week 1 showed
statistically significant (
P
⬍
.001) improvement with
both OROS MPH qd (mean: 5.58
⫾
3.64) and IR MPH
tid (mean: 5.70
⫾
3.84) over placebo (mean: 9.87
⫾
4.09). The effect sizes versus placebo were 1.05 for
OROS MPH and 1.02 for IR MPH. Results of the
primary efficacy measure, the teacher IOWA
Con-ners I/O subscale completed at end of study, also
showed that both OROS MPH qd (mean: 5.98
⫾
3.91)
and IR MPH tid (mean: 6.35
⫾
4.31) were
signifi-cantly better (
P
⬍
.001) than placebo (mean: 9.77
⫾
4.02; Fig 2). No significant difference was seen
be-tween the mean IOWA Conners scores for the OROS
MPH qd and IR MPH tid treatment groups at week
1 (
P
⫽
.838) or at the end of the study (
P
⫽
.539).
Teacher and parent IOWA Conners O/D ratings,
evaluating patients’ oppositional defiance, also
sup-ported the findings of superior efficacy for the 2
active treatments. Analysis revealed no significant
treatment by site interactions for the primary end
point at the final assessment.
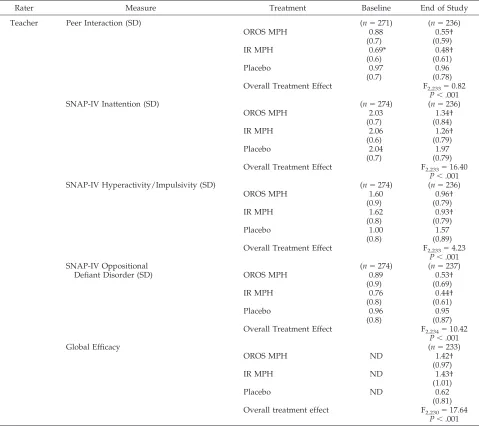
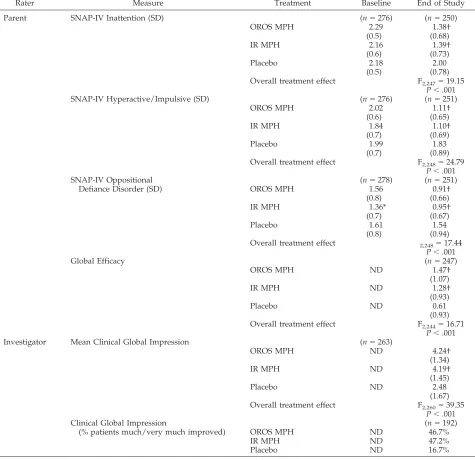
Table 5 shows the baseline and end-of-study
re-sults for the secondary efficacy endpoints. Teacher
and parent SNAP-IV scores evaluating inattention,
hyperactivity/impulsivity, and ODD behaviors were
significantly better (
P
⬍
.001) for patients who were
on the 2 active treatments than for patients who were
on placebo. No significant difference in scores was
seen between the OROS MPH and IR MPH groups
for these measures.
For the global assessment of efficacy, teachers and
parents rated the 2 active treatments significantly
better than placebo (
P
⬍
.001). Teachers rated
treat-ment efficacy as good or excellent for 42.9% of
tients who were taking OROS MPH, 46.9% of
pa-tients who were taking IR MPH, and 17.7% of
patients who were taking placebo. Parent global
as-sessment scores were similar (OROS MPH, 54.0%; IR
MPH, 46.5%; placebo, 20.3%).
Results of the clinical global impression,
com-pleted by the investigator at each site, also showed
significant benefits (
P
⬍
.001) for both active
treat-ments compared with placebo. Ratings of very much
improved or much improved were obtained by
46.7% of patients who were taking OROS MPH qd,
47.2% of patients who were taking IR MPH tid, and
16.7% of patients who were taking placebo.
Logistic regression analysis of responses to the
Parent Satisfaction Questionnaire completed at the
end of treatment showed that parents were
signifi-cantly more satisfied with the active treatments than
with placebo (
P
⬍
.001). In particular, when asked
how pleased they were with the medication for their
child’s ADHD symptoms, 62.6% and 64.0% of
par-TABLE 3. Demographic and Baseline Characteristics
OROS MPH (n⫽95) IR MPH (n⫽97) Placebo (n⫽90) Overall (n⫽282) Gender
Boys (n[%]) 74 (77.9) 84 (86.6) 75 (83.3) 233 (82.6)
Girls (n[%]) 21 (22.1) 13 (13.4) 15 (16.7) 49 (17.4)
Age
Mean [SD] age (y) 8.8 [1.7] 9.1 [1.9] 8.9 [1.8] 9.0 [1.8]
6–9 y (n[%]) 63 (66.3) 51 (52.6) 57 (63.3) 171 (60.6)
10–12 y (n[%]) 32 (33.7) 46 (47.4) 33 (36.7) 111 (39.4) Ethnicity (n[%])
White 79 (83.2) 87 (89.7) 72 (80.0) 238 (84.4)
Black 7 (7.4) 4 (4.1) 10 (11.1) 21 (7.4)
Asian 0 1 (1.0) 0 1 (0.4)
Hispanic 4 (4.2) 2 (2.1) 4 (4.4) 10 (3.5)
Other 5 (5.3) 3 (3.1) 4 (4.4) 12 (4.3)
ADHD diagnosis (n[%])
Combined 74 (77.9) 64 (66.0) 69 (76.7) 207 (73.4)
Inattentive 16 (16.8) 27 (27.8) 12 (13.3) 55 (19.5)
Hyperactive/impulsive 5 (5.3) 6 (6.2) 9 (10.0) 20 (7.1)
Comorbidities* (n[%]) 39 (41.1) 47 (48.5) 45 (50.0) 131 (46.5)
ODD 35 (36.8) 40 (41.2) 43 (47.8) 118 (41.8)
Conduct disorder 9 (9.5) 9 (9.3) 14 (15.6) 32 (11.3)
Tics disorder 6 (6.3) 5 (5.2) 4 (4.4) 15 (5.3)
Anxiety disorder 0 0 4 (4.4) 4 (1.4)
Depression 0 1 (1.0) 1 (1.1) 2 (0.7)
Previous stimulant therapy (n[%])
None 20 (21.1) 18 (18.6) 19 (21.1) 57 (20.2)
No drug† 3 (3.2) 9 (9.3) 6 (6.7) 18 (6.4)
Non-MPH 3 (3.2) 8 (8.2) 5 (5.6) 16 (5.7)
MPH 69 (72.6) 62 (63.9) 60 (66.7) 191 (67.7)
SD indicates standard deviation.
ents responded pleased, very pleased, or extremely
pleased for the OROS MPH and IR MPH treatments,
respectively, compared with 21.0% for placebo. No
significant differences were observed in this measure
for the OROS MPH and IR MPH treatments.
AEs
From all sites, patients who received at least 1 dose
of study medication (
n
⫽
306) were included in the
analysis of safety. No serious AEs were reported
during the study. Fewer than half of the 306 patients
(126 [41.2%]) reported any AEs, and the majority of
the events reported were mild. A similar percentage
of patients reported at least 1 AE on OROS MPH qd
(42.3%) and on IR MPH tid (46.2%). Fewer patients
(34.7%) reported at least 1 AE on placebo. One
pa-tient from each treatment group discontinued the
study early because of the following AEs: depression
on OROS MPH, considered by the investigator
pos-sibly to be related to treatment; emotional lability on
IR MPH tid, considered probably to be related to
treatment; and twitching (tics) on placebo, also
con-sidered by the investigator probably to be related to
treatment. (Relationship to treatment was assigned
before the blind was broken.)
The most commonly reported AEs were headache
and upper respiratory tract infection, followed by
abdominal pain, cough, pharyngitis, vomiting, and
otitis media. Of these, only headache and abdominal
pain, both known to occur with MPH, were
consid-ered to be related to study medication in the majority
of patients who reported these AEs. For patients on
OROS MPH, IR MPH, and placebo, headache
oc-curred in 14.4%, 5.8%, and 10.2% of patients and
abdominal pain occurred in 6.7%, 5.8%, and 1.0%,
respectively. Other AEs known to occur with MPH
and considered related to study drug included
ap-petite suppression (OROS treatment) and insomnia
(OROS, IR, and placebo treatments). No clinically
significant changes in vital signs occurred in any of
the treatment groups.
Sleep
At day 0, most patients were assessed as having
good or excellent sleep quality: 70.5%, 72.8%, and
76.6% of patients in the OROS MPH, IR MPH, and
placebo groups, respectively. As rated on days 14
and 28, the majority of patients (
ⱖ
65%) in each
treat-ment group continued to have good or excellent
sleep quality. No statistically significant differences
were observed in the way the individual sleep
qual-ity categories (excellent, good, fair, or poor)
distrib-uted among the 3 treatment groups.
TABLE 4. IOWA Conners Mean Scores at Baseline, Week 1, and End of Study
Rater Subscale Treatment Baseline Week 1 End of Study
Teacher (n⫽276) (n⫽238) (n⫽271)
Inattention/Overactivity* (SD) OROS MPH 9.74 5.58† 5.98† (4.1) (3.64) (3.91)
IR MPH 9.94 5.70† 6.35†
(3.7) (3.84) (4.31)
Placebo 10.28 9.87 9.77
(3.8) (4.09) (4.02) Overall treatment effect F2,235⫽30.59 F2,258⫽21.95
P⬍.001 P⬍.001 Oppositional/Defiance (SD) OROS MPH 4.34 2.16† 2.74†
(4.2) (2.81) (3.73)
IR MPH 3.83‡ 1.78† 2.50†
(4.4) (2.99) (3.70)
Placebo 5.44 5.21 5.38
(4.5) (5.12) (5.13) Overall treatment effect F2,235⫽19.33 F2,258⫽2.15
P⬍.001 P⬍.001
Parent (n⫽281) (n⫽243) (n⫽265)
Inattention/Overactivity (SD) OROS MPH 11.08§ 5.38† 6.29† (2.6) (3.38) (3.54)
IR MPH 9.90 5.44† 6.17†
(3.2) (3.22) (3.19)
Placebo 10.44 9.48 10.11
(3.0) (3.78) (3.92) Overall treatment effect F2,240⫽36.49 F2,262⫽34.22
P⬍.001 P⬍.001 Oppositional/Defiance (SD) OROS MPH 8.15 4.05† 4.91†
(4.4) (3.39) (3.93)
IR MPH 7.34 4.81† 4.98†
(4.0) (3.87) (3.81)
Placebo 8.19 8.09 8.60
(3.8) (4.63) (4.82) Overall treatment effect F2,240⫽22.94 F2,262⫽21.78
P⬍.001 P⬍.001 SD indicates standard deviation.
Appetite
Parents rated food intake as usual amount or more
than usual amount in
⬎75% of patients. At day 14,
the percentage of patients who were eating less than
usual during the previous 2 weeks was significantly
higher (
P
⬍
.001) for the 2 active treatments
com-pared with placebo (22.5%, 18.8%, and 12.0% for the
OROS MPH, IR MPH, and placebo treatments,
re-spectively). Similar results were seen on day 28.
Val-ues for patients who were receiving OROS MPH and
IR MPH treatments were not significantly different.
Tics
Thirteen patients were reported on a parent
ques-tionnaire to have had tics during the study. Nine of
these 13 patients had a history of tics prestudy. For
this study, a new onset of tics or a clinically
signifi-cant increase in tics was considered to be an AE. Five
patients had tics that were reported as AEs: 4
pa-tients on placebo and 1 on IR MPH. No patient on
OROS MPH had tics that were reported as an AE.
DISCUSSION
The results of this study show that OROS MPH
administered once a day and IR MPH administered 3
times a day were significantly better than placebo
and not significantly different from each other for the
primary efficacy measure, teacher IOWA Conners
I/O subscale score, which evaluated attention and
behavior at school. Furthermore, a significant
im-provement in attention and behavior was seen in the
first week for patients who were taking OROS MPH
qd or IR MPH tid compared with placebo, and this
improvement was maintained throughout the 4
weeks of the study. These results were consistent
across settings (home and school), raters (parents,
teachers,
clinical
investigators),
and
measures
(IOWA Conners, SNAP-IV, Peer Interaction, Global
Assessments, Parent Satisfaction) and were
statisti-cally significant.
Determination of effect sizes for the 2 active
treat-ments versus placebo yielded values of 1.05 for
OROS MPH and 1.02 for IR MPH. These values are
TABLE 5. Secondary Efficacy Measures: Mean Scores at Baseline and End of Study
Rater Measure Treatment Baseline End of Study
Teacher Peer Interaction (SD) (n⫽271) (n⫽236)
OROS MPH 0.88 0.55†
(0.7) (0.59)
IR MPH 0.69* 0.48†
(0.6) (0.61)
Placebo 0.97 0.96
(0.7) (0.78) Overall Treatment Effect F2,233⫽0.82
P⬍.001
SNAP-IV Inattention (SD) (n⫽274) (n⫽236)
OROS MPH 2.03 1.34†
(0.7) (0.84)
IR MPH 2.06 1.26†
(0.6) (0.79)
Placebo 2.04 1.97
(0.7) (0.79) Overall Treatment Effect F2,233⫽16.40
P⬍.001 SNAP-IV Hyperactivity/Impulsivity (SD) (n⫽274) (n⫽236)
OROS MPH 1.60 0.96†
(0.9) (0.79)
IR MPH 1.62 0.93†
(0.8) (0.79)
Placebo 1.00 1.57
(0.8) (0.89) Overall Treatment Effect F2,233⫽4.23
P⬍.001 SNAP-IV Oppositional
Defiant Disorder (SD)
(n⫽274) (n⫽237)
OROS MPH 0.89 0.53†
(0.9) (0.69)
IR MPH 0.76 0.44†
(0.8) (0.61)
Placebo 0.96 0.95
(0.8) (0.87) Overall Treatment Effect F2,234⫽10.42
P⬍.001
Global Efficacy (n⫽233)
OROS MPH ND 1.42†
(0.97)
IR MPH ND 1.43†
(1.01)
Placebo ND 0.62
(0.81) Overall treatment effect F2,230⫽17.64
greater than those recently reported for the highly
controlled, double-blind MTA MPH titration trial,
which reported effect sizes of 0.8 and 1.0 for MPH.
18The response rate for Clinical Global Impressions
(Clinical Global Impressions for the IR MPH group
was not different from that of the MTA Cooperative
study [55%]).
13Any comparisons between this study
and the MTA study, however, should be viewed
with caution because the 2 studies have very
differ-ent study designs (this study used a placebo
com-parator, whereas the MTA study used a “treatment
as usual” group), different age ranges (this study
enrolled children 6 –12 years of age, whereas the
MTA study involved children 7–9 years of age who
thus were more likely to have been naı¨ve to all
treatments), and different study durations (this
study lasted 1 month, whereas the MTA study lasted
14 months), and drug dosage adjustment was
al-lowed in the MTA study but not in this study.
No serious AEs were reported during this study.
The majority of patients did not report any AEs, and
the majority of those reported were mild. This may
be attributable, in part, to the fact that 75% of
pa-tients were already receiving MPH before entering
the study. The mean daily dose that patients were
receiving in this study (1.1
⫾
0.5 mg/kg/d for OROS
MPH and 0.9
⫾
0.4 mg/kg/d for IR MPH) was not
meaningfully different from the average dose given
in other studies. For example, the average dose given
at the end of the MTA study ranged from 1.2 to 1.3
mg/kg/d.
13However, these are the mean doses;
thus, the dose received by some individual patients
TABLE 5. Continued
Rater Measure Treatment Baseline End of Study
Parent SNAP-IV Inattention (SD) (n⫽276) (n⫽250)
OROS MPH 2.29 1.38†
(0.5) (0.68)
IR MPH 2.16 1.39†
(0.6) (0.73)
Placebo 2.18 2.00
(0.5) (0.78) Overall treatment effect F2,247⫽19.15
P⬍.001 SNAP-IV Hyperactive/Impulsive (SD) (n⫽276) (n⫽251)
OROS MPH 2.02 1.11†
(0.6) (0.65)
IR MPH 1.84 1.10†
(0.7) (0.69)
Placebo 1.99 1.83
(0.7) (0.89) Overall treatment effect F2,248⫽24.79
P⬍.001 SNAP-IV Oppositional
Defiance Disorder (SD)
(n⫽278) (n⫽251)
OROS MPH 1.56 0.91†
(0.8) (0.66)
IR MPH 1.36* 0.95†
(0.7) (0.67)
Placebo 1.61 1.54
(0.8) (0.94) Overall treatment effect 2,248⫽17.44
P⬍.001
Global Efficacy (n⫽247)
OROS MPH ND 1.47†
(1.07)
IR MPH ND 1.28†
(0.93)
Placebo ND 0.61
(0.93) Overall treatment effect F2,244⫽16.71
P⬍.001 Investigator Mean Clinical Global Impression (n⫽263)
OROS MPH ND 4.24†
(1.34)
IR MPH ND 4.19†
(1.45)
Placebo ND 2.48
(1.67) Overall treatment effect F2,260⫽39.35
P⬍.001 Clinical Global Impression
(% patients much/very much improved)
(n⫽192)
OROS MPH ND 46.7%
IR MPH ND 47.2%
Placebo ND 16.7%
ND indicates not done.
was significantly higher (eg, range for OROS MPH,
0.3–2.5 mg/kg/d). The low incidence of AEs thus is
unlikely to be attributable to the use of lower doses.
However, one would expect a greater incidence of
AEs in individual patients in whom higher doses are
used, as reported in previous studies of lower and
higher doses of IR MPH.
19,20Overall, the type and
incidence of AEs reported in this study were
consis-tent with previous work with MPH.
19The results from this study are limited by the 26%
attrition rate, concentrated in the placebo treatment
arm. The dropout rate in the placebo group (48%) by
the end of the treatment was higher than that found
in either the OROS MPH group (16%) or the IR MPH
group (14%). Unless adjusted for in the analysis, this
attrition biases toward a Type II error (ie, accepting
the hypothesis of no difference when there are real
differences).
The primary reason for attrition in the placebo
group was lack of efficacy, which reflects that the
appropriate patient population (ie, patients requiring
medication) was enrolled in the study. This may be
related to the fact that 75% of study patients had
been taking stimulant medication before the
begin-ning of the study. The proportion of stimulant-naı¨ve
patients (25%) was much lower than in the MTA
study, in which 66% were stimulant naı¨ve.
13Families
that are familiar with their child’s response to
stim-ulant medication would be more aware of whether
the medication showed a lack of effect and would be
quick to abandon placebo.
In comparison with the placebo group, the rate of
patient discontinuation for lack of efficacy was
sig-nificantly lower on both the OROS MPH and IR
MPH treatments (
P
⬍
.001 with log-rank and
Wil-coxon tests). No significant difference was seen in the
number of dropouts in the 2 active treatment groups.
The study was not designed to assess duration of
treatment effect and thus is not able to demonstrate
whether the duration of daily clinical effects of OROS
MPH is comparable to those of IR MPH tid.
How-ever, this has been demonstrated in previous
con-trolled crossover studies comparing OROS MPH qd
with IR MPH tid and placebo.
6,21,22Other limitations
of the current study include the participation of
eval-uators who were not independent of the clinicians
adjusting the medication and the need to exclude one
of the treatment sites.
The results of this study indicate that OROS MPH
dosed qd provides efficacy superior to placebo and
not significantly different from IR MPH dosed tid.
The convenience of once-daily dosing could provide
additional benefits. Because OROS MPH will
elimi-nate the need for dosing in school and after school,
it potentially could eliminate the embarrassment that
a child may feel when called to report to a school
authority for medication, the bureaucracy required
at school to administer a controlled substance to a
child, and the potential for diversion of the drug.
ACKNOWLEDGMENTS
This study was funded by ALZA Corporation (Mountain View, CA) on behalf of Crescendo Pharmaceuticals Corporation (Moun-tain View, CA). M.W., L.L.G., W.P., J.S., and T.W. are paid con-sultants of ALZA Corporation.
We thank the members of the Concerta Study Group and, in particular, J.S. and W.P. for their early work in this program.
The Concerta Study Group: Howard Abikoff, PhD (New York University Child Study Center); Marc Atkins, PhD (University of Illinois at Chicago); Gerald August, PhD (University of Minneso-ta); Joseph Biederman, MD (Harvard University); Oscar Bukstein, MD (Western Psychiatric Institute and Clinic, University of Pitts-burgh); C. Keith Conners, PhD (Duke University); Laurence Greenhill, MD (New York State Psychiatric Institute); Martin Hoff-man, MD (University of Buffalo School of Medicine); Marc Lerner, MD (University of California at Irvine); Keith McBurnett, PhD (University of Chicago); Donna Palumbo, PhD (University of Rochester); William Pelham, PhD (State University of New York at Buffalo); Mark Stein, PhD (Children’s National Medical Center); James Swanson, PhD (University of California at Irvine); Sharon Wigal, PhD (University of California at Irvine); Timothy Wilens, MD (Massachusetts General Hospital); and Mark Wolraich, MD (Vanderbilt University).
REFERENCES
1. IMS Health. National Prescription Audit Plus. Meeting. Plymouth, PA; December 1999
2. American Psychiatric Association.Diagnostic and Statistical Manual of Mental Disorders(DSM-IV). 4th ed. Washington, DC: American Psychi-atric Association; 1994
3. Greenhill L. Attention-deficit hyperactivity disorder: the stimulants.
Child Adolesc Psychiatr Clin North Am. 1995;4:123–169
4. Physicians’ Desk Reference. 54th ed. Montvale, NJ: Medical Economics Company, Inc; 2000:2041
5. Swanson J, Gupta S, Guinta D, et al. Evaluation of different methyl-phenidate (MPH) delivery patterns for the treatment of children with ADHD.Neurology. 2000;54 (abstract)
6. Swanson J, Gupta S, Lam A, et al. Development of a new once-a-day formulation of methylphenidate for the treatment of ADHD: Proof of concept and proof of product studies.Arch Gen Psychiatry. In press 7. Shaffer D, Fisher P, Dulcan M, et al. The NIMH Diagnostic Interview
Schedule for Children Version 2.3 (DISC-2.3): description, acceptability, prevalence rates, and performance in the MECA study.J Am Acad Child Adolesc Psychiatry. 1996;35:865– 877
8. Swanson J.School-Based Assessments and Interventions for ADD Students. Irvine, CA: K. C. Publishing; 1992
9. Loney J, Milich R. Hyperactivity, inattention, and aggression in clinical practice. In Wolraich M, Routh DK, eds.Advances in Development and Behavioral Pediatrics. Greenwich, CT: JAI Press; 1982:113–147 10. Shaffer D, Gould MS, Brasic J, et al. A children’s global assessment scale
(CGAS).Arch Gen Psychiatry. 1983;40:1228 –1231
11. Swanson J, Greenhill L, Pelham W, et al. Initiating Concerta (OROS methylphenidate HCl) qd in children with attention-deficit hyperactiv-ity disorder.J Clin Res. 2000;3:59 –76
12. Atkins MS, Pelham WE, Licht MH. The differential validity of teacher ratings of inattention/overactivity and aggression.J Abnorm Child Psy-chol. 1989;17:423– 435
13. MTA Cooperative Group. 14-month randomized clinical trial of treat-ment strategies for attention deficit hyperactivity disorder.Arch Gen Psychiatry. 1999;56:1073–1086
15. Connors CK, Barkley RA. Clinical Global Impression Scale (CGI). Psy-chopharmacol Bull. 1985;21:809 – 843
16. Emslie GJ, Rush AJ, Weinberg WA, et al. A double-blind, randomized, placebo-controlled trial of fluoxetine in children and adolescents with depression.Arch Gen Psychiatry. 1997;54:1031–1037
17. Modi NB, Lindemulder B, Gupta SK. Single and multiple-dose phar-macokinetics of an oral once-a-day osmotic controlled release OROS (methylphenidate HCl) formulation.J Clin Pharmacol. 2000;40: 379 –388
18. Swanson JM, Kraemer HC, Hinshaw SP, et al. Clinical relevance of the primary findings of the MTA: success rates based on severity of symp-toms at the end of treatment.J Am Acad Child Adolesc Psychiatry. 2001; 40:168 –179
19. Barkley RA, McMurray M, Edelbrock CS, Robbins K. Side effects of
methylphenidate in children with attention deficit hyperactivity disorder: a systemic, placebo-controlled evaluation.Pediatrics. 1990;86: 184 –192
20. Ahmann PA, Waltonen SJ, Olson KA, Theve FW, Van Erem AJ, LaPlant RJ. Placebo-controlled evaluation of Ritalin side effects.Pediatrics. 1993; 91:1101–1106
21. Pelham WE, Hoffman MT, Lock T, and the SUNY CONCERTA Study Group. Evaluation of once-a-day OROS methylphenidate HCl (MPH) extended-release tablets versus MPH tid in children with ADHD in natural school settings.Pediatric Res. 2000;47:31A (abstract)
22. Pelham WE, Hoffman MT, Lock T, and the SUNY CONCERTA Study Group. Evaluation of once-a-day OROS methylphenidate HCl (MPH) extended-release tablets versus MPH tid in children with ADHD in a laboratory school.Pediatric Res. 2000;47:31A (abstract)
‘‘SOUTH PARK’ TAKES GROSS TO NEW FRONTIER
“In the last decade, the occasional profanity has crept into network and
basic-cable television. Dennis Franz has made an array of taboo utterances on ABC’s
”NYPD Blue.“ Mark Harmon used the 4-letter word for dung last year on CBS’s
”Chicago Hope.“ Even Ted Koppel used a variation on that word in the heat of a
tough interview 2 years ago on ABC’s ”Nightline.“
But Comedy Central’s “South Park” took the cursing crown last week. In an
episode first shown on Wednesday, characters used the dung-related word 162
times with nary a censor’s beep. . . . The Comedy Central executive vice-president
said he had hardly received any reaction from viewers—just 4 e-mail messages, all
supportive . . . “No one cares anymore,” he relented. “The standards are almost
gone.”
New York Times. June 25, 2001