Randomized Trial of Nasal Synchronized Intermittent Mandatory
Ventilation Compared With Continuous Positive Airway Pressure After
Extubation of Very Low Birth Weight Infants
Keith J. Barrington, MBChB, MRCP, FRCP*; Dale Bull, MD‡; and Neil N. Finer, MD, FRCP‡
ABSTRACT. Objective. To determine whether nonin-vasive, nasal synchronized intermittent mandatory ven-tilation (nSIMV) improves the likelihood that very low birth weight infants will be successfully extubated.
Methods. Infants of<1251-g birth weight who were due to be extubated before 6 weeks of age were eligible once they were receiving <35% oxygen and were on a ventilator rate of<18 breaths per minute (bpm). Extuba-tion was performed following intravenous loading with aminophylline, after a successful trial of 12 hours of endotracheal synchronized intermittent mandatory ven-tilation at a rate of 8. Infants were randomized to either nasal continuous positive airway pressure (nCPAP) at 6 cm H2O or nSIMV after extubation. nSIMV was com-menced at a rate of 12 bpm with pressure on the venti-lator set to achieve a delivered pressure of at least 12 cm H2O and a peak end expiratory pressure of 6 cm H2O. Continuous recording for diagnosis of apnea was per-formed for 72 hours after extubation. Objective criteria for failure of extubation were as follows: a PaCO2 >70; FIO2>0.7; or severe recurrent apnea (>2 apneas requiring intermittent positive-pressure ventilation in 24 hours or
>6 apneas>20 seconds per day). The study ended after 72 hours postextubation or when infants satisfied failure criteria. A sample size of 54 was determined by power analysis.
Results. Mean birth weight (831 standard deviation [SD]: 193 g) and gestation (26.3 SD: 1.8 weeks) did not differ between groups. Mean age at extubation was 7.6 (SD: 9.7) days, range 1 to 40 days. The nSIMV group had a lower incidence of failed extubation 4/27 compared with the continuous positive airway pressure group, 12/ 27. This was attributable to both a decreased incidence of apnea and a decreased incidence of hypercarbia. There was no increase in the incidence of abdominal distension or feeding intolerance.
Discussion. nSIMV is effective in preventing extuba-tion failure in very low birth weight infants in the first 72 hours after extubation. Noninvasive ventilation may have other roles in the care of the very low birth weight infant. Pediatrics 2001;107:638 – 641; extubation,
prema-ture infant, randomized trial, continuous positive airways pressure, noninvasive ventilation.
ABBREVIATIONS. VLBW, very low birth weight; CPAP, contin-uous positive airway pressure; nSIMV, nasal synchronized inter-mittent mandatory ventilation; nCPAP, nasal continuous positive airway pressure; SIMV, synchronized intermittent mandatory ventilation; SD, standard deviation.
E
arly extubation of the very low birth weight (VLBW) infant holds the potential for a num-ber of benefits for the infant, including a de-crease in calorie consumption,1 decreased trachealand laryngeal injury, decreased nosocomial pneumo-nia2and sepsis,3and a decreased incidence and
se-verity of bronchopulmonary dysplasia. VLBW in-fants, however, frequently fail attempts at extubation because of severe apnea, hypoventilation, atelectasis, or other intercurrent illnesses. It has recently been demonstrated by our group that noninvasive venti-lation via nasal prongs can provide respiratory sup-port in the VLBW infant.4This mode of ventilation
holds the promise of providing significant respira-tory support without endotracheal intubation and its accompanying complications. We wanted to deter-mine if this means of support would improve the likelihood of infants being successfully extubated.
Systematic reviews of the previous randomized controlled trials have demonstrated the efficacy of pre-extubation aminophylline loading, at least in in-fants⬍1 kg,5and postextubation continuous positive
airway pressure (CPAP)6 in improving the chances
of successful extubation. A single study of routine pre-extubation doxapram loading proved ineffective, however.7 We hypothesized that there would be a
significant reduction in the incidence of failed extu-bation in aminophylline treated infants of ⬍1251 g birth weight, before 42 days of age, with nasal syn-chronized intermittent mandatory ventilation (nSIMV) compared with nasal CPAP.
METHODS
Infants of⬍1251 g birth weight, in the neonatal intensive care unit of the University of California, San Diego medical center, who were due to be extubated before 6 weeks of age were eligible for the study once they were receiving⬍35% oxygen and were on a ventilator rate of ⬍18 breaths per minute. Infants with lethal anomalies were excluded. The study took place between March 1996 and January 1999. Parental consent was obtained before randomization. The randomization codes were generated from a table of random numbers and placed in sequentially numbered opaque sealed envelopes. Masked randomization was to either nasal continuous positive airway pressure (nCPAP) or nSIMV after extubation. Infants were loaded with intravenous
aminoph-From the *Department of Pediatrics, McGill University, Montreal, Quebec, Canada and ‡Division of Neonatal/Perinatal Medicine, Department of Pe-diatrics, University of California-San Diego, San Diego, California. Received for publication Jan 20, 2000; accepted Aug 3, 2000.
Reprint requests to (K.J.B.) Royal Victoria Hospital, 687 Pine Ave W, Room C7.68, Montreal, Quebec, H3A 1A1 Canada. E-mail: [email protected]
ylline in a dose of 6 mg/kg before extubation, followed by a maintenance dose of 2 mg/kg every 8 hours. If⬎24 hours elapsed between aminophylline loading and extubation, the serum con-centration was checked. The ventilator rate was weaned every 3 hours as long as the arterial or capillary blood Pco2was⬍65 mm
Hg. Transcutaneous Pco2was measured routinely and blood gas
analysis was performed at least every 6 hours as well as to confirm significant elevations in the transcutaneous Pco2. Extubation was
performed, after a successful trial of 12 hours of endotracheal synchronized intermittent mandatory ventilation (SIMV) at a rate of 8, without elevation in the Pco2to above 65 mm Hg or increase
in the Fio2to⬎35%. nSIMV was commenced at a rate of 12 with
ventilator pressures set at a peak of 16 cmH2O and a peak end
expiratory pressure of 6 cmH2O. The Infantstar ventilator with the
pneumatic Starsync capsule applied to the infant’s abdomen was used (Mallinckrodt, St Louis, MO) with the Hudson nasal prong system (Hudson Co, Temecula, CA). Set ventilator pressures were increased to achieve a measured pressure of at least 12 cmH2O;
nCPAP was administered with the same prong system at a pres-sure of 6 cmH2O.
Continuous recording for diagnosis of apnea was performed for 72 hours after extubation. Recordings of transthoracic imped-ance, heart rate, pulse oximeter saturation, and nasal air flow by thermistor were performed, although the thermistor signal was often difficult or impossible to interpret because of the gas flow from the CPAP system. Failure of extubation was diagnosed when any 1 of the following was present: a Paco2⬎70, an Fio2⬎0.7 to
maintain pulse oximeter saturation above 92%, or severe recurrent apnea (⬎2 apneas requiring IPPV in 24 hours or⬎6 apneas⬎20 seconds per day). Apnea was diagnosed from the recordings when bradycardia to⬍100 beats per minute or acute desaturation to
⬍80% was seen, without obvious respiratory airflow on the re-cording. The system used for nSIMV will deliver a breath every 5 seconds at a regular rate when the infant is apneic; these breaths were often visible on the recordings during spontaneous apnea, and may be differentiated from spontaneous breaths by their precisely regular appearance. However, we recognize that there is potential for error in the interpretation of these recordings. The majority of the apneas were diagnosed from the occurrence of acute bradycardia, and with the frequent failure to obtain nasal airflow tracings, obstructive apneas without bradycardia will have been missed. The study ended at 72 hours after extubation or when infants satisfied failure criteria.
During nCPAP or nSIMV, the infants continued to be fed either by bolus feedings every 3 hours or by continuous nasogastric infusion. Gastric aspirates were measured every 3 hours and if the volume was⬎20% of the previous feed or the past 3 hours feeding volume, then the next feed was usually withheld or the continu-ous feeds were stopped, particularly if accompanied by abdominal distension. After an additional 3 hours, if there was no longer a residual and the clinical examination of the abdomen was accept-able, then feeds were restarted at a lower volume.
The study was approved by the institutional review board of University of California San Diego medical center.
We hypothesized that a reduction in extubation failure as de-fined above from 30% to 10% would be clinically useful. Using a
of 0.8 and␣of 0.05 and a 2-tailed test, a sample size of 54 was determined.
Statistical comparison of the outcomes of the 2 groups was by Fisher’s exact test for proportions and by the 2-tailed unpaired t test for continuous variables.
RESULTS
Fifty-four infants were enrolled in the study; 27 per group. Mean birth weight (831 standard devia-tion [SD]:193 g) and gestadevia-tion (26.3 SD: 1.8 weeks) did not differ between groups. Mean age at extuba-tion was 7.6 (SD: 9.7) days, range 1 to 40 days; there was no significant difference between groups (Table 1). The age of extubation had a very skewed distri-bution with a preponderance of infants extubated in the first 3 days. Median age of extubation was 3 days in each group, with ranges from 12 hours to 29 days in the nSIMV group and 12 hours to 40 days in the
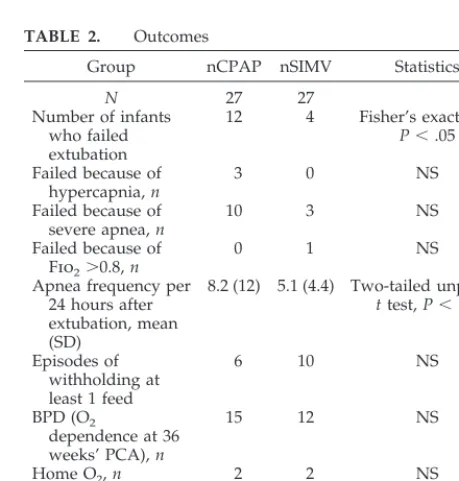
nCPAP group. The nSIMV group had a lower inci-dence of failed extubation (4/27) compared with the nCPAP group, (12/27), Fisher’s exact test P ⬍ .05. This was attributable to both a decreased incidence of apnea and a decreased incidence of hypercarbia (Table 2). There was no increase in the incidence of abdominal distension or feeding intolerance. There were no cases of GI perforation, and no infants de-veloped necrotizing enterocolitis after randomiza-tion.
DISCUSSION
We have demonstrated an improvement in the success rate of extubation of VLBW infants by the application of nSIMV in comparison to nasal CPAP. This is a relatively new approach to respiratory as-sistance in the newborn and holds the potential for reducing the iatrogenic complications of neonatal intensive care. Previous work from this center showed that the application of nSIMV was associated with a reduction in thoraco-abdominal asynchrony.4
This suggested that the chest wall was effectively stabilized during nSIMV, and that overall lung me-chanics were thereby improved.
Failure of extubation is a common problem in very premature infants, and methods for preventing such failure have been the subject of a number of stud-TABLE 1. Characteristics of Study Infants
nCPAP nSIMV Statistics Birth weight 864 (167) 816 (241) NS Gestation 26.1 (1.4) 26.1 (1.7) NS Age at extubation 7.9 (6.7) 6.8 (7.2) NS Fio2before
extubation
0.26 (0.1) 0.23 (0.14) NS
NS indicates not significant.
TABLE 2. Outcomes
Group nCPAP nSIMV Statistics
N 27 27
Number of infants who failed extubation
12 4 Fisher’s exact test,
P⬍.05
Failed because of hypercapnia, n
3 0 NS
Failed because of severe apnea, n
10 3 NS
Failed because of Fio2⬎0.8, n
0 1 NS
Apnea frequency per 24 hours after extubation, mean (SD)
8.2 (12) 5.1 (4.4) Two-tailed unpaired
t test, P⬍.05
Episodes of withholding at least 1 feed
6 10 NS
BPD (O2
dependence at 36 weeks’ PCA), n
15 12 NS
Home O2, n 2 2 NS
Duration of hospital stay, days, mean (SD)
92 (26) 86 (23) NS
NS indicates not significant; BPD, bronchopulmonary dysplasia; O2, oxygen; PCA, postconceptional age.
ARTICLES 639 at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news
ies.5–7 We combined the 2 techniques previously
demonstrated effective, nasal CPAP and aminophyl-line, to compare with the application of the new technique.
Noninvasive ventilation by nasal mask or prongs has been long practiced in adults8 and older
chil-dren9 with many reports of efficacy and reduced
complications2compared with endotracheal
intuba-tion. However, there are no previous controlled stud-ies of nSIMV in the newborn infant. Older uncon-trolled studies of unsynchronized nasal ventilation suggested that occasional gastrointestinal perfora-tion could occur,10and a controlled study of
unsyn-chronized nasal intermittent mandatory ventilation, which we performed, showed no advantages in the treatment of apnea of prematurity.11A more recent
small trial of unsynchronized intermittent manda-tory ventilation12 suggested, in contrast, that there
may be an effect in the therapy of apnea of prema-turity, but apnea diagnosis in that trial was largely from nursing observations, which are notoriously unreliable for that purpose.13 The development of
synchronized ventilators for the newborn infant pre-sents a number of potential advantages for nasal ventilation. Thus, positive pressure ventilator breaths will be delivered only after initiation of a respiratory effort by the infant, when the glottis is likely to be open, or after an apneic interval, the duration of which would depend on ventilator set-tings. There are 2 additional studies using nSIMV that we are aware of, both of which are published as abstracts. Visveshwara et al14presented preliminary
information on the use of nSIMV in a group of in-fants recovering from respiratory distress syndrome and showed that those infants with a low expiratory resistance may be successfully managed with this approach. Friedlich et al15have provided results of
a prospective trial of 41 VLBW infants who were randomized at extubation to either nSIMV or nasal CPAP. They reported a significantly lower incidence of extubation failure in the nSIMV group (5% vs 37%,
P⫽.016). Friedlich’s study (n⫽41) used a different methodology, using a single, long nasopharyngeal prong, but the similar direction of the results sup-ports the suggestion that noninvasive ventilation may have a role to play in the extubation of the VLBW infant.
The current study has confirmed that nSIMV has a therapeutic effect in decreasing apnea and decreas-ing the incidence of elevated Paco2. As a result,
nSIMV is effective in preventing extubation failure, as we defined it, in VLBW infants in the first 72 hours after extubation when extubated during the first 42 days of life. We chose to only study infants during this period as we believed that extubation failure in infants with established fibrotic lung disease, ie, after 6 weeks of age, would be less likely to be affected by nSIMV, although we do not have any data to support that contention. We did not demonstrate an increase in complications, but the power of the study to detect an increase in rare complications was low.
We also recognize the difficulties in diagnosing
apnea while receiving nasal ventilation; although fre-quently the apneas were obvious, the large airflows made recordings from the thermistor frequently dif-ficult or impossible to interpret.
Noninvasive ventilation may have other roles in the care of the VLBW infant; whether this method could be used for initial respiratory support in pref-erence to endotracheal intubation deserves investi-gation. Use of nSIMV for primary or back-up therapy of apnea should also be studied. Larger prospective studies would be required to determine the potential incidence of rare complications such as gastrointes-tinal perforation, and the effects of longer term nSIMV.
Our study was not designed to evaluate long-term outcomes, which would require a much larger study. We suggest that a trial of noninvasive ventilation used as both an alternative to initial intubation and an aid to even earlier successful extubation should be considered. The primary outcome for such a study should be the development of bronchopulmonary dysplasia, as this disorder has substantial health im-plications. Secondary outcomes, such as length of hospital stay and cost of treatment, should also be considered. Although our average age of extubation was between 6 to 8 days, the median age was 3 days, and we currently believe that an even shorter period of intubation is possible using noninvasive ventila-tory support. We believe that the use of noninvasive ventilatory techniques will significantly reduce neo-natal morbidity, and hope that our observations will stimulate additional prospective evaluations of these approaches.
REFERENCES
1. Roze JC, Chambile B, Fleury MA, Debillon T, Gaultier C. Oxygen cost of breathing in newborn infants with long term ventilatory support. J
Pe-diatr. 1995;127:984 –987
2. Guerin C, Girard R, Chemorin C, DeVarax R, Fournier G. Facial mask noninvasive mechanical ventilation reduces the incidence of nosocomial pneumonia. Intensive Care Med. 1997;23:1024 –1032
3. Stoll BJ, Gordon T, Korones SB, et al. Late-onset sepsis in very low birth weight neonates: a report from the National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1996; 129:63–71
4. Kiciman N, Andreasson B, Bernstein G, et al. Thoracoabdominal motion in newborns during ventilation delivered by endotracheal tube or nasal prongs. Pediatr Pulmonol. 1998;25:175–181
5. Henderson-Smart DJ, Davis PG. Prophylactic methylxanthine for extu-bation in preterm infants (Cochrane Review). In: The Cochrane Library. Issue 4. Oxford, England: Update Software;1998
6. Davis PG, Henderson-Smart DJ. Prophylactic post-extubation nasal CPAP in preterm infants (Cochrane Review). In: The Cochrane Library. Issue 4. Oxford, England: Update Software; 1998
7. Barrington KJ, Muttitt SC. Randomized, controlled, blinded trial of doxapram for extubation of the very low birthweight infant. Acta
Pae-diatr. 1998;87:191–194
8. Keenan S, Kernerman PD, Cook DJ, Martin CM, McCormack D, Sibbald WJ. Effect of noninvasive positive pressure ventilation on mortality in patients admitted with acute respiratory failure: a meta-analysis. Crit
Care Med. 1997;25:1685–1692
11. Ryan CA, Finer NN. Nasal intermittent positive-pressure ventilation offers no advantages over nasal continuous positive airway pressure in apnea of prematurity. Am J Dis Child. 1989;143:1196 –1198
12. Lin C-H, Wang S-T, Lin Y-J, Yeh T-F. Efficacy of nasal intermittent positive pressure ventilation in treating apnea of prematurity. Pediatr
Pulmonol. 1998;26:349 –353
13. Muttitt SC, Finer NN, Tierney AJ, Rossmann J. Neonatal apnea: diag-nosis by nurse versus computer. Pediatrics. 1988;82:713–720
14. Visveshwara N, Caliwaq W, Peck M, et al. Feasibility of early extubation in RDS, with application of nasal ventilation, as predicted by end-expiratory resistance. Pediatr Res. 1996;39:355A
15. Friedlich P, Lecart C, Posen R, Ramicone E, Chan L, Ramanathan R. A randomized trial of nasopharyngeal-synchronized intermittent manda-tory ventilation versus nasopharyngeal continuous positive airway pressure in very low birth weight infants after extubation. J Perinatol. 1999;19:413– 418
SURVEY SHOWS SEX PRACTICES OF BOYS
After decades in which researchers concerned about teenage pregnancy focused only on intercourse, a study by the Urban Institute, financed by the federal government, provides the first national data on the sexual practices of 15- to 19-year-old boys . . . The report of findings from the National Survey of Adolescent
Males was released in the latest issue of Family Planning Perspectives, a publication
of the Alan Guttmacher Institute. The issue includes a report on the policy impli-cations of oral sex among young people.
The survey of adolescent boys was based on in-person interviews with 1297 nationally representative males ages 15 to 19 in 1995, including an oversampling of black and Hispanic youths. An earlier round in 1988 surveyed 1880 boys.
. . . According to the findings, more than 1 in 10 boys had engaged in anal intercourse, half had received oral sex from a girl, and slightly more than a third had performed oral sex on a girl . . . Many adolescents, according to the report, consider oral sex to be a precursor or substitute for intercourse and something that does not count as “sex.”
In 1996, as part of an effort to reduce teenage pregnancy, Congress provided $50 million a year for 5 years for abstinence-only education. To be eligible for the money, states had to offer programs teaching “abstinence from sexual activity outside marriage as the expected standard for school-age children.”
Since then, researchers, public health experts and health care workers have found that many young people perceive oral and anal sex as something other than sex—and often, even, as abstinence.
In research last year among Midwestern teenagers 12 through 17 who had received abstinence education, there was no consensus on what qualified as absti-nence.
And in an earlier survey of college freshmen and sophomores in the South, a quarter considered anal intercourse as abstinence, and more than a third thought the same of oral sex. Another study found that more than half of the college undergraduates surveyed did not consider oral sex to be sex, and that the propor-tions were even higher if the act had not resulted in orgasm.
And in 1998, President Clinton, in testimony about an affair with a White House intern, said he had not had “sexual relations” but had engaged only in oral sex.
Abstinent or not, the public health risks of oral and anal sex are real.
Lewin T. New York Times. December 19, 2000
Noted by JFL, MD
ARTICLES 641 at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news
DOI: 10.1542/peds.107.4.638
2001;107;638
Pediatrics
Keith J. Barrington, Dale Bull and Neil N. Finer
Low Birth Weight Infants
Compared With Continuous Positive Airway Pressure After Extubation of Very
Randomized Trial of Nasal Synchronized Intermittent Mandatory Ventilation
Services
Updated Information &
http://pediatrics.aappublications.org/content/107/4/638
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/107/4/638#BIBL
This article cites 13 articles, 2 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
http://www.aappublications.org/cgi/collection/agency_abcs
Agency ABC's
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.107.4.638
2001;107;638
Pediatrics
Keith J. Barrington, Dale Bull and Neil N. Finer
Low Birth Weight Infants
Compared With Continuous Positive Airway Pressure After Extubation of Very
Randomized Trial of Nasal Synchronized Intermittent Mandatory Ventilation
http://pediatrics.aappublications.org/content/107/4/638
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2001 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news