Charles W. Kerber1
Received August 14, 1979; accepted Septem-ber 19, 1979.
This work was supported in part by a grant from W. I. Patterson Charitable Fund, Pittsburgh, PA 15222.
This manuscript appears in January/February AJNR and March AJR.
Presented at the annual meeting of the Ameri-can Society of Neuroradiology, Toronto, May 1979.
, Department of Radiology, Presbyterian-Un
i-versity Hospital, DeSoto at O'Hara St., Pittsburgh, PA 15213.
AJNR 1:77-81, January/February 1980 0195-6108/80/0011-0077 $00.00 © American Roentgen Ray Society
77
Flow-Controlled Therapeutic
Embolization:
A Physiologic and Safe Technique
A feared complication of therapeutic embolization is loss of control of one or more particles with resultant ischemic infarction of normal tissues. To avoid passage of emboli into normal arteries, the delivery catheter may be wedged tightly into the artery or the artery completely occluded with a balloon catheter during embolus injection. These techniques, termed occlusion control, were a valuable forward step and signifi-cantly enhanced patient safety. However, occluding the vessel completely may cause spasm, and allows the operator to introduce fluid and emboli under higher than normal perfusion pressures which can open extra- to intracranial shunts and cause disastrous intracranial embolization.
A further refinement is suggested. First, the emboli are suspended in contrast agent; then the particles are introduced while arterial runoff of the contrast agent is watched so the acceptance rate of the artery is not exceeded. Normal perfusion pressures and flow then carry the embolus distally into the abnormality being treated. This technique is safe, easily learned, and gives the radiologist direct vision control over the emboli-zation process. It has been used in 39 patients with only one serious complication.
Therapeutic embolization, the deliberate occlusion of the blood supply of vascular tumors and arteriovenous malformations is of value both as a primary treatment and as an adjunct to surgery when operative blood loss should be reduced [1 -11]. Most complications of this technique occur when emboli pass to
normal tissues and cause ischemic infarction [12-14].
To avoid this problem, some have advocated tightly wedging the catheter into the feeding vessel or occluding the artery completely with a balloon catheter
[15]. We have developed, used, and favor a different, more physiologic technique
of control and report its rationale and use.
Technique
A 4 standard, 5 standard, or 5.8 French, thin-wall, polyethylene catheter is directed into the artery to be occluded using percutaneous techniques and fluoroscopic control. Entry into the femoral or other artery is usually via a 6 or 5 French Cordis sheath. The catheter tip position is verified with cut films, fluor-oscopy, or preferably instant electronic subtraction. Care is taken not to cause arterial spasm either with the leading guide wire or the catheter. The embolic material is prepared by suspending it in full strength Conray 60 [16-18].
A contrast-filled syringe of the same size as that containing the emboli is connected to the catheter, and contrast agent is introduced while the arterial runoff is watched fluoroscopically. The angiographer thus learns the injection rate that will exceed arterial acceptance and cause contrast agent reflux. The syringe containing contrast agent and emboli is then attached to the catheter, and infusion under fluoroscopic control begins (fig. 1).
78
KERBER
sec
0.0
0.3
0.6
0.9
1.2
1.5
AJN R: 1 , Jan uary / February 1 980
[image:2.612.55.388.84.728.2]AJNR: 1 . January/February 1980 FLOW-CONTROLLED THERAPEUTIC EMBOLIZATION 79
Fig. 2.-Common carotid arterio-gram. left anterior oblique position. sub-traction. magnification technique. A. Vascular mass within carotid bifurcation displaces proximal internal carotid artery posteriorly. B, After embolization: 5 French polyethylene catheter was placed just distal to superior thyroid ar-tery, and flow controlled infusion of par-ticles was carried out. Despite proximity of internal carotid artery, no emboli were lost. Only a few small feeding vessels remain; these were smaller than infused particles. Surgery 4 days later was tech -nically easy and nearly bloodless.
A
is obvious and the eye-hand coordination to slow the infu-sion is automatic, taking place via subconscious cybernetic pathways.
Complete blood flow obliteration is rarely necessary. If
the therapist waits a few minutes, or occludes a second
vessel and then returns to the original vessel to perform the
follow-up angiography, the body's own clotting mechanism
has usually completed the occlusion.
Care must still be taken when the infusion of emboli is
judged complete. Particles may remain within the catheter
or adapter. A guide wire effectively pushes these residual emboli through, but too rapid advancement of the guide wire
can have the same effect as a too rapid push on the plunger
of a syringe: emboli may enter the artery faster than they can be accepted, and reflux back alongside the catheter into normal organs. During introduction of the guide wire, contrast agent leaving the catheter tip is watched and the rate of wire advancement is slowed as necessary.
As a final safety measure, a syringe is attached to the
catheter, and 4-6 ml of blood is withdrawn. The contents of that syringe are delivered onto an absorbent towel. Fre-quently, emboli are visible. When two successive syringes
are free of emboli, it is assumed that follow-up angiography
may be performed safely.
Results
In the past 5 years, 39 patients with 37 extracranial and
two intracranial abnormalities have been treated with this
B
technique. Multiple vessels were occluded in almost all patients. An abnormality near a major normal vessel was not considered a contraindication (fig. 2).
One serious complication occurred in this series, but was
not related to this technique of flow control. A scalp slough
occurred when nonselective catheter placement allowed emboli to occlude not only a middle meningeal feeder of a
meningioma, but also a dominant superficial temporal artery
[19]. Surgery the next day further devitalized the scalp.
The procedures were performed by fellows with neurora
-diology staff supervision, or by staff alone. All radiologists
reported ease in learning the technique and felt comfortable
in its control.
Discussion
Complications from therapeutic embolization may result
from the infarction of catecholamine-producing tumors, from
passage of emboli through arteriovenous shunts into the
lungs, from clot introduced through the manipulation of
inadequately perfused coaxial catheters, and from passage of emboli through patent extra- to intracranial anastomoses [19-21]. But these are uncommon problems; the vast ma-jority of complications are caused by the reflux of embolic
materials out of the injected artery back into normal vascular
beds causing ischemic infarction.
This problem has long been recognized [12-14], and to
avoid embolus loss, tight wedging of the catheter into the
[image:3.614.196.557.85.389.2]balloon-80
KERBER AJNR: 1 , January/February 1980A
8
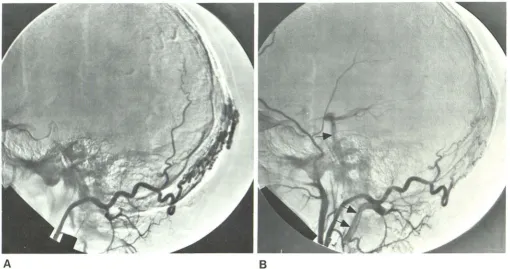
Fig. 3.- Lateral view, magnification, subtraction technique. A, Selective catheterization and nonocclusive injection of occipital artery, one of many feeders
of this scalp arteriovenous malformation. B, Alter embolization: vertebral and basilar arteries (arrows) fill when injection is performed. No particles entered these
vessels as emboli were introduced at normal perfusion pressures. One posterior fossa stroke has been caused by failing to appreciate this normal anastomosis
and potential pathway for emboli [19, 12).
tipped catheter has been advocated [1 5]. This technique is termed occlusion control of embolization because it
de-pends on the complete blockage of the artery to prevent
embolic reflux. Many safe embolizations have been pe
r-formed by occlusion control and I do not suggest that the occlusion control technique should not be used.
Occlusion control does have certain disadvantages, how -ever. Wedging a catheter into an artery frequently causes
spasm, and wedging is not practical in vessels that are large
and tortuous, such as arteries feeding arteriovenous malfor
-mations [16]. Balloon-tipped catheters are more compli -cated than simple straight catheters and add an additional
technical maneuver to the procedure. However, the most severe criticism is that occlusion control stops forward flow
of blood, contrast agent, and, most importantly, of emboli. Pressure in these blocked arteries may be high during injection, and the normal external carotid to intracranial
artery shunts may be opened to allow passage of emboli intracranially [19, 21]. Blocking the artery during injection
of material sacrifices a most important natural element of
delivery: normal forces carrying an embolus distally. Perhaps a better method is to place a catheter into a feeding artery gently so that no spasm is produced. Emboli
may then be introduced into normally flowing blood, blood
that will carry the embolus to a distal point, to impact itself there onto the arteriovenous malformation or tumor bed under normal perfusion pressures. With this flow-controlled technique, there is no chance of increasing intraluminal
pressures beyond normal, and one may embolize even in the face of patent extra-to intracranial anastamoses (fig. 3),
Most importantly, with flow-controlled embolization, the angiographer feels secure. He can see instantaneously the change in vessel runoff and may slow his injection rate appropriately before relux occurs. Large numbers of emboli may be introduced rapidly-but with control-since the fluoroscope shows real-time decreasing vessel acceptance.
Flow-controlled therapeutic embolization has shown itself to be an easily learned and safe technique. First, the partic -ulate emboli are suspended in full strength contrast agent.
Second, the feeding artery is gently catheterized so that no
spasm is produced, and good runoff remains about the catheter tip. Finally, and most importantly, the ever-decre
as-ing vessel acceptance of contrast agent (and emboli) is watched and the infusion slowed appropriately. With this
simple set of maneuvers, particles flow under physiologic pressures to the tumor bed, no arterial spasm is produced, extra- to intracranial shunts are not forced open, and the radiologist has moment-by-moment control of the
emboli-zation process.
ACKNOWLEDGMENTS
I thank Gretchen Fischer for manuscript preparation, and Norman Rabinovitz and Joseph Winstein for photographic assistance.
REFERENCES
1. Djindjian R, Cophignon J, Rey A, Theron J, Merland JJ,
[image:4.613.52.562.77.346.2]-AJNR: 1 , January/February 1980 FLOW-CONTROLLED THERAPEUTIC EMBOLIZATION 81
oral route in neuroradiology. Neuroradiology 1973; 6: 1 4 3-152
2. Serbinenko AF. Balloon catheterization and occlusion of major
cerebral vessels. J Neurosurg 1974; 41 : 125-145
3. Debrun G, Lacour P, Caron JP, et al. Traitment de fistules arterioveineuses et d'aneurysmes par balloon gonfavle et larg -able. NouvPress Med 1975; 4:2315-2318
4. Kerber CW, Bank WO, Cromwell LD. Calibrated leak mic
ro-catheter: a device for arterial exploration and occlusive
ther-apy. AJR 1979; 132:207-212
5. Luessenhop AJ, Kachmann R, Shevlin W, Ferrero AA. Clinical
evaluation of artificial embolization in the management of large
cerebral arteriovenous malformations. J Neurosurg 1965; 23: 400-417
6. Boulous R, Kricheff II, Chase NE. Value of cerebral angiogr
a-phy in the embolization treatment of cerebral arteriovenous
malformation. Radiology 1970; 97: 65-70
7. Newton TH, Adams JE. Angiographic demonstration and now
surgical embolization of spinal cord angioma. Radiology 1968;
91 :873-876
8. Hilal SK, Michelsen JW. Therapeutic percutaneous emboli
za-tion for extraaxial vascular lesions of the head, neck, and
spine. J Neurosurg 1975; 43: 275-287
9. Rosch J, Dotter CT, Brown MJ. Selective arterial embolization.
A new method for control of acute gastrointestinal bleeding.
Radiology 1972; 102: 303-306
10. Goldman ML, Land WC, Bradley EL, Anderson J. Transcatheter
intestinal bleeding. Radiology 1976; 120: 513-521
11. Hebster RE, Matricali B, Luyendijk W. Presurgical transfemoral
catheter embolization to reduce operative blood loss. J Neu
-rosurg 1974; 41 : 396-398
12. Woodside J, Schwarz H, Bergreen P. Peripheral embolization
complicating bilateral renal infarction with Gelfoam. AJR 1976;
126: 1 033-1 034
13. Gang DL, Dole KB, Adelman LS. Spinal cord infarction foll
ow-ing therapeutic renal artery embolization. JAMA 1977; 237:
2841-2842
14. Bradley EL III, Goldman ML. Gastric infarction after therapeutic embolization. Surgery 1976; 79: 421 -424
15. Greenfield AJ, Athanasoulis CA, Waltman AC, LeMoure ER.
Transcatheter embolization: prevention of embolic reflux using
balloon catheters. AJR 1978; 131 : 651 -655
16. Kerber CWo Catheter therapy: fluoroscopic monitoring of deli
b-erate embolic occlusion. Radiology 1977; 125: 538-540
17. Bank WO, Kerber CWo Gelfoam embolization: a simplified
technique. AJR 1979; 132: 299-301
18. Kerber CW, Bank WO, Horton JA. Polyvinyl alcohol foam:
prepackaged emboli for therapeutic embolization. AJR 1978;
1 30: 1 193-11 94
19. Berenstein A, Kerber CW, Edwards JH, Bank WO, Kricheff II,
Cromwell LD. Complications of therapeutic transarterial em
-bolization: cooperative study. Presented at annual meeting of
the American Society of Neuroradiology, Toronto, May 1979 20. Pamdyia SK, Megpal RD, Desai AP, Purrhit AV. Death following
external carotid artery embolization for a functioning glomus jugulary chemodectoma. J Neurosurg 1978; 48: 1 030-1 034 21. Ahn HS, Kerber CW, Deeb ZL. Stroke during therapeutic
embolization via external carotid to intracerebral anastamoses.
Presented at the annual meeting of the American Society of