Patch Testing in Children, Adults, and the
Elderly: Influence of Age and Sex on
Sensitization Patterns
Stefan Wo¨hrl, M.D., M.S.,
*
Wolfgang Hemmer, Ph.D.,
*
Margarete Focke, Ph.D.,
*
Manfred Go¨tz, M.D.,
*
à
and Reinhart Jarisch, M.D.
*
*FAZ – Floridsdorf Allergy Center, Division of Immunology, Allergy, and Infectious Diseases (DIAID), Department of Dermatology, University of Vienna Medical School, andàDepartment of Pediatrics,
Wilhelminenspital, Vienna, Austria
Abstract:
Patch testing was done on 2776 consecutive patients (76.5% female) with a locally revised standard series of 34 contact allergens and the results analyzed for age- and gender-specific differences. At least one positive epicutaneous test reaction occurred in 48.9% of patients. Nickel (20.9%), eth-ylmercuric chloride (13.2%), thimerosal (11.8%), fragrance mix (9.3%), metallic mercury (8.9%), palladium (5.8%), balsam of Peru (3.8%), copper (3.7%), cobalt (3.3%), and chromium (2.3%) were the 10 most important sensitizers. The fol-lowing tested allergens with sensitization rates of more than 1% were not part of the usual standard series: ethylmercuric chloride, metallic mercury, copper, propolis (1.3%), propylene glycol (1.0%). Reactions to nickel, cobalt, and pal-ladium, but not to chromium, were significantly more abundant in females (p < 0.002, chi-squared test). The overall sensitization rate was highest in children less than 10 years old (62%) and decreased steadily, to be lowest among patients more than 70 years old (34.9%). The rate of positive reactions to nickel and thimerosal decreased with age, while fragrance mix and metallic mercury stayed at the same level through all age groups.Patch testing is an important step in diagnosing contact allergy. Some common sensitizers (e.g., nickel, cobalt, chromium, or balsam of Peru [myroxylon Perei-rae])are of worldwide relevance (1–4)and are the basis for the standard series of the International Contact Dermatitis Research Group (ICDRG)(5). However, some contact allergens, such as thimerosal, are not equally important in all areas (6). Therefore standard series are locally modified (7).
Contact allergies depend on several parameters. The importance of age, sex, race (8), and occupation
(2)has been shown in many studies. Furthermore, geographic factors (9), atopic dermatitis (10), and even seasonal parameters (11)can influence skin reactivity.
We compiled a database from patch test results obtained with a locally revised standard series in 2766 consecutive children and adult patients. The tests were carried out over 3.75 years at our allergy clinic in Vienna, Austria, and were analyzed retrospectively with special reference to the relationship between age, sex, and indi-vidual sensitization patterns.
Address correspondence to Stefan Wo¨hrl, M.D., FAZ – Flor-idsdorf Allergy Center, Franz-Jonas-Platz 8/6, A-1210 Vienna, Austria, or e-mail: [email protected].
PATIENTS AND METHODS
Between September 1997 and December 2000 (1186 days), 2766 consecutive patients suspected of contact allergy were routinely patch tested at our outpatient allergy clinic in Vienna, Austria. The vast majority of patients presented with eczema (mainly face, hands, limbs, and trunk). Only about 5% of patients had pri-marily a putative oral allergy. The patch tests were done using the EPIcheck system, which consists of 8 cm·18 cm polyurethane tapes covered with 22 empty plastic chambers (Innovall Medica; Duisburg, Germany). All patients (2115 females with an average age of 40.05 ± 17.40 years [range 2–92 years]; 561 males with an average age of 38.32 ± 17.92 years [range 2–89 years])were tested with a locally revised standard series of 34 allergens (see Table 1). All allergens were purchased from Brial Allergen (Greven, Germany), except for the
fragrance mix (Hermal; Reinbek, Germany). Patches remained occluded for 72 hours and a single 72-hour reading was done 30 minutes after removing the patches, according to ICDRG criteria (12).
Data were processed using the Star Office 5.2 software package (Sun Microsystems). A chi-squared test was used for analysis of associations of the various allergens and the analysis of differing sensitization rates between both sexes. The significance level was set to be p < 0.01. For analysis of age-dependent differences, patients were subdivided into the following age groups: 1–10, 11–20, 21–30, 31–50, 51–70, >70 years.
RESULTS
In accordance with many previous studies (2,7,9,13), nickel, palladium, cobalt, chromium, thimerosal,
TABLE 1. ‘‘Hit List’’ of Contact Allergens in this Locally Revised Standard Series
Allergen Total (%)Female (%)Male (%)
Difference in sex distribution (chi-squared test)
N 2766 2115 651
Average age (years)39.6 40.1 38.3 Positive patch test to at least one allergen 48.9 52.3 37.9
1 Nickel sulfate 5% 20.9 24.9 7.8 p < 0.0001 2 Ethylmercuric chloride 0.05% 13.2 13.7 11.8 3 Thimerosal 0.05% 11.8 12.4 10.0 4 Fragrance mix 8% 9.3 9.6 8.1 5 Metallic mercury 0.5% 8.9 9.4 7.4 6 Palladium chloride 1% 5.8 6.9 2.3 p < 0.0001 7 Balsam of Peru (myroxylon Pereirae)25% 3.8 4.3 2.3 n.s. 8 Copper sulfate 2% 3.7 4.1 2.2 n.s. 9 Cobalt chloride 1% 3.3 3.9 1.4 p < 0.002 10 Potassium dichromate 0.5% 2.3 2.1 3.1 n. s. 11 Neomycin (sulfate)20% 1.6 1.6 1.4
12 Euxyl K400 0.5% 1.5 1.6 1.2 13 Propolis (bees glue)10% 1.3 1.3 1.1 14 Colophony (resin)20% 1.2 1.2 0.9 15 p-Phenylenediamine (PPD)1% 1.2 1.2 1.1 16 Propylene glycol 5% 1.0 0.9 1.4 17 Amalgam 5% 0.9 0.8 1.4 18 Sesquiterpene lactone mix 0.1% 0.8 0.9 0.5 19 Epoxy resin 1.0% 0.7 0.8 0.6 20 Mercaptobenzothiazole 2.0% 0.6 0.5 0.9 21 2-Hydroxyethyl methacrylate (2-HEMA)2% 0.6 0.7 0.2 22 Isothiazolinone MI/MCI (Kathon CG)0.01%a 0.6 0.7 0.3 23 Ethylene glycol dimethacrylate (EGDMA)2% 0.5 0.4 0.8 24 Paraben mix 15% 0.5 0.5 0.3 25 PPD mix 0.1% 0.5 0.4 0.6 26 Formaldehyde 1.0%a 0.4 0.5 0.3 27 Diphenylguanidine 1% 0.4 0.2 0.9 28 Tetramethylthiuram disulfide (TMTD)0.25% 0.4 0.4 0.5 29 4-Hexylresorcin 0.25% 0.4 0.4 0.3 30 Benzocaine 5.0% 0.4 0.4 0.3 31 Phenylmercuric nitrate 0.01% 0.3 0.3 — 32 Panthenol 5% 0.2 0.1 0.6 33 Ammoniumtetrachloroplatinate (platinum)0.25% 0.2 0.2 0.2 34 Zinc-diethyldithiocarbamate 1% 0.1 0.1 —
Positive reactions to nickel, palladium, and cobalt were significantly more common in females than in males. All samples were tested in petrolatum at the concentrations indicated.
a
fragrance mix, and balsam of Peru (myroxylon Pereirae) were among the top 10 contact allergens (Table 1). Sixteen of the 34 tested contact allergens exceeded the critical incidence of 1%. Many of these are not found in the standard patch test series (2,5,7,9): ethylmercuric chloride 13.2%, metallic mercury 8.9%, copper sulfate 3.7%, propolis (bees glue)1.3%, and propylene glycol 1.0%.
Age and Sensitization Rates
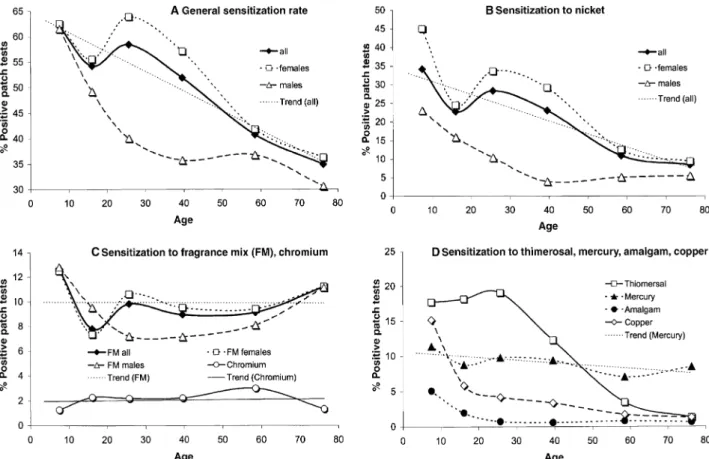
The overall incidence of patch test reactivity was highest in children up to 10 years of age (62.0%)and steadily decreased to be lowest among patients more than 70 years of age (34.9%)(Fig. 1A). Hypersensitivity to the metals nickel, cobalt, palladium, and copper steadily decreased with age (Fig. 1B,D; Table 2). There was a high proportion of young children sensitized to mercury (11.4%)and copper (15.2%), both major compounds of dental amalgams (5.1%; Fig. 1D). High sensitization rates were also observed for other allergens (Table 2). In contrast to the other metal allergens, sensitization to mercury and chromium was at around the same level among all age groups (Fig. 1C,D). Sensitization to
thimerosal, presumably resulting from thimerosal-containing vaccines, depended on age and began to decline at ages greater than 30 years (Fig. 1D). Sensiti-zation to fragrance mix was highest among children, decreased in adults, and increased again among elderly patients (Fig. 1C; Table 2). On average, sensitization to fragrance mix and colophony remained at the same level through all age groups, whereas balsam of Peru, another screening substance for fragrance allergy (14), showed an increase from 1.9% in the 10- to 20-year-old age group to 5.3% in patients more than 70 years old (Table 2). Fragrances, preservatives, and metals were the most prominent allergens in the elderly (Table 2).
Sex-Specific Allergens
The overall incidence of patch test reactivity was higher in female patients (Fig. 1A; Table 1)and this was mainly due to the high frequency of nickel hypersensi-tivity (Fig. 1B). A significant difference in the frequency of sensitization between the sexes was found with the metals nickel, cobalt, and palladium, but not with chro-mium. Of interest is that sensitization to nickel (Fig. 1B) and fragrance mix (Fig. 1C)did not differ significantly
Figure 1. Age and sex dependence of positive reactions to various contact allergens in the standard patch test series. X values represent the average age of the referring age group (see Patients and methods).
between the sexes in the youngest and oldest patients. In males, sensitization to both allergens decreased steadily until it reached a bottom in the 30- to 50-year-old age group. In females there were two peaks, one in the youngest patients and another one in patients 20–30 years old (Fig. 1B). Sensitization to fragrance mix showed another peak in patients more than 70 years old in both sexes (Fig. 1C).
DISCUSSION
The results observed in this study population largely correspond to Middle European data published previ-ously (2,7,9)although some less important standard al-lergens have been found at comparatively low frequencies. This may be due to several factors, including the predominance of females in the study population, the performance of a single 72 hour reading potentially leading to underreporting of ‘‘late-onset’’ allergens, as well as a less restrictive indication for patch testing patients as compared with other investigations. The high frequency of sensitization to thimerosal in Austria has been described previously (6). The significantly higher rate of sensitization to nickel, cobalt, and palladium in females is an observation well established in the medical literature (1). However, we did not observe a significantly higher rate of sensitization to chromium in males, as published many times before (7,15). The strong skew toward females in this analysis was simply due to the more frequent referral of female patients to our outpa-tient clinic. As no patch test results have been omitted from the analysis, the observed gender-specific differ-ences do not result from selection bias.
Positive patch test reactions decreased with age (Fig. 1A). This observation confirms the findings of Wantke et al (16), but contradicts data from Goh (8),
who found positive reactions preferentially in elderly subjects, and also contradicts data from Pevny et al (17), who found a generally low rate of sensitization in chil-dren. In recent years there has been an increasing number of reports describing a high rate of sensitization to nickel, mercurials (thimerosal, ethylmercuric chloride, metallic mercury), and fragrances in young children (16,18–20). Shah et al (21)found positive patch tests in children to be specific and of clinical relevance. The uncertain clinical relevance of a positive patch test reaction in the children included in this study is somehow limiting. However, the primary focus of our study was to show that contact sensitization is not uncommon in young children. Even though many of these reactions fail to be clinically rele-vant, our findings might indicate a very high suscepti-bility to sensitization by common contact sensitizers early in life. This appears to be particularly obvious in the study of nickel hypersensitivity, showing a peak in young girls as well as in young boys. However, there was a second peak at around 30 years in females which might only reflect the gender-specific use of costume jewelry, an effect also observed by others (16,22,23).
In this study, copper was found to be an important allergen, especially in young children (Table 2). Reac-tions to copper were shown to be specific and to originate from nickel-copper cross-reactive T-cell clones (24). The major constituents of amalgam alloys are mercury, silver, copper, tin, and in some cases, zinc (25). The high number of young children sensitized to metallic mercury, copper, or amalgam may be explained by the use of amalgam dentures in young children (Fig. 1D). The decrease in sensitization to amalgam with age paralleled the decrease in sensitization to copper, and it might be speculated that copper is the most relevant allergen in dental amalgams because patch test reactions to the other components, with the exception of mercury, are very rare (26).
TABLE 2. ‘‘Top 10 List’’ of Contact Allergens in Children, Young Adults, and the Elderly
1–10 years (average 7.5 years)21–30 years (average 25.7 years) >70 years (average 76.2 years)
n(F/M)79 (40/39) 550 (425/125) 152 (116/36) Positive percentage (n)62.0 (49) 58.4 (271) 34.9 (53)
Positive % (n)Positive % (n)Positive % (n) 1 Nickel sulfate 34.2 (27)Nickel sulfate 28.4 (156) Fragrance mix 11.2 (17) 2 Ethylmercury 25.3 (20)Thimerosal 19.1 (105) Metallic mercury 8.6 (13) 3 Thimerosal 17.7 (14)Ethylmercury 17.8 (98) Nickel sulfate 8.6 (13) 4 Copper sulfate 15.2 (12)Metallic mercury 9.8 (54) Balsam of Peru 5.3 (8) 5 Fragrance mix 12.7 (10)Fragrance mix 9.8 (54) Ethylmercury 3.3 (5) 6 Metallic mercury 11.4 (9)Palladium chloride 7.3 (40) Paraben mix 2.0 (3) 7 Palladium chloride 11.4 (9)Copper sulfate 4.2 (23) Cobalt chloride 2.0 (3) 8 Cobalt chloride 6.3 (5)Cobalt chloride 3.8 (21) Euxyl K400 2.0 (3) 9 Amalgam 5.1 (4)Balsam of Peru 3.6 (20) Colophony 1.3 (2) 10 Balsam of Peru 3.8 (3)Potassium dichromate 2.2 (12) Copper sulfatea 1.3 (2) Reactions to copper and amalgam were much more common in children than in adults. Nickel and thimerosal are of less importance in elderly subjects.
a
Fragrances, often regarded as typical allergens in el-derly people, were important allergens in all age groups and in both sexes. Obviously, young children become sensitized to fragrances at a very early age.
CONCLUSION
Metals, mercurials, and fragrances were the most im-portant contact sensitizers in this study from Vienna, Austria. Reactions to ethylmercuric chloride, thimerosal, copper, propolis, and propylene glycol—not regularly tested in standard series—were observed in more than 1% of patients. The incidence of sensitization was highest among young children and steadily decreased along with age. Fragrances and metallic mercury were important sensitizers in all age groups. Reactions to nickel, cobalt, and palladium, but not to chromium, were significantly more common in females.
REFERENCES
1. Albert MR, Gonzalez S, Gonzalez E. Patch testing reac-tions to a standard series in 608 patients tested from 1990 to 1997 at Massachusetts General Hospital. Am J Contact Dermatitis 1990;9:207–211.
2. Brasch J, Geier J, Schnuch A. Differenzierte Kontaktal-lergenlisten dienen der Qualita¨tsverbesserung. Hautarzt 1998;49:184–191.
3. Singhal V, Reddy BS. Common contact sensitizers in Delhi. J Dermatol 2000;27:440–445.
4. Greig JE, Carson CF, Stuckey MS, Riley TV. Prevalence of delayed hypersensitivity to the European standard series in a self-selected population. Australas J Dermatol 2000; 41:86–89.
5. De Groot AC, Frosch PJ. Patch test concentration and vehicles for testing contact allergens. In: Rycroft RJG, Menne´ T, Frosch PJ, Benezra C, eds. Textbook of contact dermatitis. Berlin: Springer, 1992:795–805.
6. Aberer W, Kra¨nke B. Thiomersal is a frequent sensitizer but is not in the standard series. Contact Dermatitis 1995;32:367–368.
7. Kra¨nke B, Binder M, Derhaschnig J, et al. Epikutante-stung mit der Standardreihe ‘‘O¨sterreich’’ – testepidemio-logische Kenngro¨ßen und Ergebnisse. Wien Klin Wochenschr 1995;107:323–330.
8. Goh CL. Prevalence of contact allergy by sex, race and age. Contact Dermatitis 1986;14:237–240.
9. Schnuch A, Geier J, Uter W, et al. National rates and regional differences in sensitization to allergens of the standard series. Population-adjusted frequencies of sensi-tization (PAFS)in 40,000 patients from a multicenter study (IVDK). Contact Dermatitis 1997;37:200–209.
10. Manzini BM, Ferdani G, Simonetti V, Domini M, Seide-nari S. Contact sensitization in children. Pediatr Dermatol 1998;15:12–17.
11. Basketter DA, Griffiths HA, Wang XM, Wilhelm KP, McFadden JM. Individual, ethnic and seasonal variability in irritant susceptibility of skin: the implication for a pre-dictive human patch test. Contact Dermatitis 1996;35:208– 213.
12. Wahlberg JE. Patch testing. In: Rycroft RJG, Menne´ T, Frosch PJ, Benezra C, eds. Textbook of contact dermatitis. Berlin: Springer, 1992:239–268.
13. Aberer W, Reiter E. Kontaktekzem und Epikutantest – Allergenverteilung und Wandel des Spektrums in Wien. Wien Klin Wochenschr 1991;103:263–267.
14. Wo¨hrl S, Hemmer W, Focke M, Go¨tz M, Jarisch R. The significance of fragrance-mix, balsam of Peru, colophony and propolis as screening tools in the detection of fragrance allergy. Br J Dermatol 2001;145:268–273.
15. Walton S, Nayagam AT, Keczkes K. Age and sex inci-dence of allergic contact dermatitis. Contact Dermatitis 1986;15:136–139.
16. Wantke F, Hemmer W, Jarisch R, Go¨tz M. Patch test reactions in children, adults and the elderly. A comparative study in patients with suspected allergic contact dermatitis. Contact Dermatitis 1996;34:316–319.
17. Pevny I, Brennenstuhl M, Razinskas G. Patch testing in children. (I)Collective test results; skin testability in chil-dren. Contact Dermatitis 1984;11:201–206.
18. Brasch J, Geier J. Patch test results in schoolchildren. Results from the Information Network of Departments of Dermatology (IVDK)and the German Contact Dermatitis Research Group (DKG). Contact Dermatitis 1997;37: 286–293.
19. Romaguera C, Vilaplana J. Contact dermatitis in children: 6 years experience (1992–1997). Contact Dermatitis 1998; 39:277–280.
20. Bruckner AL, Weston WL, Morelli JG. Does sensitization to contact allergens begin in infancy? Pediatrics 2000; 105:e3.
21. Shah M, Lewis FM, Gawkrodger DJ. Patch testing in children and adolescents: five years’ experience and follow-up. J Am Acad Dermatol 1997;37:964–968.
22. Veien NK, Hattel T, Justesen O, Nørholm A. Why do young girls become nickel sensitive? Contact Dermatitis 1986;15:306–307.
23. Gonc¸alo S, Gonc¸alo M, Azenha A, et al. Allergic contact dermatitis in children. Contact Dermatitis 1992;26:112– 115.
24. Wo¨hrl S, Hemmer W, Focke M, Go¨tz M, Jarisch R. Copper allergy revisited. J Am Acad Dermatol 2001;45: 863–870.
25. Guy RH, Hosty´nek JJ, Hinz RS, Lorence CR. Metals and the skin—topical effects and systemic absorption. New York: Marcel Dekker, 1999:204.
26. Wo¨hrl S, Hemmer W, Focke M, Go¨tz M, Jarisch R. Oral symptoms due to zinc as a minor component in dental amalgam. Contact Dermatitis 2001;44:252–253.