What Do Collaborative
Improvement Projects Do?
Experience from Seven Countries
Performance Improvement
Tim Wilson, MD
Donald M Berwick, MD, MPP
Paul D. Cleary, PhD
T
he chasm between what is possible and what is routinely achieved in health care has never appeared wider.1 In the search for a remedy,health care organizations are increasingly using formal quality improvement methods2–4 that often involve
groups working together on specific pressing issues.5,6
Improvement collaboratives were first developed in the United States, but models have also been developed in Australia, France, the Netherlands, Norway, Sweden, and the United Kingdom (UK). The reform plan for the National Health Service (NHS) in the UK calls for the establishment of collaboratives on a wide variety of top-ics nationally.7 Many of the large collaboratives in the
world, and all the ones studied in this article, are derived from the Institute for Healthcare Improvement (IHI) Breakthrough Series (BTS) model of quality improve-ment collaboratives.8,9In the IHI model (Table 1, p 86),
organizations are invited to work collaboratively on spe-cific improvement topics.
To our knowledge, there have been no studies that have described how variations in different aspects of collaboratives affect their effectiveness or even what the most salient dimensions of variation are. In essence, col-laboratives are “black boxes.” What makes evaluating these activities especially difficult is that what is inside the boxvaries considerably.
In this study, we first developed a framework for describing collaboratives based on the IHI model. We then interviewed collaborative leaders to ask them what they think the critical components of collaboratives are and used that information to refine our framework. In this article, we examine the components identified in terms of theories of organizational change10,11 and
Background:Health care organizations are in-creas-ingly adopting multiorganizational collaborative approaches to quality improvement. Collaboratives have been conducted in many countries. There are large variations in the way collaboratives are structured and run, but there is no widely accepted framework for describing the components of collaboratives. Thus, it is difficult to study which approaches are most effective.
Method: The authors conducted semistructured interviews with 15 leaders of collaboratives to ascer-tain the common components of collaboratives and identify variations in the ways these components are implemented.
Results:The study identified seven features of collab-oratives that the leaders interviewed thought were criti-cal determinants of how effective the collaboratives were: sponsorship, topic, ideas for improvements, partic-ipants, senior leadership support, preliminary work and learning, and strategies for learning about and making improvements. For example, every interviewee mentioned that having participants collect data, perform audit work, or analyze the system they were in before the collaboration started was important to understanding their organization and the nature of the problems they had and to developing baseline data for later comparison. The authors describe variations in how these features have been implemented and possible functions of these features.
Conclusion:Systematically studying the impact of vari-ations in the seven key features of collaboratives could yield important information about their role and impact.
diffusion of innovation12 to identify the potential
func-tions of these features.
Research Methods
Survey
To develop an initial framework, we reviewed the available literature describing the IHI model of collaborative improvement and developed a preliminary list of compo-nents. We interviewed four colleagues at IHI responsible for developing and running collaboratives and asked them to comment on our list. We then developed a semistruc-tured interview (Table 2, p 87) that asked respondents about each component, whether they felt it was important, and how they had implemented it. The interview also asked whether there were other components of collabora-tives that had had an important impacts on their success.
Sample
We asked IHI staff to identify a convenience sample of people in different countries who had experience leading
collaboratives based on the IHI model for at least a year and who had tried significant variations of the model typi-cally used in the United States. We identified 15 potential respondents in seven countries: Australia, France, the Netherlands, Norway, Sweden, the United Kingdom, and the United States. We selected many respondents from outside the United States because we thought there would be more variability in how those collaboratives were run.
Interview
The experts were contacted by the lead author [T.W.] by telephone in September–October 2000. Every identi-fied respondent was interviewed.
Analysis
We reviewed interviews as they were completed and used an informal consensus process to determine the changes to the framework that were needed. We collec-tively reviewed the explanations of the leaders about why different components were important to the suc-cess of their collaborative and used that information, as well as published theory, to develop explanations of the potential functions of each of the components identified.
Results: The Seven Key Components
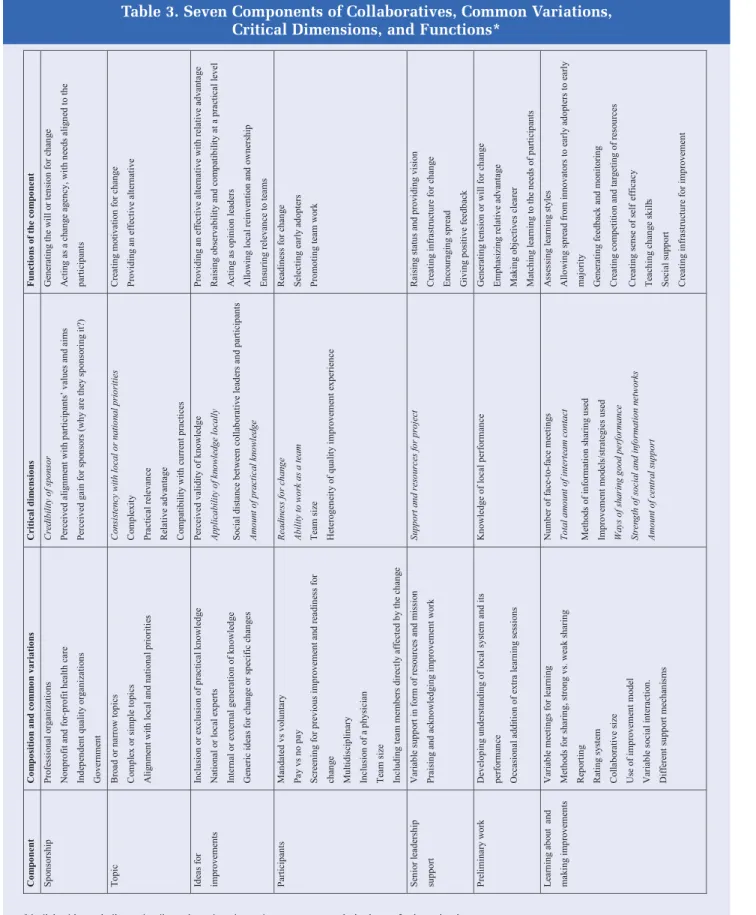
Interviewees confirmed that collaboratives had seven components that they thought were important determi-nants of success: sponsorship, topic, ideas for improve-ment, participants, senior leadership support, preliminary work, and strategies for learning about and making improvements (Table 3, p 88). There were substantial variations in how these components were implemented.
Sponsorship
All respondents thought that sponsorship is an impor-tant determinant of the success of a collaborative. There was tremendous variability, however, in sponsors (Table 3), including government and independent professional, membership, and independent quality and health care organizations. Respondents suggested that in many cases sponsorship improved an effort’s credibility or per-ceived importance (for example, professional organiza-tions). Conversely, in one case of government sponsor-ship, the interviewee perceived that sponsorship gener-ated cynicism about the aims of the collaborative. 1. Sponsoring organization identifies topics where a
sig-nificant gap exists between best and typical practice. 2. The Institute for Healthcare Improvement (IHI) then assembles an expert panel.
3. Expert panel prepares a package of ideas for closing the gap.
4. IHI recruits participating teams to be part of the collaborative.
5. Participants engage in prework: forming local improvement team, develop of goals and measure-ments, and characterizing current practice.
6. During a collaborative’s life, usually 6 to 12 months, teams from participating organizations attend three learning sessions in which they learn about ideas for better practice and improvement methods that they implement between sessions.
7. Between learning sessions, teams share experiences and maintain contact through such mechanisms as conference calls and Internet e-mail listservs while submitting progress reports.
8. The lessons learned are spread through a national meeting (congress) and reports.
Table 1. Steps in the Breakthrough Series Collaborative Model
Topic
All leaders interviewed said that the choice of topic was a critical determinant of how successful a collabo-rative would be, but opinions varied on the characteris-tics of an ideal topic. Broad topics were felt to be more attractive to external funding sources (as was found in the case of the French elderly care collaborative), and three respondents claimed that broader topics led to the most innovation. Some thought that highly specific top-ics might be less relevant for local organizations with dif-ferent priorities (for example, a Norwegian intensive care unit [ICU] collaborative had issues that were inap-propriate for some participating hospitals) but were more conducive to rapid improvement.
Leaders thought that collaboratives that focused on complex or technically unfamiliar topics were less likely than others to be successful or attractive to participants. For instance, in the UK, primary care collaborative par-ticipants were initially more attracted to work on the simpler and more familiar topic of improving cardiovas-cular disease care than access or capacity demand man-agement until later in the collaborative process, when they began working on all the topics.
In some countries the topic became a national priority during the collaborative, which appeared to motivate participants. For example, in the course of a UK primary care collaborative, national standards for access7and coronary disease13were introduced. In
con-trast, Swedish leaders proposed but then deferred a cesarean section collaborative because it was felt that the topic was not yet viewed by organizations as impor-tant enough.
Ideas for Improvement
Most collaboratives used outside expert groups (national or local, as appropriate) rather than partici-pants themselves to suggest improvements. Having an expert panel to legitimize the knowledge was thought to be most likely to lead to adoption, especially when the knowledge was not yet in mainstream practice (for example, the use of clot busters for stroke). However, two interviewees mentioned that experts were occasion-ally too different from the participants for their advice to appear relevant.
Most, but not all, interviewees included experts in quality improvement and systems thinking in identifying knowledge to provide general concepts that allowed local changes for implementation (reinvention).
A few collaboratives allowed teams to generate their own knowledge. It was felt that this created commit-ment, although the interviewees thought that changes were less rapid than when knowledge was generated externally. Most interviewees thought having an expert with practical knowledge was crucial. One interviewee described how assembled “experts” did not understand ground-level issues, which stalled improvement.
Participants
A few of the interviewees agreed that it was important to select participants carefully, but there was great vari-ability in exactly how participants were selected. Some collaboratives were voluntary, whereas others were mandatory. A few interviewees described how participa-tion criteria were used to select participants with previ-ous experience in quality improvement, commitment to the collaborative and topic, and participation of a senior executive. The majority of collaboratives relied on volunteers and had no selection.
1. Sponsoring organization (including the financing system)
2. Topic selection
3. Identifying knowledge for improvement
4. Participating organizations (including local team formation)
5. Leadership
6. Mechanisms for learning and change
7. Mechanisms for sharing within the collaborative 8. Mechanisms for spread and dissemination 9. Sustainability
10. Judging the degree of success 11. National differences
12. Collaborative 13. General 14. Results
Table 2. Topics for Semistructured Interview for International Comparison of
Collaborative Improvement*
Table 3. Seven Components of Collaboratives, Common Variations, Critical Dimensions, and Functions*
One interviewee highlighted the need for a certain number of teams to participate in a collaborative, sug-gesting that very small collaboratives had problems with identifying best practice and engaging in constructive criticism. Many interviewees described how they identi-fied good and poor performers and encouraged them to work together. Involvement of governmental organiza-tions occasionally led to some reluctance to disclose information.
In terms of funding strategies, in some collaboratives participants covered all costs and paid fees. Other collab-oratives required no fees and provided extra resources. In some settings, such as the NHS, it was felt that it would be countercultural to ask participants to pay, whereas many other interviewees, especially those in the United States, expressed the opinion that payment was more likely to lead to commitment. Interviewees who had experience with both systems discerned little difference.
Teams always included clinicians, and all but one col-laborative team included a physician. Two interviewees emphasized how many changes involve physician behavior, and how spread was dependent on communi-cations from clinician to clinician, especially among physicians. Every collaborative had multidisciplinary teams. Managers were less often included. The inclusion of a quality improvement officer or project manager varied. All interviewees felt that it was important to include personnel (clinical and nonclinical) who were to be directly affected by the changes.
Teams attending learning sessions were usually com-posed of three or four people but ranged from two to eight. Many teams had additional members who partici-pated in the improvement process in their organization but did not attend the collaborative.
Senior Leadership Support
Most interviewees emphasized that support from senior organizational leaders (for example, chief execu-tive officer of a hospital or health system, head of a department) was crucial. For example, in Sweden some teams withdrew from a collaborative because of weak support from senior leadership. Other teams that were thinking of dropping out stayed only after receiving help from their organizations’ leaders. One exception to this observation was when the teams worked
independently, (in relatively self-contained units such as a neonatal ICU, although in that case senior leaders were kept informed.
Doing Preliminary Work
Every interviewee mentioned that having participants collect data, perform audit work, or analyze the system they were in before the collaboration started was impor-tant to understanding their organization and the nature of the problems they had and to developing baseline data for later comparison.
Some leaders added early sessions to teach partici-pants about setting aims and quality improvement tech-niques. This varied from residential courses for selected members of the teams to video links. In the Netherlands, testing was covered in the preliminary work, whereas the Vermont Oxford Network (U.S.) teaches improve-ment methods and encourages teams to complete some improvement cycles before the first learning session.
Strategies for Learning About and Making
Improvements
All interviewees thought that teaching collaborative participants about quality improvement theory and techniques was extremely important. Each used the improvement model developed by Langley and colleagues. This model encourages teams to assess the aims, measurements, and changes needed for improvement and then work on rapid cycles of change and evaluation.14
Every interviewee thought that having participants share improvement strategies facilitated improvement. In only a few collaboratives was this a problem, with one country having cultural barriers to open exchange. Those interviewed thought that less sharing resulted in slower improvement. Although all respondents empha-sized the importance of having participants share expe-riences, showcasing high-achieving teams was not felt to be appropriate in all countries (especially in the UK, where the term was altered from showcasingto how we
solved a problem). Many interviewees stated that they
felt competition was important because the collabora-tive fulfilled three important characteristics for competi-tion: Everyone can win (or make an improvement), the rules are fair (success is judged on the improvement
from where you started), and the teams themselves are the major determinants of success.15
The meetings ranged in number from two to seven and in length from half a day to 3 days. Most collaboratives had three meetings of 2 days each. Shorter sessions did not seem any less successful than larger ones. Several interviewees mentioned that these meetings needed care-ful planning and clear agendas and objectives. There were large variations in the balance between plenary and work-shop sessions. Teams are likely to have different learning needs and styles, so collaboratives need to understand these to adapt the balance of the activities within the meetings to meet varying needs and preferences.16
All interviewees mentioned the element of social exchange within and between teams as being very important. It seemed to them that such exchange helped teams establish peer support and feel that they were “not in this alone.” Some collaborative organizers stimulate social interaction through meals, parties, and time out and encourage mixing. Three interviewees described how participants themselves arranged extra meetings to continue social interaction.
Central support from the collaborative organizers varied considerably from one part-time person for the entire collaborative to one full-time project officer per team; most collaboratives provided part-time support for every three or four teams. A few interviewees stated that having strong central project management or quality improvement support drove projects more rapidly. A few felt, however, that this led to dependency. A minority of interviewees described a very tight level of centralized collaborative control, while others had a much looser style. The leaders interviewed did not think this had a discernible effect. Two interviewees said they thought that it was important to drive teams to make improvements while maintaining friendly support: “a smile with intent.”
All the collaborative improvement projects used for-mal reporting. Interviewees felt that reporting created a discipline not otherwise present, allowed teams to judge their own progress, and helped the collaborative leaders assess progress and target extra support. Half of the interviewees used validated self-administered rating scales, generally Likert scales of 1 through 517to assess
progress toward improvement.
Discussion
Although research has been reported on quality improve-ment in health care,18–20to our knowledge there has been
nothing published on how collaborative projects func-tion. Improvement collaboratives have evolved out of several disciplines, and their structure and theoretical foundations have not always been explicit. Most make use of modern quality improvement theory, which emphasizes that changes in performance require changes in systems.21
The framework that emerged from our interviews should allow researchers to more accurately describe and test variations in the way collaboratives are imple-mented. Both the comments of those interviewed and the literature on organizational change provide insights into the possible functions and importance of these dif-ferent components. We now discuss which of the seven features of collaboratives might affect degree of involve-ment of participants, likelihood of participants making substantial changes in their organizations, how well teams work together, and rate of change.
What Features Affect Whether Participants Become
Involved?
Every leader interviewed agreed that sponsorship was a critical component of his or her collaborative, although there was great variation in the types of spon-sors selected. In Rogers’s framework,12 one could
describe the sponsor as the agency that wishes to bring about change, or the “change agency,” and the collabora-tive itself as an agent that brings about change (“change agent”). However, a change agent that is perceived as being oriented to the change agency’s—as opposed to the participant’s—needs, can be ineffective. This might explain why government sponsorship might be counter-productive.
Thus, we suggest that one of the important character-istics of sponsorship that needs to be evaluated is the extent to which participants respect and agree with the priorities of the sponsor.
According to diffusion theories, selecting a topic of sufficient priority is important to generate motivation for change. Theoretically, topics that are simple and com-patible with organizational needs and the priorities of external funding sources should be the most successful.
Leaders tended to think that broad topics were more likely to engage a broader group of participants. Thus, the perceived salience and complexity of the collabora-tive topic should be important characteristics to be con-sidered when comparing collaboratives, but the best approach to topic selection is not apparent.
What Features of Collaboratives Might Affect
Whether Participants Make Changes?
Experts, and in particular the collaborative chair, act as opinion leaders—people providing advice and infor-mation about change. Opinion leaders, who are usually part of the system in which the change is going to occur (for example, a practicing clinician in the same speciali-ty), should not be too innovative but should have a perceived high level of technical competence.
Ideas that are most likely to be adopted have a rela-tive advantage for participants and are compatible with local practices, and it is helpful if local reinvention is permitted. Furthermore, if the changes are of practical relevance to daily work, learning research suggests that adoption is more likely.12
It is generally accepted that both individuals and organizations22–25 must be ready for change before
attempts are made to help them change. Selection and requiring payment are ways of assessing such readiness. Furthermore, many interviewees were looking for early adopters of innovation in the anticipation that diffusion would occur naturally from that group to others.12
What Features of Collaboratives Might Affect How
Well Teams Perform?
Heterogeneous membership of improvement groups is important,15as is involving physicians,2while learning
in teams that work together is more likely to be effec-tive.26Theories about effective teams suggest that five to
seven members are most likely to bring about change.15
Although most collaborative teams had four members attending events, more people participated in the improvement projects at the home organizations.15
Quality problems often persist because no single person or group is clearly responsible for improving the system.27 Early improvement work showed that senior
leaders were necessary to provide a mission for a proj-ect.2We suspect that senior-level leaders support teams
in two ways—first, by facilitating teams and overcoming barriers to change (including suspending rules) and, sec-ond, by allowing and encouraging spread of the improve-ments through the whole organization. Adult learning theories suggest that an issue with higher status is likely to receive greater attention.16
What Features of Collaboratives Might Affect the
Speed of Improvement?
Work before meetings probably increased tension or motivation for change by reemphasizing the relative advantage of the proposed changes over current practice. The modification of the original breakthrough model to add extra learning sessions shows that some collaboratives have recognized that according to adult learning theories, matching the educational needs of the learner is more successful than using a set curriculum.28
Alemi and colleagues29studied improvement activities
in several health care organizations and found that results were most quickly achieved when the focus was on testing changes rather than on detailed analysis of the current practice. Thus the focus on rapid testing of small changes is probably a critical component of the models used to teach participants how to make and evaluate changes.
Diffusion theory suggests that ideas are most likely to be adopted from the same professional group. The Breakthrough Series encourages peer-to-peer spread from innovators to early adopters.12
Social support, often emphasized in the collabora-tives, is important for change, as is the development of social networks for the diffusion of ideas.10
The central support and reporting acted as both feed-back mechanisms30 and mechanisms for maintaining
the tension for change.10It has been suggested that three
factors—which are apparently present in collabora-tives—need to be in place before successful change can take place: curiosity, forgiveness (allowing for mistakes and encouraging teams to learn from them), and trust.15
Limitations
This study was limited in several ways. First, because we used IHI personnel to help identify study sites, the col-laboratives we studied do not reflect the diversity of
approaches others have adopted. However, this model is the most commonly used worldwide. Furthermore, we may not have identified important variations in which even the IHI model has been implemented. Third, we had no way of assessing the effectiveness of the collabora-tives studied. Thus, although we asked respondents to assess what components of their collaboratives con-tributed to their successes or lack or success, we could use these judgments as indicators of salience. Even if the collaboratives were successful, it probably would be extremely difficult for leaders to know which compo-nents were important for success. Aspects other than those identified might have had an important influence. It is also possible that any achieved successes are due in part to a Hawthorne effect.31
This article does not and could not attempt to demon-strate how successful the collaborative demon-strategy is, either in itself or compared with other types of improvement activities. A number of major evaluations of collaborative improvement projects are currently under way in the United States to do this. The interviewees were enthusias-tic about the benefits of collaboratives, but they are not unbiased observers. An increasing number of research articles have reported on the potential benefits of collabo-ratives,32–35although it would be difficult to generalize the
results to collaboratives conducted in different ways.
Conclusion
The interviews suggest that there tend to be a set of well-defined features of collaboratives which are often imple-mented in different ways. Making explicit, for the first time, how these components are implemented in differ-ent collaborative will facilitate the testing of hypotheses
about specific features of collaboratives (Table 3). We encourage other researchers and quality improvement experts to join this continuing international dialogue36to
accelerate development and investigation of collabora-tive improvement.
Postscript
Improvement collaboratives are being used worldwide with considerable financial, political, and personal investment in the process. Since the interviews were conducted, collaboratives have evolved; the latest variations include providing additional days at the start of a collaborative (“learning session zero”), increasing attention to teamwork, bringing together teams and organizations from diverse agencies (for example, health, social, and voluntary sectors), including users and carers in teams, and utilizing learning set techniques for participant development.
This work was supported by The Commonwealth Fund, New York. The views presented here are those of the authors and not necessarily those of The Commonwealth Fund or its directors, officers, or staff. Drs Wilson and Berwick have received funds from running and design-ing collaborative improvement projects. Dr Berwick is the CEO and President of the Institute for Healthcare Improvement, which developed the model evaluated. Dr Cleary has received separate funding for the evaluation of a collaborative improvement project. The authors acknowledge Paul Plsek, who helped with early versions of this article.
J
Tim Wilson, MD, is Director, RCGP Quality Unit, Royal College of General Practitioners, London, United Kingdom.
Donald M. Berwick, MD, MPP, is CEO and President, Institute for Healthcare Improvement, Boston. Paul D. Cleary, PhD,is Professor, Department of Healthcare Policy, Harvard Medical School, Boston. Please address correspon-dence to Tim Wilson, MD, [email protected].
1. Chassin MR, Galvin RW: The urgent need to improve health care qual-ity. JAMA280:1000–1005, 1998.
2. Berwick DM, Godfrey AB, Rossener J: Curing Health Care: New Strategies for Quality Improvement.San Francisco: Jossey-Bass, 1990. 3. Caldwell C (ed): The Handbook for Managing Change in Healthcare.Milwaukee: ASQ Press, 1998.
4. Plsek PE: Quality improvement methods in clinical medicine.
Pediatrics103:203–214, 1999.
5. Berwick DM: Eleven worthy aims for clinical leadership of health system reform. JAMA272:797–802, 1994.
6. Plsek PE: Collaborating across organizational boundaries to improve the quality of care. Am J Infect Control25(2):85–95, 1997.
7. Department of Health: The NHS Plan: A Plan for Investment, A Plan for Reform.Document #Cm 4818-I. London: Her Majesty’s Stationery Office, Jul 2000.
8. Kilo CM: A framework for collaborative improvement: Lessons learned from the Institute for Healthcare Improve-ment’s Breakthrough Series. Qual Manage Healthc 6(4):1–13, 1998.
9. Kilo CM: Improving care through collaboration. Pediatrics103(1 Suppl E):384–393, 1999.
10. Gustafson D, Cats-Baril WL, Alemi F: Systems to Support Health Policy Analysis: Theory, Models, and Uses. Chicago: Health Administration Press, 1992.
11. Nolan TW: Understanding medical systems. Ann Intern Med
128:293–298, 1998.
12. Rogers EM: Diffusion of Innovations 4th ed. New York: The Free Press, 1995.
13. Department of Health: National Service Framework for Coronary Heart Disease Modern Standards & Service Models.London: Her Majesty’s Stationery Office, 2000
14. Langley GJ, et al: The Improvement Guide: A Practical Approach to Enhancing Organizational Performance.San Francisco: Jossey-Bass, 1996.
15. Handy C: Understanding Organisations 4th ed. London: Penguin Books, 1999.
16. Honey P, Mumford A: The Manual of Learning Styles.Maidenhead, UK: Peter Honey Publications, 1992.
17. Johnson WL, Dixon PN: Response alternatives in Likert scaling.
Educational & Psychological Measurement44:563–567, 1984. 18. Shortell S, Bennett C, Byck G: Assessing the impact of continuous quality improvement on clinical practice: What it will take to accelerate progress. Milbank Q76:593–624, 1998.
19. Øvretveit J, Gustafson D: Evaluation of quality improvement pro-grammes. Qual Saf Health Care11(3):270–275, 2002.
20. Alemi F, Safaie FK, Neuhauser D: A survey of 92 quality improve-ment projects. Jt Comm J Qual Improv27:619–632, 2001.
21. Juran JM (ed): A History of Managing for Quality: The Evolution, Trends, and Future Directions of Managing for Quality. New York:McGraw-Hill, 1995.
22. DiClemente CC, Prochaska JO: Self-change and therapy change of smoking behavior: A comparison of processes of change of cessation and maintenance. Addict Behav7:133–142, 1982.
23. Argyris C: Overcoming Organizational Defenses.Boston: Allyn & Bacon, 1990.
24. Beckhard R, Harris RT: Organizational Transitions: Managing Complex Change 2nd ed. Reading, MA: Addison-Wesley, 1987. 25. Bridges W: The Character of Organizations: Using Personality
Type in Organizational Development. New York: Davis-Black
Publishing, 2000.
26. Grol R, Lawrence M: Quality Improvement and Peer Review.
Oxford General Practice Series 32. Oxford, UK: Oxford University Press: 32, 1995.
27. Juran JM: Managerial Breakthrough.New York: McGraw-Hill, 1964.
28. Knowles M: The Adult Learner: A Neglected Species 4th ed. Houston: Gulf Publishing, 1990.
29. Alemi F, et al: Rapid improvement teams. Jt Comm J Qual Improv
24:119-129, 1998.
30. Kolb DA: Experiential Learning: Experience as the Source of Learning and Development.Englewood Cliffs, NJ: Prentice Hall, 1984. 31. Mayo E: The Human Problems of an Industrial Civilization.New York: Macmillan, 1933.
32. Horbar J, et al: Collaborative quality improvement for neonatal intensive care. Pediatrics107:14–22, 2001.
33. Flamm B, Berwick D, Kabcenell A: Reducing cesarean section rates safely: Lessons from a “breakthrough series” collaborative. Birth
25:117–124, 1998.
34. Leape L, et al: Reducing adverse drug events: Lessons from a break-through series collaborative. Jt Comm J Qual Improv26:321–331, 2000. 35. Svensson C: Breakthrough: Reducing Queues and Waiting Times to, Through, and Within Healthcare: A Report of a Second Breakthrough Project. Stockholm: Swedish Federation of County Councils, 2000.
36. Øvretveit J: How to run an effective improvement collaborative. Int J Health Care Qual Assur15:192–196, 2002.