THE EFFECTS OF USING ORAL HIV SELF-TESTING KITS ON UPTAKE OF MALE PARTNER TESTING AMONG PREGNANT WOMEN IN
SELECTED COUNTIES IN KENYA
TOM MARWA MACHERA (MSc, MPH) Q97/24416/2013
A RESEARCH THESIS SUBMITTED IN PARTIAL FULLFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF DOCTOR OF PHYLOSOPHY IN EPIDEMIOLOGY IN THE SCHOOL OF PUBLIC HEALTH
OF KENYATTA UNIVERSITY
ii
DECLARATION
“This Thesis is my original work and has not been presented for a degree in any other University”
Signature. ……….. Date………
Tom Marwa Machera
Department of Community Health and Epidemiology
Supervisors:
This thesis has been submitted with our approval as University Supervisors.
Signature. ……….. Date………
Prof. Alloys S.S Orago (Ph.D) Department of Pathology Kenyatta University
Signature. ……….. Date………
Dr. Justus O.S Osero (Ph.D)
iii
DEDICATION
iv
ACKNOWLEDGEMENTS
v
TABLE OF CONTENTS Contents
DECLARATION ... ii
DEDICATION ... iii
ACKNOWLEDGEMENTS ... iv
TABLE OF CONTENTS ...v
LIST OF FIGURES ... ix
LIST OF TABLES ...x
DEFINITIONS OF OPERATIONAL TERMS ... xi
ABBREVIATIONS AND ACRONYMS ... xii
ABSTRACT ... xiii
CHAPTER I: INTRODUCTION ...1
1.1 Background information ... 1
1.2: Statement of the problem ... 3
1.3: Justification ... 5
1.4: Research questions ... 6
1.5: Null hypotheses ... 6
1.6: Objectives of the study ... 7
1.6.1: General objective ... 7
1.6.2: Specific objectives ... 7
1.7: Significance of the study ... 7
1.8:Study limitations ... 9
1.9:The conceptual framework of the study ... 9
CHAPTER II: LITERATURE REVIEW ... 11
2.1: Global picture and progress achieved to date in PMTCT and HTC interventions ... 11
2.2: PMTCT interventions in Sub-Saharan Africa ... 12
2.3: PMTCT interventions in Kenya ... 13
2.4: HTS as an entry point to HIV care, treatment and other HIV support ... 14
2.5: Male involvement into HTS interventions and programs ... 15
2.6: Summary of literature review ... 20
CHAPTER THREE: MATERIALS AND METHODS ...22
3.1: The study design... 22
3.2: The study sites and the facility sampling design ... 22
3.3: The study variables ... 23
3.4: The study population ... 23
3.5: The study participants ... 23
vi
3.5.3: Inclusion criteria for the male partner ...23
3.5.2: Consenting and GBV/IPV Screening ...24
3.5.5:Description of the intervention ...25
3.6: Sample size determination ... 26
3.7: Research instruments and data collection methods ... 29
3.7.1: Research instruments ...29
3.7.2: Data collection methods ...30
3.7.2.3: Focus group discussions ...33
3.8:Pre-Test. ...35
3.9: Validity and reliability ... 35
3.10: Data Analysis ... 36
CHAPTER FOUR: RESULTS ...39
4.1: Introduction ... 39
4.2: The numbers and demographic characteristics of participants recruited and followed up .... 39
4.2.1: Demographic characteristics of women enrolled into study arms ...40
4.2.2: Demographic characteristics of men who participated in the study ...42
4.2.3: Demographic characteristics of men who reported testing ...43
4.3: HIV self-testing acceptability rates among male partners ... 44
4.3.2 Male testing against the demographic characteristics of the ANC partner ...47
4.3.3: Determinants of HIV testing among male partners (as reported by men) ...49
4.4: Effectiveness of HIV oral selftesting kit and improved invitation letter in increasing couple testing rates ... 50
4.4.1: Women who reported discussing HIV and testing with their partners ...50
4.5: Prevalence of GBV, IPV, gender inequity and other harm associated with introduction of Oral HIV self-testing ... 53
4.6: Operational challenges by ANC mothers in providing HIV counselling and test kits to their partners ... 54
4.6.1: Person conducting the test ...55
4.6.2: Location of HIV testing ...55
4.6.3: Men who took a confirmatory test after testing at home ...56
4.5.4: Usability of test kits by the ANC mothers and their partners ...57
4.5.5: Operational challenges established in the field by the study staff ...59
4.6: Drivers and barriers of HIV self-testing among male partners ... 60
4.6.1: Stigma, fear and misinformation about HIV in the community ...60
4.6.2: Access barriers for men ...61
vii
CHAPTER FIVE: DISCUSSIONS, CONCLUSION AND RECOMMENDATIONS ...64
5.1 Introduction ... 64
5.2: Discussions ... 64
5.2.1: Socio-demographic characteristics of the study subjects ...64
5.2.2: HIV self-testing acceptability rate among male partners ...66
5.2.3: HIV testing among male partners ...69
5.2.4: Comparison of the primary outcome among the three study arms ...71
5.2.5: Effectiveness of HIV oral self-testing kit intervention package in increasing couple self-testing rates ...72
5.2.6: Prevalence of gender based violence ...72
5.2.7: Operational challenges by pregnant women in providing HIV counselling and self-test kits ...74
5.2.8: Men who took a confirmatory test after testing at home ...75
5.2.9: Location of HIV testing and person conducting the test ...76
5.2.10: Usability of test kits by the male partners ...78
5.2.11: Stigma, fear and misinformation about HIV in the community ...79
5.2.12: Access barriers for men: income, workload and distance ...80
5.2.13: Importance of privacy surrounding HIV self-testing ...81
5.2.14: Summary of discussions ...82
5.3: Summary of conclusions ... 84
5.4: Recommendations ... 86
5.4.1: Recommendations from the study ...86
5.4.2: Programmatic and policy recommendations ...87
5.4.3 Recommendations for future studies ...88
REFERENCES ...89
Appendix 1: Study Counties (Meru, Embu, Murang’a, Kitui, and Kiambu ... 95
Appendix 2: Study Counties in the Map of Kenya ... 96
Appendix 3: Improved Invitation Letter for the Male Partner ... 97
Appendix 4: Post-Test Instructions to Study Participants ... 98
Appendix 5: Recruitment and Screening Script for the Study ... 99
Appendix 6: Consent Form ... 101
Appendix 7: Consent 1- ANC Clients Swahili ... 103
Appendix 8: Tool 1: Partner testing ANC client’s demographics ... 106
Appendix 9: Tool 2: End-line questionnaire for ANC clients ... 115
Appendix 10: Tool 3: Questionnaire for male partners of ANC clients ... 130
Appendix 11: Tool 4: Qualitative Focus Group Discussion Guide ... 141
viii
Appendix 13: NACOSTI Research Authorization Certificate ... 146 Appendix 14: Kenyatta University Ethics Review Committee Approval ... 148 Appendix 15: Kenyatta University Ethics Review Committee Research Approval ... 149 Appendix 17: Abstracts of Papers submitted for Publication in Various Journals (Panafric
ix
LIST OF FIGURES
Figure 1.1 Conceptual framework of the study framework (ARRM., 2011; Catania
1990)... 10 Figure 2 Follow-Up Schedule and Interventions for Pregnant Women in study arms ... 26 Figure 3 Recruitment Process for study participants ... 32 Figure 4 Percentage of women who reported discussing HIV and testing with their
partners ... 51 Figure 5 Male partners who went/did not go for a confirmatory test after testing at
x
LIST OF TABLES
Table 3.1: The sample size determination using the power procedure Pearson
chi-square tests for two proportions ...28
Table 3.2: Sample size break down per study site ...29
Table 3.3: Number of FGDs with ANC clients, by relevant characteristics and county ....35
Table 4.1: The numbers and proportions of participants recruited and followed up in each of the three study arms ...41
Table 4.2: Demographic characteristics of women enrolled into the study ...42
Table 4.3: Wealth distribution among ANC mothers recruited into each arm ...43
Table 4.4: Demographic characteristics of men who were followed up ...44
Table 4.5: Demographic Characteristics of Males tested for HIV (N=566) ...45
Table 4.6: Males recruited, accepted testing and those who refused or did not test 46 Table 4.7: Males testing history ...47
Table 4.8: The proportions (%) of men who reported testing for HIV in the 3-month follow-up period ...47
Table 4.9: Demographic Characteristics Arm 1 ...48
Table 4.10: Demographic characteristics Arm 2 ...49
Table 4.11: Demographic characteristics Arm 3 ...50
Table 4.12: Determinants of HIV testing among male partners ...51
Table 4.13: Test of agreement on testing by ANC client and male partner enrolled in arm one. ...53
Table 4.14: Test of agreement on testing by ANC client and male partner enrolled in arm two ...53
Table 4.15: Test of agreement on testing by ANC client and male partner enrolled in three of the study arms ...54
Table 4.16: Gender equity and GBV among male respondents ...55
Table 4.17: Person conducting the test ...56
xi
DEFINITIONS OF OPERATIONAL TERMS
Theory of change: Theory of Change defines long-term goals and then maps backward to identify necessary preconditions(Development & Based, 2013).
Gender based violence (GBV): Gender-based violence refers to aggression that targets individuals or groups based on their gender. Gender‐based violence against women” shall mean aggressive behavior directed against a woman because she is a woman, which affects women disproportionately(Gender based violence, PSI, 2016). The study excluded women only if the GBV risk was directly associated with discussion of HIV testing with their partner.
Male involvement: Men knowledge about reproductive health issues and can communicate with their partners, and are more supportive during pregnancy and may make better health care decisions and can also share the responsibility of disease prevention, as well as the risks and benefits of reproductive health (Kamal, 2002). Intimate partner violence: The term intimate partner violence (IPV) describes a physical and/or sexual violence, stalking and psychological aggression (including coercive acts) by a current or former intimate partner.
HIV self -testing: refers to a process whereby a person who wants to know his or her HIV status collects a specimen, performs a test and interprets the test result in private. Study arm 1 (Control 1) received the current standards of HIV testing and counselling services offered to ANC clients in Kenya, which includes the male partner invitation, excluding mentioning of HIV testing and inviting him through a letter to come to the ANC clinic with his pregnant partner. Study arm 2 (control 2) received an improved invitation letter that described the benefits to the family and the man’s own health when both partners were tested for HIV, and was to invite the partner to return to the clinic for standard HIV testing.
Study arm 3 (Intervention 2) were given the same improved invitation letter as Study arm 2 describing the benefits of HIV testing. Participants in this group were provided with two oral self-test kits, counselling, communications materials and clear instructions on how to self-test
xii
ABBREVIATIONS AND ACRONYMS
ANC Antenatal Care Clinic
ARRM AIDS Risk Reduction Model ART Antiretroviral Therapy
BCC Behavior Change and Communication C&T Counselling and Testing
CCC HIV Comprehensive Care Centre CHVs Community Health Volunteers EMTCT
eHealth
Elimination of Mother to Child Transmission of HIV Electronic Health
FGD Focus Group Discussion FP Family Planning
GBV Gender Based Violence HCW Health Care Worker HTC
HTS
HIV Testing and Counselling HIV Testing Services
KAIS KDHS
Kenya AIDS Indicator Survey
Kenya Demographic and Health Survey KEMRI Kenya Medical Research Institute KEMSA Kenya Medical Supplies Agency mHealth Mobile Health
MOH Ministry of Health
MTCT Maternal to Child Transmission of HIV NASCOP
NACC VMMC SMS OVC
National AIDS and STI Control Programme National AIDS Control Council
Voluntary Medical Male Circumcision Short Message Services
Orphans and Vulnerable Children PEPFAR
PITC
President’s Emergency Plan for AIDS Relief Provider Initiated Counselling and Testing PLHIV People Living with HIV
PMTCT IPV
Prevention of Mother to Child Transmission of HIV Intimate Partner Violence
PwP Prevention with Positives RH
RCT
Reproductive Health
Randomized Controlled Trial
xiii
ABSTRACT
1
CHAPTER I: INTRODUCTION 1.1 Background information
By 2017 over 79 million people had been infected with HIV since the beginning of the epidemic in early 1980 (UNAIDS, 2017) and AIDS related illnesses were ranked 6th in causing mortality globally (WHO, 201). By the end of 2017, 37 million people were living with HIV worldwide, of which 1.8 million people became infected in 2017 alone and 1.1 million died of AIDS-related illness (UNAIDS, 2017). Sub-Saharan Africa accounts for over 70% of all HIV related morbidity and mortality globally while in 2017, 27 million of the 37 million PLHIV were in Sub Saharan Africa. Eastern and southern Africa accounts for 43% of the global total of new HIV infections (Gaps, Barriers, & Injustices, 2018)
2
Bureau of Statistics, 2010; Cherutich et al., 2012). HIV-testing and counselling (HTS) is a very effective strategy in linking those infected with HIV into care and treatment and making appropriate referrals to other HIV support services(Sabapathyet al., 2012). Kenya adopted a number of HIV testing strategies including provider initiated testing and counselling (PITC), outreach testing and counselling, home based testing and counselling. Other strategies that have proved effective are integration of HTS in antenatal care and reproductive health (Mutemwa et al., 2013).
3
role in promoting the a woman’s health. Male partners also influence women’s treatment decisions, including whether she receives medication (Msuya et al.,2008) and whether she adheres to infant feeding advice (Katz et al., 2009).Many women in Kenya fear disclosing their HIV positive status to their male partners because of stigma or discrimination, many a time these same women will end up experiencing some form of physical or psychological violence, and/or even death,(Gielen et al.,2000). Thus, the potential for violence as a consequence of disclosure remains an important question to address empirically.
1.2: Statement of the problem
Kenya AIDS Indicator Survey of 2014 reported that up to 6.5% of pregnant women in Kenya were living with HIV, and that each year, close to 45,000 infants becomes infected with HIV through maternal-to-child transmission of HIV (ROK- NASCOP, 2014).In Kenya, women are more likely to have been tested for HIV (79.8%) than their male counterparts (62.5%) are, (Republic of Kenya, KDHS 2009). Inadequate up-take of testing for HIV remains a primary challenge towards universal access to treatment and care as well as an obstacle to realizing the potential of new interventions for preventing HIV infection, including treatment and prevention.
4
during ANC services, such as having male-only clinics on special days or evening clinics have been tried without much success (Kalembo, 2012). Despite the huge roll out of HIV testing services in Kenya, the uptake has continued to remain low especially among the males and young persons.
KAIS findings on why the low uptake of HIV testing services among the males and young persons have shown several factors that includes poor access to HIV testing services, non-autonomy, confidentiality issues, client not empowered and the service not convenient most of the time to the client. Engagement and enrolment of male partners remains a challenge in scaling up couples services. Men are less likely than women to go and test for HIV (Peltzer, et al., 2009; Majaja, 2009). There is limited information on male involvement in HIV counseling and testing at the antenatal setting in the developing world (Koo et al., 2013b). Correlates of male HIV testing behavior and the reasons for obtaining HIV tests have been examined in sub-Saharan Africa using population-based studies and within workplace and clinic-based HTC trials (Manuscript & Long, 2008), this studies used the standard testing approaches, however there is need to use newer HIV testing technologies such as oral HIV testing oral kit to determine male involvement.
5
partners. The study findings will provide some deep understanding on the drivers and barriers of HIV self-testing among male partners.
1.3: Justification
HIV self-testing has a number of benefits and the potential to meet the needs and address challenges of access to knowledge of HIV status. Some of the benefits includes promoting access to HIV testing services; it increases autonomy and assures convenience and confidentiality to the user. It is on this premise that this study used the HIV oral self-testing kits to determine its effects on male partner testing rates among other outcomes. This study used the ANC platform to reach the male partner with the self-testing test kit, this was done to determine if barriers such as access to test kits, stigma associated with walking to the ANC by the male partner if removed would it increase male testing rates among other primary outcomes. In order to bring interventions for couples to scale, efforts are clearly needed to address and specifically appeal to male partners and to link them to HIV prevention, care and treatment services.
Antenatal clinics in Kenya have the potential of being key entry points to HTS not only for pregnant women, but also their partners and that is why this study had a special focus on the ANC service delivery points in five counties. The ANC platform provides an opportunity to offer the HIV oral self-test kit as an innovative way to increase the rate of testing for male partners of pregnant women without requiring men to come to the health facility for their initial HIV test.
6
superior to their observational counterparts in generating accurate findings that could be used to advice policy and program implementation. There are several factors contributing to utilization and uptake of HIV counseling and testing services. This state’s detailed analysis of the interaction of this multiple factors that includes individual demographic, socio-economic, individual knowledge and practices and other factors. This study used both qualitative and quantitative research approaches to explore the interaction of this factors and how they influenced uptake and acceptability of HIV self-testing among the male partners in Kenya.
1.4: Research questions
1. What are the self-testing acceptability rates among male partners of the ANC mothers in the study counties?
2. What are the effects of HIV oral self-testing kit and improved HIV prevention message card in increasing couple testing rates in the study counties?
3. What were the GBV/IPV associated with introduction of oral HIV self-testing on male partner among women in the study counties?
4. What were some of the operational challenges experienced by pregnant women in providing counselling and HIV self-testing kits to their male partners?
5. What were the factors that affect HIV self-testing among male partners of the ANC clients?
1.5: Null hypotheses
1. Provision of HIV oral self-test kits by ANC mothers to their male partners has no association with increased male partner testing rates in the study counties 2. Provision of HIV oral self-test kits by ANC mothers to their male partners has
7
3. Provision of HIV oral self-test kits by ANC mothers to their male partners at home is not associated with GBV among women
1.6: Objectives of the study 1.6.1: General objective
To describe the effects of using self-testing kits on uptake of male partner testing among ANC women in Meru, Kiambu, Kitui, Embu and Murang’a counties
1.6.2: Specific objectives
1. To determine HIV self-testing acceptability rates among male partners of ANC mothers in the study counties
2. To establish the effectiveness of HIV oral self-testing kit and improved invitation letter in increasing couple testing rates in the study counties
3. To determine the prevalence of GBV associated with introduction of oral HIV self-testing in the study counties
4. To establish operational challenges by pregnant women in providing counselling and HIV self-test kits to their partners
5. To determine factors affecting HIV self-testing among male partners of the ANC clients.
1.7: Significance of the study
The Kenya AIDS indicator survey of 2014 showed that 50% of men and women reported not knowing the status of their last sexual partner within the past year(Republic of Kenya- National AIDS and STI Control Programme, 2014).
8
demonstrated that by increasing male partner testing using the HIV self-testing kits (from 6% to 82%) at the ANC platform, could greatly contribute to male involvement in PMTCT and HIV services, and hence the potential to reduce MTCT and other new HIV infections among adults.
The findings from this study have presented a new and exciting frontier to further understand the dynamics of self-testing among men, while also bringing about health impact for their pregnant partners, as it does not require men to go to antenatal clinics in person.
In Kenya about4.8% of all married or cohabitating couples are sero-discordant (one partner is HIV-positive while the other is HIV-negative), based on this, the study findings will inform HIV programmers and policy makers on how to formulate robust strategies to reach the negative partner in a discordant relationship and intervene on time. The finding from this study will also inform on how best to close in the gap in HIV testing and help to inform on how to reach 90% of all people with HIV by 2020 according to World Health Organization 90-90-90 global HIV targets, specifically the first target of diagnosing 90% of all people with HIV.
The findings of this study will provide information on how best to roll out the oral HIV test kits in the general population and provide more information on how to support countries to provide two new additional HIV testing services (HTS) options to reach people who may not otherwise be reached with the existing routine HTS services.
9
challenges in advance and start thinking on how to mitigate and deal with operational barriers and challenges
1.8: Study limitations
In each study arm, the participants were followed up in several ways to learn of partner testing. It was assumed that it was going to be easy to access and enroll all eligible ANC mothers’ male partners; this limitation was overcome by involving CHVs, study research assistant to follow up with a visit to the ANC client’s residence in a discreet manner when asking about partner testing. To avoid a tendency by study assistants to more aggressively follows up women in one of the study groups (arm three) regarding partner testing or another study outcome, study assistants were encouraged to have unbiased follow-up and outcome assessment in all groups. To avoid or minimize unintended consequences such as GBV and IPV, the study excluded women only if the GBV risk was directly associated with discussion of HIV testing with their partner. This exclusion criterion was administered prior to randomizing women into the study arms
1.9: The conceptual framework of the study
10
partner HIV counselling, provision of self-testing Kits and referrals to GBV centers as illustrated in figure 1
Figure 1.Conceptual framework of the study framework (ARRM., 2011;Catania 1990)
Independent variables
Socio-Demographic
• Socio economic factors • Age • Gender • Education level
Factors influencing acceptability
• Communication
• Culture
• Myths and misconceptions
GBV prevalence • Culture • Relationship • Communication • Poverty
Operational challenges
• Partner communication • Test Kits storage • Partners counselling • Results interpretation
Intervening variables
• Provision of self-testing kits to the male partner of the ANC client
Dependent variables
11
CHAPTER II: LITERATURE REVIEW
2.1: Global picture and progress achieved to date in PMTCT and HTC interventions
12
programme, particularly in sub-Saharan Africa. Among the main barriers are low access to low acceptability of testing(Arnold, 2013), As a result, guidelines recommend implementation of routine counselling and testing as part of the ANC services (World Health Organization, 2007). HIV testing and counselling (HTC) empowers individuals and couples to adopt measures to prevent the transmission or acquisition of HIV infection. Furthermore, testing provides access to HIV prevention services, including prevention of mother-to-child transmission (PMTCT), male circumcision, and ART, including pre-exposure prophylaxis (PrEP), and microbicides. Furthermore, recent evidence of the effectiveness of early initiation of antiretroviral therapy (ART) to prevent HIV transmission in sero-discordant couples (Cohen et al., 2011; Meyer et al., 2011) highlighted the need to expand access to testing services that reach couples. At the community level the expanded availability of HIV testing services (HTS) may help reduce the stigma and discrimination associated with HIV and HIV testing (Khumalo-Sakutukwa et al., 2008; Kimaiyo et al., 2010).
2.2: PMTCT interventions in Sub-Saharan Africa
13
involvement in PMTCT programme with an aim of increasing the uptake of PMTCT services (Potterat, 2011).
2.3: PMTCT interventions in Kenya
14
2.4: HTS as an entry point to HIV care, treatment and other HIV support
15
2.5: Male involvement into HTS interventions and programs
16
as well as improved compliance with PMTCT measures such as nevirapine (NVP) uptake. Little published information is available that examines the role of couples counselling in an antenatal setting with PMTCT uptake and social adverse events. The rapid expansion of PMTCT programs in low-resource settings makes it crucial to evaluate strategies to improve the effectiveness of PMTCT interventions while minimizing the potential risks and harm to women.
In 2009, the Kenyan Government emphasized the importance of male involvement in PMTCT and family planning services, and in 2010 started a campaign to encourage partner testing, exclusive breastfeeding and the delivery of ART to children. Male involvement in PMTCT remains very low in Kenya at 4.5 % (Republic of Kenya- NASCOP’s KAIS report. 2014).
2.5.1: Male partner’s role in HTS and HIV prevention
Mother-to-child HIV transmission (MTCT) remains a significant problem in the developing world despite the development and growing availability of effective prevention methods appropriate for resource-limited settings. HTC in the context of antenatal care serves as the entry point for targeted prevention of MTCT, and majority of pregnant women accept antenatal HTC in these settings (Katz et al., 2009), many do not learn their HIV status, or participate in prevention programs, to reduce the risk of MTCT HIV transmission (Kinuthia et al., 2011).
17
Couple HTC has been shown to be more effective and beneficial than accompanying the female partner for individual HTC (Farquhar et al., 2004), and further analyses in this findings by Farquhar showed that couple counselling was similar in terms of cost-effectiveness for preventing MTCT to standard antenatal HTC. Unfortunately, few men accompany their partners to antenatal clinics and even fewer participate in couple counselling when it is available.
18
Awareness rate of HIV and AIDS in Kenya is one of the highest in Africa. Many people living with HIV in Kenya face high levels of stigma and discrimination and these results in many infected people not seeking treatment (Stangl et al., 2013). A study on stigma as a barrier to health facilities births (Turan et al., 2011), showed that pregnant women often do not test for HIV because they fear stigmatization from their family or healthcare workers. The survey report (Republic of Kenya- KDHS 2014) indicated that 92% of women in Kenya received antenatal care from a medical professional, either from doctors (29%), or nurses and midwives (63%). A very small fraction (less than one percent) receives antenatal care from traditional birth attendants, and 7% do not receive any antenatal care at all.
2.5.1.1:Self-testing Procedure, steps and concept
19
To date, there is limited evidence on the feasibility, accuracy, and acceptability of self-testing for HIV. High levels of “informal” self-self-testing have been reported among health workers in sub-Saharan Africa (Alfred & Nzala, 2014)and there are reports of the unregulated use for self-testing of rapid diagnostic tests, purchased through the Internet, by groups such as men who have sex with men in China. Self-testing is currently being explored for use by health care workers in Kenya (Choko et al.,2011; Republic of Kenya self-testing, 2017) and in communities in Malawi. Despite the dearth of evidence on the feasibility of self-testing at home, studies in the United States of America find that people at risk of HIV infection and people with no history of HIV testing consider the concept acceptable (WHO, 2012).
A cross-sectional feasibility study in Malawi, which provided consenting individuals with the option of HIV self-testing followed by standard VCT or else standard VCT alone, reported that 92% of participants selected HIV self-testing (Choko et al., 2011). The accuracy of self-testing was high, with 99.2% of results concordant with subsequent repeat confirmatory HIV testing. Furthermore, 98.5% of participants said that the testing kits were “very easy” to use, and all who self-tested said that they would recommend HIV self-testing to others. Exit interviews with randomly selected individuals indicated that most would prefer self-testing in future.
20
at the last minute thus fueling poor male participation and resistance. Other gaps that emerged from this literature review are lack of supportive and routine voluntary HIV self-testing services as part of a public health approach to delivering HTS at the community and household level.
2.6: Summary of literature review
The literature reviewed comprised research, randomized controlled studies, cross sectional studies, case studies, demographic health surveys, AIDS surveys, programme reports and qualitative studies conducted in African countries especially Sub Saharan Africa, Asia and North America from 1995 to 2016. The key words during literature search were HIV self-testing, male partner involvement in ANC and PMTCT programme, HTS and ANC. It also included searches on facilitators and barriers in involving the male partner of the pregnant woman. It concluded by capturing lessons learnt and gaps in requisite knowledge that needs to be filled to have a successful HIV Programme with greater male involvement. This was done by reviewing studies done in other countries on male involvement, potential and viability of introducing self-testing concept into the key populations and the general population.
21
22
CHAPTER THREE: MATERIALS AND METHODS 3.1: The study design
This was a mixed method study design where both qualitative and quantitative data were collected. Randomized controlled trial (RCT) with three study arms were used to collect quantitative data while focus group discussions (for ANC mothers)were
conducted to collect qualitative data.
3.2: The study sites and the facility sampling design
Fourteen (14) health facilities were purposively selected from 180 MOH and one mission health facilities in Meru, Embu, Kiambu, Kitui and Murang’a counties based on the high volume of clients and also huge attendance of ANC mothers. Embu, Kiambu, Kitui, Murang’a and Meru Counties were purposefully selected based on the following reasons:
1. Good social support mechanism for the Pregnant mothers e.g. the availability of mentor mothers groups, HIV psychosocial support groups, to mitigate other unwanted outcomes such as GBV; and other crucial services for male partners who test positive and need immediate support among other services such ART, STI treatment, and psychosocial support
2. High volume facilities and the support from other HIV and AIDS implementing partners. These organizations were key when it came to HIV support, care treatment and referrals outcomes that needs available intervention.
23
In other high to medium HIV prevalence counties such as Nyanza, Western, Coast, Rift valley, Migori and Homabay; there were other HIV self-testing ongoing studies on the general population but not on ANC clients. This would have greatly affected this study if it were to be conducted in these counties.
3.3: The study variables
The independent variables were social demographic factors, factors influencing acceptability, prevalence of GBV and operational challenges, while the dependent variable was increased uptake of HIV-testing by the male partner of ANC mother using the self-administered HIV testing kits. The intervening variable included provision of HIV self-testing Kits to the male partner.
3.4: The study population
These were ANC mothers, ANC mothers’ male partners
3.5: The study participants
These were women attending ANC clinic for the first time (first ANC visit in their current pregnancy). HIV-negative women and HIV-positive women (because their male sexual partners could be either HIV negative or positive)
3.5.1: Inclusion and exclusion criteria 3.5.1.1: Inclusion criteria expectant women
ANC mothers
First ANC visit in this pregnancy
3.5.3: Inclusion criteria for the male partner
Male partner of ANC client enrolled in the study
24
Has good cognitive abilities and mentally sound to respond to the survey
questions
3.5.1.2: Exclusion criteria expectant women
Had no current male partner / does not have at least weekly contact with
partner
Woman reported that her partner is HIV positive.
Woman reported that her partner has tested within last three months ` Woman concerned for her safety or feel at risk of GBV if she asked her
partner to self-test, or woman currently does not feel safe at home to encourage HIV testing
3.5.2: Consenting and GBV/IPV Screening
The research assistants screened women for eligibility and those who agreed to participate in the study signed informed consent. The women were also informed that their male partners would be contacted to discuss HIV testing. Following the consent of the female participants, the study nurse administered a structured questionnaire at baseline to collect socio-demographic and behavioral information. Informed consent was also obtained from the participants’ male partners willing to participate in an interview.
25
Are you worried that your partner (or another person close to you) will be
angry and/or hurt you if s/he finds out you were tested for HIV in antenatal care?
Do you feel unsafe returning to your home today?
Are you afraid that your partner may harm you in any way if you shared
your HIV test results with him?
For women who tested HIV positive, ask: “Do you think that your partner
may physically hurt you if you tell him that you have tested for HIV and your HIV test results are positive?”
3.5.5:Description of the intervention
26
Figure 1.Follow-Up Schedule and Interventions for Pregnant Women in study arms
3.6: Sample size determination
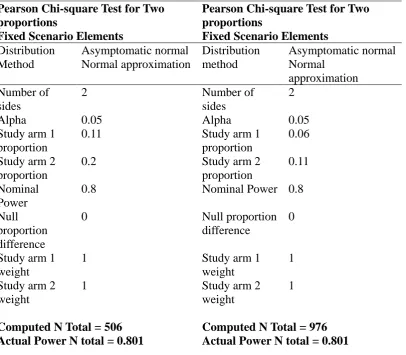
SAS software system was be used to calculate the sample size using the power procedure Pearson chi-square test for two proportions. At the facility levels, each facility was allocated sample size based on first ANC visits as per the year 2014 (KDHS data), see Table 3.1 above.Sample size was calculated by comparing Study arm 1 and Study arm 2, and Study arm 2 and Study arm 3. Sample size calculation comparing Study arm 1 and Study arm 3 was not performed because it was expected that the difference between the two groups would always be larger than any other comparison. In all sample size calculations, level of significance was assumed at 5% and power was at a minimum of 80%. Groups 1 and 2 sample sizes were calculated Interview for Women and men after 12 weeks
27
based on equivalence test. It was assumed that 5% was the limit of equivalence, i.e., any difference bigger than 5% made the two groups not equivalent. If there were no difference between Study arm 1 and Study arm 2,5% limit of equivalence, n=475 per group for 80% power to detect difference of more than 5%, 475 per group ANC clients were required to be 80% sure that the limits of a two-sided 95% confidence interval were excluded in difference between the two groups of more than 5%.
28
Table 3.1: The sample size determination using the power procedure Pearson chi-square tests for two proportions
The SAS system
Pearson Chi-square Test for Two proportions
Fixed Scenario Elements
Pearson Chi-square Test for Two proportions
Fixed Scenario Elements
Distribution Asymptomatic normal Distribution Asymptomatic normal Method Normal approximation method Normal
approximation Number of
sides
2 Number of
sides
2
Alpha 0.05 Alpha 0.05
Study arm 1 proportion
0.11 Study arm 1
proportion
0.06 Study arm 2
proportion
0.2 Study arm 2
proportion
0.11 Nominal
Power
0.8 Nominal Power 0.8
Null proportion difference
0 Null proportion
difference
0
Study arm 1 weight
1 Study arm 1
weight
1 Study arm 2
weight
1 Study arm 2
weight
1
Computed N Total = 506 Actual Power N total = 0.801
29
Table 3.2: Sample size break down per study site
Facility Arm 1 Arm 2 Arm 3 Total
Githunguri Health Centre 36 36 36 108
Kihara Sub-District Hospital 42 42 42 126
Lari Health Centre 31 31 31 93
Maragua D.Hospital 32 32 32 96
Tigoni District Hospital 25 25 25 75
Uthiru Health Centre 22 22 22 66
Embu PGH 56 56 56 168
Kangeta Health Centre 28 28 28 84
Kanyakine District Hospital 17 17 17 51
Muthale Mission Hospital 28 28 28 84
Nyambene District Hospital 40 40 40 120
Kiritiri Health Centre (Mbeere) 21 21 21 63
Mbeere District Hospital 28 28 28 84
Meru Level 5 69 69 69 207
Total 475 475 475 1425
3.7:Research instruments and data collection methods 3.7.1: Research instruments
30
3.7.2: Data collection methods 3.7.2.1: Quantitative method
A study questionnaire was completed with all enrolled clients demographics. Date of client’s next ANC visit was recorded in the study materials and reviewed in ANC client register. At 12 weeks, an end line questionnaire was administered to generate data on both primary and secondary outcomes (i.e., GBV, invalid tests, Linkages to care) of the study. Given that over 90% of women brought their children to immunization clinics, this provided an optimal in-person follow-up opportunity for third trimester enrollees. For first ANC clients who were eligible for the study, the study assistant obtained consent from them. Clients were told that the study is about HIV testing among male partners and that information and support about male partner testing may be given to each participant. This was done in private space in clinic, immediately after determining eligibility.
3.7.2.1.1: Recruitment of ANC mothers
31
3.7.2.1.2: Randomization of ANC mothers into study arms
Participants were individually randomized into one of the three study arms following their informed consent. During randomization, each study arm was assigned a distinct color (yellow for study arm 1, green for study arm 2, and blue for study arm 3). Computer generated numbers were used to randomize the participants into each study arm, generated numbers were then put in opaque envelopes and each participant was requested to randomly select an envelope from the basket indicating the arm of study to which she was assigned.
Study arm 1 (Control 1) received the current standards of HTS (HIV testing and
counselling services) offered in Kenya to ANC clients, which includes the male partner invitation, not excluding mentioning of HIV testing and inviting him through a letter to come to the ANC clinic with his pregnant partner.
Study arm 2 (Control 2) received an improved invitation letter that described the
benefits to the family and the man’s own health when both partners were tested for HIV, and was to invite the partner to return to the clinic for standard HIV testing. The rationale for inclusion of this control group was to isolate the impact of self-testing kit availability, and control for the additional information that must be provided to test-kit recipients.
Study arm 3(Intervention arm) were given the same improved invitation letter as
32
randomized group had475 women. For each ANC mother meeting eligibility criteria and consenting to participate, the intervention itself (for two of three study groups) were added to the end of the standard first ANC visit. At the end of the visit, the pregnant woman’s HIV status were known for most women. Both HIV-positive and HIV-negative women were invited to participate, as well as women with unknown status. This included women who knew they were HIV-positive before coming to their first ANC visit. Women enrolled in the study received a sticker in their Mother Child Clinic Booklet so that other health workers can easily identify that these women were participating in the study without compromising confidentiality.
Figure 2 Recruitment Process for study participants
The ANC client
proceeds with the routine ANC services
Identification of potential study participants
Screening for eligibility using inclusion criteria
Study intervention offered at the exit of ANC services
Randomize theparticipants Study arm 1 = Yellow Study arm 2 = Green
33
3.7.2.2: Qualitative method
The study expanded the description of the qualitative data collection and analysis through FGD. The qualitative component helped understand why the intervention worked or did not work, and the factors or conditions under which partner self-testing were possible or not. The study explored barriers and facilitating factors as demonstrated in Theory of Change. To create a robust analysis of the focus group discussions, the most appropriate analytical technique was to create a framework analysis. This is because framework analysis suits analyzing cross sectional and descriptive data, such as the data collected from the FGD. Framework analysis is also suited to creating themes of analysis that can be used to gain an understanding of a specific research topic (Snape et al., 2003). Although significant themes emerged from initial observations, to minimize any researcher bias initial codes and corresponding categories were created based solely on respondents answers during the focus group. It is already known that partners of ANC service users are much more likely to take an HIV test at home rather than going to a clinic.
3.7.2.3: Focus group discussions
34
discussions randomly selected from the 14 study sites. The participants gave their contribution and views on issues, experiences, benefits and challenges concerning testing their male partners. Those interviewed included women (given test kits) who their male partners tested and those whose partners never tested. In each group, women were invited based on whose partner tested. The study transcribed interviews, identified existing and emerging themes, categorized responses into identified themes, and used the qualitative data both to enrich the in-depth understanding of the self-testing results and inform where to look for quantitative differences between study arms. The qualitative research helped inform recommendations.
Table 3.3Number of FGDs with ANC clients, by relevant characteristics and county
Meru Embu Kiambu Muranga
Younger Women (<25)
1 group (8) 1 group (8) 1 group (8) 1 group (8)
Older Women (25+) 1 group (8) 1 group (8) 1 group (8) 1 group (8)
3.6.2.4: Male partner follow up
35
consent. After the consent, the research assistant proceeded with the interviews. Alternatively, if the male partner accompanied the ANC client to the follow up ANC appointments or the birth at the clinic, research assistant approached him and recruited him
3.7.2.5: Social Harm/Gender-Based Violence
In supporting the ANC clients to counsel and give the test kit to the spouses, a comprehensive counselling was required for the success of the proposed intervention. Counselling of ANC clients included role-playing and instructions to help the woman be ready to counsel her partner and demonstrate how the test kit is used to perform the test. Counselling also included pictorial counselling materials. The study relied heavily on the existence of mentor mother groups and/or peer educators to mitigate any negative outcome and also follow up. Most community health workers in the study area were sensitized on gender-based violence prevention and response, and how to provide appropriate support to HIV+ regarding disclosure.
3.8:Pre-Test
The study instruments and tools were tested to ensure that they are suitable, a pre-test was conducted in Kiambu county hospital at the ANC clinic. The changes and recommendations from the pre-testing exercise was incorporated into the final main study tools. The researcher was responsible for day to day record of the study questionnaires. All the questionnaires were numbered and checked for completeness and accuracy at the end of each day
3.9: Validity and reliability
36
the study, the instruments were constructed as precise and clear as possible to cover adequately the study goal and objectives. Study tools had close-ended questions with a number of possible outcomes given and for the prediction on the existence of some outcomes; open-ended questions were used to capture the information.
3.10: Data Analysis
37
controlling for socio-demographic information and other characteristics. Subgroup analysis were conducted for specific subgroups to determine if there was a differential effect of the interventions by subgroups. The key subgroups of interest were: clients’ HIV status, marital status, education and economic status.
The main focus of the FGD analysis was to gain an understanding of the barriers and drivers which decide whether or not male partners of ANC clinics decide to test for HIV. This was done by building an analysis of the experiences and opinions of the ANC service users through multiple focus group discussions. From the framework analysis output there consistently emerged five main themes which helped to explain some of the barriers and also the successes of HIV testing for male partners of ANC clinics. This analysis presented some of the differences in experiences between women who were sent with the self-testing kits and those who were tested at the ANC clinics. The qualitative component allowed ANC clients, partners and providers to tell their story in their own words to shed more light on the local context and influential actors and processes.
3.11: Ethical and logistical considerations
38
39
CHAPTER FOUR: RESULTS 4.1: Introduction
The study analyzed the following demographic characteristics of the study participants; age distribution, marital status, testing history, gender and religion. The results were presented in respect to the objectives of the study, that is, results on the determinants of HIV self-testing acceptability rates among male partners of ANC mothers, effectiveness of HIV oral self-testing kit and improved invitation letter in increasing couple testing rates, operational challenges among male partners by pregnant women in providing counselling and HIV self-test kits, barriers and drivers of HIV testing among male partners of ANC mothers in Meru, Kiambu, Kitui, Embu and Murang’a counties.
4.2: The numbers and demographic characteristics of participants recruited and followed up
40
Table 4.19:The numbers and proportions of participants recruited and followed up in each of the three study arms
Target Sample size
Control 1 N = 475
Control 2 N = 475
Intervention N = 475
Total 1425 No of Women recruited 471 (99%) 467 (98%) 472 (99%) 1410 (99%)
Number of women followed up
408 (87%) 387 (83%) 422 (89%) 1217 (86%)
Number of men recruited
375 (80%) 362 (78%) 396 (84%) 1033(80%)
Complete pairs of man and woman followed up
366 (78%) 352 (75%) 389 (82%) 1107 (79%)
4.2.1: Demographic characteristics of women enrolled into study arms
41
interviewed were aged 18 – 34 years with 91% being in arm one, arm two (92%) and arm three (88%). A test of association between the demographic characteristics and the study arms were insignificant, evidence that women were randomly allocated without any bias, meaning that your demographic characteristic did not influence the study arm that you belonged.
Table 4.20: Demographic characteristics of women enrolled into the study
Demographic
characteristics Arm 1 Arm 2 Arm 3
²Test
Significance Level of Education
Primary 279 (59.2) 265 (56.7) 247 (52.3)
P=0.096;df=2 Secondary 192 (40.8) 202 (43.3) 225 (47.7)
Religion
Catholic 83 (17.6) 103 (22.1) 107 (22.7)
P=0.251;df=4 Protestant 382 (81.1) 355 (76.0) 359 (76.1)
Other 6 (1.3%) 9 (1.9%) 6 (1.3%)
Employment
Self-employed 160 (34.0) 159 (34.0) 145 (30.7) Employed 70 (14.9) 74 (15.8) 83 (17.6)
P=0.737;df=4 Unemployed 241 (51.2) 234 (50.1) 244 (51.7)
Marital status
Single 5 (1.1) 9 (1.9) 8 (1.7)
Cohabitating 58 (12.3) 49 (10.5) 54 (11.4)
P=0.751;df=4 Currently married 408 (86.6) 409 (87.6) 410 (86.9)
Age (years)
18-34 430 (91.3) 430 (92.1) 419 (88.8)
P=0.189;df=2
≥ 35 41 (8.7) 37 (7.9) 53 (11.2)
4.2.1.1: Wealth status among mothers recruited into the study
42
status in those who tested and did not test for HIV was statistically significant among women in arm one and arm two (P= 0.001 and 0.005,df= 3, respectively). However it was not significant in arm three where the women received the test kits and improved male invitation letter (P= 0.16df= 3,)
Table 4.21: Wealth distribution among ANC mothers recruited into each arm
Study arm one
Wealth Not tested N (%) Tested N (%) P-value
Wealth 1 48 (50.5) 47 (49.5)
<0.001
Wealth 2 60 (61.9) 37 (38.1)
Wealth 3 88 (82.2) 19 (17.8)
Wealth 4 96 (89.7) 11 (10.3)
Study arm two
Wealth 1 45 (52.3) 41 (47.7)
0.005
Wealth 2 61 (60.4) 40 (39.6)
Wealth 3 61 (62.2) 37 (37.8)
Wealth 4 78 (76.5) 24 (23.5)
Study arm three
Wealth 1 19 (16) 100(84)
0.160
Wealth 2 19 (17.6) 89 (82.4)
Wealth 3 27 (27.3) 72 (72.7)
Wealth 4 22 (22.9) 74 (77.1)
4.2.2: Demographic characteristics of men who participated in the study
43
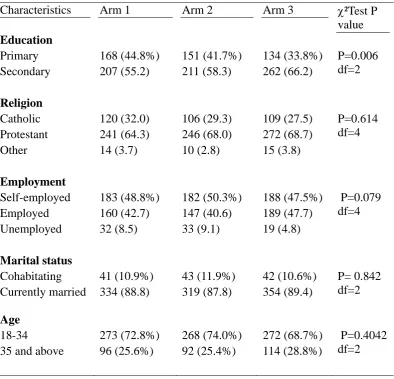
Overall, results demonstrate balance across study arms for most measures. There were statistically significance (P = 0.006df= 2) in the level of education among the men who participated in the study, with more men having attained secondary education Table 4.22: Demographic characteristics of men who were followed up
Characteristics Arm 1 Arm 2 Arm 3 ²Test P value
Education
Primary 168 (44.8%) 151 (41.7%) 134 (33.8%) P=0.006 df=2 Secondary 207 (55.2) 211 (58.3) 262 (66.2)
Religion
Catholic 120 (32.0) 106 (29.3) 109 (27.5) P=0.614 df=4 Protestant 241 (64.3) 246 (68.0) 272 (68.7)
Other 14 (3.7) 10 (2.8) 15 (3.8)
Employment
Self-employed 183 (48.8%) 182 (50.3%) 188 (47.5%) P=0.079 df=4 Employed 160 (42.7) 147 (40.6) 189 (47.7)
Unemployed 32 (8.5) 33 (9.1) 19 (4.8)
Marital status
Cohabitating 41 (10.9%) 43 (11.9%) 42 (10.6%) P= 0.842 df=2 Currently married 334 (88.8) 319 (87.8) 354 (89.4)
Age
18-34 273 (72.8%) 268 (74.0%) 272 (68.7%) P=0.4042 df=2 35 and above 96 (25.6%) 92 (25.4%) 114 (28.8%)
4.2.3: Demographic characteristics of men who reported testing
44
Table 4.23: Demographic Characteristics of Males tested for HIV (N=566)
Characteristics Arm 1 (N=106)
Arm 2 (N=133)
Arm 3 (N=327)
²test P value
Level of Education
Primary 37 (34.9%) 39 (29.3%) 103 (31.5%) P=0.652;df=2 Secondary 69 (65.1) 94 (70.7) 224 (68.5)
Religion
Catholic 27 (25.5%) 45 (33.8%) 89 (27.2%) P=0.476;df=4 Protestant 77 (72.6) 84 (63.2) 226 (69.1)
Other 2 (1.9) 4 (3.0) 12 (3.7) Employment status
Self-employed 55 (51.9) 70 (52.6) 151 (46.2) P=0.283;df=4 Employed 43 (40.6) 55 (41.4) 162 (49.5)
Unemployed 8 (7.5) 8 (6.0) 14 (4.3) Marital status
Cohabitating 6 (5.7) 12 (9.0) 35 (10.7) P=0.298;df=2 Currently
Married
100 (94.3) 121 (91) 292 (89.3)
Age group
18-34 80 (75.5) 104 (78.2) 220 (67.3) P=0.087;df=2 35 and above 26 (23.6) 29 (21.8) 107 (30.3)
4.3: HIV self-testing acceptability rates among male partners
45
Table 4.24: Males recruited, accepted testing and those who refused or did not test
Arm 1 Number (%)
Arm 2 Number (%)
Arm 3 Number (%)
Total
Males recruited into the study
375 262 396 1033
Males who reported accepting testing
106 (28%) 133(37%) 327(83%) 566
Males who did not test or refused to test
269 (72%) 229 (53%) 69 (17%) 567
4.3.1: Males testing history across the three study arms
46
Table 4.25: Males testing history
Ever tested for HIV Arm 1 Arm 2 Arm 3 ²Test P value
Yes 314 (84%) 311 (86%) 365 (92%)
0.009
No 61 (16%) 51 (14%) 31 (8%)
Total 375 (100) 362 (100) 396 (100)
When was the last HIV test
Less than 3 months 67 (21%) 106 (34%) 174 (48%)
<0.001*
3-5 months ago 44 (14%) 47 (15%) 87 (24%)
6-11 months ago 42 (13%) 30 (10%) 25 (7%)
1-2 years ago 79 (25%) 65 (21%) 31 (9%)
More than 2 years 78 (25%) 59 (19%) 47 (13%)
Don't know 4 (1.3%) 3 (1.0%) 1 (0.3%)
Total 314 (100%) 310 (100%) 365 (100%)
A three-month follow-up questionnaire was administered to assess whether the men reported testing for HIV during the follow-up period, and details of testing behavior. The Table4.8 showed that 82.6% of the men in the self-testing arm tested for HIV in the three study months compared to only 37.0% in arm two and 28.3% in the standard control arm (Arm 1).
Table 4.26: the proportions (%) of men who reported testing for HIV in the 3-month follow-up period
Arm 1
(N=375)
Arm 2 (N=362)
Arm 3 (N=396) Tested for HIV in the last three months 106 (28.3) 133 (36.7) 327 (82.6) T test P-value for the comparisons 0.01* <0.001** * two sided proportions test comparing Arm 1 and Arm 2
47
4.3.2 Male testing against the demographic characteristics of the ANC partner Tables4.9 - 4.11: below illustrates the relationship between the male testing and the demographic characteristics of women in each study arm. In arm one (control), Marital status (P< 0.001), and wealth status (P< 0.001) played a significant role in determining male partner testing.
Table 4.27: Demographic Characteristics Arm 1
Not tested N (%) Tested N (%) ²Test P value
Religion
Catholic 49 (69) 22 (31) 0.201
Protestant 239 (72) 91(28)
Other 4 (80) 1(20)
Age (years)
18-34 265 (71) 106 (29) 0.601
≥ 35 27 (77) 8 (23)
Employment
Self-employed 96 (71) 40 (29) 0.273
Employed 36 (64) 20 (36)
Unemployed 160 (75) 54 (25)
Level of Education
Primary 173 (71) 70 (29) 0.775
Secondary 119 (73) 44 (27)
Marital status
Single 5 (100) 0 (0) < 0.001
Cohabitating 45 (82) 10 (18) Currently married 242 (70) 104 (30)
Wealth status
Wealth 1 48 (50) 47 (50) < 0.001 Wealth 2 60 (62) 37 (38)
Wealth 3 88 (82) 19 (18) Wealth 4 96 (90) 11 (10)
48
Table 4.28: Demographic characteristics Arm 2
Not tested (%) Tested (%)
²test P-value
Religion
Catholic 56 (66) 29 (43) 0.162
Protestant 187 (63) 108 (37)
Other 2 (29) 5 (71)
Age (years)
18-34 220 (62) 126 (38) 0.087
≥ 35 25 (81) 6 (19)
Employment
Self-employed 84 (64) 48 (36)
Employed 34 (56) 27 (44) 0.387
Unemployed 127 (66) 67 (34)
Level of Education
Primary 157 (68) 74 (32) 0.027
Secondary 88 (56) 68 (44)
Marital status
Single 5 (71) 2 (29) 0.846
Cohabitating 24 (61) 16 (39)
Currently married 215 (63) 124 (37)
Wealth status
Wealth 1 45 (52) 41 (48) 0.005
Wealth 2 61 (60) 40 (40)
Wealth 3 61 (62) 37 (38)
Wealth 4 78 (77) 24 (23)
49
Table 4.29: Demographic characteristics Arm 3
Not tested (%) Tested (%)
²test P-values
Religion
Catholic 21 (23) 70 (77) 0.315
Protestant 64 (20) 262 (80)
Other 2 (40) 3 (60)
Age (years)
18-34 72 (19) 305 (81) 0.041
≥ 35 15 (33) 30 (67)
Employment
Self-employed 30 (24) 97 (76) 0.493
Employed 12 (17) 60 (83)
Unemployed 45 (20) 178 (80)
Level of Education
Primary 46 (21) 177 (79) 0.894
Secondary 41 (21) 158 (79)
Marital status
Single 1 (13) 7 (87) 0.125
Cohabitating 5 (10) 44 (90)
Currently married 81 (22) 284 (78)
Wealth status
Wealth 1 19 (16) 100 (84) 0.160
Wealth 2 19 (18) 89 (82)
Wealth 3 27 (27) 72 (73)
Wealth 4 22 (23) 74 (77)
50
had primary education. The wealthier the ANC woman was, the less likelihood of testing by their male partners was as shown in Table 4.12 below
Table 4.30: Determinants of HIV testing among male partners
Un-Adjusted Adjusted
Odds ratio 95% CI Odds ratio 95% CI Age
18-24 1.00 1.00
25-34 1.16 0.72 1.88 0.99 0.57 1.69
>=35 1.31 0.63 2.73 0.55 2.42
Study arm
Arm 1 1.00 1.00
Arm 2 1.58 1.19 0.57 1.58 1.25 2.00
Arm 3 11.86 7.00 20.10 12.45 7.35 21.08
Employment
Employed 1.00 1.00
Un-Employed 0.63 0.40 1.01 1.09 0.56 2.02
Self-Employed 0.87 0.64 1.16 1.09 0.88 1.35
Religion
Catholic 1.00 1.00
Other 1.19 0.72 1.98 1.21 0.68 2.15
Protestant 1.17 1.02 1.35 1.04 0.88 1.23
Wealth Index
wealth 1 1.00 1.00
wealth 2 0.70 0.49 1.00 0.84 0.53 1.31
Wealth 3 0.49 0.32 0.75 0.64 0.37 1.13
wealth 4 0.42 0.24 0.76 0.57 0.28 1.14
Education
Primary 1.00 1.00
Secondary ( and above) 2.21 1.76 2.76 2.05 1.74 2.42
4.4: Effectiveness of HIV oral self-testing kit and improved invitation letter in increasing couple testing rates
51
tested in arms two and one, respectively as shown in Figure 4.1 below
Figure 3: Percentage of women who reported discussing HIV and testing with their partners
The ANC client and their partners were separately asked if they had tested together or knew whether their partner had tested. As shown in tables 4.13- 4.15 below, there is a strong agreement as reported by both respondents from Cohen’s Kappa statistical analysis (P-value < 0.001). The Tables below showed a strong agreement in all the three arms as shown by the Kappa agreement statistical analysis. Table 14.13below illustrated test of agreement between men and women who both reported that the man
13
395 298
110
16
371 251
136
9
413 88
334
No Yes No Yes
Dis
cuss
ed
HIV
testing
w
ith
Partner
Tested
tog
ether w
ith
Par
tn
er
Women who reported discussing HIV and testing with their partners
52
tested. In arm one, men who reported that they tested and their women reported that the men tested were 97 (92%) (P< 0.001). Also, six women (2.3%) reported that man tested and these men did not report that they tested. A total of eight (8%) men reported that they tested whereas the women denied it.
Table 4.31: Test of agreement on testing by ANC client and male partner enrolled in arm one.
Man reported that he tested test of agreement (Cohen’s Kappa statistics) 0.90 (0.86 - 0.95) P-value < 0.001
Woman report that man tested
YES NO Total
Woman reported that man tested
YES 97 (92%)
6 (2.3%) 103
NO 8
(8%)
255 (86%)
263
Total 105 261 366
Similarly, Table 14indicated a strong test of agreement (P< 0.001) between men and women who both reported that the man tested. In arm two, men who reported that they tested and women who reported that man tested were 115 (87%). Thirteen (6%) women reported that man tested while these men did not report so. A total of 17(13%) men reported that they tested and the women did not report so.
Table 4.32: Test of agreement on testing by ANC client and male partner enrolled in arm two
Man reported that he tested test of agreement (Cohen’s Kappa statistics) 0.87 (0.81 – 0.92)P-value < 0.001 Woman report that man tested
YES NO Total
Woman reported that man tested
YES 115
(87%) 13
(6%)
128
NO 17
(13%) 207
(94%) 224