_____________________________________________________________________________________________________ www.sciencedomain.org
Assessment of Left Ventricular Diastolic Function
Morbidity in Chronic Obstructive Lung Disease in
Population of West Bengal
Jayanta Kr. Mallick
1, Kaushik Ghosh
2*, Sanat Kumar Jatua
3,
Ambarish Bhattacharya
4, Sisir Chakraborty
5, Kabita Dabadi
6,
Susmita Ghosh
7and Mrinal Pal
81
Department of Pulmonary Medicine, Nilratan Sircar Medical College, Kolkata, W.B. PIN- 700014, India. 2
Department of Medicine, Burdwan Medical College, Burdwan, W.B., India. 3
Department of Medicine, Nilratan Sircar Medical College, Kolkata, W.B. PIN- 700014, India. 4
Visiting Consultant, Charnock Hospital, Kolkata 7000157, India. 5
Department of Medicine, College of Medicine and Sagore Dutta Hospital, Kolkata, India. 6
Consultant Pathologist, Dr. Lals Path Lab, Kolkata, India. 7
Department of Anaesthesiology, Murshidabad Medical College, Berhampore, India. 8
Department of Biochemistry, Burdwan Medical College, Burdwan, W.B., India.
Authors’ contributions
This work was carried out in collaboration between all authors. Authors JKM, KG and MP designed the study, wrote the protocol and wrote the first draft of the manuscript. Authors SKJ and SG managed the literature searches, analyses of the study performed the spectroscopy analysis and authors MP, AB, SC and KD managed the experimental process. All authors read and approved the final manuscript.
Article Information
DOI: 10.9734/BJMMR/2016/20607 Editor(s): (1) Valeria Denninghoff, Molecular Pathology and Molecular Onco-Hemathology laboratory,
University Institute CEMIC, Argentina. (2)S. U. Fuhong, ICU Laboratory, Erasme Hospital, Free University Brussels, Brussels, Belgium. (3)Philippe E. Spiess, Department of Genitourinary Oncology, Moffitt Cancer Center, USA and Department of Urology and Department of Oncologic Sciences (Joint Appointment), College of Medicine, University of South Florida, Tampa, FL, USA. Reviewers: (1) Anonymous, Aalborg University, Denmark. (2)Lei Xu, Capital Medical University, China. (3)Mra Aye, Melaka Medical Manipal College, Malaysia. (4)Andrea Borghini, IFC-CNR Institute of Clinical Physiology, CNR, Pisa, Italy. (5)Anonymous, University of São Paulo, SP, Brazil. Complete Peer review History:http://sciencedomain.org/review-history/12473
ABSTRACT
Introduction: Right ventricular dysfunction is a well known complication or association of Chronic
obstructive pulmonary disease (COPD). Only recently the association of Left ventricular dysfunction with COPD has gained importance. Whether this is an independent co-morbidity or a consequence of the COPD is yet to be clearly ascertained but more and more studies are showing Left ventricular dysfunction to be present in patients with COPD.
Materials and Methods: We conducted a pilot study in our institutes with 50 patients in our
institution. This was an observational Cross sectional study where patients were diagnosed and classified according to GOLD criteria.
Results: We found Left Ventricle (LV) dysfunction in about 84% of these patients. Systolic and
diastolic dysfunctions were present in 2% cases. Patient’s presenting age, duration and stage of the disease has significant positive correlation with left ventricular diastolic dysfunction.
Conclusion: Treatment of this Left ventricular dysfunction was absolutely necessary in the holistic
treatment of the patient as left ventricular dysfunction has an independent detrimental effect in COPD patients. As such, we recommend that all COPD patients should have an Echocardiography on first presentation.
Keywords: COPD; GOLD criteria; LV dysfunction; Co-morbidity.
1. INTRODUCTION
COPD or Chronic obstructive lung disease (COLD) is a pulmonary condition which is characterized by airflow limitation which is not fully reversible and the airflow limitation is usually progressive in nature [1]. It is a major cause of chronic morbidity and mortality worldwide. World Health Organization (WHO) predicted that COPD will be the third leading cause of mortality and fifth leading cause of morbidity by 2020 [2].
Chronic hypoxia in COPD leads to secondary pulmonary arterial hypertension (PAH) and right ventricular hypertrophy or ‘ cor-pulmonale’ and ultimately right heart failure. Although, left ventricular (LV) dysfunction has been observed by several authors, treating physicians and pulmonologists suspect associated LV dysfunction o n l y when a COPD patient fails to respond to bronchodilators and antibiotics or there is a disproportionate dyspnoea. Already existent but undocumented Left Ventricular (LV) dysfunction secondary to ischemic heart disease (IHD), is probably high in COPD patients because they share many of the risk factors such as age, male pr edom inan ce, cigarette smoking, etc. [3]. Other factors such as hypoxia, and hyper-viscosity of blood secondary to polycythemia and shifting of inter-ventricular septum towards left side may also contribute to the LV dysfunction.
It is difficult to distinguish between these disorders clinically, as produce paroxysmal
nocturnal dyspnea (PND), orthopnea and cough. Radiographical findings of pulmonary congestion and cardiomegaly may be obscured by barrel chest and hyper-inflated lungs. Although Brain natriuretic peptide (BNP) and amino terminal pro-BNP have been used to identify heart failure [4-6] However, BNP secretion might be secondary to both left ventricular stress as well as right ventricular stress [7]. Evidence of airway obstruction and a broncho-dialator response on pulmonary function test (PFT) is found not only in COPD, but also to some extent in acute congestive cardiac failure [8,9].
Hence, echocardiography is essential for objectively quantifying the cardiac status, but sadly it is not universally available. There is also lack of awareness of the co-existence of these entities amongst the primary care physicians and some Pulmonologists. So, the purpose of our study w as to assess left ventricular function in COPD patient without previous history of cardiac disease.
2. MATERIALS AND METHODS
2.1 Study Area
2.2 Selection of Subjects
A total of 152 patients with a diagnosis of COPD aged minimum 30 years who attended Nil Ratan Sircar Medical College and Hospital were screened as case and out of them finally 50 cases of stable COPD patients were included in the study. Stable uncomplicated COPD cases without any pre existing cardiac diseases evident on history, clinical examination or relevant investigations were finally included in the study. Patients with apparent cardiac disease like hypertension, ischemic heart disease, valvular heart disease, congenital heart disease, suffering from arrhythmia or poor echogenic window on echocardiography were excluded. All patients were examined and structured interview was performed. In short, such as respiratory symptoms including cough with phlegm and dyspnea were reported through self completed pre validated questionnaire [10]. Information about smoking habits, comorbidities, medication use and exacerbations was gathered. All subjects with suspicious or diagnosis of autoimmune diseases, asthma or cancer in the last 5 years was excluded from the study but subject with common comorbidities including cardiovascular diseases and diabetes were not excluded. A smoking history of ≥10 pack-years and a FEV1/FVC ratio < 0.7 and FEV1 < 80% predicted were criteria for inclusion [11].
2.3 Exacerbation Identification
Every 3 months patients were reviewed in the outpatient clinic and their diary cards collected. Previously accepted criteria of exacerbations are as follows [11,12].
Major Criteria: Increase in dyspnoea, sputum purulence or sputum volume, Minor criteria: Increase in nasal discharge, wheeze, sore throat, cough or fever. Symptom pattern persists for minimum two consecutive days, either two or more major symptoms or one major with anyone of the minor symptoms was considered as exacerbation of COPD. Then annual exacerbation rate of each patient was calculated by dividing the number of exacerbations bythe number of days they participated in the study, and multiplying by 365 and classify the exacerbators in two, frequent and infrequent exacerbators. Frequent exacerbators are those who are having ≥2 exacerbations treated with antibiotics and / or oral steroids and/or hospitalization the last 12 months and infrequent exacerbator are having <2 exacerbations.
2.4 Pulmonary Function Tests
Pulmonary function was measured both pre-and post-inhalation of 0.4 mg salbutamol, on aspirometer (HELIOS 401) by trained study staff. As the FEV1 is the most reproducible lung function test parameter therefore is best adopted to assessment of large group of people. Presence of COPD was defined by a post bronchodilator FEV1/FVC ratio <0.7 and severity of disease was staged by FEV1 expressed as percentage of Forced Vital Capacity (FVC), predicted according to the latest GOLD (Global Initiative for Obstructive Lung Disease) Classification [1,11].
2.5 Anthropometric Measurements
Weight and height measurements were obtained, using the Rosscraft Tom Kit Anthropometric Instrument Set, Canada (12). BMI was calculated as the weight in kilograms divided by the square of height in meters. Body mass index (BMI) was calculated as the weight (kg) divided by the square of height (m2), and was categorized as underweight (BMI <18.5), normal (BMI 18.5– 24.99), overweight (BMI 25.0–29.99), and obese (BMI 30.0 or more) according to the current World Health Organization (WHO) classification.
2.6 For estimation of Cardiological Status
The study populations were then subjected to echocardiography for detection of left ventricular systolic and diastolic function. The parameters recorded during echocardiographic study were:
To assess systolic function- Ejection Fraction (EF %) [Normal 55%-85%], any wall motion abnormality
To assess diastolic function-- Early rapid
filling phage /late rapid filling phase (E/A) [Normal -1-1.5]
Deceleration time (DT) (Normal -160-240ms) & Isovolumetric relaxation time(IVRT) [Normal -70-90 ms].
2.7 Statistical Analysis
3. RESULTS
We conducted a observational cross sectional study to assess the left ventricular function in COPD patients without any apparent cardiac disease or history of cardiac disease. 50 patients diagnosed as COPD (GOLD criteria) between the ages of 30 and 65 years were recruited into the study.
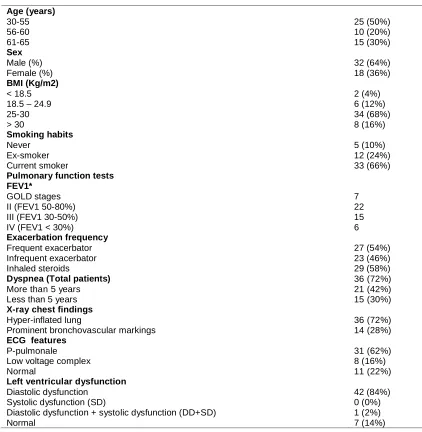
Table 1 show the age and sex distribution of all patients. Dyspnoea (72%) and cough (28%) were the main symptoms (Table 2). Other symptoms included expectoration (22% cases), chest tightness (16% cases), fever (42% cases)
and wheezing (36% cases). Long standing dyspnoea (for more than 5years) was found in 2 1 (42%) cases. Cough for more than 5yrs was found in 6 (12%) cases. Severity of the disease was classified according to GOLD criteria (Table 1). Majority of the patients were in stage II and III (74%). Probably due to lack of awareness of early symptoms of COPD, stage I COPD was missed and we got less number of patients in that stage of disease. We incorporated less number of patients in stage IV as most of patients had poor echo-window.
ECG findings of patients in our study were depicted in Table 1. P-pulmonale was found in
Table 1. Personal profile and clinical details of patients suffering from COPD
Age (years)
30-55 56-60 61-65
25 (50%) 10 (20%) 15 (30%)
Sex
Male (%) Female (%)
32 (64%) 18 (36%)
BMI (Kg/m2)
< 18.5 18.5 – 24.9 25-30 > 30
2 (4%) 6 (12%) 34 (68%) 8 (16%)
Smoking habits
Never Ex-smoker Current smoker
5 (10%) 12 (24%) 33 (66%)
Pulmonary function tests FEV1*
GOLD stages II (FEV1 50-80%) III (FEV1 30-50%) IV (FEV1 < 30%)
7 22 15 6
Exacerbation frequency
Frequent exacerbator Infrequent exacerbator
27 (54%) 23 (46%)
Inhaled steroids 29 (58%)
Dyspnea (Total patients)
More than 5 years Less than 5 years
36 (72%) 21 (42%) 15 (30%)
X-ray chest findings
Hyper-inflated lung
Prominent bronchovascular markings
36 (72%) 14 (28%)
ECG features
P-pulmonale Low voltage complex Normal
31 (62%) 8 (16%) 11 (22%)
Left ventricular dysfunction
Diastolic dysfunction Systolic dysfunction (SD)
Diastolic dysfunction + systolic dysfunction (DD+SD) Normal
31(62%) cases, low voltage complex was found in 8(16%) cases, right bundle brunch block pattern was noted in (4,8%) and ECG picture of right ventricular hypertrophy was observed in (1, 2%) case. In 11 (22%) cases ECG was normal. P-pulmonale was the predominant ECG finding in our study, and that signified right atrial enlargement as a result of RV hypertrophy secondary to pulmonary arterial hypertension in COPD.
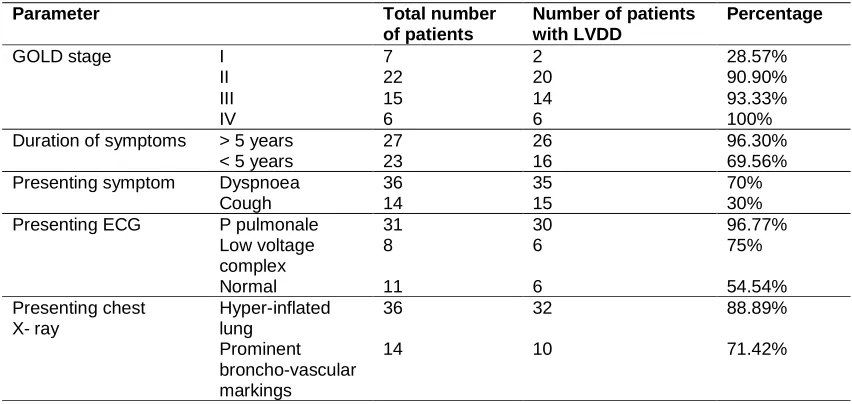
Echocardiography was performed in all cases and the findings were depicted in Table 2. Left ventricular diastolic dysfunction was noted in 42(84%) cases, both systolic and diastolic dysfunction was recorded in one (2%) case and isolated systolic dysfunction was not found in any case. Seven patients had normal echocardiography. Diastolic dysfunction was predominant echocardiographic finding. We did not get isolated systolic dysfunction as we excluded diseases that cause systolic dysfunction of LV from the study population.
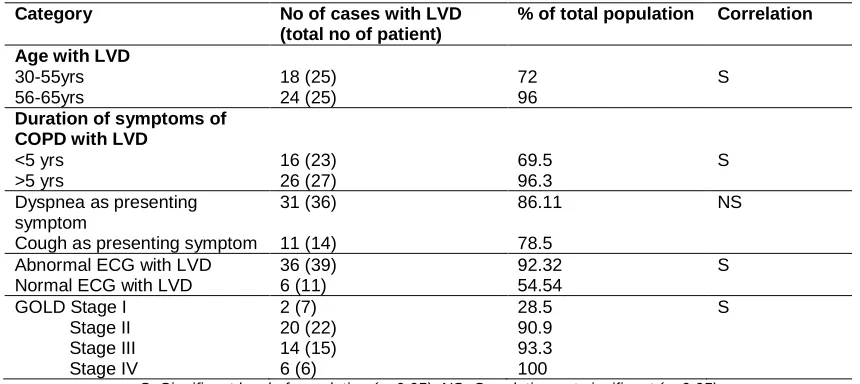
We analyzed the correlation between age of the patients and the prevalence of LV diastolic dysfunction. Between 50 to 55 yrs of age LV diastolic dysfunction was observed in 18 out of 25(72%) cases, whereas it was 24 out of 25 (96%) in 56 to 65 yrs age groups. There was statistically significant correlation exists between the age of patients and the prevalence of LV diastolic dysfunction. We analyzed the correlation between duration of symptoms of
the patients and prevalence of diastolic dysfunction and that was depicted in Table-3. Less than 5 years duration group the prevalence of LV diastolic dysfunction was 16 out of 23 cases (69.56%) and that was 96.30% (26 out of 27 cases) in patients with symptoms more than 5 years. There was a statistically significant correlation between the duration of illness and the prevalence of LV diastolic dysfunction.
LV diastolic dysfunction was found in 86.11% (31 out of 36) patients presenting with dyspnea and 78.57% (11 out of 14) patients presented with cough. We did not find any statistical significant association between symptoms nature and diastolic dysfunction. LV dysfunction was found in 96.77% (30 out of 31) patients with p-pulmonale in ECG and 75% (6 out of 8) patients with low voltage complex in ECG had LV diastolic dysfunction. On the other hand 54.54% (6 out of 11) patients with normal ECG had LV dysfunction. There was statistical significant correlation between abnormal ECG findings and LV dysfunction. The correlation between staging of COPD and prevalence of diastolic dysfunction.
In stage 1 COPD the prevalence of LV diastolic dysfunction was 28.57% (2 out of 7 patients), 90.90% (20 out of 22 patients) in stage II COPD, 93.33% (14 out of 15patients) in stage III COPD
and 100% (6 out of 6 patients) in stage IV COPD. So, there was a statistically highly
Table 2. Table showing the proportion of LVDD with respect to different study parameters
Parameter Total number
of patients
Number of patients with LVDD
Percentage
GOLD stage I 7 2 28.57%
II 22 20 90.90%
III 15 14 93.33%
IV 6 6 100%
Duration of symptoms > 5 years 27 26 96.30%
< 5 years 23 16 69.56%
Presenting symptom Dyspnoea 36 35 70%
Cough 14 15 30%
Presenting ECG P pulmonale 31 30 96.77%
Low voltage complex
8 6 75%
Normal 11 6 54.54%
Presenting chest
X-ray
Hyper-inflated lung
36 32 88.89%
Prominent broncho-vascular markings
Table 3. Summery of statistical analysis
Category No of cases with LVD
(total no of patient)
% of total population Correlation
Age with LVD
30-55yrs 56-65yrs
18 (25) 24 (25)
72 96
S
Duration of symptoms of COPD with LVD
<5 yrs >5 yrs
16 (23) 26 (27)
69.5 96.3
S
Dyspnea as presenting symptom
Cough as presenting symptom
31 (36)
11 (14)
86.11
78.5
NS
Abnormal ECG with LVD Normal ECG with LVD
36 (39) 6 (11)
92.32 54.54
S
GOLD Stage I Stage II Stage III Stage IV
2 (7) 20 (22) 14 (15) 6 (6)
28.5 90.9 93.3 100
S
S=Significant level of correlation (p<0.05); NS=Correlation not significant (p>0.05) significant correlation between the staging of
COPD and the prevalence of LV diastolic dysfunction. We analyzed the correlation between radiological finding of chest and the prevalence of LV diastolic dysfunction. Radiological findings of LV diastolic dysfunction was observed in 32 out of 36 (88.89%) cases with hyper-inflated lung in CXR, whereas it was10 out of 14(71.42%) in patients with prominent broncho-vascular marking in CXR. T here was no significant relation between chest x-ray findings and LV diastolic dysfunction.
4. DISCUSSION
We assessed left ventricular function in COPD patients and have found that majority of them have statistically significant LVDD (p<0.05). We also found that dyspnoea was the most predominant presenting symptom. Some studies have indicated a weak relationship between dyspnoea and disease severity (FEV1, VEF) with left ventricular ejection fraction but others did not find any such correlation [10,13]. We too did not find any significant association between dyspnoea and LV diastolic dysfunction (p>0.05) [13,14].
There are publications reporting that COPD patients died due to cardiovascular complications especially in patients younger than 65 years [15]. Funk GC et al. reported that “the maximal atrial filling velocity was increased and the early filling velocity was decreased in patients with COPD compared to control subjects” [16]. The atrial contribution to total
left diastolic filling was increased in patients with COPD even in patients with normal pulmonary artery pressure(PAP) not to mention those with higher PAP.
We found that E/A ratio were markedly decreased in patients with COPD along with increased values of DT and IVRT. We found a significant correlation between the occurrence of P-pulmonale and LV diastolic dysfunction (p<0.05). This indirectly proved that there was a further increased atrial contribution to total left diastolic filling in COPD patients. This is just an observation of the study. Several studies have indicated that the interaction between chronic obstructive pulmonary disease (COPD) and cardiovascular comorbidity is complex and bidirectional. Although cardiac abnormalities in COPD have been mainly with the right ventricle,
several studies have reported that the left ventricle may also be affected in this disease [17].
We observed that there was increased prevalence of LV diastolic dysfunction in our subset of patients, but only one patient had systolic dysfunction which was not significant statistically. LV diastolic dysfunction was also more commonly seen in stable COPD patients. Poddar et al.reported parameters of LV systolic function like EF were depressed in patients of COPD with cor-pulmonale [24,25]. However, we did not find any such co-relation. A definite correlation of LV diastolic dysfunction and the age was found in patients with LV diastolic dysfunction. However, age-related myocardial changes are known to occur in even in normal individuals [26].
LV diastolic dysfunction was significantly (p<0.05) more prevalent in our study in patients whose duration of symptoms was more than 5 years. It was also found to be more prevalent in those who presented with predominant dyspnoea. However, statistical analysis failed to show any significant association between symptom nature and LV diastolic dysfunction (p>0.05). Another important observation in our study was that LV diastolic dysfunction was significantly more marked in the advanced stage of COPD ( GOLD stage IV) than in early stage of the disease (GOLD stage I). Higher percentage of pulmonary hypertension and right ventricular strain by the virtue of inter-ventricular dependence in advanced COPD was the probable responsible factor.
4.1 Short-comings of the Study
We got less number of patients in stage I probably due to lack of awareness of early symptoms of COPD by both the patients as well as their primary physicians.
We incorporated less number of patients in stage IV as most of patients were too unstable to be enrolled and had poor echo-window.
We could not establish the cause of systolic dysfunction in one patient as cardiac catheterization, coronary angiography or myocardial biopsy were necessary but these procedures were not included in our study.
5. SUMMARY AND CONCLUSION
We concluded that there was a definite association between LV diastolic dysfunction and COPD. Although cardiac abnormalities in COPD have been mainly with the right ventricle,
several studies have reported that the left ventricle may also be affected in this disease. Increasing age is an independent factor for developing LVD. However, further studies with larger population groups are necessary to prove COPD as a cause of LV diastolic dysfunction.
CONSENT
All authors declare that ‘written informed consent was obtained from the patient (or other approved parties) for publication of this case report and accompanying images.
COMPETING INTERESTS
Authors have declared that no competing interests exist.
REFERENCES
1. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532-55.
2. Murray C, Lopez A. Evidence-based health policy-lessons from the global burden of disease study. Science. 1996;274(5288): 740-743.
3. World Health Report. Geneva: World Health Organisation; 2000.
Available:http://www.who.int/whr/2000/en/s tatistics.htm
4. Sin D, McAlister F, Man S, et al. Contemporary management of chronic obstructive pulmonary disease. JAMA. 2003;290(17):2301, 290:2301-2312. 5. Maisel A, Hollander J, Guss D, et al.
1001-25 Primary results of the rapid emergency department heart failure outpatient trial (REDHOT): A multicenter trial examining B-type natriuretic peptide levels, emergency physician decision making and outcomes in patients presenting with shortness of breath. Journal of the American College of Cardiology. 2004; 43(5):A6-A7.
6. Maisel A, Krishnaswamy P, Nowak R, et al. Rapid Measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. New England Journal of Medicine. 2002;347(3):161-167.
Investigation of Dyspnea in the Emergency department (PRIDE) study. The American Journal of Cardiology. 2005;95(8):948-954. 8. Light R. Serial pulmonary function in
patients with acute heart failure. Arch Intern Med. 1983;143(3):429.
9. Cabanes L, Weber S, Matran R, et al. Bronchial hyperresponsiveness to methacholine in patients with impaired left ventricular function. New England Journal of Medicine. 1989;320(20):1317-1322. 10. Eagan TM, Ueland T, Wagner PD, Hardie
JA, Mollnes TE, et al. Systemic inflammatory markers in COPD: Results from the Bergen COPD cohort study. Eur Respir J. 2010;35:540–548.
11. Pal M, Datta S, Mitra R, Malik T, Ghosh S. Association of vitamin d status in chronic Obstructive pulmonary diseases and its Explanatory variables in Burdwan. World Journal of Pharmaceutical Research. 2013;3(1):658-674.
12. Deepa M, Pradeepa R, Rema M, Mohan A, Deepa R, Shanthi Rani S, et al. The Chennai urban rural epidemiology study (CURES): Study design and Methodolgy (Urbancomponent) CURES -1 J. Assoc.
Physicians India. 2003;51:863-870. 13. Arnold R, Ranchor A, Koëter G, et al.
Consequences of chronic obstructive pulmonary disease and chronic heart failure: The relationship between objective and subjective health. Social Science & Medicine. 2005;61(10):2144-2154. 14. Rector TS, Anand IS, Cohn JN. Effect of
inhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary disease. New England Journal of Medicine. 2000;343(26):1902-1909. 15. Wijnhoven H. Determinants of different
dimensions of disease severity in asthma and COPD. Chest. 2001;119(4):1034. 16. Herlitz J, Wiklund I, Sjöland H, et al. Relief
of symptoms and improvement of health-related quality of life five years after coronary artery bypass graft in women and men. Clin Cardiol. 2001;24(5):385-392.
17. Portillo K, Abad-Capa J, Ruiz-Manzano J. Enfermedad pulmonar obstructiva crónica y ventrículo izquierdo. Arch Bronconeumol. 2015;51:227–234.
18. Sidney S, Sorel M, Quesenberry CP, et al. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser permanente medical care program. Chest. 2005;128:2068–2075.
19. Funk GC, Lang I, Schenk P, Valipour A, et al. Left ventricular diastolic dysfunction in patients with COPD in the presence and absence of elevated pulmonary arterial pressure. Chest. 2008;133:1354–9. 20. Suchon E, Tracz W, Podolec P, et al.
Evaluation of left ventricular function in patients with chronic obstructive pulmonary disease. Pol Arch Med Wewn. 2007; 117(3); 26-30.
21. Gupta NK, Agrawal RK, Srivastav AB, et al. Echocardiographic evaluation of heart in chronic obstructive pulmonary disease patient and its co-relation with the severity of disease. Lung India. 2011; 28(2):105-9.
22. Render ML, Weinstein AS, Blaustein AS. Left ventricular dysfunction in deteriorating patients with chronic obstructive pulmonary disease. Chest. 1995;107:162–168. 23. Vizza CD, Lynch JP, Ochoa LL, et al. Right
and left ventricular dysfunction in patients with severe pulmonary disease. Chest. 1998;113:576–83.
24. Louridas G, Patakas D, Stavropoulos C. Left ventricular function in patients with chronic obstructive pulmonary disease. Cardiology. 1981;67:73–80.
25. Funk GC, Lang I, Schenk P, et al. Left ventricular diastolic dysfunction in patients with COPD in the presence and absence of elevated pulmonary arterial pressure. Chest. 2008;133:1354–9.
26. Poddar AK, Chakraborti BN, Ghosh JL, et al. Assessment of left ventricular function in patients of COPD. Ind J Tub. 1997;44:181.
_________________________________________________________________________________ © 2016 Mallick et al.; This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Peer-review history: