Int J Clin Exp Med 2016;9(8):15961-15966 www.ijcem.com /ISSN:1940-5901/IJCEM0031000
Original Article
Systematic evaluation of an animal model for maxillary
sinus floor elevation with immediate implant
Ji-Si Zheng1, Shan-Yong Zhang1, Chi Yang1, Yong-Dae Kwon2, Yong-Jin Kim3
1Department of Oral and Maxillofacial Surgery, Ninth People’s Hospital, Collage of Stomatology, Shanghai
Jiaotong University School of Medicine, and Shanghai Key Laboratory of Stomatology & Shanghai Research Institute of Stomatology, Shanghai, China; 2Department of Oral and Maxillofacial Surgery, College of Dentistry,
Kyung Hee University, South Korea; 3Department of Oral and Maxillofacial Surgery, Insan Apsun Dental Clinic,
South Korea
Received April 21, 2016; Accepted July 10, 2016; Epub August 15, 2016; Published August 30, 2016
Abstract: Objective: The goal of this study was to introduce and evaluate an animal model for maxillary sinus floor elevation with immediate implant placement. Materials and methods: Six beagles were included in our study. Computed tomography (CT) for all beagles was obtained and transformed into the Mimics 18.0 software preopera-tively. A section located between the first molar and the greater palatine foramen was selected to reach the sinus floor. All beagles had the sinus floor raised from this section. Then, the elevated spaces were filled with Bio-Oss. Finally, the implants were placed simultaneously. The initial stability, implant stability quotient (ISQ), postopera-tive CT, and histological observation were used to evaluate the animal model. The results were analyzed by the Wilcoxon signed rank test. Results: All lifting surgeries were successfully performed from the section without sinus membrane perforation. Initial stability of all implants ranged between 35 and 55 N·cm. The mean (SD) of ISQ intra-operatively and 3 months postintra-operatively were 65.3 (3.0) and 78.7 (2.7). There was a significant difference for ISQ (P < 0.0001). Immediate postoperative CT revealed that all implants were located in the middle of the sinus floor, and no peri-implant indication changes were noted in the 3 months postoperative CT. Histological analysis showed a 66.3% bone-implant contact (BIC) in situ. Conclusions: The mentioned section is a suitable surgical approach for sinus floor elevation and a stable implant placement area. Therefore, this is a favorable animal model for the sinus elevation with immediate implant placement.
Keywords: Maxillary sinus floor elevation, immediate implant, implant stability, beagle
Introduction
The main rehabilitation obstacle in the posteri-or region of the maxilla is the process of the maxillary posterior alveolar bone resorption that occurs after the loss of teeth, with later pneumatization of the maxillary sinus [1]. Researchers are conducting extensive preclini-cal base research in finding new techniques and materials for treating this obstacle on ani-mal models. Usually canines, sheep, pigs or rabbits serve as animal models for implants in the maxillary posterior teeth area [2-5]. Canines are considered as one of the commonest mod-els used for dental animal experiments, be- cause they are abundant in quantity, easy to keep, adaptable to their environment, durable, strong against infection, and have bigger oral clefts than the other models [2].
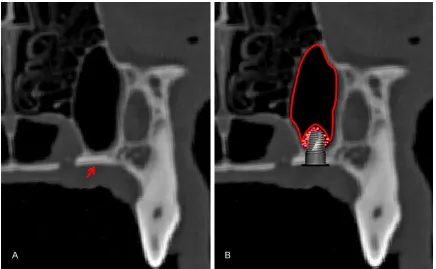
on the palatal side of the first maxillary molar distal cusp, and on the lateral area of the pala-tine foramen instead of the lateral bony wall of the sinus (Figure 1A). With this modified mini-mal invasive technique, extraction of the poste-rior teeth and the 3 months of tissue healing period are no longer required [9]. Therefore, the modified lifting surgery was more convenient for the research in the maxillary sinus area. Afterwards, our team used the endoscope to assist the lifting of the sinus membrane in this model, and confirmed that endoscopic lifting of the floor of the maxillary sinus is a safe and effective approach based on direct observation [10]. However, this study solely reported the process of modified maxillary sinus floor eleva-tion. No further details on whether implant could be placed simultaneously with surgical approach on the model are presented. There- fore, it is necessary to further confirm the pos-sibility of the model for maxillary sinus floor elevation with immediate implant placement (Figure 1B), which will also increase the indica-tions for the field of research of implant place-ment and new implant materials.
Materials and methods
Animals
6 healthy beagles, aged 18 months old, with an average weight of 13.4 Kg, were used in this study. This study was conducted in accordance with the Ethics Committee of Shanghai Jiao Tong University School of Medicine.
Surgical procedure
[image:2.612.89.525.70.339.2]A modified animal model for sinus lifting
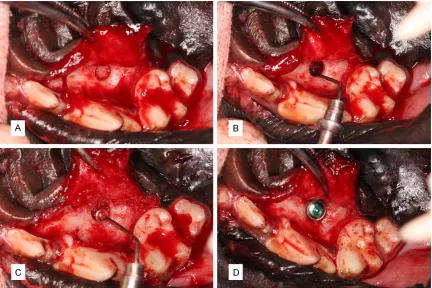
combination with a stopper in the Crestal Approach Sinus (CAS) kit (Osstem, Seoul, South Korea) (Figure 2A). Next, the membrane was elevated to 10 mm with the help of a sinus membrane elevator, which was designed and manufactured by the authors (Figure 2B). Afterwards, the elevated space was filled wi- th Bio-Oss (0.8 mL, Geistlich Biomaterials, Wolhusen, Switzerland) (Figure 2C), and the implant (4 × 8 mm, TS III, Osstem, South Korea) was placed from the section (Figure 2D). Finally, the full-thickness mucoperiosteal flap was repositioned and sutured. All beagles received penicillin for one day postoperatively and were kept on a soft diet during the first week after surgery in order to prevent postoperative infec-tions [9, 10].
Determination of the initial stability
The implant wrench was used to confirm the initial stability (IS) immediately after implant placement. The initial stability was recorded as follows: 1) IS ≤ 35 N·cm; 2) 35 N·cm < IS ≤ 55 N·cm; 3) IS > 55 N·cm.
Measurement of implant stability quotient
The implant stability quotient (ISQ) was mea-sured intraoperatively and 3 months postoper-atively (before the animal was to be put at rest) by using the Osstell® system (Integration Dia- gnostics, Goteborg, Sweden). Every ISQ was measured 3 times from the buccal and lingual sides, respectively [11, 12].
CT examination
[image:3.612.91.523.71.359.2]CT scans for all beagles were obtained with a 64-slice spiral imager (0.625-mm slice thick-ness) (Light Speed Ultra; General Electric, Millwaukee, WI) immediately and 3 months after surgery, to examine the implant position in the sinus floor and the bone contact between the implant and the bone in the sagittal image [9, 10].
Histological analysis
ly embedded in polymethymetacrylate (PMMA). The specimens were cut in 150 μm thick sec-tions using a microtome (Leica, Hamburg, Germany), and were subsequently ground and polished to a final thickness of about 40 μm. The cuts were further stained with Van Gieson’s picro fuchsin for histological analysis. Two ran-domly selected sections from each sample were analyzed for the bone-implant contact (BIC) ratio in the middle third of implant’s mesi-al and distmesi-al parts [8, 13].
Statistical analysis
Wilcoxon signed rank test in SPSS software package (version 16.0, Chicago, IL) was used to compare ISQ. A significant difference was set at P < 0.05.
Results
All beagles that survived the operations were healthy, and there were no implants loss during the entire period of observation with uneventful wound healing. The sinus floor was successfully raised from the section, and the intact sinus membrane could be observed during every surgery.
Initial stabilities of all implants were obtained between 35 and 55 N·cm. The mean (SD) of ISQ intraoperatively and 3 months postoperatively were 65.3 (3.0) and 78.7 (2.7). There was a sig-nificant difference for ISQ from intraoperatively to 3 months postoperatively (Z=1176.0, P <
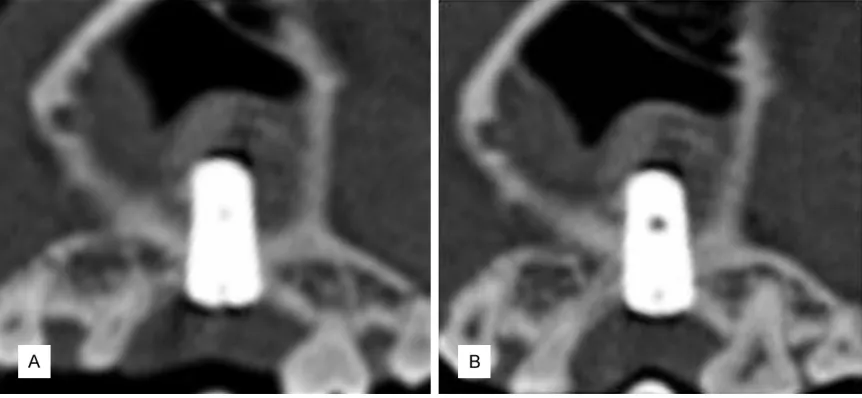
0.0001). Immediate postoperative CT revealed that all implants were located in the middle of the sinus floor (Figure 3A), and there were no peri-implant pathologic changes noted in the 3 months postoperative CT (Figure 3B). Histo- logical analysis showed favorable bone con-tacts between the implants and the autoge-neous or grafted bone, and there were 66.3% BIC in the middle third of implant (Figure 4).
Discussion
[image:4.612.91.522.72.271.2]A modified animal model for sinus lifting
performed the floor elevation of the maxillary sinus, grafted the bone materials, and placed the implant simultaneously to check the feasi-bility of the model. The measurements of the initial stability and ISQ showed that the placed implant can obtain favorable implant stability intraoperatively. The CT and histological analy-sis proved a successful bone-implant contact after healing.
From the results of the current study, we here-by present some possible explanations for achieving the implant stability. First, the bone in this region is a part of the palatal bone, not the alveolar bone; therefore the bone quality is very compact. Second, the bone of this section is bi-cortical bone, included the oral surface of palatal bone and the sinus floor, and the amount of the cortical bone is the decisive fac-tors for optimal implant stabilization. Third, the implant cavity was prepared into 3.5 mm, whereas the diameter of placed implant was 4.0 mm. The bone compression may support the implant stability. Forth, more blood applied from the maxilla may provide the basic needs for bone connection between the palatal bone and implant. Moreover, the new bone forma-tion in the grafted area may further increase
the success of the implant placement. Therefore, there is no worry that the implant placed in the section would be loss.
In fact, lots of researches showed that implants can be placed in alveolar bone with sever defi-ciencies in experiments or clinical trials. In prospective clinical series studies, most dis-cussed the relationship between the RBH and the height of the newly formed bone, or the implant survival rate in short or long terms fol-low up [14, 15]. Few studies evaluated the implant stability in less than 2 mm of the RBH in the posterior maxillary area. Fenner et al per-formed sinus floor augmentations with simulta-neous implant placements in mini pigs to evalu-ate the influences on the implant stability and osseointegration in the different RBH sections (including 2, 4, 6, and 8 mm). Although the implant stabilities in high RBH sections were better than in low RBH, the implants placed in 2 and 4 mm of the RBH also obtained suffici- ent stabilities, and the osseointegration and implant survival were not significantly affected [17, 18]. Urban et al compared the success and survival rate of implants (156 implants in total) placed following a staged approach in clinical scenarios with a minimal RBH (≤ 3.5 mm). Only one implant failed at the time of abutment placement, and three more failed after 5 years from abutment connection [19]. All of these confirmed the same results with this study. In conclusion, this model is not limited in prac-tice of maxillary sinus floor elevation surgical procedure or the study of new bone materials in sinus, but also unrestricted in used for new implant materials and bone connections between the implant and bone materials in the maxillary sinus region.
Acknowledgements
This study was partially supported by Osstem company in Korea. This study was supported by the Science and Technology Commission of Shanghai (No. 134119a5400), the National Natural Science Foundation (No. 81371668), and the Seventh College Students Innovation Training Program of Shanghai Jiao Tong University School of Medicine (No. 2013061).
Disclosure of conflict of interest
[image:5.612.89.291.69.339.2]None. Figure 4. Histological analysis showed favorable
Address correspondence to: Dr. Shan-Yong Zhang, Department of Oral and Maxillofacial Surgery, Ninth People’s Hospital, Collage of Stomatology, Shanghai Jiaotong University School of Medicine, and Shanghai Key Laboratory of Stomatology & Shanghai Research Institute of Stomatology, Shang- hai, China. E-mail: [email protected]; Dr. Yong-Dae Kwon, Department of Oral and Maxillofacial Surgery, College of Dentistry, Kyung Hee University, South Korea. E-mail: [email protected]; Dr. Yong-Jin Kim, Department of Oral and Maxillofacial Surgery, Insan Apsun Dental Clinic, South Korea. E-mail: [email protected]
References
[1] Wallace SS, Froum SJ. Effect of maxillary sinus floor augmentation on the survival of endosse-ous dental implants. A systematic review. Ann Periodontol 2003; 8: 328-343.
[2] Liu N, Sun F, Xu C, Lin T, Lu E. A comparative study of canine models forosteotome sinus floor elevation and dental implants in posterior max-illa subjacent to the maxillary sinus. Oral Surg Oral Med Oral Pathol Oral Radiol 2013; 115: e15-20.
[3] Estaca E, Cabezas J, Usón J, Sánchez-Margallo F, Morell E, Latorre R. Maxillary sinus-floor ele-vation: ananimal model. Clin Oral Implants Res 2008; 19: 1044-8.
[4] Zeng D, Xia L, Zhang W, et al. Maxillary sinus floor elevation usinga tissue-engineered bone with calcium-magnesium phosphate cement and bone marrow stromal cells in rabbits. Tissue Eng Part A 2012; 18: 870-81.
[5] Martini L, Fini M, Giavaresi G, Giardino R. Sheep model in orthopedic research: a litera-ture review. Comp Med 2001; 51: 292-9. [6] Kim HR, Choi BH, Xuan F, Jeong SM. The use
of autologous venous blood for maxillary sinus floor augmentation in conjunction with sinus membrane elevation: an experimental study. Clin Oral Implants Res 2010; 3: 346-9. [7] Wang S, Zhang Z, Xia L, Zhao J, Sun X, Zhang X,
Ye D, Uludağ H, Jiang X. Systematic evaluation of a tissue-engineered bone for maxillary sinus augmentation in large animal canine model. Bone 2010; 46: 91-100.
[8] Wetzel AC, Stich H, Caffesse RG. Bone apposi-tion onto oral implants in the sinus area filled with different grafting materials. A histological study in beagle canines. Clin Oral Implants Res 1995; 6: 155-63.
[9] Zheng J, Zhang S, Yang, Zhang W, Zhao J. Systematic modification and evaluation of an animal canine model for maxillary sinus floor elevation. Br J Oral Maxillofac Surg 2014; 52: 784-8.
[10] Zheng J, Zhang S, Yang, Zhang W, Zhao J. Endoscopic lift of the maxillary sinus floor in beagles. Br J Oral Maxillofac Surg 2014; 52: 845-9.
[11] Morita K, Doi K, Oue H, Kajihara S, Hayashi K, Akagawa Y. Influence of formalin fixation on the implant stability quotient and mechanical characteristics of bone. Br J Oral Maxillofac Surg 2013; 51: 550-4.
[12] da Silva Neto UT, Joly JC, Gehrke SA. Clinical analysis of the stability of dental implants after preparation of the setion by conventional drill-ing or piezosurgery. Br J Oral Maxillofac Surg 2014; 52: 149-53.
[13] Zhang W, Wang X, Wang S, Zhao J, Xu L, Zhu C, Zeng D, Chen J, Zhang Z, Kaplan DL, Jiang X. The use of injectablesonication-induced silk hydrogel for VEGF(165) and BMP-2 delivery for elevation of the maxillary sinus floor. Biomaterials 2011; 32: 9415-24.
[14] Emmerich D. Sinus floor elevation using osteo-tomes: a systematic review and meta-analysis. J Periodontol 2005; 76: 1237-51.
[15] Fugazotto PA. Treatment options for augmen-tation of the posterior maxilla. Implant Dent 2000; 9: 281-7.
[16] Misch CE. Maxillary sinus augmentation for endosteal implants: organized alternative treatment plans. Int J Oral Implantol 1987; 4: 49-8.
[17] Fenner M, Vairaktaris E, Fischer K, Schlegel KA, Neukam FW, Nkenke E. Influence of resid-ual alveolar bone height on osseointegration of implants in the maxilla: a pilot study. Clin Oral Implants Res 2009; 20: 555-9.
[18] Fenner M, Vairaktaris E, Stockmann P, Schlegel KA, Neukam FW, Nkenke E. Influence of resid-ual alveolar bone height on implant stability in the maxilla: an experimental animal study. Clin Oral Implants Res 2009; 20: 751-5.