Coronary Heart Disease
A Prospective Follow-Up Study of 14 786 Middle-Aged Men and
Women in Finland
Pekka Jousilahti, MD; Erkki Vartiainen, MD; Jaakko Tuomilehto, MD; Pekka Puska, MD
Background—Coronary heart disease (CHD) is markedly more common in men than in women. In both sexes, CHD risk
increases with age, but the increase is sharper in women. We analyzed the extent to which major cardiovascular risk factors can explain the sex difference and the age-related increase in CHD risk.
Methods and Results—The study cohort consists of 14 786 Finnish men and women 25 to 64 years old at baseline. The
following cardiovascular risk factors were determined: smoking, serum total cholesterol, HDL cholesterol, blood pressure, body mass index, and diabetes. Risk factor measurements were done in 1982 or 1987, and the cohorts were followed up until the end of 1994. The Cox proportional hazards model was used to assess the relation between risk factors and CHD risk. CHD incidence in men compared with women was'3 times higher and mortality was'5 times higher. Most of the risk factors were more favorable in women, but the sex difference in risk factor levels diminished with increasing age. Differences in risk factors between sexes, particularly in HDL cholesterol and smoking, explained nearly half of the difference in CHD risk between men and women. Differences in serum total cholesterol level, blood pressure, body mass index, and diabetes prevalence explained about one-third of the age-related increase in CHD risk among men and 50% to 60% among women.
Conclusions—Differences in major cardiovascular risk factors explained a substantial part of the sex difference in CHD
risk. An increase in risk factor levels was associated with the age-related increase in CHD incidence and mortality in both sexes but to a larger extent in women. (Circulation. 1999;99:1165-1172.)
Key Words: agingnepidemiologyncoronary diseasensexnrisk factors
T
here is a marked difference in coronary heart disease (CHD) risk between sexes.1– 8Among middle-agedpeo-ple, CHD is 2 to 5 times more common in men than in women, and this sex ratio varies between populations.8 In
both sexes, the risk of CHD increases markedly with age.1,5,7
Lipid abnormalities, high blood pressure, and smoking are major risk factors for CHD.9 –15 Obesity and diabetes also
contribute to CHD risk.16 –18The role of major cardiovascular
risk factors in the development of CHD is well established among men. Among women, the data are less extensive. Reasons for the sex difference in CHD risk are not fully understood. Even though in most populations, cardiovascular risk factor patterns are more favorable among women than among men,8 very limited data are available to assess the
extent to which cardiovascular risk factors can explain the observed sex difference in CHD risk.
The aim of this study was to assess (1) whether the association of smoking, total cholesterol, HDL cholesterol, HDL cholesterol/total cholesterol ratio, blood pressure, dia-betes, and obesity with CHD risk is similar in men and
women; (2) the extent to which differences in these risk factors can explain the sex difference in CHD incidence and mortality; and (3) how much the changes in the risk factor levels by aging explain the difference in CHD risk between age groups.
Methods
Participants and Surveys
Baseline surveys were carried out in North Karelia and Kuopio provinces in eastern Finland and in the Turku-Loimaa region in southwestern Finland in 1982 and 1987.19In both years, age- and
sex-stratified random samples were taken from the age group of 25 to 64 years according to the international World Health Organization (WHO) MONICA (Monitoring of Trends and Determinants in Cardiovascular Disease) project protocol.20In this study, the 1982
and 1987 cohorts were combined. The samples included 9789 men and 9538 women. The participation rate was 79% among men and 85% among women. The 168 subjects who participated in both surveys were included only in the 1982 survey cohort. Excluded were 261 subjects because of their previous history of myocardial infarction and 611 because of incomplete data on$1 risk factors.
Received April 30, 1998; revision received November 2, 1998; accepted November 18, 1998.
From the National Public Health Institute, Department of Epidemiology and Health Promotion, Helsinki, Finland.
Reprint requests to Dr Pekka Jousilahti, National Public Health Institute, Department of Epidemiology and Health Promotion, Mannerheimintie 166, FIN-00300 Helsinki, Finland. E-mail pekka.jousilahti@ktl.fi
© 1999 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org
1165
Thus, 7090 men and 7696 women were included in the present analyses.
Risk Factor Assessment
A self-administered questionnaire was sent to the participants in advance. Current smoking status was assessed by a set of standard-ized questions. At the study site, height, weight, and blood pressure were measured according to the WHO MONICA project protocol.20
Body mass index (BMI, kg/m2) was used as a measure of relative
body weight. Total and HDL cholesterol were determined from fresh serum samples by an enzymatic method (CHOD-PAP, Boehringer Mannheim). On the questionnaire, the subjects were asked to report the presence of diabetes. The data were complemented by informa-tion from the Social Insurance Instituinforma-tion’s register on persons receiving free-of-charge medication for diabetes.
Prospective Follow-Up
Mortality data were obtained from the Central Statistical Office of Finland. Data on nonfatal coronary events were received from the national hospital discharge register. The International Classification of Diseases, Injuries, and Causes of Death (ICD, 8th and 9th revisions) codes 410 to 414 were classified as coronary deaths and ICD codes 410 to 411 in the hospital discharge register as nonfatal acute coronary events.
Two separate end points, an incident case of CHD and CHD death, were analyzed. An incident CHD event was defined as either the first acute nonfatal coronary event or CHD death without a preceding nonfatal coronary event. The follow-up of each subject in our present analyses continued through the end of 1994. During the follow-up, 156 095 person-years were accumulated. The numbers of incident CHD events were 520 among men and 208 among women, and the numbers of CHD deaths were 231 and 63, respectively.
Statistical Analyses
ANOVA was used to test the difference in risk factors between sexes. Multivariate analyses were performed by use of a Cox proportional hazards model.21 All models were adjusted for age,
study year, and area. To assess whether the association of risk factors with CHD risk is different in men than in women, first-level interactions between sex and risk factors were tested. To assess the extent to which the sex difference in the risk of CHD may be explained by differences in the risk factors, a model was built including data for both sexes and using sex as an explanatory variable. The model was then completed by addition of the other risk factors. The proportion of the excess risk of CHD in men compared with women that was explained by the differences in risk factors was estimated by comparing the risk ratios of CHD associated with sex
before and after adjustment for the other risk factors [(RR02RR1)/
(RR021), where RR0is age-, area-, and study year–adjusted risk ratio
and RR1is age-, area-, study year–, and risk factor–adjusted risk
ratio]. A similar procedure was used to analyze the extent to which the age-related changes in risk factors may explain the difference in CHD risk between the age groups. The statistical analyses were performed with the SAS statistical programs.22
Results
CHD incidence and mortality were 786 and 339 per 100 000 person-years among men and 256 and 76 per 100 000 person-years among women, respectively (Table 1). Relative difference in CHD risk between sexes was largest among the youngest subjects, 25 to 49 years old, and smallest among the oldest subjects, 60 to 64 years old. The absolute difference in CHD risk, however, was largest in the oldest age group.
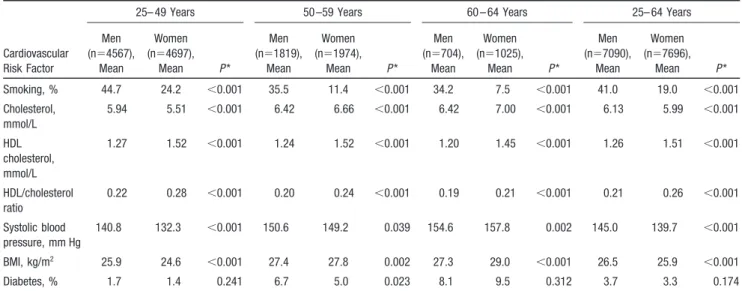
Smoking was more common, total cholesterol and blood pressure were higher, HDL cholesterol was lower, and BMI was higher among men in both the 25- to 64- and 25- to 49-year age groups (Table 2). In the age group 50 to 59 years, systolic blood pressure of women nearly reached that of men, and serum total cholesterol and BMI were already higher in women. In the age group 60 to 64 years as well, systolic blood pressure was higher in women. The HDL/total cholesterol ratio was higher among women, but this difference dimin-ished with increasing age. Diabetes prevalence was fairly similar and increased similarly with age in both sexes.
The above-mentioned risk factors, except BMI, predicted the risk of CHD in both sexes (Table 3). In univariate analyses, BMI and CHD risk had a statistically significant association (risk ratio, 1.04 [P50.002] for incidence and 1.04 [P50.024] for mortality in men and 1.04 [P50.002] for incidence and 1.08 [P50.002] for mortality in women), but the association disappeared when the other risk factors were included in the analyses. BMI and diabetes had a stronger association with coronary mortality in women than in men. Otherwise, the association of risk factors with CHD incidence and mortality was similar in both sexes.
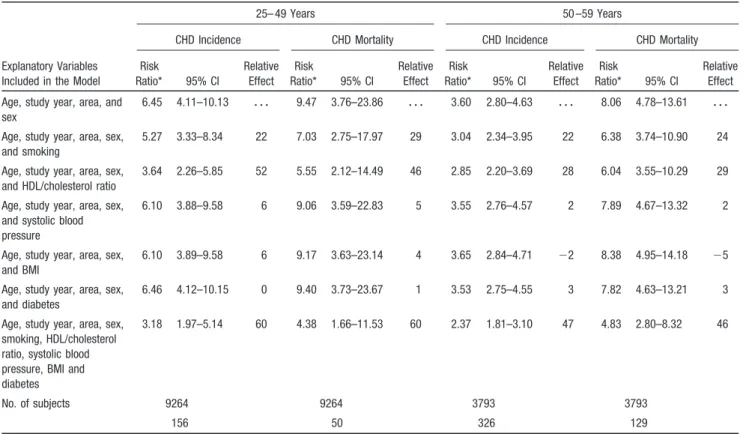
The risk ratio of CHD associated with sex (men versus women) was 3.38 for incidence and 5.00 for mortality (Table 4). The risk ratios decreased to 2.31 and 3.20 after smoking, TABLE 1. CHD Incidence and Mortality per 100 000 Person-Years and Relative and Absolute Risk Differences Between Sexes by Age Group
25– 49 Years 50 –59 Years 60 – 64 Years 25– 64 Years* Men (n54567) Women (n54697) Men (n51819) Women (n51974) Men (n5704) Women (n51025) Men (n57090) Women (n57696) Incidence (No. of events) 275 (134) 44 (22) 1391 (246) 391 (80) 2308 (140) 1036 (107) 786 (520) 256 (209) Relative risk 6.25 3.56 2.23 3.07 Absolute risk difference† 231 1000 1272 530 Mortality (No. of deaths) 92 (45) 10 (5) 611 (113) 77 (16) 1124 (73) 393 (42) 339 (231) 76 (63) Relative risk 9.20 7.94 2.86 4.46 Absolute risk difference† 82 534 731 263
*Adjusted for age. †Per 100 000 person-years.
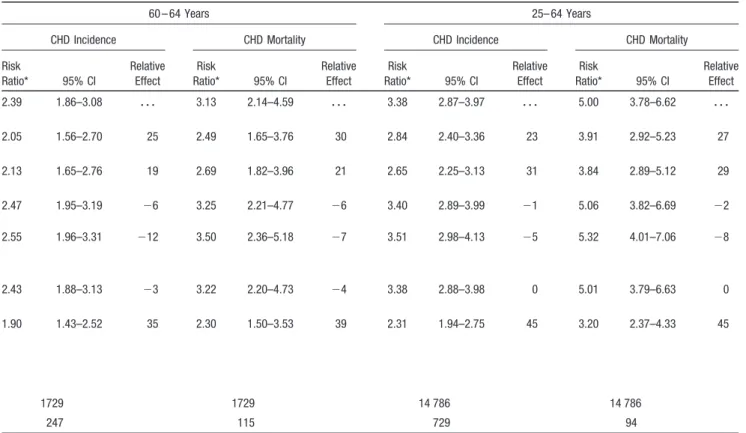
HDL/total cholesterol ratio, systolic blood pressure, BMI, and diabetes were introduced into the model. Thus,'45% of the excess CHD risk of men was associated with the sex differences in cardiovascular risk factors. This proportion was highest,'60% for both CHD incidence and mortality, in the age group 25 to 49 years. The corresponding proportions were 47% and 46% in the age group 50 to 59 years and 35% and 39% in the age group 60 to 64 years. In all age groups, the sex difference in the HDL/total cholesterol ratio explained most of the risk factor–associated excess CHD risk. Smoking was the second most important determinant of the sex difference in CHD risk.
Age-related change in risk factors explained about one-third in men and over half in women of the higher CHD risk in the age group 50 to 64 years compared with the age group 25 to 49 years (Table 5). A decrease in the HDL/total cholesterol ratio and increase in systolic blood pressure
contributed most to the risk factor–associated increase of CHD risk by aging. Also, the increase in BMI and diabetes prevalence was associated with the increase of CHD inci-dence and mortality by aging.
Discussion
The role of major cardiovascular risk factors in the develop-ment of CHD was fairly similar in both sexes. Among young subjects, the overall risk factor level was more favorable in women. With age, however, this advantage of women dimin-ished markedly.
CHD incidence among men was '3-fold and mortality '5-fold greater than in women. The sex differences in the measured cardiovascular risk factors explained nearly half of the observed sex difference in CHD incidence and mortality. The difference in the HDL/total cholesterol ratio was the major determinant of the sex difference in CHD risk. In TABLE 2. Levels of Cardiovascular Risk Factors by Age Group and Sex
Cardiovascular Risk Factor
25– 49 Years 50 –59 Years 60 – 64 Years 25– 64 Years Men (n54567), Mean Women (n54697), Mean P * Men (n51819), Mean Women (n51974), Mean P * Men (n5704), Mean Women (n51025), Mean P * Men (n57090), Mean Women (n57696), Mean P * Smoking, % 44.7 24.2 ,0.001 35.5 11.4 ,0.001 34.2 7.5 ,0.001 41.0 19.0 ,0.001 Cholesterol, mmol/L 5.94 5.51 ,0.001 6.42 6.66 ,0.001 6.42 7.00 ,0.001 6.13 5.99 ,0.001 HDL cholesterol, mmol/L 1.27 1.52 ,0.001 1.24 1.52 ,0.001 1.20 1.45 ,0.001 1.26 1.51 ,0.001 HDL/cholesterol ratio 0.22 0.28 ,0.001 0.20 0.24 ,0.001 0.19 0.21 ,0.001 0.21 0.26 ,0.001 Systolic blood pressure, mm Hg 140.8 132.3 ,0.001 150.6 149.2 0.039 154.6 157.8 0.002 145.0 139.7 ,0.001 BMI, kg/m2 25.9 24.6 ,0.001 27.4 27.8 0.002 27.3 29.0 ,0.001 26.5 25.9 ,0.001 Diabetes, % 1.7 1.4 0.241 6.7 5.0 0.023 8.1 9.5 0.312 3.7 3.3 0.174 *Difference between men and women, adjusted for age.
TABLE 3. Risk Ratio* of CHD Incidence and Mortality Associated With Smoking, Cholesterol, HDL Cholesterol, HDL/Cholesterol Ratio, Systolic Blood Pressure, BMI, and Diabetes Among Men and Women 25 to 64 Years Old
CHD Incidence, Risk Ratio (95% CI) CHD Mortality, Risk Ratio (95% CI) Men Women Men Women Smoking (smokers vs nonsmokers) 1.77 (1.49–2.11) 2.14 (1.46–3.14) 2.19 (1.68–2.84) 3.03 (1.53–6.00) Cholesterol (per mmol/L) 1.34 (1.26–1.43) 1.21 (1.10–1.33) 1.36 (1.24–1.49) 1.21 (1.03–1.43) HDL cholesterol (per 0.1 mmol/L) 0.92 (0.89–0.94) 0.91 (0.87–0.95) 0.91 (0.87–0.95) 0.90 (0.84–0.98) HDL/cholesterol ratio 0.45 (0.38–0.54) 0.50 (0.39–0.64) 0.42 (0.33–0.55) 0.49 (0.31–0.78) Systolic blood pressure (per 10 mm Hg) 1.11 (1.07–1.16) 1.11 (1.04–1.18) 1.11 (1.04–1.19) 1.11 (1.00–1.23) Body mass index (per kg/m2) 0.99 (0.97–1.01) 1.01 (0.98–1.04) 0.99 (0.96–1.02) 1.04 (0.99–1.09)
Diabetes (diabetics vs nondiabetics) 2.00 (1.51–2.61) 2.29 (1.57–3.35) 2.37 (1.63–3.44) 4.26 (2.42–7.60) No. of subjects 7090 7696 7090 7696 No. of events/deaths 520 209 231 63
Interactions between risk factors and sex: Coronary disease incidence: smoking3sexP50.773, cholesterol3sexP50.180, HDL cholesterol3sex P50.385, HDL/cholesterol ratio3sex P50.984, systolic blood pressure3sex P50.650, BMI3sex P50.079, diabetes3sex P50.301. Coronary disease mortality: smoking3sex P50.998, cholesterol3sex P50.597, HDL cholesterol3sex P50.181, HDL/cholesterol ratio3sexP50.484, systolic blood pressure3sexP50.271, BMI3sexP50.014, diabetes3sexP50.009.
*Adjusted for age, study year, and other risk factors.
TABLE 5. CHD Incidence and Mortality in Age Groups 50 –59 Years and 60 – 64 Years Compared With the Age Group 25– 49 Years* and the Proportion of CHD Risk Increase Associated With Age-Related Risk Factor Changes†
Explanatory Variables Included in the Model
Men 50 –59 Years Men 60 – 64 Years
CHD Incidence CHD Mortality CHD Incidence CHD Mortality Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Study year, area, and
age group
5.18 4.20–6.39 z z z 6.79 4.81 –9.59 z z z 9.08 7.16–11.53 z z z 12.93 8.91–18.77 z z z Study year, area, age
group, and smoking
5.51 4.46–6.80 28 7.32 5.22 –10.45 210 9.75 7.68–12.39 27 14.21 19.78–20.66 211 Study year, area, age
group, and HDL/cholesterol ratio
4.44 3.59–5.49 18 5.67 4.20 –8.02 19 7.45 5.86–9.49 20 10.24 7.83–14.94 23
Study year, area, age group, and systolic blood pressure
4.43 3.57–5.50 18 5.73 4.02 –8.16 18 7.04 5.78–9.47 25 10.29 6.99–15.14 22
Study year, area, age group, and BMI
4.84 3.91–5.99 8 6.33 4.47 –8.98 8 8.59 6.76–10.92 6 12.16 8.35–17.70 6 Study year, area, age
group, and diabetes
4.82 13.90–5.96 9 6.16 4.35 –8.74 11 8.33 6.55–10.60 9 11.55 7.90–16.80 Study year, area, age
group, smoking, HDL/cholesterol ratio, systolic blood pressure, BMI, diabetes 4.02 3.22–5.00 28 5.14 3.52 –7.36 28 6.43 4.99–8.78 33 8.81 5.94–13.07 35 No. of subjects 1819 1819 704 704 No. of CHD events/deaths 246 113 146 73 *Reference group.
†(RR02RR1)/(RR021); RR05study year– and area-adjusted risk ratio; RR15study year–, area-, and risk factor–adjusted risk ratio.
TABLE 4. Risk Ratio of CHD Incidence and Mortality Associated With Sex* and the Proportion (%) of Excess Risk in Men Associated With the Difference of Risk Factors Included in Each Model†
Explanatory Variables Included in the Model
25– 49 Years 50 –59 Years
CHD Incidence CHD Mortality CHD Incidence CHD Mortality Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Age, study year, area, and
sex
6.45 4.11–10.13 z z z 9.47 3.76–23.86 z z z 3.60 2.80–4.63 z z z 8.06 4.78–13.61 z z z Age, study year, area, sex,
and smoking
5.27 3.33–8.34 22 7.03 2.75–17.97 29 3.04 2.34–3.95 22 6.38 3.74–10.90 24 Age, study year, area, sex,
and HDL/cholesterol ratio
3.64 2.26–5.85 52 5.55 2.12–14.49 46 2.85 2.20–3.69 28 6.04 3.55–10.29 29 Age, study year, area, sex,
and systolic blood pressure
6.10 3.88–9.58 6 9.06 3.59–22.83 5 3.55 2.76–4.57 2 7.89 4.67–13.32 2
Age, study year, area, sex, and BMI
6.10 3.89–9.58 6 9.17 3.63–23.14 4 3.65 2.84–4.71 22 8.38 4.95–14.18 25 Age, study year, area, sex,
and diabetes
6.46 4.12–10.15 0 9.40 3.73–23.67 1 3.53 2.75–4.55 3 7.82 4.63–13.21 3 Age, study year, area, sex,
smoking, HDL/cholesterol ratio, systolic blood pressure, BMI and diabetes
3.18 1.97–5.14 60 4.38 1.66–11.53 60 2.37 1.81–3.10 47 4.83 2.80–8.32 46
No. of subjects 9264 9264 3793 3793
156 50 326 129
*Men vs women.
†(RR02RR1)/(RR021); RR05age-, study year–, and area-adjusted risk ratio; RR15age-, study year–, area-, and risk factor–adjusted risk ratio.
TABLE 4. Continued
60 – 64 Years 25– 64 Years
CHD Incidence CHD Mortality CHD Incidence CHD Mortality Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect 2.39 1.86–3.08 z z z 3.13 2.14–4.59 z z z 3.38 2.87–3.97 z z z 5.00 3.78–6.62 z z z 2.05 1.56–2.70 25 2.49 1.65–3.76 30 2.84 2.40–3.36 23 3.91 2.92–5.23 27 2.13 1.65–2.76 19 2.69 1.82–3.96 21 2.65 2.25–3.13 31 3.84 2.89–5.12 29 2.47 1.95–3.19 26 3.25 2.21–4.77 26 3.40 2.89–3.99 21 5.06 3.82–6.69 22 2.55 1.96–3.31 212 3.50 2.36–5.18 27 3.51 2.98–4.13 25 5.32 4.01–7.06 28 2.43 1.88–3.13 23 3.22 2.20–4.73 24 3.38 2.88–3.98 0 5.01 3.79–6.63 0 1.90 1.43–2.52 35 2.30 1.50–3.53 39 2.31 1.94–2.75 45 3.20 2.37–4.33 45 1729 1729 14 786 14 786 247 115 729 94 TABLE 5. Continued
Women 54 –59 Years Women 60 – 64 Years
CHD Incidence CHD Mortality CHD Incidence CHD Mortality Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect Risk Ratio* 95% CI Relative Effect 9.01 5.62–14.44 z z z 7.84 2.87–21.40 z z z 24.12 15.24–38.17 z z z 40.38 15.38–102.01 z z z 9.88 6.14–15.91 211 8.78 3.26–24.71 217 27.47 17.19–43.89 215 49.29 19.10–127.17 223 6.18 3.82–10.00 35 4.90 1.77–13.58 43 13.90 8.60–22.47 44 20.30 7.76 –53.13 51 7.06 4.35–11.47 24 5.61 2.01–15.65 33 16.84 10.35–27.38 32 24.82 9.39 –65.59 40 7.69 4.76–12.44 17 5.92 2.14–16.38 28 19.59 12.19–31.48 20 28.11 10.87 –72.69 31 8.42 5.25–13.51 7 6.67 2.43–18.26 17 20.83 13.10–33.14 14 28.64 11.16 –73.50 30 5.53 3.36–9.08 44 4.10 1.44–11.6 55 11.40 6.83–19.05 55 15.04 5.40 –41.91 64 1974 1974 1025 1025 80 16 107 42
addition, differences in smoking rate contributed markedly to the excess CHD risk of men. The role of smoking in the sex difference in CHD risk may be even larger than estimated in our analyses, because smoking may also decrease HDL cholesterol level.23
In both sexes, the risk of CHD increased markedly with age. In most populations, serum total cholesterol increases as age increases. In men, this increase usually levels off around the age of 45 to 50 years, whereas in women, the increase continues sharply until the age of 60 to 65 years.24Like serum
cholesterol, blood pressure also tends to increase with age, and more prominently in women than in men.25The increase
in blood pressure and its different relations to age in men and women are probably explained in part by obesity.25,26
In the 1970s, on the basis of Framingham data, Johnson27
analyzed the role of cardiovascular risk factors on sex difference in CHD risk. His conclusions were that differences in smoking, serum total cholesterol, blood pressure, and the occurrence of left ventricular hypertrophy and glucose intol-erance did not explain the observed sex difference in CHD risk. The shortcoming of the study, however, was that HDL cholesterol was not included in the analyses.
In the early 1990s, Larsson and colleagues28 analyzed
whether sex differences in smoking rate, serum total choles-terol, blood pressure, BMI, and waist-to-hip ratio could explain the sex difference in CHD incidence among 54-year-old Swedish men and women. Their conclusion was that differences in waist-to-hip ratio explained practically all of the sex difference in CHD risk and that the other risk factors included in the analyses altered the results only marginally. This study did not include HDL cholesterol in the analyses, either. Another problem was that waist-to-hip ratio largely depends on anatomic structure, which differs markedly be-tween sexes. Therefore, it is questionable whether the same reference values can be applied in both men and women.
The WHO MONICA Project and ARIC Study researchers recently analyzed the contribution of sex differences in cardiovascular risk factors to sex differences in CHD mortal-ity between 46 communities.8 In this study, communities
were used as the unit of the analyses. Sex differences in CHD mortality between communities were correlated with sex differences in the following risk factors: smoking, obesity, high blood pressure, high total cholesterol, and low HDL cholesterol. Approximately 40% of the variation in the sex ratios of CHD mortality could be explained by differences in the sex ratios of the 5 risk factors examined.
In our study, the major cardiovascular risk factors ex-plained nearly half of the sex difference in CHD risk. An interesting question is which factors explain the other half. The phenomenal difference between men and women is determined by the X and Y chromosomes. During the fetal period, male and female phenotypes are developed through the action of sex hormones. Among women, estrogen is the predominant sex hormone. The decrease in estrogen produc-tion after menopause changes the female lipid metabolism toward a more atherogenic form by decreasing the HDL cholesterol level and by increasing LDL and total cholesterol, triglyceride, and lipoprotein(a) levels.29,30In addition to the
lipid effect, estrogen may have cardioprotective effects
through glucose metabolism and the hemostatic system, and it may also have a direct effect on endothelial cell function.31,32
The role of the major risk factors for the sex difference in CHD risk may also be larger than estimated from our models. Because we measured the risk factors only once, we have probably underestimated the association between the risk factors and CHD risk because of regression dilution bias.33
Atherosclerosis is also a cumulative process, starting at a fairly young age.34 Even though sex differences in serum
cholesterol levels and blood pressure disappeared with age, it is possible that the cumulative effects of these risk factors on arteriosclerosis remain larger in men than in women, because of the longer exposure time in men. In addition to the risk factors included in our analyses, other factors, such as family history of CHD, physical activity, nutrition, and alcohol intake, may explain part of the sex difference in CHD risk. The prevalence of positive family history of CHD and its association with CHD risk does not differ markedly between sexes.35Even though physical activity, nutrition, and alcohol
intake differ somewhat between sexes, their role in the sex difference in CHD risk is probably small.
The major clinical and public health challenges are how to reduce the risk of CHD among middle-aged men closer to that in women and how to prevent the marked increase in CHD risk with aging, particularly in women. The HDL/total cholesterol ratio was the major determinant of the sex difference in CHD risk, and the increase in risk factor levels, particularly in serum cholesterol and blood pressure, ex-plained a substantial part of the age-related increase in CHD incidence and mortality. Both HDL and total cholesterol levels can be modified by dietary and lifestyle changes.36,37
The increase in serum cholesterol and blood pressure with age is not an inevitable physical phenomenon. It does not occur in some nonwesternized populations, and in western populations, it can be prevented.24,38 Reduction in smoking
would also reduce CHD incidence and mortality markedly, particularly in men.
In addition to lifestyle changes, cardiovascular risk can be controlled by pharmacological means, such as antihyperten-sive and cholesterol-lowering drug treatments.39 – 42Two
fac-tors, however, need to be noted when drugs are used in the primary prevention of CHD. First, the initiation of drug treatment should be based on the assessment of the expected absolute reduction in disease risk. Even though the relative risk of CHD associated with risk factors is similar or even higher in women than in men, the risk factors operate at different levels. Second, because the number of people who have only moderately increased CHD risk is large, most of the coronary events occur among them.37,43 Therefore, the
public health impact of even small but population-wide risk factor reduction is usually larger than more marked risk reduction among the high-risk individuals alone.
Even though the major cardiovascular risk factors were the same in both sexes, there are also preventive strategies that are unique to women. Several studies have shown that in postmenopausal women, hormone replacement therapy re-duces the risk of CHD markedly.44 – 47 In clinical trials, the
CHD risk of women in the treatment group has decreased by 40% to 50% compared with the control group. Part of this
reduction in risk has been attributed to changes in the levels of lipoproteins, but other mechanisms are also involved. Even though the evidence supporting the cardioprotective effect of hormone replacement therapy is quite strong, the overall health effects of hormone replacement therapy in women is still a controversial issue.7
In conclusion, differences in major cardiovascular risk factors, particularly in HDL cholesterol level and smoking rate, explained a substantial part of the sex difference in CHD risk. Increases in serum total cholesterol, blood pressure, relative weight, and diabetes prevalence were associated with the age-related increase of CHD incidence and mortality in both sexes but to a larger extent in women. In both sexes, CHD can be effectively prevented by reducing the levels of these risk factors.
References
1. Castelli WP. Epidemiology of coronary heart disease: the Framingham Study. Am J Med. 1984;76:4 –12.
2. Thelle D. Women and coronary heart disease: a review with special emphasis on some risk factors. Lipid Rev. 1990;4:33–39.
3. Thom TJ, Epstein FH, Feldman JJ, Leaverton PE, Wolz M. Total Mor-tality and MorMor-tality From Heart Disease, Cancer and Stroke From 1950 to 1987 in 27 Countries. Bethesda, Md: National Institutes of Health, 1992. NIH publication 92–3088.
4. Kuhn FE, Rackley CE. Coronary artery disease in women: risk factors, evaluation, treatment, and prevention. Arch Intern Med. 1993;153: 2626 –2636.
5. WHO MONICA Project (prepared by Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas A-M, Pajak A). Myocardial infarction and coronary deaths in the World Health Organization MONICA Project: registration procedures, event rates, and case-fatality rates in 38 populations from 21 countries in four continents. Circulation. 1994;90:583– 612.
6. Njolstad I, Arnesen E, Lund-Larsen PG. Smoking, serum lipids, blood pressure, and sex differences in myocardial infarction: a 12-year follow-up of the Finnmark Study. Circulation. 1996;93:450 – 456. 7. Rich-Edwards JW, Manson JAE, Hennekens CH, Buring JE. The primary
prevention of coronary heart disease in women. N Engl J Med. 1995;332: 1758 –1766.
8. Jackson R, Chambless L, Higgins M, Kuulasmaa K, Wijnberg L, Williams D (WHO MONICA Project, and ARIC Study). Sex difference in ischaemic heart disease mortality and risk factors in 46 communities: an ecologic analysis. Cardiovasc Risk Factors. 1997;7:43–54. 9. Keys A. Seven Countries: A Multivariate Analysis of Death and Coronary
Heart Disease. Cambridge, Mass, and London, UK: Harvard University Press; 1980.
10. The Pooling Project Research Group. Relationship of blood pressure, serum cholesterol, smoking habit, relative weight, and ECG abnormalities to incidence of major coronary events: final report of the Pooling Project. Dallas, Tex: American Heart Association Monograph No. 60, 1978. 11. Neaton JD, Wentworth D, for the Multiple Risk Factor Intervention Trial
Research Group. Serum cholesterol, blood pressure, cigarette smoking and death from coronary heart disease. Arch Intern Med. 1992;152: 56 – 64.
12. NIH Consensus Conference. Triglyceride, high-density lipoprotein and coronary heart disease. JAMA. 1993;269:505–510.
13. Corrao JM, Becker RC, Ockene IS, Hamilton GA. Coronary heart disease risk factors in women. Cardiology. 1990;77(suppl 2):8 –24.
14. Jacobs DR Jr, Mebane IL, Bangdiwala SI, Criqui MH, Tyroler HA. High density lipoprotein cholesterol as a predictor of cardiovascular disease mortality in men and women: the follow-up study of the Lipid Research Clinics Prevalence Study. Am J Epidemiol. 1990;131:32– 47.
15. Willett WC, Green A, Stampfer MJ, Speizer FE, Colditz GA, Rosner B, Monson RR, Stason W, Hennekens CH. Relative and absolute excess risk of coronary heart disease among women who smoke cigarettes. N Engl J Med. 1987;317:1303–1309.
16. Manson JE, Colditz GA, Stampfer MJ, Willet WC, Rosner B, Monson RR, Speizer FE, Hennekens CH. A prospective study of obesity and risk of coronary heart disease in women. N Engl J Med. 1990;322:882– 889.
17. Head J, Fuller JH. International variations in mortality among diabetic patients: the WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia. 1990;33:477– 481.
18. Jousilahti P, Tuomilehto J, Vartiainen E, Pekkanen J, Puska P. Body weight, cardiovascular risk factors, and coronary mortality: 15-year follow-up of middle-aged men and women in eastern Finland. Circu-lation. 1996;93:1372–1379.
19. Vartiainen E, Puska P, Jousilahti P, Korhonen HJ, Tuomilehto J, Nissinen A. Twenty year trends in coronary risk factors in North Karelia and in other areas in Finland. Int J Epidemiol. 1994;23:495–503.
20. WHO MONICA Project Principal Investigators. The World Health Orga-nization MONICA Project (monitoring trends and determinants in car-diovascular disease): a major international collaboration. J Clin Epi-demiol. 1988;41:105–114.
21. Cox DR. Regression models and life tables. J R Stat Soc B. 1972;34: 187–220.
22. SAS Institute, Inc. SAS/STAT User’s Guide, Version 6. 4th ed, volume 1–2. Gary, NC: SAS Institute Inc; 1990.
23. Tuomilehto J, Tanskanen A, Salonen JT, Nissinen A, Koskela K. Effects of smoking and stopping smoking on serum high-density lipoprotein cholesterol levels in a representative population sample. Prev Med. 1986; 15:35– 45.
24. Jousilahti P, Vartiainen E, Tuomilehto J, Puska P. Twenty-year dynamics of serum cholesterol in middle-aged population of eastern Finland. Ann Intern Med. 1996;125:713–722.
25. National High Blood Pressure Education Program Working Group Report on Primary Prevention of Hypertension. Arch Intern Med. 1993;153: 186 –208.
26. Jousilahti P, Tuomilehto J, Vartiainen E, Valle T, Nissinen A. Body mass index, blood pressure, diabetes, and the risk of anti-hypertensive drug treatment: 12-year follow-up of middle-aged people in eastern Finland. J Hum Hypertens. 1995;9:847– 854.
27. Johnson A. Sex differentials in coronary heart disease: the explanatory role of primary risk factors. J Health Soc Behav. 1977;18:46 –54. 28. Larsson B, Bengtsson C, Bjo¨rntorp P, Lapidus L, Sjo¨stro¨m L, Sva¨rdsudd
K, Tibblin G, Wedel H, Welin L, Wilhelmsen L. Is abdominal body fat distribution a major explanation for the sex difference in the incidence of myocardial infarction? The Study of Men Born in 1913 and the Study of Women, Go¨teborg. Am J Epidemiol. 1992;135:266 –273.
29. Matthews KA, Meilahn E, Kuller LH, Kelsey SF, Caggiula AW, Wing RR. Menopause and risk factors for coronary heart disease. N Engl J Med. 1989;321:641– 646.
30. Bonithon-Kopp C, Scarabin P-Y, Darne B, Malmejak A, Guize L. Menopause-related changes in lipoproteins and some other cardiovascular risk factors. Int J Epidemiol. 1990;19:42– 48.
31. Grady D, Rubin SM, Petitti DB, Fox CS, Black D, Ettinger B, Ernster VL, Cummings SR. Hormone therapy to prevent disease and prolong life in post menopausal women. Ann Intern Med. 1992;117:1016 –1037. 32. Shahar E, Folsom AR, Salomaa VV, Stinson VL, McGovern PG,
Shimakawa T, Chambless LE, Wu KK, for the Atherosclerosis Risk in Communities (ARIC) Study Investigators. Relation of hormone-replacement therapy to measures of plasma fibrinolytic activity. Circu-lation. 1996;93:1970 –1975.
33. MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, Abbott R, Godwin J, Dyer A, Stamler J. Blood pressure, stroke and coronary heart disease, I: effects of prolonged differences in blood pressure: evidence from nine prospective observational studies corrected for the regression dilution bias. Lancet. 1990;335:765–774.
34. Viikari J, Ro¨nnemaa T, Seppa¨nen A, Marniemi J, Porkka K, Ra¨sa¨nen L, Uhari M, Salo MK, Kaprio EA, Nuutinen EM, Pesonen E, Pietika¨inen M, Dahl M, Åkerblom HK. Serum lipids and lipoproteins in children, ado-lescents and young adults in 1980 –1986. Ann Med. 1991;23:53–59. 35. Jousilahti P, Puska P, Vartiainen E, Pekkanen J, Tuomilehto J. Parental
history of premature coronary heart disease: an independent risk factor of myocardial infarction. J Clin Epidemiol. 1996;49:497–503.
36. Wood PD, Stefanick ML, Dreon DM, Frey-Hewitt B, Garay SC, Williams PT, Superko HR, Fortmann SP, Albers JJ, Vranizan KM, Albers JJ, Vranizan KM, Ellsworth NM, Terry RB, Haskell WL. Changes in plasma lipids and lipoproteins in overweight men during weight loss through dieting as compared with exercise. N Engl J Med. 1988;319:1173–1179. 37. Jousilahti P, Vartiainen E, Pekkanen J, Tuomilehto J, Sundval J, Puska P. Serum cholesterol distribution and coronary heart disease risk: obser-vations and predictions among the middle-aged population in eastern Finland. Circulation. 1998;97:1087–1094.
38. Law MR, Frost CD, Wald NJ. By how much does dietary salt reduction lower blood pressure? III: analysis of data from trials of salt reduction. BMJ. 1991;302:819 – 824.
39. Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, Goldwin J, Qizilbash N, Taylor JO, Hennekens CH. Blood pressure, stroke, and coronary heart disease, II: short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335:827– 838.
40. Staessen JA, Fagard R, Lutgarde T, Celis H, Arabidze GG, Birkenha¨ger WH, Bulpitt CJ, de Leeuw PW, Dollery CT, Fletcher AE, Forette F, Leonetti G, Nachev C, O’Brien ET, Rosenfeld J, Rodicio JL, Tuomilehto J, Zanchetti A, for the Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet. 1997;350:757–764.
41. Scandinavian Simvastatin Survival Study Group. Randomised trial of cho-lesterol lowering in 4444 patients with coronary heart disease: the Scandi-navian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–1389. 42. Johannesson M, Jo¨nsson B, Kjekshus J, Olsson AG, Pedersen TR,
Wedel H. Cost effectiveness of simvastatin treatment to lower
cho-lesterol levels in patients with coronary heart disease. N Engl J Med. 1997;336:332–336.
43. Stamler J, Neaton JD, Wentworth DN. Blood pressure (systolic and diastolic) and risk of fatal coronary heart disease. Hypertension. 1989; 13(suppl I):I-2–I-12.
44. Stampfer MJ, Colditz GA. Estrogen replacement therapy and coronary heart disease: a quantitative assessment of the epidemiologic evidence. Prev Med. 1991;20:47– 63.
45. Belchetz PE. Hormonal treatment of postmenopausal women. N Engl J Med. 1994;330:1062–1071.
46. Bush TL, Barret-Connor E, Cowan LD, Criqui MH, Wallace RB, Such-indran CM, Tyroler HA, Rifkind BM. Cardiovascular mortality in non-contraceptive use of estrogen in women: results from the Lipid Research Clinics Program Follow-up Study. Circulation. 1987;75:1102–1109. 47. Stampfer MJ, Colditz GA, Willett WC, Manson JE, Rosner B, Speizer
FE, Hennekens CH. Postmenopausal estrogen therapy and cardiovascular disease: ten-year follow-up of the Nurses’ Health Study. N Engl J Med. 1991;325:756 –762.