Testosterone Levels in Umbilical-Cord Blood and Risk
of Pyloric Stenosis
WHAT’S KNOWN ON THIS SUBJECT: Infantile hypertrophic pyloric stenosis is⬃5 times more common in male infants. The male hormone testosterone is known to induce muscle
hypertrophy, and the testosterone levels are several-fold higher in male infants than female infants.
WHAT THIS STUDY ADDS: This study is the first of its kind, and the results add new insight to the etiology of pyloric stenosis. No evidence was found to support the hypothesis that high
testosterone levels at birth are associated with an increased risk of pyloric stenosis.
abstract
OBJECTIVE:The risk of infantile hypertrophk pylonc stenosis is ⬃5 times more common in male than female infants. It has been hypothe-sized that the higher risk among male infants is associated with high levels of testosterone causing hypertrophy of the pylorus muscle. To test this hypothesis, we examined the association between the testos-terone levels in the umbilical-cord blood and the risk of infantile hyper-trophic pyloric stenosis.
PATIENTS AND METHODS:We conducted a matched case-control study nested in the Danish National Birth Cohort using risk-set sampling. From a cohort of 101 042 pregnancies, we identified umbilical-cord blood samples from 46 case subjects (43 male and 3 female infants) who developed infantile hypertrophic pyloric stenosis in the first year of life and 150 gender- and gestational age–matched control subjects. The testosterone levels were measured by liquid chromatography– tandem mass spectrometry. Rate ratios were estimated by using con-ditional logistic regression.
RESULTS:In male infants, the mean testosterone level at birth was 0.78 nmol/L in case subjects and 0.91 nmol/L in control subjects. The rate of infantile hypertrophic pyloric stenosis was inversely, albeit insignifi-cantly, associated with the testosterone levels in male infants; there was a 29% (95% confidence interval:⫺46% to 65%;P⫽35) lower rate per nmol/L. The association was not modified according to age, gesta-tional age, or birth order.
CONCLUSIONS:We found no support for the hypothesis that high tes-tosterone levels in the umbilical-cord blood are strongly associated with a subsequently higher risk for infantile hypertrophic pyloric ste-nosis in male infants. Pediatrics2011;127:e197–e201
AUTHORS:Camilla Krogh, MD,aArieh S. Cohen, PhD,b
Saima Basit, MSc,aDavid M. Hougaard, DMSc,bRobert J.
Biggar, MD,aJan Wohlfahrt, DMSc,aMads Melbye, DMSc,a
and Thea K. Fischer, DMSca
Departments ofaEpidemiology Research andbClinical
Biochemistry and Immunology, Statens Serum Institut, Copenhagen, Denmark
KEY WORDS
infantile hypertrophic pyloric stenosis, testosterone, umbilical cord blood, etiology
ABBREVIATIONS
RR—rate ratio CI—confidence interval
Drs Krogh, Cohen, Basit, Hougaard, Wohlfahrt, Melbye, and Fischer made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; Drs Krogh, Cohen, Hougaard, Biggar, Wohlfahrt, Melbye, and Fischer contributed to the drafting of the article or revising it critically for important intellectual content; and Drs Krogh, Cohen, Basit, Hougaard, Biggar, Wohlfahrt, Melbye, and Fischer contributed to the final approval of the version to be published.
www.pediatrics.org/cgi/doi/10.1542/peds.2010-2127
doi:10.1542/peds.2010-2127
Accepted for publication Sep 29, 2010
Address correspondence to Camilla Krogh, MD, Department of Epidemiology Research, Statens Serum Institut, 5 Artillerivej, DK-2300 Copenhagen S, Denmark. E-mail: ckr@ssi.dk
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
tion in which apparently healthy in-fants, typically from 2 to 8 weeks old,1–3
develop an inability to pass food from the stomach into the duodenum. Pylo-ric stenosis is characterized by hyper-trophy of the pylorus smooth circular muscle layer, which blocks the gastric outlet and leads to severe postpran-dial vomiting. Mortality was as high as 50%4until successful treatment by
py-loromyotomy was developed by Ramst-edt in 1911.5Currently, pyloric stenosis
is the most common condition that re-quires surgery in the first months of life.6The incidence of pyloric stenosis
in Denmark was 1 to 2 per 1000 infants in 2000.1
Although the clinical presentation, di-agnosis, and treatment of pyloric ste-nosis are well established, the etiology remains unclear. Other than aggrega-tion in families,2,6–9 the most
consis-tently reported risk factor for pyloric stenosis is that it occurs predomi-nantly in male infants. The risk of pylo-ric stenosis is strikingly 4 to 5 times more common in male than female in-fants.2,3,8,9Male infants have higher
lev-els of testosterone,10and 1 hypothesis
is that the known effect of testosterone in causing muscle hypertrophy11,12
ex-plains the higher risk of pyloric steno-sis in male infants. Consteno-sistent with this suggestion, firstborn male infants have been reported to have higher tes-tosterone levels in the umbilical cord than next-born male infants,13,14 and
firstborn male infants seem to be af-fected with pyloric stenosis more of-ten than later-born male infants.2,3,15
Therefore, high early postnatal andro-gen levels have been proposed to be a cause of pyloric stenosis.13,16However,
this hypothesis has, to our knowledge, never been tested.
To study whether high umbilical-cord blood testosterone levels are a risk factor for pyloric stenosis, we
per-within the Danish National Birth Cohort by using risk-set sampling.
MATERIALS AND METHODS
Study Population
The study was based on the Danish Na-tional Birth Cohort,17which is a
preg-nancy cohort that enrolled 101 042 pregnancies from a total of 91 827 Dan-ish women from 1996 to 2002. The cur-rent study population was defined as live-born singleton children who were included in the Danish National Birth Cohort and who had umbilical-cord blood samples. Information on age, birth order, and gender was obtained from the Danish Civil Registration Sys-tem. Since April 1968, the Danish Civil Registration System has registered gender, date, and place of birth and updated information on vital status and emigration, using a unique per-sonal identification number assigned to each Danish resident.18This
num-ber permits accurate linkage of individual-level information between the nationwide registers in Den-mark. Data on gestational age were based on information from the Dan-ish Birth Registry.19
Identification of Case and Control Subjects
Information on a diagnosis of pyloric stenosis was obtained from the Danish National Patient Register.20Pyloric
ste-nosis case subjects were defined as children who, in their first year of life, had a pyloromyotomy determined by the surgery codes KJDH60 and KJDH61 (Nordic Classification of Surgical Pro-cedures). In a few cases, a diagnosis code for pyloric stenosis was available according to the Danish National Pa-tient Register (Q40.0, DK31.1, K31.1A, DK31.3, and DK31.8B [International Classifications of Diseases, 10th Revi-sion]), but no additional codes
docu-were individually reviewed, and when
the file included a definite record of pyloric stenosis surgery, the child was included as a case subject. For each case subject, 4 control subjects were
sampled using a risk-set sampling technique. Control subjects were sam-pled among singleton births from the same cohort, who at the time of
diag-nosis of the case subject were alive and living in Denmark without prior di-agnosis of pyloric stenosis.21 Control
subjects were matched on gender and gestational age at birth (weeks). When
the sample set was determined, serum samples were sought. Only those with adequate amounts of umbilical-cord blood (200L of serum) for the
hor-mone laboratory tests were used.
Testosterone Analysis
The umbilical-cord serum was stored at⫺30°C. Testosterone was measured
by liquid chromatography–tandem mass spectrometry.22,23A total of 20L
of internal standard solution was added to 200-L aliquots of
umbilical-cord serum. The samples were ex-tracted with diethyl ether and recon-stituted in 50% methanol. The liquid chromatography–tandem mass spec-trometry system consisted of a
Sur-veyor quaternary pump (Thermo Fisher Scientific, Waltham, MA), a CTC autosampler (CTC Analytics AG, Zwingen, Switzerland), and a TSQ
ul-tra triple quadrupole mass spectrom-eter (Thermo Fischer Scientific). Chromatographic separation was achieved using a Hypersil Gold C18
column (50 ⫻ 2.1 mm, 3 m chro-matographic material; Thermo Fisher Scientific). Testosterone was detected by tandem mass spectrometry using selective reaction monitoring. The
Statistical Analysis
The association between testosterone levels in umbilical-cord blood and the risk of pyloric stenosis was evaluated by (incidence) rate ratios (RRs) esti-mated in a conditional logistic regres-sion using proc logistic in SAS 9.1 (SAS Institute, Inc, Cary, NC),21taking into
ac-count matching by gender and gesta-tional age at birth. The analyses of ef-fect modification were conducted by including an interaction term in the conditional logistic regression. All tests were 2-sided with a 5% signifi-cance level.Pvalues were calculated by using likelihood ratio tests.
Ethics
Women enrolled in the Danish National Birth Cohort gave both verbal and writ-ten consent to participate. The women gave permission to include interview information, blood samples, and health information from other regis-ters in the Danish National Birth Co-hort. The study was approved by the Danish National Birth Cohort, the Dan-ish Data Protection Board, and the Sci-entific Ethical Committee.
RESULTS
A total of 46 pyloric stenosis case sub-jects (50% firstborn) and 150 control subjects (44% firstborn) were avail-able for analysis. The mean gestational age at birth was 39.7 weeks for both
case and control subjects. The average age at pyloric stenosis diagnosis for case subjects was 36 days.
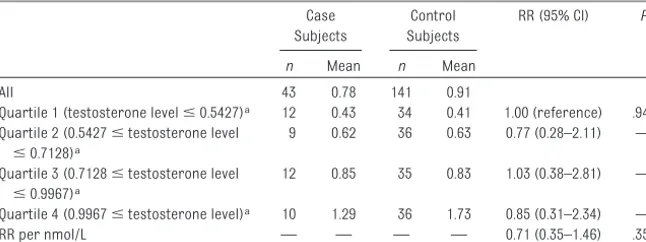
Table 1 shows the RRs of pyloric steno-sis in male infants according to umbilical-cord testosterone levels. The mean testosterone level for 43 male case subjects and 141 matching con-trol subjects was 0.78 nmol/L and 0.91 nmol/L, respectively. The rate of pylo-ric stenosis for male infants was in-versely but insignificantly associated with testosterone level, with a 29% (95% confidence interval [CI]:⫺46% to 65%;P⫽ .35) lower rate per nmol/L (RR: 0.71 [95% CI: 0.35–1.46]). Adjust-ment for being firstborn gave almost similar results (RR: 0.67 [95% CI: 0.31– 1.44]).Testosterone levels divided into quartiles to allow for a nonlinear ciation showed the same lack of asso-ciation (P⫽.94). There was no signifi-cant modification of the overall association with testosterone levels and pyloric stenosis according to age (P⫽.59), gestational age (P⫽.84), or birth order (P⫽.95).
Overall, the testosterone levels of the female infants were lower than the tes-tosterone levels of the male infants. In female infants, the mean testosterone level for 3 case subjects and 9 match-ing control subjects was 0.76 and 0.50 nmol/L, respectively. The rate of pylo-ric stenosis for female infants was
in-significantly associated with the tes-tosterone level (P⫽.33).
DISCUSSION
The aim of this study was to examine the hypothesis that a high testoster-one level in umbilical-cord blood is a risk factor for pyloric stenosis. To the best of our knowledge, this evaluation has not previously been made. In this study, we found no support for an as-sociation between pyloric stenosis risk and testosterone levels at birth in male infants. Pyloric stenosis is pre-dominantly observed among male infants, and we had little power to as-sess testosterone levels in female-infant case subjects.
Awareness of the much higher risk of pyloric stenosis in male than female infants has prompted speculation about male gender–related factors, of which testosterone levels is an obvi-ous candidate. In our study and oth-ers,10testosterone levels at birth were
higher in male than female infants and, therefore, were consistent with the difference in the higher pyloric ste-nosis incidence in male infants. How-ever, testosterone levels at birth were not significantly different in male in-fants who did versus those who did not develop the condition. Indeed, male in-fants with pyloric stenosis had slightly lower testosterone levels than control subjects.
In the present study, liquid chromatography–tandem mass spec-trometry was used to obtain the preci-sion and accuracy necessary to mea-sure the low testosterone levels found in umbilical-cord blood samples. In most clinical studies, testosterone lev-els are determined using direct im-munoassays. However, this method is not precise enough to be used for serum samples from women and children with low concentrations of testosterone because of matrix ef-fects and inherent cross-reactivity
TABLE 1 RRs for Infantile Hypertrophic Pyloric Stenosis in Male Infants According to Umbilical-Cord Testosterone Levels
Case Subjects
Control Subjects
RR (95% CI) P
n Mean n Mean
All 43 0.78 141 0.91
Quartile 1 (testosterone levelⱕ0.5427)a 12 0.43 34 0.41 1.00 (reference) .94b Quartile 2 (0.5427ⱕtestosterone level
ⱕ0.7128)a
9 0.62 36 0.63 0.77 (0.28–2.11) —
Quartile 3 (0.7128ⱕtestosterone level
ⱕ0.9967)a
12 0.85 35 0.83 1.03 (0.38–2.81) —
Quartile 4 (0.9967ⱕtestosterone level)a 10 1.29 36 1.73 0.85 (0.31–2.34) —
RR per nmol/L — — — — 0.71 (0.35–1.46) .35c
aQuartiles of testosterone levels (nmol/L) with 25% of the observations in each category. bP: test for no difference in rates between quartiles.
cP: test for no change in rate per nmol/L.
ing liquid chromatography–tandem mass spectrometry.25
The Danish National Birth Cohort is one of the world’s largest birth cohorts, with storage of biological material such as umbilical-cord blood, which of-fers a unique opportunity to study hy-potheses such as the one in question. We obtained information on age, birth order, and gender from the Danish Civil Registration System, and this reg-ister has been proven close to being complete.18Our pyloric stenosis
diag-noses were obtained from the Danish National Patient Register, in which hos-pital discharge diagnoses are manda-torily recorded. In particular, surgical diagnoses are likely to be both accu-rate and well recorded.26 In addition,
we evaluated medical records to en-sure the correctness of the diagnosis. We therefore consider misclassifica-tion of the diagnosis unlikely. The risk-set sampling design allows for a direct comparison of the pyloric stenosis
the onset of pyloric stenosis, which rules out inverse causality.
We acknowledge that despite the avail-ability of a large birth cohort the num-ber of case subjects was rather small. However, the number of male case subjects seemed sufficient to exclude an association above a 50% increase in pyloric stenosis rate per nmol/L of tes-tosterone. In the Danish National Birth Cohort, ⬃60% of the children have umbilical-cord samples, but there is no apparent reason to suspect selec-tion bias related to the availability of umbilical-cord blood samples. Be-cause we did not collect the blood sam-ples at the time of disease onset, we cannot exclude that testosterone lev-els may have changed differentially since birth in those who did and those who did not develop pyloric stenosis.
CONCLUSIONS
We found no evidence to support the hypothesis that high umbilical-cord
ric stenosis. Other endocrine factors with a pronounced sexual dysmor-phism in early infancy may explain the male propensity for pyloric ste-nosis. Also, the ratio between testos-terone and cortisol might be an influ-ence, and the field definitely needs
additional investigation.
ACKNOWLEDGMENTS
This study was funded by grants from the Lundbeck Foundation (27/06), the Faculty of Health Sciences (University of Copenhagen), and the Danish Agency for Science, Technology, and In-novation. None of the Foundations had
a role in the design or conduct of the study; in the collection, management, analysis, or interpretation of the data; or in the preparation, review, or ap-proval of the manuscript.
We thank the Danish National Birth Co-hort for permission to use the data and umbilical-cord samples.
REFERENCES
1. Haahr P, Nielsen JP. Infantile hypertro-phic pyloric stenosis: a 25-year study from the county of Viborg [in Danish].
Ugeskr Laeger. 2000;162(24):3456 –3459 2. MacMahon B. The continuing enigma of
py-loric stenosis of infancy: a review. Epidemi-ology. 2006;17(2):195–201
3. Schechter R, Torfs CP, Bateson TF. The epi-demiology of infantile hypertrophic pyloric stenosis. Paediatr Perinat Epidemiol. 1997;11 (4):407– 427
4. Hernanz-Schulman M. Infantile hypertro-phic pyloric stenosis. Radiology. 2003; 227(2):319 –331
5. Ramstedt C. Surgery of congenital pylonic steno-sis. [in German].Med Klin. 1912;8:1702–1705
6. Chung E. Infantile hypertrophic pyloric stenosis: genes and environment.Arch Dis Child. 2008;93(12):1003–1004
7. Carter CO, Evans KA. Inheritance of congen-ital pyloric stenosis.J Med Genet. 1969;6(3): 233–254
8. Krogh C, Fischer TK, Skotte L, et al. Familial aggregation and heritability of pyloric ste-nosis.JAMA. 2010;303(23):2393–2399
9. Mitchell LE, Risch N. The genetics of infan-tile hypertrophic pyloric stenosis: a re-analysis. Am J Dis Child. 1993;147(11): 1203–1211
10. Troisi R, Potischman N, Roberts J, et al. As-sociations of maternal and umbilical cord hormone concentrations with maternal, gestational and neonatal factors (United States).Cancer Causes Control. 2003;14(4): 347–355
11. Sinha-Hikim I, Artaza J, Woodhouse L, et al. Testosterone-induced increase in mus-cle size in healthy young men is associ-ated with muscle fiber hypertrophy.Am J Physiol Endocrinol Metab. 2002;283(1): E154 –E164
12. Lane HA, Grace F, Smith JC, et al. Impaired vasoreactivity in bodybuilders using andro-genic anabolic steroids.Eur J Clin Invest. 2006;36(7):483– 488
13. James WH. Evidence that intrauterine and postnatal androgens affect the develop-ment of pyloric stenosis.Birth Defects Res A Clin Mol Teratol. 2004;70(1):37–39
14. Maccoby EE, Doering CH, Jacklin CN,
Krae-mer H. Concentrations of sex hormones in umbilical-cord blood: their relation to sex and birth order of infants.Child Dev. 1979; 50(3):632– 642
15. Jedd MB, Melton LJ, III, Griffin MR, et al. Fac-tors associated with infantile hypertrophic pyloric stenosis.Am J Dis Child. 1988;142(3): 334 –337
16. Cui W, Ma CX, Tang Y, et al. Sex differences in birth defects: a study of opposite-sex twins.
Birth Defects Res A Clin Mol Teratol. 2005; 73(11):876 – 880
17. Olsen J. The Danish National Birth Cohort: its background, structure and aim.Scand J Public Health. 2001;29(4):300 –307
18. Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The Danish Civil Registration System: a cohort of eight million persons.
Dan Med Bull. 2006;53(4):441– 449
19. Knudsen LB, Olsen J. The Danish Medical Birth Registry.Dan Med Bull. 1998;45(3): 320 –323
for modern health sciences.Dan Med Bull. 1999;46(3):263–268
21. King G, Zeng L. Estimating risk and rate lev-els, ratios and differences in case-control studies.Stat Med. 2002;21(10):1409 –1427
22. Bay K, Cohen AS, Jorgensen FS, et al. Insulin-like factor 3 levels in second-trimester am-niotic fluid.J Clin Endocrinol Metab. 2008; 93(10):4048 – 4051
23. Cawood ML, Field HP, Ford CG, et al.
Testos-terone measurement by isotope-dilution liquid chromatography-tandem mass spectrometry: validation of a method for routine clinical practice.Clin Chem. 2005; 51(8):1472–1479
24. Wang C, Catlin DH, Demers LM, Starcevic B, Swerdloff RS. Measurement of total serum testosterone in adult men: comparison of current laboratory methods versus liquid chromatography-tandem mass
spectrome-try.J Clin Endocrinol Metab. 2004;89(2): 534 –543
25. Soldin SJ, Soldin OP. Steroid hormone anal-ysis by tandem mass spectrometry. Clin Chem. 2009;55(6):1061–1066
26. Mosbech J, Jorgensen J, Madsen M, Rost-gaard K, Thornberg K, Poulsen TD. The na-tional patient registry: evaluation of data quality [in Danish]. Ugeskr Laeger. 1995; 157(26):3741–3745
DOI: 10.1542/peds.2010-2127 originally published online December 20, 2010;
2011;127;e197
Pediatrics
Jan Wohlfahrt, Mads Melbye and Thea K. Fischer
Services
Updated Information &
http://pediatrics.aappublications.org/content/127/1/e197
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/127/1/e197#BIBL
This article cites 26 articles, 4 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2010-2127 originally published online December 20, 2010;
2011;127;e197
Pediatrics
Jan Wohlfahrt, Mads Melbye and Thea K. Fischer
Camilla Krogh, Arieh S. Cohen, Saima Basit, David M. Hougaard, Robert J. Biggar,
Testosterone Levels in Umbilical-Cord Blood and Risk of Pyloric Stenosis
http://pediatrics.aappublications.org/content/127/1/e197
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.