International Journal of Current
Medical and Pharmaceutical
Research
Available Online athttp://www.journalcmpr.com
DOI: http://dx.doi.org/10.24327/23956429.ijcmpr20170232
RESEARCH ARTICLE
DISEASE ACTIVITY SCORE 28 IS A GOOD PREDICTOR OF CARDIOVASCULAR
DISORDERS IN EGYPTIAN PATIENTS WITH RHEUMATOID ARTHRITIS
Hafez A. Abd-Elhafeez
1., El-Sayed El-Meghawary El-Sayed
2., Khaled Nagy Elfayoumy
2*.,
Khaled Ibraheem Naguib
3., Ahmed Salama AL-Adl
2and Mohamad Abdelmoez Ali
42, 3, 4
Faculty of Medicine, Al-Azhar University, New Damietta, Damietta, Egypt
2
Internal Medicine Department
3
Cardiology Department
4
Rheumatology Department
1
Internal Medicine Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
ARTICLE INFO ABSTRACT
Background: The risk of cardiovascular morbidity and mortality is exaggerated in patients with rheumatoid arthritis than non-rheumatoid subjects. There are conflicting data whether acute phase reactants are good predictors of such diseases. The aim of the study was to determine the different varieties of cardiovascular disorders in Egyptian patients with rheumatoid arthritis, and the relation of these disorders with the activity of the rheumatoid disease as indicated by Disease Activity Score 28.
Materials and methods: The study was a cross-sectional study including 100 Egyptian patients with rheumatoid arthritis on regular treatment. Disease activity was assessed, in addition to carotid duplex study and echocardiography evaluation.
Results: Seventy of our patients had seropositive rheumatoid arthritis, and the other 30 patients were seronegative. The latter were rarely affected by cardiovascular disorders. A large scale of cardiovascular disorders was encountered in rheumatoid patients, but atherosclerosis was the most frequent one (51% of the study population). All types of cardiovascular disorders are associated with a higher Disease Activity Score 28.
Conclusion: Egyptian patients with seropositive rheumatoid arthritis were prone to many types of cardiovascular disorders. High Disease Activity Score 28 was the most sensitive indicator of associated cardiovascular disorders. Patients with rheumatoid arthritis should be screened for early detection and control of these disorders.
Copyright © 2017 Khaled Nagy Elfayoumy et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic inflammatory disease with predominant articular affection. Patients with RA experience excess cardiovascular (CV) morbidity and mortality that are not explained by traditional cardiac risk factors, but attributed to chronic systemic inflammation1, 2. A wide range of cardiovascular disorders (CVD) has been described including; coronary heart disease(CHD), pulmonary hypertension (HTN), left ventricular diastolic dysfunction (LVDD), and heart failure (HF) 3-5. On the other hand, there is controversy whether C-reactive protein (CRP) is a sensitive measure of disease activity; Gonzalez-Gay MA et al. (2005) stated that CRP is good indicator of systemic inflammation, and is the best biomarker for the excess CV morbidity associated with RA6. Conversely, Pereira IA et al. (2009) demonstrated that isolated inflammatory markers or
noncumulative activity scores are not sensitive predictors of cardiovascular disorders (CVD) 7.
This study aimed at determination of the different varieties of CVD among Egyptian patients with RA, and their relation with the activity of the latter as indicated by Disease Activity Score 28 (CRP) {DAS28 (CRP)}.
MATERIALS AND METHODS
This cross-sectional study included 100 Egyptian patients with RA. They were periodically following up at the outpatient clinic of Al-Azhar University Hospital at New Damietta, Egypt, from January 2014 to September 2014. The patients were previously diagnosed according to American College of Rheumatology (ACR) ∕ European League against Rheumatism
(EULAR) 2010 classification criteria for rheumatoid arthritis8.
All patients had documented history of their disease and were
Article History:
Received 20th June, 2017 Received in revised form 3rd July, 2017
Accepted 27th August, 2017
Published online 28th September, 2017
Key words:
Rheumatoid arthritis, cardiovascular disorders, rheumatoid factor, disease activity score 28.
on the specific anti-rheumatoid medication. Patients with diabetes mellitus, uncontrolled HTN, rheumatic heart disease, and pulmonary or thyroid disorders were excluded from this study. Those who were smokers, severely anemic, or having morbid obesity or significant liver or renal disorders were excluded too.
Assessment of Disease Activity
Assessment of rheumatoid activity was done using first hour-erythrocyte sedimentation rate (ESR), CRP titer, and DAS28 (CRP). DAS28 employs a simplified 28-joint count. This includes the number of swollen and tender joints of the shoulders, elbows, wrists, metacarpophalangeal and proximal interphalangeal joints of the hands, thumb interphalangeal joints, and knees. It excludes the hips, ankles, and feet9. DAS28 (CRP) was done using levels
of CRP (mg/L) as an acute phase response in addition to a measure of the general health (GH; patient assessment of disease activity using a 100 mm visual analogue scale (VAS) with 0 = best, 100 = worst), by the following formula: DAS28(CRP) =0.56√(TJC28)+0.28√(SJC28)+0.014GH+0.36
in(CRP+1)+0.96, where TJC = tender joint count and
SJC = swollen joint count, with a score ranging from 0 to 9.4.
The patient was considered to be in remission if he achieved 2.6< in this score, otherwise he had active disease10.
Laboratory Investigations
Complete blood count (CBC), ESR (estimated by Western method), CRP titer and RF titer using latex agglutination test were done. CRP was considered positive if ≥ 6 mg/L, and the
positive RF was considered on ≥ 8mg/L.
Imaging
Carotid duplex study was performed to estimate the intima-media thickness (IMT). The carotid arteries were examined while the patient was in the supine position with the examiner seated at the patient's head, and the transducer at 2 to 3 cm proximal to the bifurcation. Patients who had IMT >0.7 mm were diagnosed as having atherosclerosis11.
Cardiac Assessment Methods
1. ECG. 2. Standard 2D/Doppler echocardiography was performed for the following parameters: left ventricular (LV) internal dimensions, LV ejection fraction, percentage of fraction shortening, resting segmental and / or regional wall motion abnormalities, and valvular lesions.
CHD was diagnosed on the presence of either: angina
pectoris, documented history of myocardial infarction or coronary revascularization procedures, or specific motion abnormalities by echocardiography
Ethical Approval
Informed agreement was obtained from all participants, and all procedures were in accordance with the standards of the 1964 Helsinki Declaration and its later amendments ethical standards.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD). Categorical variables are reported as number and proportions. The continuous data were checked for normality and equality of distribution, prior to any analysis performed. Comparisons between the groups were made using independent t test for continuous normally-distributed variables, while chi-square test was used for comparison
between categorical variables. All calculations were performed using SPSS 17.0 software for Windows. P<0.05 was considered significant.
RESULTS
This study included 100 patients with RA (67% female). Seventy patients had positive RF; 45 of them were female. Seronegative patients were 22 female and 8 male patients
According to the carotid duplex and Echocardiographic findings, 51% of patients had atherosclerosis, and 34% had carotid plaques. In addition, 23% had CHD, 32% LVDD, 12% pericardial effusion, 6% pulmonary HTN, 5% cardiomyopathy and 12% had valvular affection (Figure 1). So, atherosclerosis, diagnosed by increased IMT, was the most prevalent CVD among our patients. The average IMT of the carotid artery was 0.81 ±0.24 mm. Carotid plaques was nearly absent in seronegative patients (a single case only) (p<0.001), but significantly associated with male gender (p=0.032). Atherosclerosis, in general, was significantly associated with higher disease activity as indicated by higher DAS28 (CRP) (p=0.02) in seropositive patients (table 2).
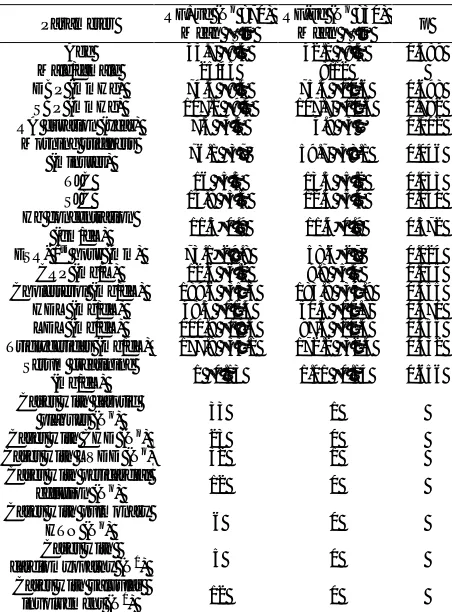
Table 1 Statistical comparison between seropositive and
seronegative patients of the study
Parameter RF+ve (N
o
=70) Mean ±SD
RF-ve (No =30)
Mean ±SD p
Age 43.7 ±8.5 42.1 ±8.5 0.389
Male/female 25/45 8/12
DBP (mmHg) 74.5 ±9.4 75.5 ±10.6 0.698
SBP (mmHg) 107.1 ±9.4 107.7 ±10.6 0.782
RA duration (year) 7.3 ±3.5 4.9 ±3 0.002
Morning stiffness
(minutes) 76.1 ±37 59.7 ±38.1 0.046
TJC 16 ±5.3 13.5 ±5.2 0.033
SJC 14.8 ±5.3 12.4 ±5.4 0.040
Hb concentration
(gm/dL) 11.5±0.9 11.4±0.9 0.572
ESR- 1st hour (mm) 73.1±29.8 58.6±27 0.024
CRP (mg/L) 12.6 ±6.2 9.8 ±5.5 0.035
Cholesterol (mg/dL) 189.6 ±35.3 183.8 ±34.9 0.455
HDL (mg/dL) 48.5 ±11.4 50.3 ±11.7 0.470
LDL (mg/dL) 100.9 ±19.5 97.6 ±20.3 0.455
Triglycerides (mg/dL) 177.8 ±33.1 172.2 ±32.4 0.432 Serum creatinine
(mg/dL) 1 ±0.13 1.01 ±0.14 0.656
Cases with carotid
plaques (No) 33 1
Cases with CHD (No) 23 0
Cases with LVDD (No) 32 1
Cases with pericardial
effusion (No) 12 0
Cases with pulmonary
HTN (No) 6 0
Cases with
cardiomyopathy (N0) 5 0
Cases with valvular
involvement (N0) 12 0
RF=rheumatoid factor; SBP=systolic blood pressure; DBP= systolic blood pressure; RA=rheumatoid arthritis; TJC tender joint count;
SJC = swollen joint count; ESR=erythrocyte sedimentation rate; CRP=C
23 of the RF +ve patients (32.8%) had CHD. Those patients were significantly older in age, with longer disease duration, had significantly higher DAS28 (CRP), higher ESR, and higher CRP titers. CHD was not diagnosed in seronegative patients (table 3).
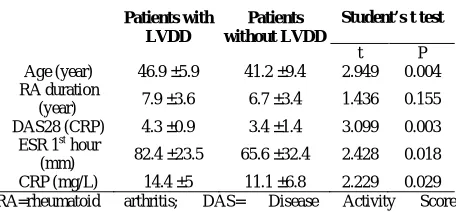
Only a single case with seronegative disease had LVDD. Conversely, 44.28% of the RF +ve patients had LVDD. This was more frequent among male than female patients (45.5% versus 25.4% respectively, p=0.043). RA patients with LVDD were significantly older, had significantly higher DAS28 (CRP), ESR, and CRP than patients without (table 4).
5 of the RF +ve patients had cardiomyopathy(two female patients).Those patients were significantly older with longer disease duration, and higher DAS28 (CRP), ESR, and CRP than rheumatoid patients without cardiomyopathy. The latter was absent among seronegative subjects (table 5).
12% of our patients had pericardial effusion, and 6 patients had pulmonary HTN. All were positive for Rf. No significant difference regarding age, gender, duration of RA or its activity parameters between patients affected by either of them and other patients. Lastly, 12 of the RF +ve patients (17%) had valvular involvement (6 male and 6 female patients). Patients with valvular involvement were significantly older with increased disease duration, and had significantly higher DAS28 (CRP), ESR, and CRP than patients without valvular involvement (p<0.001 for each). None of the RF –ve patients had valvular involvement.
DISCUSSION
Rheumatoid arthritis is a chronic inflammatory disease of the joints with extra-articular features. One of the prognostic extra-articular features of RA is histological vasculitis with associated CVD12.The present study revealed that atherosclerosis was the most common CVD encountered with rheumatoid patients. Increased IMT was detected in 51% of the study population, and carotid plaques were found in 34% of them. Salmon JE and Roman MJ (2008) Stamatelopoulos KS et al (2009) reported the prevalence of plaques among patients with RA to be 44% and 48% respectively13, 14. Conversely, Gerasimova EV et al. (2014) found that only 17% of patients with RA had carotid plaques15. The lower rate of carotid plaques in that study can be attributed to its lower percentage of males compared to ours (13% versus 33% respectively). Also, Pereira IA et al. (2009) found that 47% of the RA patients had increased IMT while only 14.1% had carotid plaques. Unlike our study, Pereira IA et al. excluded all patients who had previous history of CVD from their study which may impact their results7.
This study revealed that atherosclerosis was significantly associated with higher DAS28 (CRP), RF positivity, male gender and older age. Patients with atherosclerosis showed, however, non-significant increase of the disease duration, ESR and CRP than patients without. These results are in agreement with that reported by Pereira IA et al. (2009)7. The positive relationship between the inflammatory burden and the increased IMT has been demonstrated (although mostly throughout acute phase reactant markers)6, 16, 17. Another study found that patients with RA with elevated ESR have a higher rate of atherosclerosis than those without elevated ESR. It reported that this inflammatory marker increased linearly with increased IMT in both patients and healthy controls18.
Figure 1 The frequency of cardiac diseases among rheumatoid patients
of the study.
Table 2 The associations of atherosclerosis with the
clinical and laboratory characteristics among seropositive patients
Patients with Atherosclerosis
Patients without Atherosclerosis
Student’s t test
t p
Age (year) 46.2 ±6.9 41.5 ±9.2 2.397 0.019
RA duration (year) 7.8 ±3.5 6.8 ±3.6 1.254 0.214
DAS28 (CRP) 4.2 ±1.1 3.4 ±1.4 2.390 0.020
ESR 1st hour (mm) 79.2 ±26.7 67.6 ±31.7 1.647 0.104
CRP (mg/L) 14 ±5.7 11.3 ±6.5 1.828 0.072
RA=rheumatoid arthritis; DAS= Disease Activity Score; ESR=erythrocyte sedimentation rate; CRP=C-reactive protein
Table 3 The relations of CHD with the clinical and
laboratory characteristics among seropositive patients
Patients with CHD
Patients without CHD
Student’s t test
t P
Age (year) 47.4 ±5 41.7 ±9.1 2.911 0.005
RA duration (year) 8.5 ±3.5 6.6 ±3.4 2.138 0.036
DAS28 (CRP) 4.4 ±0.8 3.5 ±1.4 3.044 0.003
ESR 1st hour (mm) 86 ±21 66.8 ±31.6 2.648 0.010
CRP (mg/L) 15.1 ±4.6 11.3 ±6.6 2.440 0.017
RA=rheumatoid arthritis; DAS= Disease Activity Score; ESR=erythrocyte sedimentation rate; CRP=C-reactive protein
Table 4 The association of LVDD with the clinical and
laboratory parameters among seropositive patients
Patients with LVDD
Patients without LVDD
Student’s t test
t P
Age (year) 46.9 ±5.9 41.2 ±9.4 2.949 0.004
RA duration
(year) 7.9 ±3.6 6.7 ±3.4 1.436 0.155
DAS28 (CRP) 4.3 ±0.9 3.4 ±1.4 3.099 0.003
ESR 1st hour
(mm) 82.4 ±23.5 65.6 ±32.4 2.428 0.018
CRP (mg/L) 14.4 ±5 11.1 ±6.8 2.229 0.029
RA=rheumatoid arthritis; DAS= Disease Activity Score; ESR=erythrocyte sedimentation rate; CRP=C-reactive protein
Table 5 The relations of cardiomyopathy with the clinical
and laboratory characteristics among patients with +ve RF
Patients with cardiomyopathy
Patients without cardiomyopathy
Student’s t test
t p
Age (year) 54.2 ±2.4 42.9 ±8.2 3.049 0.003
RA duration
(year) 11.6 ±1.7 6.9 ±3.4 2.999 0.004
DAS28 (CRP) 5.5 ±0.3 3.7 ±1.3 3.129 0.003
ESR 1st hour
(mm) 106 ±9.3 70.6 ±29.4 2.671 0.009
CRP (mg/L) 20.7 ±2.2 11.9 ±6 3.2 44 0.002
In agreement with our results, Sahari NS et al. (2014) reported that seropositive RA patients had significantly higher rate of atherosclerosis as compared with seronegative patients and the disease activity was independently associated with thickened carotid IMT19. Also, Boyer JF et al. (2011) found that male gender and older age are risk factors for the development of atherosclerosis in RA patients20. Hjeltnes G et al. (2011) stated that immune system plays an important role in the development of atherosclerosis and associated complications. Immunological abnormalities such as auto-antibodies production may be involved in endothelial dysfunction and the progression of atherosclerotic plaque21.
Indeed, it has been demonstrated that RF is an independent risk factor for ischemic heart disease, even in the absence of RA22. In our results, 23% of patients had CHD. The occurrence of coronary ischemia was associated with older age, increased disease duration, and markers of disease activity (DAS28 (CRP), ESR, and CRP). These associations were reported by other studies23-25. Isolated LVDD occurs frequently without clinically recognized HF, and is one mechanism for the excess development of HF in patients with RA26.In the present study, LVDD was diagnosed in 32% of the patients constituting the second prevalent CVD. A comparable figure (31%) was reported by Liang KP et al. (2010)27. Other studies reported higher prevalence (43% and 47.2%) 28, 29. Indicators of diastolic function used in their study are different than that used in our study.
It has been suggested that cardiac affections are likely to be caused by the chronic inflammation of the rheumatoid disease as this heart impairment was correlated to the time-integrated markers of inflammation30. In our study, RA patients with LVDD had significantly higher DAS28 (CRP), ESR and CRP, and were significantly older in age than RA patients without LVDD. Also RA patients with LVDD were more frequent in male and seropositive patients. These results confirm that reported by Sharma A et al. (2015) who assessed the LVDD and its predictors in RA, and found that LVDD had significant association with age, and DAS28. Moreover, Garza-García C et al (2013) investigated the echocardiographic abnormalities in 105 patients with RA and found theLVDD to be associated with RF positivity31. Conversely, Abdul Muizz AM et al
(2011) found no association between the LVDD and the DAS28. The patients having history or presented with clinical CVD were excluded from that study29.
Sadeghi s et al. (2015) reported that RA patients with pulmonary HTN tended to be older in age than those without pulmonary HTN32. Udayakumar N et al (2008), on the other hand, found a strong association between pulmonary HTN and disease duration among patients with RA5. Our study, however, showed that RA patients with pulmonary HTN had non-significant relations regarding the age or duration of the disease with respect to patients without pulmonary HTN. Only 6 patients were affected by pulmonary HTN in our study, and this may explain this negative significance.
Our results showed that RA patients who had cardiomyopathy had significantly higher DAS28 (CRP) and higher CRP level. These results are consistent with the results of Sen D et al. (2014) who reported that cardiomyopathy was significantly associated with RA activity33.
Finally, our results revealed that 12% of the RA had pericardial effusion. All were positive for RF. Cauduro SA et
al. (2006) found that 80% of the RA patients with pericardial effusion had +ve RF test34.
CONCLUSION
Data of this study indicate that Egyptian patients with RA were prone to a wide range of CVD, yet atherosclerosis was the most prevalent. Seropositivity, rheumatoid activity and duration, male gender and age of the patient were implicated in the risk for CVD, confirming that the underlying inflammatory process of the RA plays an important role in that risk. DAS28 (CRP) was the most sensitive indicator of subsequent CVD in those patients in comparison with isolated acute phase reactants. Subjects with RA having high DAS should be screened for subclinical CVD.Further studies are still required to determine the link between chronic inflammation and the initiation and progression of CVD.
Declaration of interest: there is no conflict of interest that
could be perceived as prejudicing the impartiality of the research reported.
Funding: This research did not receive any specific grant from
any funding agency in the public, commercial or not-for-profit sector.
Disclosure Statement: The authors have nothing to disclose.
References
1. del Rincón ID, Williams K, Stern MP, Freeman GL, Escalante A. High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheum. 2001 Dec; 44(12):2737-45.
2. Gullick NJ, Scott DL. Co-morbidities in established rheumatoid arthritis. Best Pract Res ClinRheumatol. 2011 Aug;25(4):469-83.
3. Nicola PJ, Crowson CS, Maradit-Kremers H, Ballman KV, Roger VL, Jacobsen SJ, Gabriel SE Contribution of congestive heart failure and ischemic heart disease to excess mortality in rheumatoid arthritis. Arthritis Rheum. 2006 Jan; 54(1):60-7.
4. Correa de Sa DD, Hodge DO, Slusser JP, Redfield MM, Simari RD, Burnett JC, Chen HH Progression of preclinical diastolic dysfunction to the development of symptoms. Heart. 2010 Apr; 96(7):528-32.
5. Udayakumar N, Venkatesan S, Rajendiran C. Pulmonary hypertension in rheumatoid arthritis--relation with the duration of the disease. Int J Cardiol. 2008 Jul 21;127(3):410-2. Epub 2007 Aug 8.
6. Gonzalez-Gay MA, Gonzalez-Juanatey C, Piñeiro A, Garcia-Porrua C, Testa A, Llorca J. High-grade C-reactive protein elevation correlates with accelerated atherogenesis in patients with rheumatoid arthritis. J Rheumatol. 2005 Jul; 32(7):1219-23.
7. Pereira IA, Laurindo IM, Zimmermann AF, Werner Castro GR, Mello F, Borba EF Single measurements of C-reactive protein and disease activity scores are not predictors of carotid atherosclerosis in rheumatoid arthritis patients. ActaReumatol Port. Jan-Mar 2009;34(1):58-64.
classification criteria for rheumatoid arthritis: methodological report phase I. Ann Rheum Dis. 2010 Sep;69(9):1589-95.
9. van der Heijde DM, van 't Hof MA, van Riel PL, Theunisse LA, Lubberts EW, van Leeuwen MA, van Rijswijk MH, van de Putte LB. Judging disease activity in clinical practice in rheumatoid arthritis: first step in the development of a disease activity score. Ann Rheum Dis.
1990 Nov;49(11):916-20.
10.Wells G, Becker JC, Teng J, Dougados M, Schiff M, Smolen J, Aletaha D, van Riel PL. Validation of the 28-joint Disease Activity Score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann Rheum Dis. 2009 Jun;68(6):954-60.
11.Bots ML, Baldassarre D, Simon A, de Groot E, O'Leary DH, Riley W, Kastelein JJ, Grobbee DE. Carotid intima-media thickness and coronary atherosclerosis: weak or strong relations? Eur Heart J. 2007 Feb;28(4):398-406. Epub 2007 Feb 2
12.Gonzalez A, MaraditKremers H, Crowson CS, Ballman KV, Roger VL, Jacobsen SJ, O'Fallon WM, Gabriel SE. Do cardiovascular risk factors confer the same risk for cardiovascular outcomes in rheumatoid arthritis patients as in non-rheumatoid arthritis patients? Ann Rheum Dis. 2008 Jan;67(1):64-9
13.Salmon JE, Roman MJ. Subclinical atherosclerosis in rheumatoid arthritis and systemic lupus erythematosus.
Am J Med. 2008 Oct;121(10 Suppl 1):S3-8.
14.Stamatelopoulos KS, Kitas GD, Papamichael CM, Chryssohoou E, Kyrkou K, Georgiopoulos G, Protogerou A, et al. Atherosclerosis in rheumatoid arthritis versus diabetes: a comparative study. ArteriosclerThrombVasc Biol. 2009 Oct;29(10):1702-8.
15.Gerasimova EV, Popkova TV, Novikova DS, Nasonov EL. Cardiovascular diseases in patients with rheumatoid arthritis during long-term methotrexate therapy. TerArkh.2014;86(5):26-31.
16.Bonetti PO, Pumper GM, Higano ST, Holmes DR Jr, Kuvin JT, Lerman A. Noninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemia. J Am CollCardiol. 2004;Dec 7; 44(11):2137-41.
17.Mohan A, Sada S, Kumar BS, Sarma KV, Devi BV, Rao PV, Rajasekhar D, Katyarmal DT. Subclinical atherosclerosis in patients with rheumatoid arthritis by utilizing carotid intima-media thickness as a surrogate marker. Indian J Med Res. 2014; Sep;140(3):379-86. 18.Libby P. Role of inflammation in atherosclerosis
associated with rheumatoid arthritis. Am J Med. 2008;Oct; 121(10 Suppl 1):S21-31.
19.Sahari NS, Shaharir SS, Ismail MR, Rajalingham S, Mohamed Said MS. Subclinical atherosclerosis among rheumatoid arthritis patients without overt cardiovascular risk factors. Mod Rheumatol.2014;24(6):920-5.
20.Boyer JF, Gourraud PA, Cantagrel A, Davignon JL, Constantin A. Traditional cardiovascular risk factors in rheumatoid arthritis: a meta-analysis. Joint Bone Spine.2011; 78:179-83.
21.Hjeltnes G, Hollan I, Førre Ø, Wiik A, Mikkelsen K, Agewall S Anti-CCP and RF IgM: predictors of impaired
endothelial function in rheumatoid arthritis patients.
Scand J Rheumatol. 2011;Nov; 40(6):422-7
22.Edwards CJ, Syddall H, Goswami R, Goswami P, Dennison EM, Arden NK, Cooper C; Hertfordshire Cohort Study Group. Rheumatoid factor may be an Independent risk factor for ischaemic heart disease.
Heart. 2007; Oct;93(10):1263-7.
23.Kobayashi H, Giles JT, Polak JF, Blumenthal RS, Leffell MS, Szklo M, Petri M, Gelber AC, Post W, Bathon JM. Increased prevalence of carotid artery atherosclerosis in rheumatoid arthritis is artery-specific. J Rheumatol. 2010; Apr; 37(4):730-9.
24.Evans MR, Escalante A, Battafarano DF, Freeman GL, O'Leary DH, del Rincón I. Carotid atherosclerosis predicts incident acute coronary syndromes in rheumatoid arthritis. Arthritis Rheum. 2011;May;63(5):1211-20. 25.Chen Y, Dawes PT, Packham JC, Mattey DL. Interaction
between smoking and polymorphism in the promoter region of the VEGFA gene is associated with ischemic heart disease and myocardial infarction in rheumatoid arthritis. J Rheumatol. 2011;May;38(5):802-9.
26. Redfield MM, Jacobsen SJ, Burnett JC Jr. Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic.
JAMA.2003;289(2):194-202.
27.Liang KP, Myasoedova E, Crowson CS, Davis JM, Roger VL, Karon BL, Borgeson DD, Therneau TM, Rodeheffer RJ, Gabriel SE Increased prevalence of diastolic dysfunction in rheumatoid arthritis. Ann Rheum Dis. 2010; Sep;69(9):1665-70..
28.Sharma A, Kaushik R, Kaushik RM, Kakkar R Echocardiographic evaluation of diastolic dysfunction in rheumatoid arthritis - a case-control study. Mod Rheumatol. Jul. 2015;25(4):552-7.
29.Abdul Muizz AM, MohdShahrir MS, Sazliyana S, Oteh M, Shamsul AS, Hussein H A cross-sectional study of diastolic dysfunction in rheumatoid arthritis and its association with disease activity. Int J Rheum Dis.
2011;Feb;14(1):18-30.
30.Tomáš L, Lazúrová I, Oetterová M, Pundová L, Petrášová
D, Studenčan M Left ventricular morphology and
function in patients with rheumatoid arthritis. Wien KlinWochenschr.2013; May;125(9-10):233-8.
31.Garza-García C, Rocío S, Orea-Tejeda A, Castillo-Martínez L, Eduardo C, López-Campos JL, Keirns-Davis C. Risk factors for asymptomatic ventricular dysfunction in rheumatoid arthritis patients. ISRN Cardiol. 2013;Dec 3;:635439.
32.Sadeghi S, Granton JT, Akhavan P, Pasarikovski CR, Roos AM, Thenganatt J, Moric J, Johnson SR. Survival in rheumatoid arthritis-associated pulmonary arterial hypertension compared with idiopathic pulmonary arterial hypertension. Respirology.2015;Apr;20(3):481-7. 33.Sen D, González-Mayda M, Brasington RD Jr.
Cardiovascular disease in rheumatoid arthritis. Rheum Dis
Clin North Am. 2014;Feb;40(1):27-49.
34.Cauduro SA, Moder KG, Luthra HS, Seward JB Echocardiographically guided pericardiocentesis for treatment of clinically significant pericardial effusion in
rheumatoid arthritis. J Rheumatol.
ABBREVIATIONS
CHD =coronary heart disease CRP = C-reactive protein CV = cardiovascular
CVD = cardiovascular disorders DAS = disease activity score DD = diastolic dysfunction
ESR = erythrocyte sedimentation rate GH = general health
HF = heart failure HTN = hypertension.
IL = interleukin
IMT = Intima media thickness LV = left ventricle
LVDD = left ventricular diastolic dysfunction MI = myocardial infarction
RA=rheumatoid arthritis RF= rheumatoid factor TJC = tender joint count
SJC = swollen joint count