Clinical Correlation of Upper
Gastrointestinal Endoscopic
Biopsies with Histopathological
Findings and To Study the
Histopathological Profile of
Various Neoplastic and
Non-Neoplastic Lesions
Copyright © 2016 INTRODUCTION
The pathological conditions of upper gastrointestinal tract (GIT) are respon-sible for a wide range of morbidity and mortality and are also most commonly encountered disorder in routine clinical practice1. In 1968, the successful adventure of flexible fibreoptic endoscope had a revolutionary impact on the diagnosis of upper GIT lesions and its histopathological interpretation1. Among various disorders, acid peptic disease is the most common condi-tion world wide often warranting medical and surgical gastroenterology interventions.
The diagnosis of Helicobacter pylori in the gastric biopsy is very crucial from pathologist perspective. H. pylori is known to cause inflammatory as well as neoplastic lesions like adenocarcinoma and gastric lymphoma with asso-ciated morbidities and hence, H. pylori is termed as viral carcinogens2. The severity of histomorphological changes in H. pylori induced infections are variable and graded according to the updated Sydney system1.
Endoscopic visualisation helps in clinical diagnosis, however it often warrants histopathological correlation of biopsy specimen for accurate final diagnosis. This aids in diagnosing the suspected malignancies as well as for
ORIGINAL ARTICLE
Shanmugasamy K1*,
Bhavani K1,
Anandraj Vaithy K1,
Narashiman R2,
Dhananjay S Kotasthane3
1 MD, Assistant Professor, Department
of Pathology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidhyapeeth University, Puducherry, India
2MD, Emeritus Professor, Department of
Pathology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidhyapeeth University, Puducherry, India
3 MD, Professor and HOD, Department
of Pathology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidhyapeeth University, Puducherry, India
Address reprint requests to *Dr. Shanmugasamy K, MD, Assistant Professor, Department of Pathology, Mahatma Gandhi Medical College and Research Institute, SBV University, Pillaiyarkuppam, Puducherry, 607402, India E-mail: samypatho@gmail.com
Article citation: Shanmugasamy K, Bhavani K, Anandraj VK, Narashiman R, Kotasthane DS. Clinical correlation of upper gastrointestinal endoscopic biopsies with histopathological findings and to study the histopathological profile of various neoplastic and non-neoplastic lesions.
J Pharm Biomed Sci2016;06(04): 220–224.
Available at www.jpbms.info Statement of originality of work: The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and that each author believes that the manuscript represents honest and original work.
Sources of funding: None.
Competing interest / Conflict of interest:
The author(s) have no competing interests for financial support, publication of this research, patents, and royalties through this collaborative research. All authors were equally involved in discussed research work. There is no financial conflict with the subject matter discussed in the manuscript.
Disclaimer: Any views expressed in this paper are those of the authors and do not reflect the official policy or position of the Department of Defense.
NLM Title J Pharm Biomed Sci
CODEN JPBSCT
2230-7885 ISSN No
ABSTRACT
Background The pathological conditions of upper gastrointestinal tract (GIT) are responsible for a wide range of morbidity and mortality and are also most commonly encountered disorder in routine clinical practice. Endoscopic visualisation helps in clinical diagnosis, however, it often warrants histopathological correlation of biopsy specimen for accurate final diagnosis. Aim and Objectives To determine the profile of histopathological lesions of upper GIT and to correlate the various histopathological lesions of upper GIT with age, sex and clinical presentation.
Materials and Methods The study was conducted in the Department of Pathology in Mahatma Gandhi Medical College and Research Institute, Puducherry on 115 upper gastrointestinal endoscopic biopsies during the period of 1 year from January 2014 to December 2014. Brief clinical data were documented. The biopsies were examined for various inflammatory and neoplastic lesions. The findings were then correlated with the clinical parameters.
Results and Conclusion Among 115 cases studied, non-neoplastic lesions were more common in gastrointestinal pathological lesions. The prevalence of gastrointestinal pathol-ogy is more common among males around the fourth and fifth decades of life. Dyspepsia and dysphagia were the most significant presenting clinical features. Helicobacter pylori
association was demonstrable in nearly one-fourth of chronic gastritis cases. In gas-tric region, adenocarcinoma was the commonest neoplastic conditions, whereas in the oesophagus, squamous cell carcinoma is the predominant. In duodenum, inflammatory lesions are more common than malignancy.
KEYWORDS endoscopy, histopathology, chronic gastritis, adenocarcinoma
J Pharm Biomed Sci JPBSCT
2230-7885
http://dx.doi.org/10.20936/jpbms/160226
monitoring the course of the disease, response to therapy and to prevent the complications3,4.
AIM AND OBJECTIVES
• To determine the profile of histopathological lesions of upper GIT.
• To correlate the various histopathological lesions of upper GIT with age, sex and clinical presentation. • To evaluate the incidence of H. pylori gastritis among
gastric lesions.
MATERIALS AND METHODS
The study was conducted in the Department of Pathology in Mahatma Gandhi Medical College and Research Institute, Puducherry on 115 upper gastrointestinal endoscopic biopsies during the period of 1 year from January 2014 to December 2014. Brief clinical data including age, sex and clinical symptoms from case records of patients were documented.
Biopsies obtained were oriented, fixed in 10% neu-tral formaldehyde and routinely processed for paraffin tissue embedding. Sections were taken at 5 µ thickness and stained with hematoxylin and eosin (H & E). In addition, a special stain Giemsa was performed to confirm the pres-ence of H. pylori.
The sections were examined for various histopatho-logical features related to gastritis including chronic and mixed inflammatory infiltrates, neutrophilic activity, intestinal metaplasia, atrophy and presence of H. pylori. The sections were also examined for the presence of malignant changes. The findings were then correlated with the age, sex and clinical presentation.
OBSERVATIONS AND RESULTS
The present study including 115 upper gastrointestinal endoscopic biopsies were observed during the period of January 2014 to December 2014 are as follows:
Among 115 cases analysed, higher incidence was observed in fourth and fifth decades of life with male preponderance, as shown in Table 1 and Fig. 1.
Table 1 Age distribution.
Age Frequency %
10–20 1 0.8
21–30 16 14.3
31–40 24 20.8
41–50 32 27.8
51–60 18 15.6
61–70 20 17.3
71–80 2 1.7
>80 2 1.7
Total 115 100
Fig. 1 Gender distribution.
Nearly, a third of cases (39%) dyspepsia was the pre-senting complaints followed by dysphagia (Table 2).
Among all gastrointestinal endoscopic biopsies, gas-tric biopsies constituted of high incidence (70.50%), followed by duodenum biopsies in 18 cases, oesophagus in 11 cases and 5 cases at oesophago-gastric junction as represented in Fig. 2.
Among 11 oesophagus biopsies, 3 cases (27.5%) showed features of reflux oesophagitis and squamous cell carcinoma (SCC)—moderately differentiated in each (Table 3) and Figs. 3–5.
Among 18 duodenum cases in GIT biopsies, 14 were affected by chronic non-specific duodenitis and in addition, 2 cases of chronic duodenitis showed features of dysplasia and superficial erosive duodenitis respec-tively (Table 4) and Figs. 6–9.
The gastrointestinal endoscopic biopsies in 115 cases included 5 cases from OG junction. The disease frequencies were described in Table 5.
Among the overall 115 GIT biopsies, 24 cases fall in the category of neoplastic lesion and the remaining 91 cases in non-neoplastic lesion as shown in Table 6. Table 2 Chief complaints.
Chief complaints Frequency %
Epigastric pain 22 19
Dyspepsia 45 39
Dysphagia 36 31
Hematemesis 6 5.5
Recurrent vomiting 6 5.5
Total 115 100
Fig. 3 Squamous cell papilloma showing classical papillary configuration (H & E, 4×).
Table 3 Frequency and percentage of lesions in the oesophagus.
HPE diagnosis Frequency %
Reflux oesophagitis 3 27.5
Oesophageal candidiasis 2 18
Squamous papilloma 1 9
Ca-in situ: oesophagus 1 9
Squamous cell ca: mod. diff. 3 27.5
Squamous cell ca: poorly diff. 1 9
Total 11 100
Fig. 4 Moderately differentiated squamous cell carcinoma—
oesophagus (H & E, 10×).
Fig. 5 Frequency and percentage of lesions in the stomach.
Table 4 Frequency and percentage of lesions in the duodenum.
HPE diagnosis Frequency %
Chronic non-specific duodenitis 14 78
Chronic duodenitis with dysplasia 2 11
Superficial erosive duodenitis 2 11
Total 18 100
Fig. 6 Chronic gastritis shows lymphocytic infiltration in the lamina
propria (H & E, 40×).
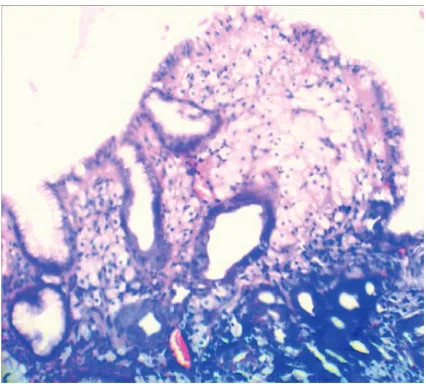
Fig. 7 Helicobacter pylori gastritis (H & E, 40×).
Table 5 Frequency and percentage of lesions in the OG junction.
HPE diagnosis Frequency %
Chronic gastritis 3 60
Reflux oesophagitis 1 20
Adenocarcinoma 1 20
Total 5 100
Table 6 Frequency of neoplastic and non-neoplastic lesions.
HPE diagnosis Frequency %
Neoplastic lesions 24 21
Non-neoplastic lesions 91 79
Total 115 100
Table 7 Neoplastic lesions.
S. no. Site Papilloma Adenomatous polyp Ca-in situ Adenocarcinoma SCC
1. Oesophagus 1 – 1 – 4
2. OG junction – – – 1 –
3. Stomach – 2 – 13 –
4. Duodenum – – 2 – –
Total 1 2 3 14 4
Fig. 9 Xanthelasma of stomach (H & E, 10×).
DISCUSSION
This study was conducted from January 2014 to December 2014 dealing with 115 gastrointestinal endo-scopic biopsies, considering factors like age, sex and clinical symptoms of the patients. Of these case reports considered, 11 cases (9.50%) were oesophagus biopsies, 5 cases (4%) with OG junction biopsies, 81 cases
(70.50%) with stomach and 18 cases (16%) with duo-denum biopsies.
Among the 115 case reports considered, there were 24 neoplastic lesions (21%) and 91 non-neoplastic lesions (79%) were observed.
In the present study, high incidence was observed between the age group of fourth and fifthdecade account-ing for 27.8% of overall case distribution with 32 cases. The age-related difference could be due to varied expo-sure to the risk factors among the different age groups especially in relation to the dietary habits of both qualita-tive and quantitaqualita-tive.
In aspect of sex distribution, male preponderance was noted when compared to female patient with a ratio of 1.5:1. Similar findings were observed in study done by Hussain et al. (2015)5 showing male preponderance. The gender ratio favouring males could be reflective of the fact that males are exposed to more risk factors than female.
In regards to oesophageal biopsies (11 cases), 6 cases showed neoplastic features and 5 with non-neoplastic lesions. The neoplastic lesions were further categorised as SCC moderately differentiated (3 cases), poorly dif-ferentiated SCC (1 case), ca-in situ (1 case) and squa-mous papilloma (1 case). The study is in concordance with observations studied by Sheik et al. (2015)1 in which neoplastic lesions were predominant (Table 7).
Of the 115 gastrointestinal endoscopic biopsies, 5 cases (4%) were found to be represented from OG junction. Among these 5 cases, 3 cases (60%) were affected by chronic gastritis, 1 case showed features of mucin secreting moderately differentiated adeno-carcinoma and the remaining 1 case showed features of reflux oesophagitis as similar to the result found in Sheikh et al. (2015)1.
Among the 115 cases, 18 were found to be affected by duodenum with non-neoplastic lesions. In this study, chronic duodenitis were 78% as similar to Hussain et al. (2015)5. From the remaining cases, 1 case with chronic duodenitis with dysplasia and the other one with super-ficial erosive duodenitis.
Incidence of neoplastic lesions was more common in stomach and the most common lesion was adenocarci-noma. Among 14 cases of adenocarcinoma, 13 cases were seen in stomach and 1 case in OG junction which was in concordance with Poudel et al. (2013)4 were adenocarci-noma was the maximum. Among this 14 cases of adeno-carcinoma, predominant were of moderately differentiated type which was also in concordance with other studies8–10.
CONCLUSION
The prevalence of GIT pathological lesions and associated morbidity is on higher margins among the tropical coun-tries. Endoscopic procedure in adjunction with histo-pathological interpretation remains as a mainstay of diagnostic modality. The prevalence of gastrointestinal pathology is more common among males around the fourth and fifth decades of life. Dyspepsia and dysphagia were the most significant presenting clinical features. H. pylori association was demonstrable in nearly one-fourth of chronic gastritis cases. In gastric region, adenocarci-noma was the commonest neoplastic conditions, whereas in the oesophagus, squamous cell carcinoma is the pre-dominant. In duodenum, inflammatory lesions are more common than malignancy.
REFERENCES
1. Sheikh BA, Hamdani SM, Malik R. Histopathological spec-trum of lesions of upper gastrointestinal tract: a study of endoscopic biopsies. Global J Med Public Health. 2015;4(4): 1–8.
2. Duduyemi BM, Ojo BA, Olaomi OO, Atiba AS. Histopathological pattern of endoscopic gastric biopsy in a district hospital in Nigeria: a review of 118 consecutive cases. Am J Med Biol Res. 2014;2(3):83–86.
3. Godkhindi VM, Meshram DP, Deshpande SA, Kadam PN, Chavan YH. The histopathological study of various gastroduodenal lesions and their association with Helicobacter pylori infection. IOSR J Dent Med Sci (IOSR-JDMS). 2013;2(3):51–55.
4. Poudel A, Regmi S, Poudel S, Joshi P. Correlation between endo-scopic and histopathological findings in gastric lesions. J Univ College Med Sci. 2013;1(3):37–41.
5. Hussain SI, Reshi R, Akhter G, Beigh A. Clinico histopathlogical study of upper gastrointestinal tract endoscopic biopsies. Int J Cur Res Rev. 2015;7(16):78–85.
6. Venugopal LS, Rao BS. Endoscopic biopsies of lower 1/3rd
oesophagus and gastric lesions and its clinic-pathological
correlation with Helicobacter pylori. IJRRMS. 2013;3(3):42–44.
7. Rashmi K, Horakerappa MS, Karar A, Mangala G. A study on his-topathological spectrum of upper gastrointestinal tract endo-scopic biopsies. Int J Med Res Health Sci. 2013;2(3):418–424. 8. Rumana M, Khan AR, Khurshid N. The changing pattern of
oesophago-gastric cancer in Kashmir. JK Pract. 2005;12(4): 189–192.
9. Marson BC, Dawson IMP. Gastrointestinal pathology, 2nd ed. London: Black Well Scientific Publications; 1998. pp. 148–151. 10. Mills SE, Carter D, Greenson JK, Oberman HA, Reuter V, Stoler MH.