Original Research Article
Evaluation of a maternal, neonatal and child health intervention
package in a rural district of Pakistan: a quasi-experimental study
Muhammad Atif Habib
1*, Kirsten I. Black
2, Camille Raynes Greenow
3, Mushtaq Mirani
1,
Sajid Muhammad
1, Fariha Shaheen
1, Monika Christofori Khadka
4, Annette Vondeling
4,
Shabina Ariff
1, Sajid Bashir Soofi
1INTRODUCTION
Pakistan is one of the main countries contributing to the global burden of maternal, neonatal and child morbidity and mortality.1,2 The present MMR, NMR and U5MR in
Pakistan is 178 per 100,000 live births, 42 per 1000 live births and 74 per 1,000 live births respectively.2-4 The recent countdown report for MDGs in Pakistan shows that Pakistan did not achieve the targets related to maternal and under-five mortality.4 The leading causes of
ABSTRACT
Background: Pakistan is among the countries which have the highest maternal, neonatal and child mortality rates. Immediate efforts are required to enable Pakistan to achieve the health related sustainable development goals. The continuum of care interventions can substantially reduce the mortality burden, however local evidence to implement them is lacking in Pakistan. We implemented the maternal, neonatal and child health intervention package comprised of health facility strengthening, capacity building, continuum of care interventions and community mobilization and evaluated its effectiveness on maternal, neonatal and child health care practices and neonatal mortality.
Methods: The intervention package was delivered through existing public health system in a rural district of Pakistan. We used a quasi-experimental design to assess the impact of interventions. Baseline and end line surveys were conducted and neonatal mortality was considered as the primary outcome measure. Data were analysed using bivariate and difference and difference analysis techniques.
Results: We found a reduced risk of neonatal mortality (RR 0.704; 95% CI 0.557-0.889; p=0.0033), in intervention areas compared to control area. For secondary outcomes; including mortality for infants and under five children, antenatal care, skilled birth attendance, institutional deliveries, postnatal care, delayed bathing, inappropriate cord care practices, birth asphyxia, exclusive breastfeeding and immunization a significant difference (p<0.001) was observed in the intervention area compared to control area.
Conclusions: This study provides local evidence from Pakistan that effective methods for delivering MNCH interventions within the existing health infrastructure can improve the MNCH outcomes especially in the rural areas.
Keywords: Maternal, Neonatal and child health, Intervention package, Quasi experimental study, Rural Pakistan
1Centre of Excellence for Women and Child Health, Aga Khan University, Pakistan
2Discipline of Obstetrics, Gynaecology and Neonatology, Central Clinical School, University of Sydney, Sydney
NSW, Australia
3Sydney School of Public Health, University of Sydney, Sydney NSW, Australia 4Swiss Red Cross, Berne, Switzerland
Received: 01 August 2019
Revised: 19 September 2019
Accepted: 20 September 2019
*Correspondence:
Dr. Muhammad Atif Habib, E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
maternal mortality in Pakistan are haemorrhage, eclampsia and sepsis and these are closely related to the causes of neonatal deaths which are preterm birth, sepsis and birth asphyxia.2,5 The post neonatal causes for the under-five deaths in Pakistan are mainly diarrhea and pneumonia.2,3 The majority of these morbidities and mortalities are preventable with a range of evidence based interventions proposed by the World Health Organization
(WHO).6 However, the coverage of these key
interventions in Pakistan remains low.2,3 Furthermore the inequalities outlined in the Pakistan demographic and
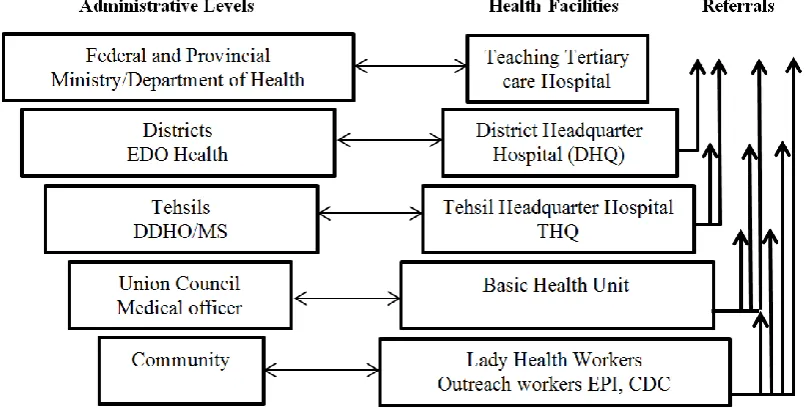
health survey between the urban and rural utilization of health services pose a substantial challenge to improving the MNCH indicators.3 Pakistan has a three tier public health system comprised of primary, secondary and tertiary health care facilities (Figure 1) supported by community based health care workers including the lady health workers and the community midwives.7-9 However due to the lack of resources (financial and human) and political commitment, this health infrastructure is not fully functional and is likely to be a major deterrent factor in achieving the health related SDGs for 2030.2,9
Figure 1: Administrative and health infrastructure of Pakistan. Source: Regional Health Systems Observatory- WHO EMRO. Health Systems Profile- Pakistan 2007.
Community-based packages including promotion of essential interventions and community mobilization of MNCH care practices have been effective in improving maternal, neonatal and child health and survival in low income countries.10-12 In Pakistan evaluation of such interventions has been limited to evaluation of individual interventions or interventions targeting a specific period of care and evidence from studies evaluating the whole continuum of care for MNCH is limited.2,13-17 Given the high burden of MNCH issues and lack of evidence for the provision and effectiveness of continuum of care, we implemented and evaluated a community based MNCH intervention package; comprised of health facility strengthening, capacity building, MNCH interventions targeting continuum of care and community mobilization. The aim of this study was to implement the MNCH intervention package and to evaluate its effectiveness on MNCH care practices and neonatal mortality.
METHODS
Study design, setting and population
We conducted pretest/post-test quasi experimental design with a non-equivalent control group. The interventions
were delivered between January 2013 and August 2015 in selected union councils of taluka (sub-district) Khairpur Nathan Shah of district Dadu which is a rural district of Sindh province in Pakistan (Figure 2). Women and children under five years were eligible for inclusion.
Description of the project
During the devastating floods of 2011 in Pakistan the taluka Khairpur Nathan was badly affected and most of the health infrastructure was non-functional.18 Given the poor health care situation, we delivered the MNCH intervention package in five of the badly damaged union councils (union council is the smallest administrative unit in Pakistan with an average population of 25000). We selected five union councils in the neighboring taluka Meher of district Dadu as a control area for comparison (Figure 2).
Situation analysis and intervention package
each union council and the taluka headquarter hospital (secondary care hospital). These health facilities were partially functional with very little support to MNCH services (Table 1). Our MNCH intervention package targeted the communities and health facilities and
comprised a four prong approach which is described below. The union councils of the control area continued to receive standard MNCH care through the public health care system.
Figure 2: Map of Pakistan, district Dadu and study talukas. Source: https://www.britannica.com/event/Pakistan-Floods-of-2010.
Table 1: Household socio demographic characteristics.
Variables Intervention area Control area
Household visited 15618 15081
Completed 15589 15076
Population 128655 117342
HH density 33450 29835
Married women of reproductive age 15-49 years with birth outcome in last
one year 3177 3018
Married women of reproductive age 15-49 years with live birth in last one
year 3071 2916
Mean maternal age 26.8±7.2 26.2±7.8
Education level of women N (%) N (%)
Illiterate 2017 (63.5) 1877 (62.2)
Primary or less (1-5 years of schooling) 515 (16.2) 534 (17.7)
Middle(6-8) 280 (8.8) 226 (7.5)
Matric(9-10) 203 (6.4) 235 (7.8)
Intermediate & above (>10) 162 (5.1) 145 (4.8)
Wealth quintiles
Poorest 534 (16.8) 495 (16.4)
Poor 677 (21.3) 676 (22.4)
Middle 635 (20.0) 613 (20.3)
Rich 696 (21.9) 619 (20.5)
Richest 632 (19.9) 616 (20.4)
Intervention union councils Gozo, Chorre, Burira, Khandechuki, Bhugio
Control union councils Ghai Mehesar, Khan Jo Goth, Kazi Arif, Kolachi
and Mangwani
Variables Intervention area Control area
WASH indicators N (%) N (%)
Access to protected toilet 1944 (61.2) 2176 (72.1)
Access to improved water 2780 (87.5) 2924 (96.9)
Treats water to make it safe 197 (6.2) 238 (7.9)
Hand washing after defecation 3107 (97.8) 3015 (99.9)
Hand washing before preparation of meal 3148 (99.1) 3006 (99.6)
Availability of soap 1643 (51.7) 1977 (65.5)
Health infra-structure
Number of functional basic health units for MNCH services 02 05
Number of functional tehsil headquarter hospital for MNCH services 00 01
Number of female doctor (public sector) 02 07
Number of functional LHWs 68 76
Health facility strengthening
To provide a conducive working environment the study team renovated the buildings of all five Basic Health Units and the taluka headquarter hospital Khairpur Nathan Shah and also provided WHO recommended basic equipment and medicines for each health facility.19 We also provided a team of lady health visitors (LHVs) for community and facility based activities. The LHVs usually provide a variety of services to communities, including basic nursing care, maternal child health services, and training of community workers and they also manage normal labor and delivery.20 One LHV was based at each basic health unit and three LHVs for community based activities (home based care and referrals) linked to the Basic Health Unit in each union council. Further, to operationalize the 24 hours MNCH services at the taluka headquarter hospital we employed three LHVs, one gynecologist and one pediatrician.
Capacity building
The master trainers of the Aga Khan University and Ministry of Health Pakistan provided a range of training to the project and public health care providers in the targeted areas. The health care providers were trained on basic and comprehensive emergency obsterics and newborn care, integrated management of neonatal and childhood ilnesses, essential neonatal care and helping babies breath using the standard WHO curricula.21
Community and facility based interventions
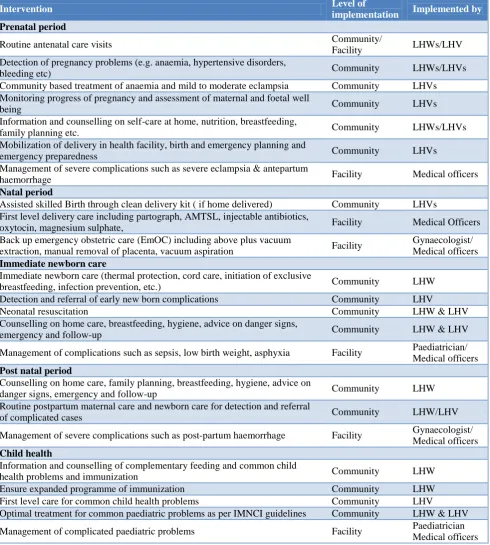
The project team developed the range of interventions targeting the continuum of care approach on the basis of the WHO recommended interventions for MNCH care and survival.6 The interventions were targeted to prenatal, natal, post-natal and child health care and were implemented by the lady health workers, LHVs and health facility staff. The interventions are described in Table 2. The field based study LHVs in collaboration with the government lady health workers identified pregnant women and visited them on a monthly basis to provide health and nutrition education and counseling
during pregnancy and after delivery. The LHVs ensured that pregnant women and their neonates in the intervention group received the appropriate care, including antenatal care, skilled birth attendance, institutional delivery and a postnatal check within two days of birth. They also counseled and supported mothers about early neonatal care, exclusive breastfeeding and appropriate cord care practices. The LHVs further provided education and counseling to families about the childhood vaccination program in Pakistan.22 and referred the children for immunization to the nearest vaccination centers. The LHVs built a critical link between lady health workers, communities and health facilities to maximize referrals of complicated cases to the health facilities for proper and timely management.
Community mobilization
We developed a community mobilization plan and used community health committees in each of the union councils to engage the communities. The community health committees comprised of medical officers from the basic health unit, lady health supervisors, religious and community leaders and elders, these groups then formed male groups at the village level and conducted MNCH sessions. Further, female support groups were held at the village level on various MNCH topics using flip charts and posters. An emergency fund was established with the help of local philanthropists and community health committee members in each union council. Money was then made available to low-income families to cover expenses related to transportation and medication in the case of a medical emergency that required urgent transportation.
Evaluation of the project
Table 2: MNCH intervention package (continuum of care interventions).
Intervention Level of
implementation Implemented by
Prenatal period
Routine antenatal care visits Community/
Facility LHWs/LHV
Detection of pregnancy problems (e.g. anaemia, hypertensive disorders,
bleeding etc) Community LHWs/LHVs
Community based treatment of anaemia and mild to moderate eclampsia Community LHVs
Monitoring progress of pregnancy and assessment of maternal and foetal well
being Community LHVs
Information and counselling on self-care at home, nutrition, breastfeeding,
family planning etc. Community LHWs/LHVs
Mobilization of delivery in health facility, birth and emergency planning and
emergency preparedness Community LHVs
Management of severe complications such as severe eclampsia & antepartum
haemorrhage Facility Medical officers
Natal period
Assisted skilled Birth through clean delivery kit ( if home delivered) Community LHVs
First level delivery care including partograph, AMTSL, injectable antibiotics,
oxytocin, magnesium sulphate, Facility Medical Officers
Back up emergency obstetric care (EmOC) including above plus vacuum
extraction, manual removal of placenta, vacuum aspiration Facility
Gynaecologist/ Medical officers
Immediate newborn care
Immediate newborn care (thermal protection, cord care, initiation of exclusive
breastfeeding, infection prevention, etc.) Community LHW
Detection and referral of early new born complications Community LHV
Neonatal resuscitation Community LHW & LHV
Counselling on home care, breastfeeding, hygiene, advice on danger signs,
emergency and follow-up Community LHW & LHV
Management of complications such as sepsis, low birth weight, asphyxia Facility Paediatrician/
Medical officers
Post natal period
Counselling on home care, family planning, breastfeeding, hygiene, advice on
danger signs, emergency and follow-up Community LHW
Routine postpartum maternal care and newborn care for detection and referral
of complicated cases Community LHW/LHV
Management of severe complications such as post-partum haemorrhage Facility Gynaecologist/
Medical officers
Child health
Information and counselling of complementary feeding and common child
health problems and immunization Community LHW
Ensure expanded programme of immunization Community LHW
First level care for common child health problems Community LHV
Optimal treatment for common paediatric problems as per IMNCI guidelines Community LHW & LHV
Management of complicated paediatric problems Facility Paediatrician
Medical officers
Sample size
We estimated a sample size of 2800 eligible mothers (married woman of reproductive age 15-49 years with a birth outcome in the last one year) in the intervention area and similar number in the control area for the baseline and end line surveys. This sample size estimation was based on the NMR (55/1000 live births), with power set at 80%, margin of error of 5%, design effect of 1.5 and a
non-response rate of 5%.3 We aimed to detect a change of 20% in NMR and 50% in skilled birth attendance. We distributed the required sample size across the union councils proportionally, based on population size.
Selection of household and respondent
was defined as the household with at least one married woman of reproductive age (15-49 years) with a birth outcome in the previous year. On the day of the survey, the enumerators, after informed consent collected data from eligible women using the structured questionnaire. In case of more than one eligible woman in the target household one woman was selected randomly.
Data collection
The baseline and end line surveys were conducted using structured questionnaires, based on the Pakistan Demographic and Health Survey questionnaire.3 The survey questionnaire was translated into the local
language and was then back translated into English. The
questionnaire collected information on
socio-demographic characteristics, reproductive history and service utilization (see outcomes below). The data were collected by a team of female enumerators who were independent of the intervention implementation team. For data collection we deployed one team comprised of a team leader and two enumerators for each union council in both the intervention and control areas (ten team leaders and 20 enumerators in total). We conducted thorough training of all enumerators, including survey methodology and the data collection process. After the training, pilot data was collected in the non-sampled areas followed by a review of data collection procedures.
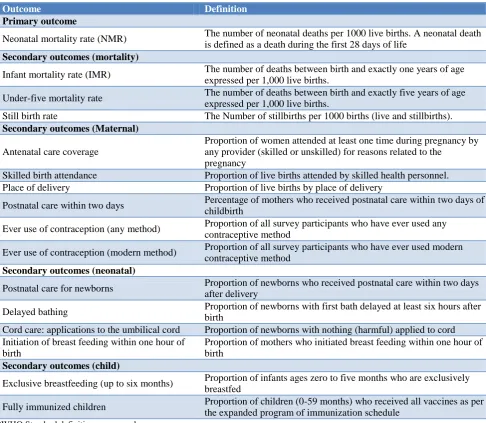
Table 3: Study outcomes and operational definitions.
Outcome Definition
Primary outcome
Neonatal mortality rate (NMR) The number of neonatal deaths per 1000 live births. A neonatal death
is defined as a death during the first 28 days of life
Secondary outcomes (mortality)
Infant mortality rate (IMR) The number of deaths between birth and exactly one years of age
expressed per 1,000 live births.
Under-five mortality rate The number of deaths between birth and exactly five years of age
expressed per 1,000 live births.
Still birth rate The Number of stillbirths per 1000 births (live and stillbirths).
Secondary outcomes (Maternal)
Antenatal care coverage
Proportion of women attended at least one time during pregnancy by any provider (skilled or unskilled) for reasons related to the
pregnancy
Skilled birth attendance Proportion of live births attended by skilled health personnel.
Place of delivery Proportion of live births by place of delivery
Postnatal care within two days Percentage of mothers who received postnatal care within two days of
childbirth
Ever use of contraception (any method) Proportion of all survey participants who have ever used any contraceptive method
Ever use of contraception (modern method) Proportion of all survey participants who have ever used modern contraceptive method
Secondary outcomes (neonatal)
Postnatal care for newborns Proportion of newborns who received postnatal care within two days
after delivery
Delayed bathing Proportion of newborns with first bath delayed at least six hours after
birth
Cord care: applications to the umbilical cord Proportion of newborns with nothing (harmful) applied to cord Initiation of breast feeding within one hour of
birth
Proportion of mothers who initiated breast feeding within one hour of birth
Secondary outcomes (child)
Exclusive breastfeeding (up to six months) Proportion of infants ages zero to five months who are exclusively breastfed
Fully immunized children Proportion of children (0-59 months) who received all vaccines as per
the expanded program of immunization schedule
*WHO Standard definitions were used.
Outcome variables
Outcome variables were categorized to those related to the mortality and MNCH service utilization and are explained in Table 3. The primary outcome variable for
contraceptives. For neonatal outcomes, birth asphyxia, delayed bathing, initiation of breastfeeding within one hour of birth, cord care practices and postnatal care for newborn by a skilled health care provider within two days of birth were assessed. For children we evaluated the exclusive breastfeeding rate and childhood immunization status.
Statistical analysis
After careful checking all paper based data, were double entered in a pre-built data entry program using Visual Fox Pro. Data were analyzed using SPSS version 19.23 We estimated the outcome indicators using the definitions described in Table 3. Population means, frequencies and proportions were calculated for data descriptions. We estimated the relative risk and compared among groups for mortality indicators along with the 95% confidence intervals and p-values. Bivariate analysis was undertaken
to determine associations between the MNCH
intervention package and the MNCH outcomes by comparing baseline and end line outcome variables in the intervention and control areas. The chi-square test was used to determine the significance of differences in the
dependent outcome proportions. A p<0.05 was
considered statistically significant. We used the difference in differences (DiD) analysis to test whether women and children residing in the areas where the intervention was provided benefited.24 The DiD was defined as the changes (end line minus baseline) in the outcome variables in intervention areas minus those in the control areas. The DiD analysis used the baseline and end line observations to estimate the effect of the intervention in “exposed” individuals relative to the comparison of “unexposed” individuals. We used 5% significance level and 95% confidence interval to report the DiD. A negative DiD represented a reduction and a positive DiD represented an increase in the outcome of interest.
Ethical approval
The Ethical Review Committee of the Aga Khan University granted approval for the study (2787-Ped-ERC-13). We obtained written informed consent from eligible women. In the case of illiterate women, consent was documented by a thumbprint on the consent form as well as a signature by a literate witness. All the names and personal information regarding the participants were kept confidential and the data was kept anonymous for analysis. All study activities followed the guidelines of Good Clinical Practice; the project protocol was
registered as a non-randomized trial with the
ClinicalTrials.gov, NCT02797353.
RESULTS
Study population and baseline characteristics
The sample size of the baseline and end line surveys was met and the refusal rate was low (<1%). In the baseline survey we interviewed a total of 3177 eligible women in
the intervention area and 3018 in the control area. Of these women, a total of 3071 (96.7%) in the intervention area and 2916 (96.6%) in the control area had a live birth. In the end line survey the total eligible women in the intervention and the control areas were 3093 and 2982 respectively. Of these women 3026 (97.8) and 2878 (96.5) had live births in the intervention and control areas
respectively (Figure 3). The socio-demographic
characteristics were comparable between the intervention and control areas (Table 3). The mean maternal age was 26.8±7.2 years in the intervention area and 26.2±7.8 years in the control area. The educational level and wealth quintiles in both areas were also similar with the majority of women being illiterate (63.5% in the intervention area and 62.2% in the control area). Among the water sanitation and hygiene indicators, women in the control area had greater access to sanitation and improved water. The health infrastructure was also found to be better in the control area with more functional health facilities and greater human resource for MNCH services.
Relative risk for mortalities
We found a reduced risk of neonatal mortality (RR 0.704; 95% CI 0.557 - 0.889; p=0.0033), infant mortality (RR 0.792; 95% CI 0.654 -0.959; p=0.0171), under five mortality (RR 0.786; 95% CI 0.659 - 0.940; p=0.0082) and stillbirth (RR 0.606; 95% CI 0.447 -0.821; p=0.0012) in the intervention area compared to the control area (Table 4).
Bivariate analysis for other MNCH outcomes
Bivariate analysis revealed that a highly significant proportion of women in the intervention areas than in control areas reported; four or more antenatal care visits during pregnancy (31.4%, p<0.001 cf. 13.5%, p-value 0.026), skilled birth attendance (33.6%, p<0.001 vs. 0.59% p-value 0.909), institutional delivery (31.3%, p<0.001 vs. 0.72%, p 0.864), postnatal care within two days of delivery (57.3%, p<0.001 vs. 1.9%, p<0.074), ever use of any contraceptive method (29.9%, p<0.001 vs. 6.2%, p=0.027 in control area) and ever use of modern contraceptive method (24.1%, p<0.001 vs. 0.8% p=0.130) (Table 5).
Figure 3: Study population.
Table 4: Relative risk estimates for mortality (intervention vs. control) at end line.
Outcome variable Study arm N Rate Relative risk 95% CI P value
Neonatal mortality/ 1000 live births
Intervention group 117 38.8 0.704 0.557 - 0.889 0.0033
Control group 158 55.5 Ref -
Infant mortality/ 1000 live births
Intervention group 180 60.5 0.792 0.654 - 0.959 0.0171
Control group 216 75.2 Ref -
Under five mortality/ 1000 live births
Intervention group 207 68.4 0.786 0.659 - 0.940 0.0082
Control group 250 87.2 Ref -
Still births/ 1000 births
Intervention group 66 21.3 0.606 0.447 - 0.821 0.0012
Control group 105 35.2 Ref -
Study Population District Dadu, Sindh Pakistan
Intervention area Taluka KN Shah
Control area Taluka Meher
Five Union Councils Union councils Gozo, Chorre, Burira, Khandechuki and Bhugio
Five Union Councils
Union councils Ghai Mehesar, Khan Jo Goth, Kazi Arif, Kolachi and Mangwani
Total HH visited (15618) Total HH Completed (15589) Total population (128655) Total WRA 15-49 years (33450) Total WRA with birth outcome in last 1 year (3177)
Total live births (3071)
Total HH visited (15081) Total HH Completed (15076) Total population (117342) Total WRA 15-49 years (29835) Total WRA with birth outcome in last 1 year (3018)
Total live births (2916) Baseline survey
pre intervention
End line survey post intervention
Total HH visited (14815) Total HH Completed (14806) Total population (121409) Total WRA 15-49 years (31566) Total WRA with birth outcome in last 1 year (3093)
Total live births (3026)
Total HH visited (14563) Total HH Completed (14539) Total population (111950) Total WRA 15-49 years (29107) Total WRA with birth outcome in last 1 year (2982)
Table 5: MNCH outcomes and their difference between intervention and control areas at baseline and end line, District Dadu
Intervention area Control area
Indicator Baseline End line Difference P value Baseline End line Difference P value
Maternal indicators
Antenatal care coverage
≥4 times 22.5 53.9 31.4 0.001 32.3 45.8 13.5 0.001
Skilled birth attendance 52.8 86.4 33.6 0.001 57.7 58.3 0.59 0.909
Institutional delivery 48.6 79.9 31.3 0.001 56.4 57.1 0.72 0.862
Post natal care within seven
days 22.3 79.6 57.3 0.001 42.6 44.2 1.9 0.074
Ever use of contraception
(any method) 18.7 48.6 29.9 0.001 24.1 30.3 6.2 0.001
Ever use of contraception
(Modern method) 12.4 36.5 24.1 0.001 16.3 15.5 0.8 0.130
Neonatal indicators
Birth asphyxia 15.6 9.5 6.1 0.001 16.7 16.1 0.6 0.262
Initiation of breast feeding
within one hour of birth 69.7 88.4 18.7 0.001 72.1 75.6 3.5 0.012
Delayed bathing 53.6 77.2 23.6 0.001 59.8 61.6 1.8 0.068
Inappropriate cord care
practice 68.2 28.1 40.1 0.001 65.5 64.3 1.2 0.081
Postnatal care for newborns 18.6 52.4 33.8 0.001 37.2 39.5 0.7 0.077
Child indicators (0-59 months)
Exclusive breast feeding 32.4 68.2 35.8 0.001 36.5 41.1 4.6 0.019
Fully immunized children 50.1 78.3 28.2 0.001 53.6 51.9 1.7 0.068
*Calculated on the basis of total births in last 1 year.
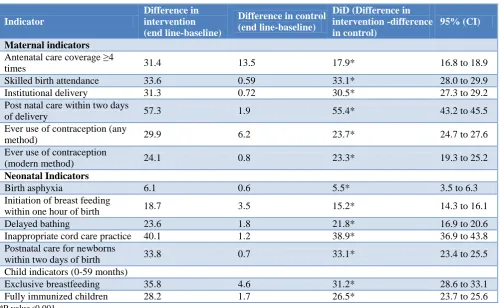
Table 6: DID analysis of the impact of the MNCH intervention package on MNCH indicators in Intervention areas, District Dadu.
Indicator
Difference in intervention (end line-baseline)
Difference in control (end line-baseline)
DiD (Difference in intervention -difference in control)
95% (CI)
Maternal indicators
Antenatal care coverage ≥4
times 31.4 13.5 17.9* 16.8 to 18.9
Skilled birth attendance 33.6 0.59 33.1* 28.0 to 29.9
Institutional delivery 31.3 0.72 30.5* 27.3 to 29.2
Post natal care within two days
of delivery 57.3 1.9 55.4* 43.2 to 45.5
Ever use of contraception (any
method) 29.9 6.2 23.7* 24.7 to 27.6
Ever use of contraception
(modern method) 24.1 0.8 23.3* 19.3 to 25.2
Neonatal Indicators
Birth asphyxia 6.1 0.6 5.5* 3.5 to 6.3
Initiation of breast feeding
within one hour of birth 18.7 3.5 15.2* 14.3 to 16.1
Delayed bathing 23.6 1.8 21.8* 16.9 to 20.6
Inappropriate cord care practice 40.1 1.2 38.9* 36.9 to 43.8
Postnatal care for newborns
within two days of birth 33.8 0.7 33.1* 23.4 to 25.5
Child indicators (0-59 months)
Exclusive breastfeeding 35.8 4.6 31.2* 28.6 to 33.1
Fully immunized children 28.2 1.7 26.5* 23.7 to 25.6
Difference in difference analysis for other MNCH outcomes
The DiD analyses found significant differences (p<0.001) for all MNCH indicators (Table 6). Among maternal outcomes a favourable DiD was seen for four or more antenatal care visits (ANC) (17.9%), skilled birth attendance (33.1%), institutional delivery (30.5%), postnatal care for women within two days of delivery (55.4%), ever use of any contraceptive method (23.7%) and ever use of modern contraceptive methods (23.3%). We also found a favourable DiD among the neonatal outcomes including initiation of breast feeding within one hour of birth (15.2%), delayed bathing (21.8%), postnatal care visit for newborn within two days of birth (33.1%) and a reduction of inappropriate cord care practices (38.9%) and birth asphyxia (5.5%). Among child outcomes a favourable DiD was observed for the proportion of exclusive breastfeeding (31.2%) and fully immunized children (26.5%).
DISCUSSION
Our study demonstrates a significant improvement in the MNCH outcomes in the intervention areas. While control areas also demonstrated improvement in some of the MNCH indicators, this change was small suggesting that the current MNCH program in Pakistan is not sufficient to bring about large improvements especially for mortality indicators. This MNCH intervention package increased utilization of improved health services offered by the study team in collaboration with public health care providers.
Continuum of care from ANC through to child health provides the best outcomes and each component supports and enhances the others resulting in improved MNCH outcomes including mortality.25,26 Our study evaluated the interventions at every level of care and we found significant reductions in NMR, IMR, U5MR and stillbirth rate. Similar reductions in mortality have been documented in previous research in other low and middle income countries.10-16,27,28
Among the components of the continuum of care, ANC plays a critical role in reducing mortality related to the complications occurring during the antenatal period such as eclampsia and antepartum hemorrhage.29 It is an opportunistic period to educate and prepare women for pregnancy and childbirth.29-31 In our study women in the intervention area had more ANC visits from a trained health care provider compared to the control area and this is likely to have contributed to the mortality reduction.32,34 Along with ANC, improved skilled birth attendant is also likely to have contributed to the reduction in mortality. The availability and quality of skilled care around birth is critical in averting maternal and neonatal morbidity and mortality however Pakistan lacks substantially in both the availability and quality of skilled birth care.3,6,10-12
Figure 4: Place of birth in intervention areas baseline vs. end line.
Our intervention package specifically targeted the perinatal period and we significantly improved skilled birth attendance and postnatal care for women. This finding was similar to the studies conducted in neighboring countries.11,12 In the intervention area of our study we also observed a significant shift from home to institutional births. Institutional births provide improved access to a higher level of care. Within the institutional births we further observed a shift from private sector health care provider to public health care provider especially at the taluka headquarter hospital, which was not observed in the control area (Figure 4). This shift also has brought about a significant reduction in the out of pocket expenses required for MNCH care of communities residing in the intervention area, which is a very important finding.
The family planning interventions in the continuum of care play a key role in promoting health and well-being for women and their babies especially in countries like Pakistan where contraceptive prevalence remains low (35.4%) and the unmet need for family planning is high (20.1%) contributing to the high fertility rate (3.8 births per woman).3,35-37 We observed a significant increase in the ever use of any contraceptive method and ever use of a modern method. These gains are in line with the 2020 target of 37.5% contraceptive prevalence rate for married women in Pakistan.38 Our results of improvements in family planning use are also consistent with previous studies.14,36,37
In their recent literature review on neonatal interventions Lassi et al concluded that neonatal morbidity and mortality can be significantly reduced with basic and low cost interventions suggested by the WHO.6,11 However, the reduction depends upon the coverage of the interventions which are low in Pakistan.3,4 Our interventions significantly improved the newborn care practices, including early initiation of breast feeding, delayed bathing and postnatal neonatal care through a skilled person. We also observed a significant reduction
51.4
1.1 4.1
in inappropriate cord care practices and birth asphyxia. Our findings of improved neonatal care practices and reduction in birth asphyxia have been corroborated by previous studies and trials which have been conducted in the similar settings.4-16
Exclusive breastfeeding during the neonatal and post neonatal period and routine immunization for children have profound effects on newborn and child health and survivalbut in Pakistan these have been documented as low, where (38% are exclusively breastfed and only 54% are fully vaccinated.3,39,40 Our interventions resulted in a significant increase in exclusive breastfeeding rates at six months as well as the proportion of fully vaccinated children.
Despite the reduction, mortality in our study area is still higher than targets set for the SDG’s suggesting that there is still a further need to enhance some of the essential interventions especially in the perinatal period. We found that about 46% of women did not receive four or more ANC visits, 20% delivered at home and a similar proportion did not have a post natal care visit. Similarly about 42% of neonates were not examined soon after birth, 32% of children were not exclusively breastfed and 23% were un-immunized. This gap in coverage indicates that to achieve the greatest reductions in mortality more work is needed.
The major strengths of our study were the use of existing public sector health care providers and locally trained LHVs. This was the first time that the complete range of continuum of care interventions was tested in Pakistan. Despite that, our study also had some limitations and the results therefore require some caution. Firstly, we used non-random allocation of the intervention, and a quasi-experimental design for evaluation which may not substantially establish the causal link between the intervention and outcome. However considering the evidence from the systematic reviews and other trialswe consider that this is sufficient evidence of the effectiveness of delivering MNCH interventions within existing infrastructure in Pakistan.10-16 Finally we collected the data using paper based retrospective questionnaires which were subjected to recall bias; however, we believe that this bias was non-differential.
CONCLUSION
Maternal, neonatal, and child morbidity and mortality are persistent challenges in Pakistan, particularly in rural areas due to poverty, lack of education, disparities in health seeking patterns and non-availability of health services. In order to improve coverage of key MNCH interventions and to reduce the mortality burden, Pakistan needs an integrated MNCH strategy with effective community involvement. The current MNCH program in Pakistan fails to offer a holistic approach that combines strengthening health infrastructure, capacity building of staff and delivery of the full range of WHO recommended
continuum of care interventions. Our study provides local evidence from Pakistan that effective methods for delivering MNCH interventions within the existing health infrastructure can improve the MNCH outcomes especially in the rural areas. The MNCH intervention package in our study brought about quality improvements and increased service utilization which stimulated a change in health seeking behavior, which in turn enhanced service utilization, service quality and improved health outcome. This study has provided guidance for future programs and evidence to persuade major stakeholders involved in MNCH care in Pakistan to adopt and scale up this approach in order to achieve the targets of the SDGs.
ACKNOWLEDGEMENTS
This manuscript is a part of MAH’s thesis to fulfill the requirement for a PhD at the University of Sydney. We are grateful to; the Women and Child Health Division, Aga Khan University for providing the support for data collection and analysis, the University of Sydney for funding MAH's PhD scholarship (IPRS/APA) and CRG's funding through an NHMRC career development fellowship #108762. We would like to thank; all the participants who took part in the study, Mr. Qamar Junejo and Mr. Abid Hussain (Field supervisors Aga Khan University) for their support in data collection, Mr. Imran Ahmed for his support in Data management and the study team for their extensive hard work.
Funding: Funded by the Swiss Red Cross, Switzerland Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committeeof Aga Khan University
REFERENCES
1. World Health Organization. Trends in maternal mortality: 1990 to 2015. Estimates by WHO, UNICEF, UNFPA, World Bank Group and the
United Nations Population Division. 2015.
Available at http://apps.who.int/iris/bitstream/ 10665/194254/1/9789241565141_eng.pdf. Accessed on 3 July 2019.
2. Bhutta ZA, Hafeez A, Rizvi A, Ali N, Khan A, Ahmad F, et al. Reproductive, maternal, newborn, and child health in Pakistan: challenges and opportunities. The Lancet. 2013;381(9884):2207-18. 3. National Institute of Population Studies (NIPS) [Pakistan] and ICF. 2018. Pakistan Demographic and Health Survey 2017-18. Islamabad, Pakistan, and Rockville, Maryland, USA: NIPS and ICF. Available at https://www.nips.org.pk/abstract_ files/PDHS%20-%202017-18%20Key%20indicator %20Report%20Aug%202018.pdf. Accessed on 3 July 2019.
fulfilling the health agenda for women and children. The Lancet. 2015;385(9966):466-76.
5. Soofi SB, Ariff S, Khan U, Turab A, Khan GN, Habib A, et al. Diagnostic accuracy of WHO verbal autopsy tool for ascertaining causes of neonatal deaths in the urban setting of Pakistan: a
hospital-based prospective study. BMC Pediatrics.
2015;15(1):1.
6. World Health Organization. WHO recommended
interventions for improving maternal and newborn health: integrated management of pregnancy and childbirth. Available at http://apps.who.int/iris/ bitstream/10665/69509/1/WHO_MPS_07.05_eng.pd f. Accessed on 3 July 2019.
7. Regional Health Systems Observatory- WHO
EMRO. Health Systems Profile- Pakistan 2007. Available at http://apps.who.int/medicinedocs/ documents/s17305e/s17305e.pdf. Accessed on 8 July 2019.
8. Word Health Organization. Pakistan’s lady health
worker programme 2007. Available at
http://www.who.int/workforcealliance/knowledge/ca se_studies/CS_Pakistan_web_en.pdf. Accessed on 12 July 2019.
9. Mumtaz Z, Levay A, Bhatti A, Salway S. Good on paper: the gap between programme theory and real world context in Pakistan’s Community Midwife programme. Br J Obstet Gynaecol. 2015;122(2):249.
10. Lassi ZS, Haider BA, Bhutta ZA. Community-based
intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Systematic Review. 2010;11:CD007754.
11. Lassi ZS, Middleton PF, Crowther C, Bhutta ZA. Interventions to improve neonatal health and later survival: an overview of systematic reviews. EBioMedicine. 2015;2(8):985-1000.
12. Gülmezoglu AM, Lawrie TA, Hezelgrave N,
Oladapo OT, Souza JP, Gielen M, et al. Interventions to Reduce Maternal and Newborn Morbidity and Mortality. Reproductive, Maternal, Newborn, and Child Health. 2016:115.
13. Jokhio AH, Winter HR, Cheng KK. An intervention
involving traditional birth attendants and perinatal and maternal mortality in Pakistan. New England J Med. 2005;352(20):2091-9.
14. Midhet F, Becker S. Impact of community-based interventions on maternal and neonatal health indicators: Results from a community randomized trial in rural Balochistan, Pakistan. Reproductive Health. 2010;7(1):1.
15. Bhutta ZA, Soofi S, Cousens S, Mohammad S, Memon ZA, Ali I, et al. Improvement of perinatal and newborn care in rural Pakistan through community-based strategies: a cluster-randomised effectiveness trial. The Lancet. 2011;377(9763):403-12.
16. Memon ZA, Khan GN, Soofi SB, Baig IY, Bhutta ZA. Impact of a community-based perinatal and newborn preventive care package on perinatal and
neonatal mortality in a remote mountainous district in Northern Pakistan. BMC Pregnancy Childbirth. 2015;15(1):1.
17. Bhutta ZA, Hafeez A. What can Pakistan do to address maternal and child health over the next
decade? Health Res Policy Systems.
2015;13(1):S49.
18. World Bank. 2014. 2011 Pakistan floods:
preliminary damage and needs assessment.
Washington DC; World Bank Group. Available at: http://documents.worldbank.org/curated/en/6557814 68058769881/2011-Pakistan-floods-preliminary-damage-and-needs-assessment. Accessed on 12 August 2019.
19. World Health Organization. Priority life saving medicines for women and children. 2012. Available at http://apps.who.int/iris/bitstream/10665/75154/1/ WHO_EMP_MAR_2012.1_eng.pdf. Accessed on 3 August 2019.
20. Upvall MJ, Sochael S, Gonsalves A. Behind the mud walls: The role and practice of lady health visitors in Pakistan. Health Care Women Int. 2002;23(5):432-41.
21. Word Health Organization. Maternal, newborn, child and adolescent health, Documents on training. Available at: http://www.who.int/maternal_child_ adolescent/documents/training/en/. Accessed on 3 August 2019.
22. Masud T, Navaratne KV. The Expanded Program on
Immunization in Pakistan: Recommendations for Improving Performance. Health, Nutrition and Population (HNP) discussion paper. 2012. World
Bank, Washington, DC. Available at:
https://openknowledge.worldbank.org/handle/10986 /13579. Accessed on 3 August 2019.
23. IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp. 24. Lechner M. The estimation of causal effects by
difference-in-difference methods. Foundations and Trends in Econometrics. 2011;4(3):165-224. 25. Yeji F, Shibanuma A, Oduro A, Debpuur C, Kikuchi
K, Owusu-Agei S, et al. Continuum of care in a maternal, newborn and child health program in Ghana: Low completion rate and multiple obstacle factors. PloS one. 2015;10(12):e0142849.
26. Owili PO, Muga MA, Chou YJ, Hsu YH, Huang N,
Chien LY. Associations in the continuum of care for maternal, newborn and child health: a population-based study of 12 sub-Saharan Africa countries. BMC Public Health. 2016;16(1):1.
27. Das JK, Lassi ZS, Salam RA, Bhutta ZA: Effect of community based interventions on childhood diarrhea and pneumonia: uptake of treatment modalities and impact on mortality. BMC Public Health. 2013;13(Suppl 3):S29.
29. World Health Organization: Antenatal Care in Developing Countries: Promises, Achievements and Missed Opportunities. Geneva; 2003.
30. Mrisho M, Obrist B, Schellenberg JA, Haws RA, Mushi AK, Mshinda H, et al. The use of antenatal and postnatal care: perspectives and experiences of women and health care providers in rural southern Tanzania. BMC Pregnancy Childbirth. 2009;9:10. 31. Tuladhar H, Dhakal N: Impact of antenatal care on
maternal and perinatal outcome: a study at nepal medical college teaching hospital. Nepal J Obstetr Gynaecol. 2011;6(2):37-43.
32. Swider SM. Outcome effectiveness of community health workers: an integrative literature review. Public Health Nursing. 2002;19(1):11-20.
33. Nemcek MA, Sabatier R. State of evaluation: community health workers. Public Health Nursing. 2003;20(4):260-70.
34. Bhutta ZA, Lassi ZS, Pariyo G, Huicho L. Global experience of community health workers for delivery of health related millennium development goals: a systematic review, country case studies, and recommendations for integration into national health systems. Global Health Workforce Alliance. 2010;1:249-61.
35. Stover J, Ross J. How increased contraceptive use has reduced maternal mortality. Maternal Child Health J. 2010;14(5):687-95.
36. Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths averted by contraceptive use: an analysis of 172 countries. The Lancet. 2012;380(9837):111-25. 37. Tsui AO, Creanga A. Does contraceptive use reduce
neonatal and infant mortality? Findings from a multi-country analysis. InAnnual Meeting of the Population Association of America, Detroit, Michigan, April 2009. Available at http://paa2009. princeton.edu/papers/91181. Accessed on 3 July 2019.
38. Government of Pakistan: Projected trends in CPR 2020. Available at http://www.familyplanning2020. org/entities/97. Accessed on 30 July 2019.
39. Lassi ZS, Mallick D, Das JK, Mal L, Salam RA, Bhutta ZA. Essential interventions for child health. Reproductive health. 2014;11(1):1.
40. Imdad A, Yakoob MY, Bhutta Z. Effect of
breastfeeding promotion interventions on
breastfeeding rates, with special focus on
developing countries. BMC Public Health
2011;11(3):24.