1
DESIGNING RESILIENT SYSTEMS FOR COLLABORATIVE
MATERNAL MENTAL HEALTH
PAR-17-264 (RO1) NIH GRANT APPLICATION
By
Sarah Buisson
A paper presented to the faculty of The University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the
degree of Master of Public Health
in the Department of Maternal and Child Health. Chapel Hill, N.C.
(11/17/17)
Approved by: _ ____
Advisor
__ ______
2
Abstract
Perinatal depression has a significant impact on the health of women and their children.
Recent data from North Carolina has revealed high rates of perinatal depression among low
income women along with low rates of access to mental health services. In order to ensure access
to mental health services for low income women with perinatal depression, this grant application
titled Designing Resilient Systems for Collaborative Maternal Mental Health, was designed in
3
Acknowledgements
I would like to thank Dr. Sarah Verbiest, Dr. Alison Stuebe, Dr. Kirsten Kainz, Dr. Lisa
Zerden and Katherine Bryant for offering me the opportunity to participate in the development of
the RO1 grant proposal which incited this more detailed exploration of grant writing, perinatal
depression, the MOMCare program and the Designing Systems for Collaborative Maternal
Mental Health program. I would also like to thank Dr. Sherri Green and Dr. Sarah Verbiest for
4
Table of Content
Foreword ………..5
Introduction ………..6
o A Call to Actiono Defining Perinatal Depression
o The Risk Factors for Perinatal Depression
o Accessing Effective Treatment for Perinatal Depression o Evidence Based Treatment for Perinatal Depression o The MOMCare Program
Materials and Methods ………...16
o Program Aimso Implementation of the Program o Program Timeline
o Program Partners o Key Indicators
o Innovation and the Program
Results ………....24
o The Grant Writing ProcessDiscussion ………..26
References ………..28
5
FOREWORD
The following paper describes the Designing Resilient Systems for Collaborative
Maternal Mental Health (DRS) grant application for thePAR-17-264 (RO1) NIH grant
opportunity titled “Innovative Mental Health Services Research Not Involving Clinical Trials.”
PAR-17-264 (RO1) is a non-clinical trial research grant opportunity offered by the National
Institutes of Health (NIH) which encourages innovative research related to the development
and/or enhancement of mental health services. In particular, the NIH is seeking to fund research
projects that have a strong ability to inform real-world practice and can be scaled up to diverse
populations and settings.Additional value is placed on applications that involve collaboration
with public and private stakeholders as well as an examination of the service delivery context.
This grant was posted on April 28th, 2017 and will accept applications until September 8th, 2020.
Application due dates occur three times a year on February 5th, June 5th and October 5th.
The NIH RO1 has specific guidelines that outline all the components necessary for the
grant application as well as the format each component should be in. The key components
include the program budget, research plan, key person profile, and a description of recruitment,
retention, milestones and timeline (see appendices 1 and 2). All NIH grant documentation should
be submitted to the online grant portal.
This proposal responds to the NIH’s second research priority to “establish
research-practice partnerships that promote dissemination, implementation, and continuous improvement
of evidence-based mental health services.” Although many of the NIH grant components are
included in this report, this paper purposefully does not follow the NIH grant format to allow for
a more detailed exploration of perinatal depression and the proposed DRS program as well as to
6
INTRODUCTION
A Call to Action
Maternal depression has been identified as a growing area of concern in North Carolina.
According to the 2010 Pregnancy Risk Assessment Monitoring System (PRAMS) data, 75.4% of
North Carolina women, ages 18 to 44, reported feeling down, depressed or sad at least once
since their baby was born; and close to 16% of women reported often feeling down, depressed or
sad since the new baby was born (North Carolina State Center for Health Statistics, 2010).
Contributing to feelings of depression, many women may not have the social support that they
need. In 2010, 14.2% of women 18-44 reported that they did not have adequate social and
emotional support available to them after delivering their baby (North Carolina State Center for
Health Statistics, 2010).
These high rates of maternal depression are particularly alarming as untreated perinatal
depression (PND) can have a devastating effect on the health of women and their children. For
instance, PND has been shown to double the risk for preterm birth and low birth weight (Grote
et al. 2010; Li & Liu, 2009). PND can lead many women to attempt suicide, accounting for up
to 20% of all postpartum deaths (Meltzer-Brody, 2011). As the infant grows older, untreated
PND commonly evolves into major depressive episodes which can impact women’s sensitivity
to their infant’s needs and the bonding between the mother and her infant (Meltzer-Brody,
2011). The impact of maternal depression has been shown to influence children all the way
through adolescence and can increase the risk of mental illness development in offspring
(Meltzer-Brody, 2011). Finally, a women’s relationship with her family, partner and friends
may also be affected by PND, further alienating women from the social support they need
7
Many barriers to accessing mental health care contribute to the high rates of PND. In
particular, North Carolina’s shortages of mental health professionals may be one explanation for
high rates of depressive symptoms as well as low levels of social and emotional support. In 2012,
20.9% of the population in North Carolina faced high shortages of mental health professionals
and 58.0% of the population faced high shortages of prescribing professionals (Substance Abuse
and Mental Health Services Administration, 2012).
To address the high rates of maternal depression, the significant public health impact of
PND, and the scarcity of mental health professionals, the North Carolina Division of Public
Health, the Department of Obstetrics and Gynecology and the Center for Maternal and Infant
Health (CMIH) propose an innovative program titled “Designing Resilient Systems for
Collaborative Maternal Mental Health” (DRS). The program is aimed at enhancing existing
mental health infrastructure by creating more opportunities for mental health providers,
increasing training for PND treatment, and implementing evidence based treatment to provide
more support to women with PND.
Defining Perinatal Depression
There is no definitive consensus on the definition of perinatal depression (PND). While
the last edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) had PND as
its own separate diagnosis, the newest edition of the DSM defines PND as a major depressive
episode that occurs during pregnancy or in the 4 weeks following delivery (American Psychiatric
Association, 2013). In contrast, in clinical practice, practitioners typically consider depressive
8
et al., 2013). The lack of consensus in defining PND has made measuring prevalence, treating
and advocating for women with PND extremely difficult.
Although the symptomatology of PND does not differ from major depressive disorder in
the newest version of the DSM, depression with perinatal onset is unique in several key ways.
For one, the content and focus of the negative thinking of women with PND typically focuses on
motherhood and/or the infant (McLoughlin, 2013). Furthermore, pregnancy, the birth and the
postpartum period can influence how and when women receive their diagnosis. Diagnosis may
be delayed as the experience of several depressive symptoms is fairly common in the first couple
weeks postpartum, and medical treatment during pregnancy and postpartum is often focused on
the infant and on the physical symptoms of the mother-to-be or the postpartum woman
(McLoughlin, 2013). Another key difference is the influence of pregnancy or the postpartum
period on the choice of treatment plan, which must not only manage PND risks, but also remain
acceptable to the woman and safe for the infant (McLoughlin, 2013). Furthermore, mental health
professionals working with patients in perinatal period must also acknowledge the impact of
neuroendocrine changes on the body, the psychosocial adjustments that occur during the
transition to motherhood, the physical changes during pregnancy and postpartum that can bring
about pain or discomfort, the impact of breastfeeding on treatment planning, and the long-term
implications of a history of PND on family planning (American Psychiatric Association, 2013).
In order to effectively treat and diagnose women with PND, these unique aspects of PND must
be understood and acknowledged by providers.
PND can be characterized by a wide range of symptoms. These symptoms can include
low mood, marked diminished interest and pleasure in activities, significant changes in weight,
9
ability to concentrate, recurrent thoughts of death and on occasion psychotic symptoms
(American Psychiatric Association, 2013). Considering the wide range of symptoms, PND may
be expressed very differently across women from different backgrounds and cultures, which may
further prevent some women from accessing the care they need (Noel & Whaley, 2012).
The true prevalence of PND remains unknown. A systematic review on the incidence and
prevalence of PND by Gaynes et al. (2005) identified that throughout the perinatal period, the
prevalence of PND is high, ranging from 6.5% to 19.2%. The incidence of PND is also difficult
to identify; however, research has revealed that 50% of “postpartum” major depressive episodes
begin prior to delivery (Yonkers et al. 2001). Some factors have been shown to increase
women’s risk for developing PND. For instance, 30% of women with a history of depression are
at risk of developing PND (Stowe & Nemeroff, 1995). Furthermore, women with PND have a
higher risk of developing PND in subsequent pregnancies. The risk of recurrence of depression
has been shown to be between 25% and 50% among women with PND (Stowe & Nemeroff
1995, Wisner et al. 2002; Munk-Olsen et al. 2009).
While PND is one of the most common mood disorders in the perinatal period, it often is
comorbid with other mental health conditions such as anxiety and panic attacks. A study by
Miller et al. (2006) revealed that while 19% of postpartum women in their sample exhibited
depressive symptoms, 10% showed symptoms of anxiety and stress without depression, and 7%
showed symptoms of both anxiety and depression. Treating only the depressive symptoms may
therefore not be fully effective in helping women cope with daily functioning. In order for
treatment to be effective providers must understand how PND may be exacerbated by other
10 The Risk Factors for Perinatal Depression
The dysregulation of the reproductive endocrine system has been one possible
explanation for the development of perinatal depression (PND) (Meltzer-Brody, 2011). There
are, however, no conclusive studies that identify the causes for PND. Many studies have
identified factors that may increase a woman’s risk of developing PND during pregnancy or the
postpartum period. The systematic review by Recto and Champion (2017) identified lack of
social support, perceived stress, prior history of depression, and history of sexual or physical
violence as risk factors for PND (Recto & Champion, 2017). According to a study by
Hodgkinson et al. (2014), maternal age may also be a risk factor for the development of PND.
Prevalence rates of PND tend to be higher among adolescents (16-44%) than among older
pregnant and postpartum women (10-20%) (Hodgkinson et al., 2014). Finally, a higher
prevalence of PND has been observed among low income populations. Depressive symptoms
have been reported to affect between 40% and 60% of low-income pregnant and postpartum
women (Earls, 2010). Furthermore, 11% of infants with families below the federal poverty line
have mothers with severe depression while 55% live with a mother who has a less severe form of
depression (Veriker et al., 2010).
When controlling for years of education and socioeconomic status, the prevalence of
PND appeared to be the same among all ethnic and racial groups (Yonkers et al., 2011).
However, it is important to note that in the U.S., due to systemic systems of oppression, a large
proportion of minority groups, have much higher rates of poverty, stress and trauma, and may
therefore experience higher rates of PND (Zayas et al. 2002). Furthermore, as PND can be
expressed differently across populations, minority racial and ethnic groups are commonly
11
Accessing Effective Treatment for Perinatal Depression
Women with perinatal depression (PND) can face many barriers to accessing the
treatment they need including physical and financial barriers, insufficient and ineffective
screening practices, and stigma. Figure 1 reveals the pathways through which different barriers
can impact a woman’s access to mental health treatment.
Figure 1: Barriers to Treatment for Perinatal Depression
Physical and financial barriers are some of the most significant barriers to seeking and
receiving mental health treatment during pregnancy and postpartum. According to Kopelman et
al (2008), the cost of care, lacking insurance, transportation barriers, long waits for treatment and
prior negative experiences with mental health providers prevents many women from seeking and
receiving the care that they need. Access to health insurance, in particular, is key to timely
prenatal and postpartum mental health treatment. Unfortunately, around 58% of prenatal and
postpartum women are vulnerable to insurance disruption due to changes in employment,
income, and program eligibility (Daw et al., 2017). Women receiving Medicaid assistance during
12
coverage. Though Medicaid can support low-income mothers’ access to treatment, the support is
time-limited. Eligible pregnant women are only covered from conception to sixty days
postpartum, after which they must apply once more for Medicaid, obtain private insurance or
become uninsured. For this reason, women on Medicaid during pregnancy have higher rates of
becoming uninsured postpartum and may lack access to timely care (Daw et al., 2017). Recent
research has revealed that up to 55% of postpartum women on Medicaid at delivery experience
at least one uninsured month and 25% experience two or more uninsured months over 6 months
postpartum (Daw et al., 2017). Considering this high rate of disrupted or fragmented
care, providing sufficient mental health care to mothers receiving Medicaid
assistance necessitates finding sustainable mechanisms to support continuity of care.
Another significant barrier to receiving treatment for depression, is lack of depression
screening by providers. According to Yonkers et al (2001), less than half of the women suffering
from PND are screened and treated. Although providers report being supportive of PND
screening (LaRocco-Cockburn et al., 2003), many providers still do not screen for PND using
validated screening tools. A study by Seehusen et al. (2005) revealed that while 70% of
obstetricians/gynecologists and 46% of pediatric providers screened for PND, only 18% used
validated tools for PND. This is particularly troubling as routine clinical evaluation has been
shown to detect only 6.3% of individuals with PND compared to a 35.4% detection rate with a
standardized screening instruments, such as the Edinburgh Postnatal Depression Scale
(Evins, Theofrastous & Galvin, 2000). Without systematic screening, some providers may
misjudge a woman’s need for mental health services. PND symptoms may go unrecognized as
changes in sleep, appetite, and libido can be attributed to the pregnancy or the postpartum period
13
Even when women are screened for depression, this may not necessarily mean they
receive treatment. The study by Marcus et al. (2003) for instance found that while 20% of
pregnant women in the study screened positive for depressive symptoms, only 14% of those
screened received treatment. Despite physical and financial barriers, stigma may also play a role
in women not accessing the treatment they need. Many women are fearful that a diagnosis of
PND would be indicative of an inability to cope as a mother and would lead to the involvement
of child protection services (McLoughlin, 2013). Furthermore, some women may feel
uncomfortable discussing their feelings with their health-care provider (McLoughlin, 2013).
Evidence-Based Treatment for Perinatal Depression
The systematic review by Morrell et al. (2016) revealed that interpersonal psychotherapy
(IPT) was the best treatment approach for women diagnosed with perinatal depression (PND),
followed by person-centered approach therapy (PCA) and cognitive-behavioral therapy (CBT).
According the Interpersonal Psychotherapy Institute, IPT is a time-limited psychotherapy that
focuses on interpersonal issues (Interpersonal Therapy Institute, 2017). In particular IPT focuses
on symptom resolution, improved interpersonal functioning and increased social support. PCA
on the other hand is based on the needs and focus of the patient relying on the establishment of a
non-judgmental and empathic relationship between the therapist and the patient. CBT focuses on
the development of coping strategies, enhancing emotional regulation, and changing unhelpful
behaviors and patterns in cognition.
Considering the significant barriers to accessing health care for patients with PND,
programs that facilitate access to mental health services by increasing the availability of
providers, provider PND screening training, and provider collaboration appear to be crucial to
14
programs that target patient-level barriers through patient engagement and resource provision
were associated with higher rates of mental health care use than screening alone. Furthermore,
interventions that target barriers at the patient, provider and health care system level by
providing patient resources, provider training and by improving access to mental health care
were associated with the best mental health care use outcomes (Byatt et al., 2015). This suggests
that while screening is important to identify women with perinatal depression, system level
changes are necessary to fully address barriers to mental health treatment (Byatt et al 2015).
Using a collaborative care model may therefore be crucial to ensuring the access to mental health
services, particularly for low income women with PND (Katon et al. 1996; Melville et al., 2014).
The MOMCare Program
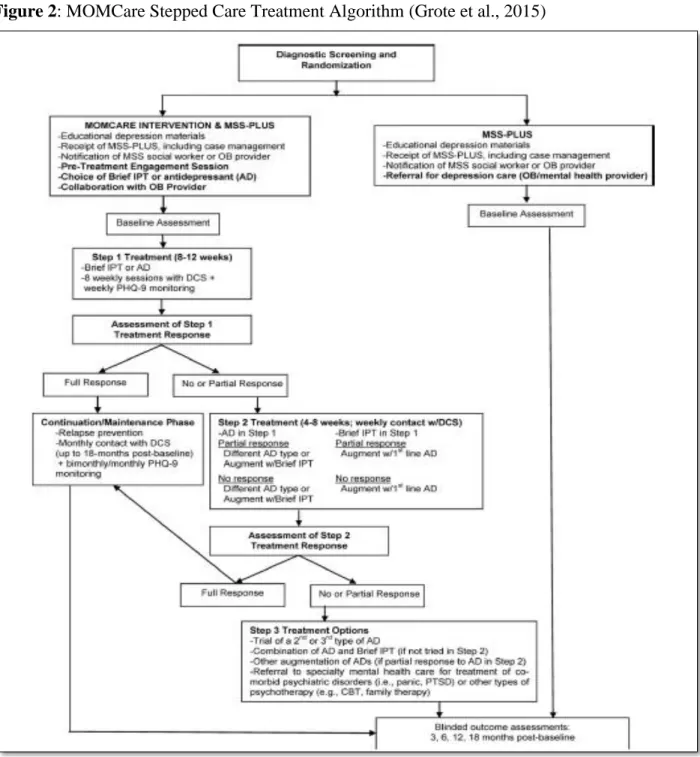
Grote et al. (2015) developed and tested a collaborative care intervention that provided
low-income women with evidenced-based care (IPT and/or antidepressants), systematic
outreach, measurement, and stepped care. As part of the MOMCare program, women were
assigned to a depression care specialist (DCS), a masters prepared social worker, who screened
women for PND, collaborated with women’s OB provider, provided depression care
management and basic case management if needed. When collaborative with women’s OB
provider, the DCS would not only inform he patient’s provider about the MOMCare program,
but also would update the provider on the patient’s progress and collaborate on medication
management if necessary. The MOMCare program offered patients multiple avenues for
treatment, including mental health treatment in public health centers, by phone, in a community
setting, or at home. The MOMCare program included a pre-therapy session that aimed to identify
specific barriers to receiving care, as well as outreach for women who were not attending their
15
IPT sessions administered by the DCS prior to birth as well as IPT maintenance sessions up to
one year postpartum. The MOMCare program ensured the DCS received support from the
program psychiatrist to identify treatment plans and help with medication management. The
stepped-care treatment approach involved weekly monitoring of depressive symptoms, which
helped determine the most effective treatment approach for the patient (see figure 2).
16
The MOMCare program was highly successful in the reduction of depressive symptoms.
The implementation of the MOMCare program was found to significantly lower depression
scores, increase depression remission and increase treatment adherence rates among participants
of the MOMCare program compared to their control group.
Materials and Methods
Program AimsConsidering the high rates of perinatal depressive symptoms in North Carolina and their
impact on maternal health and child development, the goal of the “Designing Resilient Systems
for Collaborative Maternal Mental Health” (DRS) program is to decrease by 25% the prevalence
of perinatal depression in low income women of North Carolina by 2022. This goal is supported
by three program objectives, which include:
Objective 1: To increase the number of mental health providers trained to provide evidence
based treatment for perinatal depression in North Carolina, by offering one interpersonal
psychotherapy (IPT) training for the social work case managers in each of the 14 Community
Care of North Carolina (CCNC) network sites by 2020 (see the Program Partners section for a
description of CCNC).
Objective 2: To increase access and use of mental health services for low income women in the
perinatal period, by implementing the MOMCare program within all 14 CCNC sites over 5
years.
Objective 3: To develop a tailored MOMCare implementation protocol for each network site by
1) identifying each site’s barriers to effective implementation and 2) implementing a systems
17
In order to address the program’s goal and the related objectives, we propose to use
system level quality improvement tools to implement and scale the MOMCare program within
CCNC’s North Carolina Pregnancy Medical Home program. This program will be implemented
to fit within the preexisting infrastructure and the changing context of the North Carolina
Pregnancy Medical Home program.
Program Partners
Partners will be key to the development and implementation of MOMCare in North
Carolina. In particular, Community Care of North Carolina (CCNC), and the UNC PRIME Care
program from the School of Social work have helped us develop a program that could be
integrated within pre-existing programs. A quick description of these two key programs can be
found below:
Community Care of North Carolina (CCNC) is a highly successful statewide medical
home and care management system that served more than 72,000 individuals in 2010. CCNC
has private-public partnerships with 14 network areas across all 100 North Carolina counties
serving Medicaid, and select Medicare populations. An analysis by Milliman Inc. estimated that
CCNC has saved the North Carolina Medicaid program $984 million from 2007 to 2010.
In 2011, CCNC, the NC Division of Medical Assistance and the Division of Public
Health created the Pregnancy Medical Home (PMH) for low income pregnant women on
Medicaid. The PMH program aims to improve the quality of maternity care to advance maternal
and infant outcomes and reduce health care costs. The PMH program partners with more than
350 practices to serve each year approximately 60,000 women with Medicaid coverage who are
pregnant. As part of the Pregnancy Medical Home program, a care manager is assigned to each
18
years, the North Carolina PMH has emerged as a national model for improving perinatal
outcomes (Hillemeier et al., 2017). The CCNC PMH will serve as a home for the implementation
of the MOMCare program in North Carolina.
UNC-PRIME Care is a workforce training program for students in the Social Work
Master’s program that prepares students to deliver integrated behavioral health services in
primary care settings. This program not only provides students with essential skills but also enhances the North Carolina behavioral health workforce. In 2014, the University of North Carolina School of Social Work received a $1.4 million grant from the Health Resources and Services Administration to train and expand the behavioral health workforce. This program was re-funded in 2017. From 2014 to 2018, over 90 students have participated as UNC-PRIME Care trainees. UNC-PRIME Care will strengthen the MOMCare program in North Carolina by guaranteeing that a skilled workforce is available to act as depression care specialist for the program.
Implementation of the Program
To ensure the effective implementation of the MOMCare program in CCNC’s Pregnancy
Medical Home sites, program activities must occur at the level of the depression care specialist,
the CCNC sites, and the overall program. The logic model below depicts in greater detail the
components of this program (see Appendix 4).
At the program level, three teams will lead the implementation of the MOMCare in North
Carolina. These teams will consist of a leadership team, a research team and an intervention
team. The intervention team will be responsible for working with partners, clinic staff and will
support the implementation of MOMCare. The research team will gather and analyze the data
collected during the progressive implementation of MOMCare to generate information on
19
comprised of representatives from all partner organizations to study the evidence generated from
the data and guide decision making on implementation and adaptation of the MOMCare
program.
In order to ensure this program’s success, feedback and support from community
providers as well ask key stakeholders will be crucial. For this reason, community outreach and
in person interviews will form a large part of the program level activities conducted in the first
year of the program. Outreach to community members will further identify possible barriers to
the implementation of the MOMCare program and will offer community members an
opportunity to comment on solutions to remedy these barriers.
The smooth implementation of the MOMCare program into an existing structure, will be
facilitated by a gradual introduction of the program to all CCNC sites through a stepped wedge
evaluation design. Through continuous quality improvement, Plan Do Study Act cycles, as well
as a detailed systems analysis, each site will develop a tailored MOMCare protocol that could be
used to start implementing the MOMCare program at new CCNC sites. The detailed systems
analysis will identify all possible barriers to the implementation of the MOMCare program in
each of the CCNC sites. All sites will be required to submit a quarterly report of quality
improvement activities and results to the research team. The information learned and gathered
through the quality improvement projects will be shared among all sites.
On the ground, all women in the NC Pregnancy Medical Home program will be screened
for depressive symptoms by their assigned case managers. Each patient above a certain threshold
will be referred to a social work depression care specialist (DCS) trained in interpersonal therapy
(IPT). The DCS will engage the patient either in person or by phone, provide psychoeducation,
20
medications or both medications and IPT. The DCS will then monitor the patient’s progress and
adherence to treatment, and consult with the primary care doctor and the psychiatric consultant
for expert advice on medication management and refractory cases.
The implementation of the MOMCare program into the NC Pregnancy Medical Home
will require a trained behavioral health workforce capable of implementing evidence based
treatment of perinatal depression and of collaborating with an interdisciplinary team of primary
care doctors and psychiatrists. The PRIME Care program from the UNC School of Social work
will partner with the MOMCare program and offer social work students the opportunity to work
in an integrated health care setting through their field placement. This collaboration with PRIME
Care will also ensure that there is a steady flow of knowledgeable social workers that could work
as depression care specialists. To ensure that depression care specialists are able to use evidence
based practices for the treatment of perinatal depression, a three-day training will also be
conducted by Dr. Nancy Grote, the principal investigator and one of the key designers of the
original MOMCare program. Similar to the training implemented for the MOMCare program,
the training for this program will involve short courses on motivational interviewing, brief IPT,
and the development of relapse prevention plans. Throughout the program care managers will
receive supervision for their cases and 20% of recorded sessions with patients will be reviewed
for fidelity.
Program timeline
Considering this program involves a state-wide implementation of the MOMCare
program, the proposed program will evolve across five years. The first year will consist mainly
of studying the existing infrastructure, looking for barriers to the implementation of the
MOMCare program, outreach to primary care providers, and training of social work care
21
interested CCNC sites that have capacity and willingness to implement the program. Together,
through continuous quality improvement, these sites will help develop a tailored adaptation of
the MOMCare program that fits with their population and setting. During the second and third
year, monthly Plan Do Study Act cycles will continue to enfold in the four initial sites, and the
program will be expanded to six more sites. Finally, in year four and five, all 14 CCNC sites will
implement the MOMCare program using the tailored adaptations developed by the previous sites
as support to facilitate effective implementation (see Appendix 5).
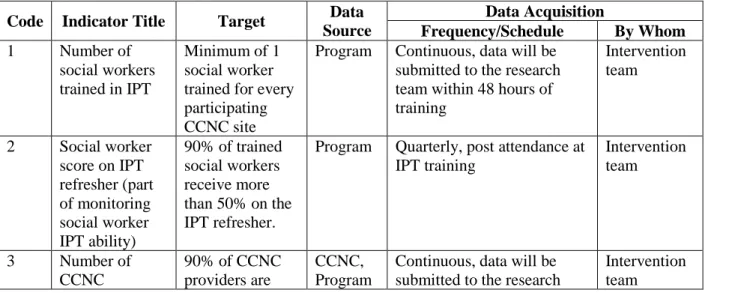
Key Indicators
Throughout this program, data will be continuously collected from the Plan Do Study Act (PDSA) cycles of each CCNC sites and a short analysis will be performed to monitor site’s
progress and effective implementation of the MOMCare program. Monitoring and evaluation
efforts will study consistency in implementing the MOMCare intervention, and evaluate the
impact of the MOMCare intervention on perinatal depression, perinatal depression screening,
and access to mental health services. Information from several key indicators will be collected to
help with monitoring and evaluation efforts (see figure 3).
Figure 3:Program Indicator Matrix
Code Indicator Title Target Data Source
Data Acquisition
Frequency/Schedule By Whom
1 Number of social workers trained in IPT
Minimum of 1 social worker trained for every participating CCNC site
Program Continuous, data will be submitted to the research team within 48 hours of training
Intervention team
2 Social worker score on IPT refresher (part of monitoring social worker IPT ability)
90% of trained social workers receive more than 50% on the IPT refresher.
Program Quarterly, post attendance at IPT training
Intervention team
3 Number of CCNC
90% of CCNC providers are
CCNC, Program
Continuous, data will be submitted to the research
22
providers contacted to educate on the MOMCare program (out of total # of providers that work with CCNC)
contacted and educated on the MOMCare program
team within 48 hours of contact with provider.
4 Number of system analysis conducted per participating CCNC site
A minimum of one system analysis report is completed per CCNC site
CCNC One-time (per site) minimum Research team
5 Number of women in the PMH screened for depression
90% of women in the PMH are screened for depression
CCNC, care managers
Continuous, screening data will be entered into the online data management system
Research team
6 Number of women in the PMH program screened positive for depressive symptoms that receive treatment through the MOMCare program
99% of women who screen positive receive treatment through the MOMCare program
CCNC Continuous, entered into the online data management system
Research team
7 Number of PDSA cycles conducted per month per CCNC site
Each CCNC site has completed a minimum of one PDSA cycle per month
CCNC Monthly, entered into online data management system
Research team
8 Prevalence of perinatal depression among low income women in CCNC’s PMH program The prevalence of perinatal depression reported by low income women in NC decreases by 25%
CCNC Continuous, data entered into the online data management system
Research team
Innovation and the Program
This program is based on two important guiding theoretical models: the dynamic
23
public health programs. Together these theoretical frameworks point to the innovation embedded
into the “Designing Resilient Systems for Collaborative Maternal Mental Health” (DRS)
program both in terms of the structure of the program and the approach to mental health
treatment.
This program will be constructed using the dynamic sustainability framework. The
dynamic sustainability framework is based on the assumption that in order to improve the
sustainability of health interventions these interventions must include continued learning,
problem solving, ongoing adaptation of interventions with a primary focus on fit between
interventions and multi-level contexts (Chambers et al., 2013). Traditionally, health interventions
are expected to perform worse in “real world practice” compared to during research. This
expectation is due to the reality that, in the “real world,” practices typically face more
heterogeneous patient populations, include providers with varying skills and priorities, and are
placed in unique settings with different sets of challenges (Chambers et al., 2013). For research,
health interventions typically demand adherence to lengthy protocols which may be impossible
in real world practice due to stricter financial and time constraints. These assumptions are
particularly relevant to the DRS program as it involves the implementation of a pre-existing
intervention into a new setting (North Carolina), different population, and a new system
(Community Care of North Carolina). Considering these challenges, our program will involve
adaptive, contextually sensitive continuous quality improvement to ensure maximal success and
benefits to the population.
The DRS program is also unique in its approach to mental health treatment which is
based on the social support theoretical framework. Social connection is a basic human need, that,
24
(Harlow & Harlow, 1966). Studies have shown that a lack of social connection is a contributing
factor to higher mortality rates, and greater incidence of infectious diseases while the presence of
social connections can act as a buffer against stress and depression (Uchino, 2006; Hung, 2004)
Considering the significant role of social connection on maintaining both physical and mental
health, it is particularly important to ensure individuals have access to social support during
periods of transition and high adversity, such as the perinatal period. The perinatal period is
marked by increased barriers in accessing a supportive network and stigma for seeking out
support from mental health specialist (Negron et al., 2013). As a consequence, many women in
the perinatal period have very small social support networks (Negron et al., 2013). Through
multiple contacts, psychoeducation, IPT sessions, and case management, this program will
provide women in the perinatal period with enhanced support targeting each of the essential
elements of social support including emotional support, informational support, esteem support
and instrumental support (Fisher et al., 2017).
Results
The Grant Writing ProcessThe process of developing and writing this RO1 grant application ran from early August
2017 until the end of September 2017. The key contributors to the grant included the North
Carolina Division of Public Health, the Department of Obstetrics and Gynecology, the School of
Social Work at UNC Chapel Hill and the Center for Maternal and Infant Health (CMIH). The
group typically met once a week to discuss the progress of the grant writing. The month of
August was mostly focused on developing the conceptual framework of the program and
identifying the ideal partners and methods to implement the MOMCare program in North
25
with the Community Care of North Carolina (CCNC) and identified CCNC as an ideal setting to
implement the MOMCare program. CCNC shared many of the key objectives of this grant which
further facilitated this partnership. Dr. Alison Stuebe, the first PI for this project, had connections
with Dr. Nancy Grote, one of the key creators of the original MOMCare program, who agreed to
provide consulting and training services throughout the length of the program. Dr. Kirsten Kainz,
the second PI for this project, had extensive experience in implementation science and provided
crucial input and direction to ensure the implementation of this program would be sustained
among CCNC’s Pregnancy Medical Home sites. During September different sections of the
grant were written, the letter of intent was submitted, and the letters of support were written and
collected from key partners. Unfortunately, near the end of September, during a call with the
NIH advisor for this program, it was discovered that this application would require more
scientific support to be accepted as an RO1 grant. The NIH advisor suggested that this grant be
re-written to fit the requirements for a R21 grant which would serve as a pilot for a larger RO1
grant. According to Yang. (2012), the R21 is aimed at funding “innovative and high risk
exploratory projects, with high potential impact, while the RO1 provides funding to projects that
are more fully developed and sure to produce progress.” Although this switch did not change the
aims of this grant proposal, due to a more limited budget the implementation of this program had
to be restricted to fewer CCNC sites. It was only due to the team’s passion and dedication to
improving mental health services for women with perinatal depression that the R01 was
modified on such a short notice to fit the R21 requirements. The final version of the R21 grant
26
Discussion
Several key takeaways have evolved out of the development and writing of this grant
application. The first key takeaway is related to the actual writing of the grant application, and
involves the fine balance between clarity and depth. Most grants limit applications to a certain
number of pages to facilitate the review process, and force applicants to distill the program into
only the essential key points. Distilling our proposal to its essential elements was particularly
challenging as the program involved so many different moving parts. While our team had
initially put a lot of research and depth into the program significance and implementation, many
elements were removed from our final draft as they were not essential to the program’s
description. According to Yang (2012), having a strong and precise organization of the grant
application can ensure that a grant application has both depth and clarity. For instance, making
the aims section of the RO1 grant application into a clear summary of the overall project can
allow for a more detailed overview of each individual part of the program in the following
sections of the grant application without leading to confusion. Our grant application used a
similar approach starting with a strong outline of our proposal and developing each section
sufficiently to add depth to the intervention.
The second key takeaway from this grant application involves the grant writing process.
Collecting all the necessary components for a grant application and forming the necessary
partnerships can be extremely challenging, particularly on a short deadline. Although our team
had a little over two months to complete the grant application, it was difficult to collaborate in
creating a vision of the MOMCare program in North Carolina, as each person contributing to the
grant had different schedules, responsibilities, and expertise in different areas. Although our
27
well as the team’s culture ensured success in collecting all the necessary components for this
grant application. Assigning specific sections to different individuals and weekly meetings
helped with distributing the work evenly, and ensured everyone could contribute their expertise
to the grant application. It was particularly helpful that both principal investigators were highly
invested in the grant writing process and receptive to ideas from team members. Despite our best
efforts, we were slightly set back from the call from our NIH advisor. This unexpected situation
revealed the importance of identifying which grant to apply to and how communicating with the
NIH advisor can be extremely helpful in recognizing appropriate funding opportunities.
The last key takeaway from this grant application revolves around partnerships and
networking. The networks of the principal investigators and the networking skills of our team
were perhaps some of the most important elements of this grant application. The support from
different statewide partners gave legitimacy to our team’s ability to implement this program
effectively. Although partnering with community organizations added to the complexity of this
program, using existing community structures that have similar goals and interests enhanced the
sustainability of this proposed program.
To conclude, being part of the development of an NIH grant application was a highly
educational experience that helped me gain a deeper understanding of perinatal depression and of
interventions that could reduce the prevalence of perinatal depression in North Carolina.
Although we will not hear back from the status of the R21 application until March 2018, this
experience has renewed my interest in maternal mental health and has provided me with
28
References
American College of Obstetricians and Gynecologists. (2015). Screening for perinatal
depression. Committee Opinion No. 630. Obstetrics & Gynecology, 125, 1268–1271. Retrieved from http://www.acog.org/ Resources-And-Publications/Committee-Opinions/Committee-onObstetric-Practice/Screening-for-Perinatal-Depression
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Bhat, A., Grote, N. K., Russo, J., Lohr, M. J., Jung, H., Rouse, C. E., … Katon, W. (2016). Collaborative Care for Perinatal Depression Among Socioeconomically Disadvantaged Women: Adverse Neonatal Birth Events and Treatment Response. Psychiatric Services, 68(1), 17–24. https://doi.org/10.1176/appi.ps.201600002
Blom, E., Jansen, P., Verhulst, F., Hofman, A., Raat, H., Jaddoe, V., … Tiemeier, H. (2010). Perinatal complications increase the risk of postpartum depression. The Generation R Study. BJOG: An International Journal of Obstetrics & Gynaecology, 117(11), 1390–1398. https://doi.org/10.1111/j.1471-0528.2010.02660.x
Brennan, P. A., Pargas, R., Walker, E. F., Green, P., Jeffrey Newport, D., & Stowe, Z. (2008). Maternal depression and infant cortisol: influences of timing, comorbidity and treatment. Journal of Child Psychology and Psychiatry, 49(10), 1099–1107.
https://doi.org/10.1111/j.1469-7610.2008.01914.x
Byatt, N., Levin, L. L., Ziedonis, D., Moore Simas, T. A., & Allison, J. (2015). Enhancing Participation in Depression Care in Outpatient Perinatal Care Settings. Obstetrics & Gynecology, 126(5), 1048–1058. https://doi.org/10.1097/AOG.0000000000001067
Chadha-Hooks, P. L., Hui Park, J., Hilty, D. M., & Seritan, A. L. (2010). Postpartum depression: an original survey of screening practices within a healthcare system. Journal of
Psychosomatic Obstetrics & Gynecology, 31(3), 199–205. https://doi.org/10.3109/0167482X.2010.484513
Chambers, D. A., Glasgow, R. E., & Stange, K. C. (2013). The dynamic sustainability
framework: addressing the paradox of sustainment amid ongoing change. Implementation Science, 8(1), 117. https://doi.org/10.1186/1748-5908-8-117
Chew-Graham, C., Chamberlain, E., Turner, K., Folkes, L., Caulfield, L., & Sharp, D. (2008). GPs’ and health visitors’ views on the diagnosis and management of postnatal depression: a qualitative study. British Journal of General Practice, 58(548), 169–176.
https://doi.org/10.3399/bjgp08X277212
Daw, J. R., Daw, Hatfield, L. A., Swartz, K., & Sommers, B. D. (2017). Women In The United States Experience High Rates Of Coverage “Churn” In Months Before And After
29
Earls, M. F. (2010). Clinical Report: Incorporating Recognition and Management of Perinatal and Postpartum Depression Into Pediatric Practice. Pediatrics. Retrieved from
http://pediatrics.aappublications.org/content/early/2010/10/25/peds.2010-2348.abstract
Evins, G. G., Theofrastous, J. P., & Galvin, S. L. (2000). Postpartum depression: A comparison of screening and routine clinical evaluation. American Journal of Obstetrics and
Gynecology, 182(5), 1080–1082. https://doi.org/http://dx.doi.org/10.1067/mob.2000.105409
Field, T. (2011). Prenatal depression effects on early development: A review. Infant Behavior and Development, 34(1), 1–14. https://doi.org/https://doi.org/10.1016/j.infbeh.2010.09.008
Fisher, E.B., Bhushan, N., Coufal, M. M., Kowitt, S., Parada, H., Sokol, R.L., et al. (2017). Peer Support in Prevention, Chronic Disease Management, and Well Being. In E.B. Fisher, L.D. Cameron, A.J. Christensen, U. Ehlert, Y. Guo, B. Oldenburg & F. J. Snoek (eds.),
Principles and Concepts of Behavioral Medicine: A Global Handbook. New York: Springer.
Gavin, N. I., Gaynes, B. N., Lohr, K. N., Meltzer-Brody, S., Gartlehner, G., & Swinson, T. (2005). Perinatal Depression. Obstetrics & Gynecology, 106(5, Part 1), 1071–1083. https://doi.org/10.1097/01.AOG.0000183597.31630.db
Gaynes, B. N., Gavin, N., Meltzer-Brody, S., Lohr, K. N., Swinson, T., Gartlehner, G., … Miller, W. C. (2005). Perinatal depression: prevalence, screening accuracy, and screening
outcomes. Evidence Report/technology Assessment (Summary), (119), 1–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15760246
Grote, N. K., Bridge, J. A., Gavin, A. R., Melville, J. L., Iyengar, S., & Katon, W. J. (2010). A Meta-analysis of Depression During Pregnancy and the Risk of Preterm Birth, Low Birth Weight, and Intrauterine Growth Restriction. Archives of General Psychiatry, 67(10), 1012. https://doi.org/10.1001/archgenpsychiatry.2010.111
Grote, N. K., Katon, W. J., Lohr, M. J., Carson, K., Curran, M., Galvin, E., … Gregory, M. (2014). Culturally relevant treatment services for perinatal depression in socio-economically disadvantaged women: The design of the MOMCare study. Contemporary Clinical Trials, 39(1), 34–49. https://doi.org/10.1016/j.cct.2014.07.001
Grote, N. K., Katon, W. J., Russo, J. E., Lohr, M. J., Curran, M., Galvin, E., & Carson, K. (2015). Collaborative Care for Perinatal Depression in Socio-economically Disadvantaged Women: A Randomized Trial. Depression and Anxiety, 32(11), 821–834.
https://doi.org/10.1002/da.22405
Grote, N. K., Simon, G. E., Russo, J., Lohr, M. J., Carson, K., & Katon, W. (2017). Incremental Benefit-Cost of MOMCare: Collaborative Care for Perinatal Depression Among
30
Harlow, H. F., & Harlow, M. (1966). Learning to love. American Scientist, 54(3), 244–272. Retrieved from http://www.jstor.org/stable/27836477
Henshaw, C. (2003). Mood disturbance in the early puerperium: a review. Archives of Women’s Mental Health, 6, s33–s42. https://doi.org/10.1007/s00737-003-0004-x
Hillemeier, M. M., Domino, M. E., Wells, R., Goyal, R. K., Kum, H.-C., Cilenti, D., & Basu, A. (2017). Does Maternity Care Coordination Influence Perinatal Health Care Utilization? Evidence from North Carolina. Health Services Research. https://doi.org/10.1111/1475-6773.12742
Hodgkinson, S., Beers, L., Southammakosane, C., & Lewin, A. (2014). Addressing the Mental Health Needs of Pregnant and Parenting Adolescents. Pediatrics, 133(1), 114 LP-122. Retrieved from http://pediatrics.aappublications.org/content/133/1/114.abstract
Hung, C.-H. (2004). Predictors of Postpartum Women’s Health Status. Journal of Nursing Scholarship, 36(4), 345–351. https://doi.org/10.1111/j.1547-5069.2004.04062.x
Interpersonal Therapy Institute. (2017). About IPT. Retrieved from http://www.ipt.br/en/institutional
Katon, J. G., Lewis, L., Hercinovic, S., McNab, A., Fortney, J., & Rose, S. M. (2017). Improving Perinatal Mental Health Care for Women Veterans: Description of a Quality Improvement Program. Maternal and Child Health Journal, 21(8), 1598–1605.
https://doi.org/10.1007/s10995-017-2285-0
Katon, W., Robinson, P., M, V. K., & al, et. (1996). A multifaceted intervention to improve treatment of depression in primary care. Archives of General Psychiatry, 53(10), 924–932. Retrieved from http://dx.doi.org/10.1001/archpsyc.1996.01830100072009
Kopelman, R. C., Moel, J., Mertens, C., Stuart, S., Arndt, S., & O Hara, M. W. (2008). Barriers to Care for Antenatal Depression. Psychiatric Services, 59(4), 429–432.
https://doi.org/10.1111/j.1747-0285.2012.01428.x.Identification
LaRocco-Cockburn, A., Melville, J., Bell, M., & Katon, W. (2003). Depression screening attitudes and practices among obstetrician–gynecologists. Obstetrics & Gynecology, 101(5, Part 1), 892–898. https://doi.org/https://doi.org/10.1016/S0029-7844(03)00171-6
Legere, L. E., Wallace, K., Bowen, A., McQueen, K., Montgomery, P., & Evans, M. (2017). Approaches to health-care provider education and professional development in perinatal depression: a systematic review. BMC Pregnancy and Childbirth, 17(1), 239.
https://doi.org/10.1186/s12884-017-1431-4
31
Marcus, S. M., Flynn, H. A., Blow, F. C., & Barry, K. L. (2003). Depressive Symptoms among Pregnant Women Screened in Obstetrics Settings. Journal of Women’s Health, 12(4), 373– 380. https://doi.org/10.1089/154099903765448880
McLoughlin, J. (2013). Stigma associated with postnatal depression: A literature review. British Journal of Midwifery, 21(11), 784–791. Retrieved from
https://auth.lib.unc.edu/ezproxy_auth.php?url=http://search.ebscohost.com/login.aspx?direc t=true&db=rzh&AN=104159054&site=ehost-live&scope=site
Meltzer-Brody, S. (2011). New insights into perinatal depression: pathogenesis and treatment during pregnancy and postpartum. Dialogues in Clinical Neuroscience, 13(1), 89–100. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181972/
Meltzer-Brody, S., Boschloo, L., Jones, I., Sullivan, P. F., & Penninx, B. W. (2013). The EPDS-Lifetime: assessment of lifetime prevalence and risk factors for perinatal depression in a large cohort of depressed women. Archives of Women’s Mental Health, 16(6), 465–473. https://doi.org/10.1007/s00737-013-0372-9
Melville, J. L., Reed, S. D., Russo, J., Croicu, C. A., Ludman, E., LaRocco-Cockburn, A., & Katon, W. (2014). Improving Care for Depression in Obstetrics and Gynecology. Obstetrics & Gynecology, 123(6), 1237–1246. https://doi.org/10.1097/AOG.0000000000000231 Miller, R. L., Pallant, J. F., & Negri, L. M. (2006). Anxiety and stress in the postpartum: Is there
more to postnatal distress than depression? BMC Psychiatry, 6(1), 12. https://doi.org/10.1186/1471-244X-6-12
Morrell, C. J., Sutcliffe, P., Booth, A., Stevens, J., Scope, A., Stevenson, M., … Stewart-Brown, S. (2016). A systematic review, evidence synthesis and meta-analysis of quantitative and qualitative studies evaluating the clinical effectiveness, the cost-effectiveness, safety and acceptability of interventions to prevent postnatal depression. Health Technology
Assessment, 20(37), 1–414. https://doi.org/10.3310/hta20370
Negron, R., Martin, A., Almog, M., Balbierz, A., & Howell, E. A. (2013). Social Support During the Postpartum Period: Mothers’ Views on Needs, Expectations, and Mobilization of
Support. Maternal and Child Health Journal, 17(4), 616–623. https://doi.org/10.1007/s10995-012-1037-4
Noël, L. T., & Whaley, A. L. (2012). Ethnic/Racial differences in depression among U.S. primary care patients: Cultural considerations in screening and detection. Journal of Ethnic and Cultural Diversity in Social Work, 21(4), 314-330. doi:10.1080/15313204.2012.729180
North Carolina State Center for Health Statistics. (2010). 2010 North Carolina Pregnancy Risk Assessment Monitoring System Survey Results: Preconception Health Indicators Women 18-44. Retrieved from
32
Oakhill, E. (2016). Postnatal depression. InnovAiT, 9(9), 531–537. https://doi.org/10.1177/1755738016654292
O’Mahen, H. A., & Flynn, H. A. (2008). Preferences and Perceived Barriers to Treatment for Depression during the Perinatal Period. Journal of Women’s Health, 17(8), 1301–1309. https://doi.org/10.1089/jwh.2007.0631
Paulden, M., Palmer, S., Hewitt, C., & Gilbody, S. (2009). Screening for postnatal depression in primary care: cost effectiveness analysis. BMJ, 339(dec22 1), b5203–b5203.
https://doi.org/10.1136/bmj.b5203
Räisänen, S., Lehto, S. M., Nielsen, H. S., Gissler, M., Kramer, M. R., & Heinonen, S. (2014). Risk factors for and perinatal outcomes of major depression during pregnancy: a
population-based analysis during 2002–2010 in Finland. BMJ Open, 4(11), e004883. https://doi.org/10.1136/bmjopen-2014-004883
Recto, P., & Champion, J. D. (2017). Psychosocial Risk Factors for Perinatal Depression among Female Adolescents: A Systematic Review. Issues in Mental Health Nursing, 38(8), 633– 642. https://doi.org/10.1080/01612840.2017.1330908
Seehusen, D. A., Baldwin, L.-M., Runkle, G. P., & Clark, G. (2005). Are Family Physicians Appropriately Screening for Postpartum Depression? The Journal of the American Board of Family Medicine, 18(2), 104–112. https://doi.org/10.3122/jabfm.18.2.104
Stowe, Z. N., & Nemeroff, C. B. (1995). Women at risk for postpartum-onset major depression. American Journal of Obstetrics and Gynecology, 173(2), 639–645.
https://doi.org/http://dx.doi.org/10.1016/0002-9378(95)90296-1
Substance Abuse and Mental Health Services Administration. (2012). Mental Health, United States 2010. HHS Publications. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from
https://www.samhsa.gov/data/sites/default/files/MHUS2010/MHUS2010/MHUS-2010.pdf
Uchino, B. N. (2006). Social Support and Health: A Review of Physiological Processes
Potentially Underlying Links to Disease Outcomes. Journal of Behavioral Medicine, 29(4), 377–387. https://doi.org/10.1007/s10865-006-9056-5
Vericker, T., Macomber, J., & Golden, O. (2010). Infants of depressed mothers living in poverty: opportunities to identify and serve. The Urban Institute, 1. Retrieved from
https://www.urban.org/sites/default/files/publication/29086/412199-Infants-of-Depressed-Mothers-Living-in-Poverty-Opportunities-to-Identify-and-Serve.PDF
33
Yonkers, K. A., Ramin, S. M., Rush, A. J., Navarrete, C. A., & al, et. (2001). Onset and persistence of postpartum depression in an inner-city maternal health clinic system. The American Journal of Psychiatry, 158(11), 1856–1863. Retrieved from
http://libproxy.lib.unc.edu/login?url=https://search.proquest.com/docview/220460610?acco untid=14244
34
Appendices
Appendix 1: Components of the RO1 grant
1) Letter of Intent (30 days prior to application due date) 2) SF 424 (R&R)
a. Cover letter attachment (optional, recommended) 3) SF 424 (R&R) Project/Performance Site Locations
4) SF 424 (R&R) Other Project Information
a. “Recruitment, Retention, Milestones and Timeline” attachment (no more than 4 pages) b. Project Summary/Abstract (30 lines of text)
c. Project Narrative (3 sentences)
d. Bibliography and References Cited (check bibliography used) e. “Facilities and Other Resources” attachment
f. “Equipment” attachment (as needed) 5) SF424 (R&R) Senior/Key Person Profile
a. Biographical sketch attachment (5 pages per person)
6) R&R (if applying for more than $250,000 per budget period in direct costs) a. Budget Justification
7) R&R Sub-award Budget (as needed) a. Budget Justification (as needed)
b. Biographical sketch attachment (5 pages) (as needed) 8) PHS 398 Cover Page Supplement
9) PHS 398 Research Plan a. Specific aims (1 page) b. Research strategy (12 pages)
i. Significance ii. Innovation iii. Approach
c. “Protection of Human Subjects” attachment d. “Inclusion of Women and Minorities” attachment e. “Inclusion of Children” attachment
f. “Multiple PD/PI Leadership plan” attachment (as needed)
g. “Consortium/Contractual Arrangements” attachment (as needed) h. Leadership plan (as needed)
i. Letters of Support
j. Resource Sharing Plan (Data Sharing Plan) 10)PHS Inclusion Enrollment Report
11)PHS Assignment Request Form (optional, recommended)
35
36
Appendix 3: Letter of Intent
September 5th, 2017
Re: Letter of Intent for R01 “Innovative Mental Health Services Research Not Involving Clinical Trials” PAR-17-264
To whomever this may concern,
This letter is intended to inform you that we plan to submit an application for the PAR-17-264 “Innovative Mental Health Services Research Not Involving Clinical Trials” RO1 tentatively titled “Designing Resilient Systems for Collaborative Maternal Mental Health.” The research team will consist of Alison Stuebe MD (PI), from the Department of Maternal and Child Health, and Kirsten Kainz Ph.D. (PI), from the School of Social Work. Additionally, Sarah Verbiest DrPH, Katherine Bryant MA MSPH, Steve Day M.C.P., Rohit Ramaswamy Ph.D., Samantha Meltzer-Brody MD, Linda Beeber PHD RN CS, Lisa DeSaxe Zerden Ph.D., Chris Ranes RN MSN APRN-BC, and Brad Gaynes MD will all contribute their knowledge and expertise to this project. This project will be submitted through the UNC School of Social Work in partnership with the UNC Center for Maternal and Infant Health. We will be collaborating with Community Care of North Carolina (CCNC) and their Pregnancy Medical Home program, the UNC School of Public Health, the UNC School of Medicine, and the National Implementation Research Network. Together, we propose to enhance the existing CCNC Pregnancy Medical Home program to improve both screening and treatment of perinatal depression.
Perinatal depression is the most common complication of childbirth, affecting one in seven women between conception and 12 months postpartum. This condition is associated with preterm birth, low birth weight, impaired bonding, suicide, and infanticide. Despite these potentially devastating consequences to maternal and infant health, perinatal depression is often unrecognized. Even when identified, most women experiencing symptoms do not receive adequate treatment.
The MOMCare model, developed and tested in the Seattle-King County Public Health system, embedded social workers into the offices of primary care OB providers to treat perinatal depression with the supervision of a psychiatric
consultant. This program was efficacious in addressed the perinatal mental health needs of women in their clinics but has not yet been implemented on a broader scale and in a different context. Our goal is to deploy the MOMCare model within the CCNC Pregnancy Medical Home program to address the unmet perinatal mental health needs of pregnant and parenting women in North Carolina.
The result would be an innovative interdisciplinary approach to perinatal mental health treatment that would be continuously improved to best fit the location of practice and the needs of the population being served. The use of continuous quality improvement will not only ensure that this program is sustainable but also that it could be replicable in a different context.
Thank you for your consideration of this proposal, please let us know if there is anything we can provide to help in the review process.
Sincerely,
Appendix 4: Logic Model
Logic Model
Inputs Activities Outputs Outcomes Impact
Key
stakeholders:
- CCNC
- CCNC partner sites
- NC DMA
- Prime Care
- UNC School of Social Work
- UNC School of Public Health - CMIH Personnel: - Social Workers - Psychiatrists
- Research PIs
- Program consultants
- Clinic staff
- Leadership team
- Research team
- Intervention team
- IPT trainers
Materials:
- Funding
- Online data management system
- IPT training curriculum
- Program consultant and intervention team conducts IPT training for social workers in all 14 CCNC sites
- Trained social workers receive supervision and IPT performance is monitored by research team
- Conduct a systems analysis of the current CCNC structure to identify best implementation course
- Conducting outreach to primary care providers to raise awareness and
understanding of the program through short seminars (online and in person) on the topic.
- Each site will conduct several PDSA cycles of
implementing the program using the A3 format.
- Providing perinatal
depression screening, as well as IPT and case management services to pregnant women on Medicaid
- Entering data collected during in the online data management system
- Monitoring and evaluation of program activities
- Present results to key stakeholders/provide feedback to CCNC locations
- IPT training sessions offered in all 14 CCNC sites
- Systems analysis conducted at CCNC locations
- Primary care providers were reached out to and received
information on the program
- Each site conducted monthly PDSA cycles
- Pregnant women enrolled in Medicaid received IPT and case management services.
- Reports of results were written and presented to key stakeholders and CCNC locations
- Increased number of mental health providers able to provide evidence based IPT treatment to low-income women with perinatal depression.
- Increased access and use of mental health services for low income women with perinatal depression.
DESIGNINGSYSTEMS FOR COLLABORATIVE MATERNAL MENTAL HEALTH 38
38
Appendix 5: Study Milestones and Timeline
Study Activity
Year 1 Year 2 Year 3 Year 4 Year 5
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4