Purpose
To provide an overview of the genetic basis of cystic fibrosis (CF) and some of the issues it presents.
Procedure
1 Read through the play script below, either as a class or in small groups.
Making decisions
Characters
VALERIE a pale, thin woman in her forties.
MATT her husband, about the same age, a cheerful sceptic.
CLAIRE aged twenty, their daughter, whose sister Rachel has cystic fibrosis.
TOM the local vicar, a very good family friend; he and Matt enjoy teasing each other. (A normal kitchen. CLAIRE is sitting at the table drinking a cup of coffee and reading a magazine. Enter VALERIE, looking very tired; she is dressed very smartly and has just returned from visiting family.)
CLAIRE Hello Mum, you look shattered. Want a coffee? The kettle’s just boiled.
VALERIE Yes please dear. (She sits down wearily. CLAIRE gets up and makes a cup of coffee while the following conversation is taking place.) I need to sit down for a bit before I start getting supper. Where’s Dad? He’s usually in by this time.
CLAIRE He’s gone to get an Indian take-away, to save you having to cook tonight. VALERIE That’s nice. I’m so tired.
CLAIRE Why did you go then? Laurie is only a distant cousin isn’t he? I’ve only met him a couple of times.
VALERIE I suppose I think that our families have things in common so want to be supportive. CLAIRE You mean the cystic fibrosis?
VALERIE (Nodding as CLAIRE hands her a cup of coffee) Yes. Thanks dear.
CLAIRE He is a thoroughly miserable little git though, isn’t he? He doesn’t seem to do anything except collect his disability benefit and watch television.
VALERIE (Slightly angry and becoming more so) If you’d had to have physiotherapy which involved being thumped on the back every day of your life, had chronic diarrhoea and other digestive problems, had one chest infection after another knowing that the next one might very well carry you off, been in and out of hospital more times than you could count, had to take antibiotics, digestive tablets and goodness knows what other medication and knew that you were unlikely ever to have children and even more unlikely to reach the age of 40. (Each time she pauses for breath CLAIRE interrupts, but isn’t quick enough) If you’d been waiting for three years for a heart and lung transplant that was your last hope, you might not be the chirpy, happy, life and soul of the party type either.
CLAIRE Spare me the lecture, Mum. I know all about that stuff. Rachel has cystic fibrosis and she’s not like that. She has to have the physiotherapy and I know she’s been pretty ill, but she’s cheerful and happy – usually. And she’s got a good job, and there’s all that music stuff she does.
VALERIE She’s been very lucky. We were always very sensible with her, we were careful, but not too protective.
Salters-Nuffield Advanced Biology Resources
Activity 2.1 Student Sheet(Pause, while they both drink coffee.)
CLAIRE Cousin Laurie is a lot younger than Rachel isn’t he? Is he in a pretty bad way? VALERIE (Exasperated) Yes, Claire, thank you very much, that cheers me up no end. CLAIRE (Hastily) Sorry Mum. (She glances out of the window and turns back to her Mum.)
Brace yourself, Tom’s just coming in the front gate. Shall I tell him you’re not back yet?
VALERIE (Hesitates for a moment then makes up her mind.) No, I’d like a chat with him.
(Exit CLAIRE again, a door bell rings. There is a short, indistinct offstage conversation between CLAIRE and TOM. TOM enters.)
TOM Hello Val, I was going to ask if you could help with the Youth Club this week. Dawn’s gone down with ʼflu but I gather you’ve had a pretty rotten day so I’ll get someone else, it’s no problem.
VALERIE Come and sit down, Tom. I’ll help, though I don’t exactly feel full of joy at the moment. I suppose going to see Laurie brought all the questions back.
TOM (Sitting opposite her) Questions? VALERIE Why do things like cystic fibrosis exist?
TOM If you want a theological answer, there are nearly as many of those as there are theologians, none of them totally convincing, I’m afraid. If you want a scientific answer, isn’t it supposed to give protection against some disease? Typhoid, possibly, or cholera, though that’s not terribly relevant in twenty-first century Britain.
VALERIE (Pause) Did we really do the right thing in bringing Rachel and Claire into the world? Rachel with cystic fibrosis and we know Claire’s got a very high chance of being a CF carrier. And Claire and Nathan are talking about starting a family. Will she have children or grandchildren who have CF as well. (Pause) Matt and I didn’t think we would have more children after Rachel. Then after a couple of years I suddenly found I was pregnant again. One doctor did suggest that we consider an abortion, but Matt and I were both absolutely against it.
TOM And so was I. We really do not have the right to end the life of a fetus just because it isn’t perfect or has a chance of producing children that aren’t. Besides, Rachel and Claire are both super, a credit to you and Matt. Claire’s training to be a biologist and isn’t she interested in research? She might be the one to find an effective cure, perhaps nobody’s children or grandchildren will have to suffer from cystic fibrosis in a few years’ time.
VALERIE She’s got a long way to go yet.
TOM She’ll manage. Seriously, they are quite near to a cure. They know an awful lot about cystic fibrosis these days, don’t they?
VALERIE They know it’s caused by a mutation in a gene. They know exactly where that gene is in a human cell. They know which chromosome it’s on. They know exactly what the gene does. It’s to do with a protein transporting sodium and chloride ions across cell membranes, apparently. They know that 1 in 25 people are cystic fibrosis carriers, which means that about 1 child in 2500 will be born with the disease. In fact, they know just about every damn thing about it except how to cure it, or even treat it effectively.
(There is a crash as the door is kicked open, MATT enters, he half staggers, half falls into the room, his arms full of the brown paper bags that Indian take-aways use.)
MATT Hello dear, did Claire tell you I was getting a take-away? Sorry I took so long, I forgot the rice and had to go back for it. (He sees TOM) Hi Tom, I think I just saw your local fan club members rushing this way. (He starts to unpack the take-away.) TOM No, that was Doris Crane and Phyllis Bendall trotting along to bingo. And I think
perhaps I should be off.
MATT Don’t go, I was looking forward to a good argument.
treatment, he might be much better today. (To TOM) Have an onion bhaji. TOM Thank you. (He takes a bhaji and starts to eat it.) That’s a bit unfair: I’m a vicar
and I don’t object to using the latest drug treatments, transplants, or gene therapy. Laurie’s mother belonged to a rather weird cult called the Divine Temple of Incarnation. Claire would not get mixed up with them.
MATT Oh? I thought I read a letter of yours in the local paper protesting about the GM crop trials.
TOM (Slightly pompously) Gene therapy is a rather different use of genetic engineering and one that hopefully will benefit people in the future, although it doesn’t seem to have helped any cystic fibrosis sufferers yet.
MATT Tom don’t forget that if Laurie receives a heart–lung transplant it would have to come from some healthy young person who would have died in tragic
circumstances.
VALERIE Even so, she could still be a carrier and have a baby with CF.
TOM Could they have genetic screening? You need to have a chat with her and make sure she understands. I must go, thanks for the food. See you later.
MATT Bye Tom.
VALERIE See you on Wednesday at the youth group. Bye. (Exit TOM. MATT has finished unpacking the take-away.)
MATT That’s about ready, I’ll give Claire a call. (CLAIRE bursts in, she is ‘dressed up’.)
CLAIRE Don’t save any for me, I’m just going out. Nathan and I are going for a meal then we are going on to The Warehouse.
MATT Hang on, I got the prawn biryani just for you: we don’t like it.
VALERIE We wanted to have a chat with you about what you were saying the other day about wanting to start a family.
MATT The Warehouse? Isn’t that the new nightclub in town? How are you going to get home? Do you want me to pick you up?
CLAIRE Oh Dad, I’m not a little girl any more. Nathan will bring me back. And don’t worry, we will do the research and make sure we have all the information we need before we make any decisions. Bye.
(Exit CLAIRE, in a hurry)
MATT Let’s hope he’s not a CF carrier. END
The play script contains a lot of information about cystic fibrosis and raises many issues that people with cystic fibrosis have to think about.
2 Read through the play script again on your own and this time underline or highlight the factual biological information about cystic fibrosis and, with another colour, highlight or underline the issues that Valerie, Matt and Claire have to think about.
3 Using these highlighted passages, work with a friend to produce a ‘mind map’ showing how the information you have gathered on cystic fibrosis is linked together.
Salters-Nuffield Advanced Biology Resources
Activity 2.1 Teacher SheetMAKING DECISIONS
Purpose
To provide an overview of the genetic basis of cystic fibrosis and some of the issues it presents.
Notes on the procedure
Discussions and teaching about genetic diseases can be a delicate issue. Many of our students will have personal experience about the diseases or know of friends and relatives who suffer from them or have conditions themselves. This may provide a good source of information for the class on genetic diseases or it may be an issue that a student finds too difficult emotionally to talk about. Teachers must be sensitive to this range of responses to genetic diseases. It may be necessary to make the storyline lower key in the topic by, for example, omitting Activities 2.1 and 2.2. Some teachers suggest that this activity be used later in the topic as a summary activity.
The introduction to this topic is a means of providing an overview and getting students to the same baseline from which the rest of the topic can develop.
The play script deals with information about cystic fibrosis, but tries to give ‘hooks’ on which a lot of the rest of the topic can be attached without giving away too much of the story. The play script can be read through as a class activity, with students taking the roles, or it could be a small group activity so that most students take a role.
The two tasks at the end of the play script are both ways to get students to interrogate the text. The highlighting exercise may be a familiar way of getting students to read a text for meaning and information. The second task encourages students to use ‘mind maps’ as tools for organising
information and ideas. The activity sheet provides a starting ‘mind map’ for the students to complete. It should be stressed that there is no one definitive ‘mind map’, but that any way that organises the information coherently is correct. Students could be encouraged to use ‘mind maps’ as revision tools as well as a mechanism to organise their thoughts and ideas. A good source of information about ‘mind maps’ is the article by Kinchin, I. (2000) Journal of Biological Education 34: 61–68.
Good sources of information about cystic fibrosis are:
The article by Welsh and Smith (Welsh, M.J. and Smith, A.E. (1995). Cystic fibrosis. Scientific American 273: 52–59), and websites in the weblinks that accompany this activity.
Purpose
To find out how cystic fibrosis (CF) affects individuals with the condition by reading some accounts by people affected by CF.
Cystic fibrosis
Cystic fibrosis is not a rare disease. In fact, 1 in 25 people of European descent carry a mutation that results in cystic fibrosis. The people carrying the mutation may not know they do so. Eighty per cent of children with cystic fibrosis are born to parents with no prior history of the disease. People with cystic fibrosis have a median predicted survival of 41 years, but many people live a lot longer than that. In fact, the oldest person to be diagnosed with cystic fibrosis was 82 years old! However, most people with cystic fibrosis are diagnosed within the first few years of life.
Procedure
Read the account and answer the questions that follow. The passage is part of an article written by Kate, a 29-year-old who has cystic fibrosis. It was published in the Daily Mail in 2008.
Living with cystic fibrosis
By Kate Smith
I have cystic fibrosis. It’s an incurable, genetic disease, where sufferers have thick mucus clogging their lungs.
Should both parents have the gene, there is a one-in-four chance their child will have it. I do, but thankfully my younger brother Nick, and elder brother Alex, don’t.
When I was diagnosed at five, the average life expectancy was 17, but each case is different. Improved medication and physiotherapy have changed my life.
Blowing out the candles on my 18th birthday cake felt very good indeed. Given my health problems – I’ve been admitted to hospital at least a dozen times with infections, sometimes for several months – I could have hidden away and given up.
Instead, I have lived life to the full – parties, travel and romance. I love new sports and I’ve been whitewater-rafting, tandem sky-diving and bungee-jumping in Australia. I know I’ve got a lot to pack in.
When I’m asked what is the worst part of my illness, I’d have to say the exhaustion. The rigorous exercise and physiotherapy regime required to help loosen the mucus on the lungs would tire anyone.
It includes swimming, yoga, gym and physiotherapy where the rib cage is beaten with cupped hands. The reduced lung capacity makes it harder still to cope with everyday life, let alone a full-time job.
The effect of absorbing a cocktail of drugs – up to 50 pills a day – plus inhalers, also saps the energy.
The onset of infection will often bring appalling pains in my chest and either side of my spine. Cystic fibrosis affects life in subtler ways, too. I never leave my hair wet, because the cold and damp would make my lungs produce more mucus.
I also avoid mould, especially in fruit, which contains the staphylococcus aureus bacteria that can grow in cystic fibrosis mucus.
Salters-Nuffield Advanced Biology Resources
Activity 2.2 Student SheetThere were no restrictions on me. My mother always threw me into exercise – swimming, dancing, trampolining and gymnastics – and I have continued into adulthood.
Some other parents didn’t get it. I remember one mum telling me I was not to blow up balloons at a party: far too strenuous for a frail little thing like me, she said. Fine, I thought, I’ll sit in the corner, chill out and eat the food.
Of course, my parents didn’t burden me with all the details about the illness immediately but I knew I was different.
When I was 12, I used to tell each of my family before I went to bed that I loved them – just in case I died in my sleep. This was before I understood that sufferers rarely die without warning.
My personality has been shaped by the disease, too. I’ve never taken the small things in life seriously and I am not easily offended or jealous.
At school I was puzzled by my friends’ obsessions with trivia. You’re unhappy with your hair? Really? Oddly, I’ve become more girly in adulthood.
As I moved from school to further education and work, I found grooming and make-up a useful way to cope with the illness.
If I can still be bothered to do my hair and make-up, then I’m not that ill. I might feel awful, but I don’t have to look awful as well.
There were a few times when I was too ill to go to school but I still got two A-levels and a degree in psychology at Kingston University, in South-West London. Students treated me no differently to anyone else, even if my housemates in Kingston could tell when I was in by my coughing.
In my early 20s I worked for the publisher Haymarket, but a severe infection brought on by my illness forced me to quit. Abandoning my career was the hardest decision I’ve made, but there was little choice.
I coughed constantly in the office and was so exhausted one day that I slept under my desk during my lunch break, asking my boss to wake me when he got back.
This might sound odd, but at 23 I retrained as an aerobics teacher. The effort of keeping fit and to a professional standard actually improved my health.
I was able to double my lung capacity – a crucial measure of my fitness – from 1.5 litres to three litres.
I liked the physical challenge, but decided to return to Kingston to do a postgraduate diploma in psychology, at the same time working two days a week in the prison service.
Because I wasn’t earning enough to pay rent, I moved home with my parents in Sunbury-on-Thames, Surrey.
In a funny way, I know I have exceeded my parents’ wildest hopes. When I was diagnosed, I was not expected to make it into my 20s. Every day since has been worthwhile and all the better for their support.
They haven’t batted an eyelid at the extravagant things I’ve done. They even trusted me to go to Ibiza with girlfriends at 16. I just danced the week away. My parents’ trust has made me strong. My illness has always made me value relationships and be wary of fickle people. My early relationships were with boys from my crowd of friends, so I never had to explain that I had cystic fibrosis.
In my mid-20s, however, I was asked out on dates by men who didn’t know me so well. That meant I had to choose the right moment to mention my illness and if it was an issue, I would walk away.
I could marry only if it felt absolutely right – an extension of my happiness. I’m not ruling out children, either, although it would be a medical decision.
Carrying a child could reduce my lung capacity, maybe permanently. By having a baby, would I reduce my life expectancy and my ability to care for the child? Would it be fair on the child and its father?
Cystic fibrosis is with me day and night but the right treatment may hold it at bay. Techniques have developed rapidly in the past two decades. Medication is more tailored to the individual;
physiotherapy is more sophisticated and intensive.
In the morning I take two medications through a nebuliser, which produces a fine spray that I inhale. I then try to cough up any mucus that has built up overnight. I take pills three times a day, many of them antibiotics, starting at breakfast.
I use three inhalers, two to prevent tightness in the lungs and one to prevent sinusitis.
Additionally, I take Ibuprofen and paracetamol for any pain either side of my spine. When I get home from work or university I am exhausted and generally flake out.
Then it’s more nebulisers before doing some physiotherapy, having dinner, doing some university work and going to bed.
One of the most sophisticated drugs I use is Pulmozyme. When inhaled, it breaks down the mucus before percussive physiotherapy – a once or twice daily beating of the ribcage lasting between 30 minutes and an hour to clear the lungs to dislodge the phlegm.
It can be administered by the patient, a therapist, a trained friend or a parent. As I say, it is tiring. In more serious bouts of illness, I take intravenous antibiotics through a permanent tube in my arm. Antibiotics are constantly swapped so the bugs in your body can’t build up immunities.
I swim and do yoga for an hour as many days a week as my energy levels allow to loosen the mucus on my lungs. I also use a Power-Plate – a vibrating platform – to strengthen joints. The right food is essential, too, to keep up my energy. Protein is important to fight infections. Guilt and anger are always there. Guilt because you worry you are a burden and anger when you’re not getting the treatment you need.
My experiences of the NHS have generally been good, but sometimes horrific. Fortunately, I now attend a good cystic fibrosis clinic at Frimley Park Hospital in Surrey for monthly sessions. Dr Ron Knight, my consultant, is a godsend.
The infection that forced me to abandon my publishing job happened during a summer heatwave. My lung capacity went down to 30 per cent, considered high risk.
I admitted myself to hospital and had to wait six hours for a bed. I was utterly exhausted, my energy drained from me. Then it hit me – this is what people experience when they are very old. When I go I will feel like this. And do you know what? I didn’t give a damn – I would have been content to slip away gently.
But it was not my time. When I awoke with a drip in my arm, I could feel my strength returning. It was clear that I wasn’t going to die.
My fighting spirit was back. I began to get bored in hospital and when you’re well enough to be annoyed, you’re clearly getting better. Stroppy people survive.
That day changed my life. Everyone wonders what it will be like when they die. I gained a sense of peace and lost my fear of death.
Salters-Nuffield Advanced Biology Resources
Activity 2.2 Student SheetSo there I was explaining my illness in front of the Prime Minister and suddenly I got the giggles. I couldn’t stop myself. I said how surreal it was to give such intimate details to a star-studded audience.
With smarter treatment, sufferers are living longer. Some have made it into their 50s, depending on the severity of their condition. But many die in childhood, so the average life expectancy can only tell us so much.
I’m having a big fundraising party on my 31st birthday, the day I overtake my life expectancy. I have no idea how long I will live.
Cystic fibrosis has taught me so much – including humility. I know that when I die, it will be peaceful. In the meantime, I’m as busy as ever, making the most of my time.
Proceeds from Kate’s website (www.Ivebeenkittened.com) go to the Cystic Fibrosis Trust.
Q1 In the article Kate says that she gets very tired. Give a reason(s) why she might experience severe tiredness.
Q2 Explain how you think chest physiotherapy will help with Kate’s condition.
Q3 The drug Pulmozyme (also known as dornase alfa) is referred to in the article. Suggest what type of chemical may occur in this medication and how it might help to break down the mucus.
Q4 Kate was diagnosed at age five. All newborn babies in the UK are now tested for a protein that is elevated in the blood of anyone with cystic fibrosis. Suggest why an early diagnosis will benefit the person found to have CF.
Purpose
To find out how cystic fibrosis affects individuals with the condition by reading some accounts by people affected by CF.
Notes on the procedure
This activity is an alternative to Activity 2.1. It has a more personal approach with less direct links to the topic.
The extract from a young woman’s account of living with CF can be used to get students to see some of the basic symptoms and treatments of cystic fibrosis, as well as getting across some of the
emotional and social issues of living with cystic fibrosis. It could provide the basis of an introductory discussion about cystic fibrosis. In addition, see YouTube clips from the Channel 4 documentary ‘A boy called Alex’ about the 16-year-old musician Alex Stobbs who has CF and an inspiring passion for life.
The introduction to this activity uses median values for life expectancy. This provides the opportunity to discuss different averages that can be calculated and when it is appropriate to use each one. See Maths and Stats Support Sheet 7 – averages, available in the support section online.
Answers
Q1 Kate may get tired for several reasons: the physiotherapy is hard physically, which will be tiring; she is likely to be tired as a side effect of any infection that she has; extra build-up of mucus in her lungs during infection may reduce the oxygen levels in her blood; if the build-up of mucus leads to disruption of her sleep this will also cause tiredness.
Q2 Chest physiotherapy is used to improve respiratory efficiency, promote expansion of the lungs, strengthen respiratory muscles, and break down and eliminate secretions from the lungs. It includes chest percussion and vibration, postural drainage, turning, deep breathing exercises and coughing.
Q3 The name would suggest an enzyme. It breaks down DNA in the mucus making it less viscous and more easily cleared from the lungs.
Salters-Nuffield Advanced Biology Resources
Activity 2.3 Student SheetTHE EFFECT OF SIZE ON UPTAKE BY DIFFUSION
Purpose
To investigate the effect of surface area to volume ratio on uptake by diffusion.
To show why a large surface area in the lungs, combined with a circulation system, is required to meet the body’s demand for oxygen and need to eliminate carbon dioxide.
YOU NEED
● Block of agar jelly
● White tile
● Scalpel or sharp knife
● Paper towel or filter paper
● Beaker (100 cm3)
● Potassium manganate (VII) solution (0.02 M) or hydrochloric acid (0.1 M)
● Ruler
● Rubber or plastic gloves
● Graph paper
Diffusion limits size
Organisms that rely completely on diffusion for the absorption of substances and their movement around the body rarely grow to be more than a few millimetres thick. The surface area to volume ratio limits the size of the organism. You can investigate the effect of increasing size on uptake by diffusion using agar jelly ‘animals’. Read the procedure carefully and correctly follow the instructions.
SAFETY
Wear eye protection, lab coats and disposable gloves.
Avoid skin contact with indicator solutions containing potassium manganate or cresol red. If potassium manganate solution is spilt do not clean it up yourself – tell the teacher/lecturer. Take care when using a knife.
Procedure
1 Cut the agar jelly to give three cubes with linear dimensions of 5 mm, 10 mm and 20 mm. Putting graph paper under the dish of agar jelly is helpful when cutting the blocks. Think how you will cut all the cubes before actually doing it.
2 Place the cubes in the beaker and cover with the potassium manganate solution. If your jelly is green due to universal indicator then use weak acid rather than the potassium manganate (VII) solution. Leave the cubes for three minutes.
3 While you wait, calculate the surface area, volume and surface area to volume ratio (surface area divided by the volume) for each of the cubes. See page 60 of the Student Book for some help.
4 Pour off the solution and blot the surfaces of each cube dry with a paper towel. Cut each of the cubes in half and measure the distance from the edge that has changed colour.
Questions
Q1 What do you notice about the increase in volume of the ‘organism’ when its length doubles?
Q2 What do you notice about the increase in surface area of the ‘organism’ when its length doubles?
Q3 What do you notice about the surface area to volume ratio as the size of the ‘organism’ increases?
Q4 Calculate how long it would take for the solution to diffuse all the way to the centre of each cube.
Q5 As a simplification, let us assume that the increase in volume will be directly related to a similar increase in need for oxygen and nutrients. Explain your experimental findings in terms of diffusion and problems the ‘organism’ would encounter if it got any larger.
Purpose
To investigate the effect of surface area (SA) to volume ratio on uptake by diffusion.
To show why a large surface area in the lungs, combined with a circulation system, is required to meet the body’s demand for oxygen and its need to eliminate carbon dioxide.
SAFETY
Ensure eye protection, lab coats and disposable gloves are worn throughout.
Skin contact with indicator solutions containing potassium manganate(VII) and cresol red should be avoided. See Hazcards 81 and 32 for further details. Alternatively, blocks stained with universal indicator are less hazardous.
Do not allow students to clean up spillages. Use a spillage kit to absorb the solution.
Notes on the procedure
This activity can be completed in conjunction with the questions on pages 60–61 of the Student Book. Students may well have conducted a practical much like this at GCSE, in which case they will find this very straightforward revision. If this is the case, the activity could be extended by using different shapes.
Agar coloured with universal indicator can be used with dilute hydrochloric acid. However, the colour change may be harder to observe. Alkaline blocks containing cresol red indicator would give a clearer colour change than universal indicator.
Table for step 3:
Liner dimension/mm Surface area/mm2 Volume/mm3 SA : volume ratio
5 150 125 1.2
10 600 1000 0.6
20 2400 8000 0.3
This activity provides an opportunity for developing maths skills, calculating the surface area and volumes of regular shapes. The final question on the sheet gives students the chance to calculate volumes of cylindrical prisms in addition to cubes.
Salters-Nuffield Advanced Biology Resources
Activity 2.3 Teacher SheetAnswers
Q1 Each time the length doubles the volume increases by a factor of eight.
Q2 Each time the length doubles the surface area increases by a factor of four.
Q3 As the ‘organism’ grows larger the surface area to volume ratio decreases; each time the length of the ‘organism’ doubles the surface area to volume ratio falls by a factor of two.
Q4 It should take twice as long to reach the centre of the block with sides of 10 mm as it does to reach the centre of the block with sides of 5 mm. It should take four times as long in the block with sides of 20 mm compared with the block with sides of 5 mm. The actual time will depend on experimental conditions (density of agar, concentration of solutions, temperature). The important point for the mathematically challenged is that it takes much longer in the larger cubes.
Q5 The distance the solution has diffused into each of the ‘organisms’ is approximately the same. Diffusion across the surface will occur at the same rate (number of molecules per mm2 per second) regardless of the size of the ‘organism’, because it is not dependent on the internal dimensions of the ‘organism’. If the volume of the ‘organism’ is increasing by a factor of eight, but the surface area is only rising by a factor of four, the surface area available for each unit of volume has decreased. The quantity of substances that will be able to diffuse across the relatively low surface area will not meet the demands of the volume of ‘organism’. The rate of diffusion cannot be increased so this will limit the size of the ‘organism’ unless it can
overcome the problem with specialised gas exchange surfaces or other mechanisms.
Q6 The surface area of a cylinder (a cylindrical prism) is the area of both circular ends plus the surface area of the sides.
Area of circular ends = 2 × πr2
Area of sides: if the sides are rolled out flat this gives a rectangle with area calculated as length × the circumference of the circular end (2πr)
Therefore area of sides = 2πrL
For a cylinder with radius of 2.5 mm and length of 5 mm Surface area = 2 × (π × 2.52) + (2π × 2.5 × 5) = 78.5 mm2 The volume of a cylinder is πr2 × length.
Length of cylinder/
mm Surface area mm
2 Volume/mm3 Surface area :
volume
5 117.8 98.2 1.2 10 196.4 196.4 1.0 20 353.4 392.7 0.9
Purpose
To investigate the effect of surface area to volume ratio on uptake by diffusion.
To show why a large surface area in the lungs, combined with a circulation system, is required to meet the body’s demand for oxygen and need to eliminate carbon dioxide.
SAFETY
Wear eye protection, lab coats and disposable gloves.
Potassium manganate (VII) solid is an oxidising agent and is harmful if swallowed (see Hazcard 81).
Cresol red is an irritant and is harmful if swallowed (see Hazcard 32).
Avoid contact with eyes or skin. In case of contact rinse skin or eyes immediately with a lot of water.
The solution will stain skin and clothes. If students mop up spills with paper towels, the towels may spontaneously combust when they dry out in the bin, especially if other materials are added to the bin. Spills should be dealt with using mineral absorbents.
Requirements per student or
group of students Notes
3 cubes of agar jelly One cube with sides 20 mm long, one with sides 10 mm long and one with sides 5 mm long. If students cut the cubes themselves they will need a block of agar, 20 mm × 30 mm × 20 mm. Alternatively, they can be cut in advance from slabs of agar 20, 10 and 5 mm deep. These are best made in sided dishes or in straight-sided ice cube trays. Agar in Petri dishes poured to the correct depth will provide enough material for at least three sets of blocks. To make agar, stir 1.5 g of agar powder into 100 cm3 water. Heat while stirring to boiling and allow to cool.
If 0.1 M hydrochloric acid is to be used to soak the cubes then the agar needs to be coloured green/yellow with universal indicator. To colour the agar, stir enough universal indicator into the agar to give a good green colour when it is cooling, but not yet set.
Dispose of used blocks by securely wrapping and disposing of as normal waste.
40 cm3 potassium manganate(VII) solution (0.02 M) or 40 cm3 hydrochloric acid (0.1 M) if agar coloured with universal indicator is being used
White tile To cut blocks of agar on.
Sharp knife To cut blocks of agar.
Paper towel or filter paper To blot blocks of agar after soaking. Beaker (100 cm3)
Ruler marked in mm Eye protection
Graph paper If students cut their own blocks.
Salters-Nuffield Advanced Biology Resources
Activity 2.4 Student SheetTHE STRUCTURE OF ALVEOLI
Purpose
To look at the detailed structure of the lungs and identify features that aid rapid diffusion of gases into the bloodstream.
To interpret structures of gas exchange surfaces and describe their properties. To use a microscope and eyepiece graticule to measure lung structures.
SAFETY
Never use a microscope with a daylight mirror in a place where sunlight could strike the mirror. Your retina could be permanently damaged.
Procedure
To remind yourself how to use a microscope, refer to Practical Skills Support Sheet 8 – using a microscope.
Looking at airways and blood vessels
The lungs contain a branching network of tubes that allow ventilation of the alveoli. The action of breathing causes air to move into the lungs along these airways into the alveoli.
1 Examine a prepared section of lung tissue under low power. Remember that you are looking at a thin, 2D section of the 3D lung. Scan across the slide and locate the different types of airway tubes found within the lungs. Your section may include the trachea, a bronchus and
bronchioles.
2 Look carefully at the cells that line the airways using a higher magnification. What do you notice about these cells? The layer of cells is called pseudostratified ciliated columnar epithelium – this should give you clues as to some of the features you are looking for. See page 59 of the Student Book for more help. Draw a simple sketch to show the structure and arrangement of cells in the epithelium.
3 Identify the mucus-secreting goblet cells within the epithelium and label them on your diagram. What is the function of the mucus produced by these cells?
4 Find an airway that has cartilage within the wall. Why do the airway cells contain cartilage?
5 Locate an artery and vein in your section. How can you distinguish between these blood vessels?
Looking at alveoli
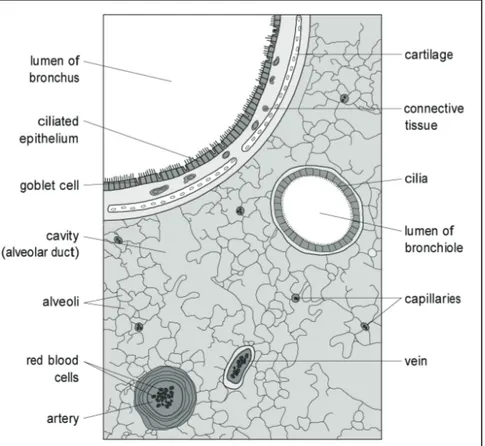
6 Most of the section will be made up of the alveoli and their associated capillaries. It often appears as if large numbers of the alveoli have broken down or are incomplete, leaving gaps on the slide. These gaps are in fact cavities that the bronchioles open into. The alveoli themselves open out from these cavities (see Figure 1). Locate a group of alveoli and identify the associated capillaries. Are all the alveoli the same size?
7 Look carefully at the cells that make up the walls of an alveolus and a capillary. Describe these cells.
Figure 1 Semi-diagrammatic section through a mammalian lung.
How far does an oxygen molecule have to diffuse to get from alveolus to
capillary?
To answer this question you need to work out the average distance an oxygen molecule would have to travel when diffusing from the centre of an alveolus through the wall and into a capillary. Use the Practical Skills Support Sheet 9 – size and scale to find out how to use an eyepiece graticule and stage micrometer to make measurements with a microscope. Decide what measurements you will need to make and plan the appropriate method you will use to make them.
Carry out your experimental work with appropriate safety precautions. Make measurements and record data in an appropriate format using suitable precision.
Once you have completed your measurements you need to analyse the data collected and state a conclusion giving the answer to the question.
Comment on the validity of your conclusion, and discuss the accuracy and precision of your results, considering any error in the procedure used.
Salters-Nuffield Advanced Biology Resources
Activity 2.4 Teacher SheetTHE STRUCTURE OF ALVEOLI
Purpose
To look at the detailed structure of the lungs and identify features that aid diffusion of gases into the bloodstream.
To interpret structures of gas exchange surfaces and describe their properties. To use a microscope and eyepiece graticule to measure lung structures.
SAFETY
Students should be made aware of the hazard of using microscopes where direct sunlight may strike the mirror. Demonstrate how to insert the slide correctly onto the stage. Ramming the slide may produce glass shards.
Notes on the procedure
The use of a light microscope and the use of a graticule are practical techniques students are required to master during the course.
Students use prepared lung slides (cross-sections) and follow the step-by-step instructions on the activity sheet to examine their detailed structure. The final task on the activity sheet is designed with the development of practical skills in mind.
The comments below relate to the numbered steps on the Student Sheet.
Looking at airways and blood vessels
The lungs contain a branching network of tubes that allow ventilation of the alveoli. The action of breathing causes air to move into the lungs along these airways to the alveoli.
1 It is possible to distinguish between the bronchus and bronchioles by size and presence of cartilage. Both have ciliated epithelium, but the smaller bronchioles lack cartilage and mucus glands in the submucosa layer below the epithelium.
2 If the slide does not show the cilia and epithelium effectively the student can be directed to the photograph in the Student Book (page 58).
3 The mucus traps dust and microorganisms, and the beating of cilia moves the mucus to the pharynx.
4 Often difficult to see. The cartilage holds open the airways. As the intercostals and diaphragm muscles increase the volume of the chest cavity the air pressure within the lungs drops; the cartilage prevents the airways collapsing as the air pressure falls.
5 The arteries can be distinguished by their thicker muscular walls and more rounded shape (although this depends on the angle of the section).
Looking at alveoli
6 The alveoli appear to be different sizes, although this may be in part due to where the section cuts through them.
7 Students should identify these cells as squamous epithelium or at least note that they are thin, flattened cells.
capillary?
To answer the question posed, students need to measure the average radius of the alveoli, and the thickness of the barrier between the alveolus and a capillary, using the eyepiece graticule and stage micrometer correctly. Alveoli in human lungs have an average diameter of about 300 μm. For help on using the eyepiece graticule and stage micrometer, refer to the Practical Skills Support Sheet 9 – size and scale. The activity sheet encourages students to consider other practical skills focusing on the quality of their data and the validity of their conclusion. See the Developing Practical Skills
Framework on SNAB Online.
Extension
Salters-Nuffield Advanced Biology Resources
Activity 2.4 Technician SheetTHE STRUCTURE OF ALVEOLI
Purpose
To look at the detailed structure of the lungs and identify features that aid diffusion of gases into the bloodstream.
To interpret structures of gas exchange surfaces and describe their properties.
To use a microscope and eyepiece graticule to measure lung structures.
SAFETY
Do not place daylight illumination microscopes on benches that will catch the direct rays of the Sun.
Requirements per student or
group of students Notes
Microscope Students will need a microscope that has both low- and high-power
lenses. Slide of cross-section of mammalian
lungs with the trachea, bronchus or other large airway visible
An eyepiece graticule and stage micrometer
Purpose
To work out how the surface area of the lungs is greatly increased by the presence of numerous alveoli.
To establish an approximate total surface area for the lungs by calculating volume and surface area of spheres.
Procedure
Use the interactive tutorial that accompanies this activity to compare the surface area of lungs with and without alveoli. Alternatively, complete the calculations yourself using this worksheet and remember to give your answer to the appropriate number of significant figures. See Maths and Stats Support Sheet 4 if you need help with significant figures.
For these calculations we are assuming: a) that the lungs are two perfect spheres
b) that each sphere has a radius of 89 mm, giving a volume of 3 dm3, or 3 ×106 mm3 c) that the diameter of an alveolus is 0.25 mm.
First, find the surface area of these two 3 dm3 spheres by working out:
1 Surface area of one sphere = 4πr2
= __________ mm2
2 Surface area of the two spheres = answer to part (1) × 2 = __________ mm2
Now calculate the volume and surface area of an alveolus by working out:
3 Diameter of one alveolus = __________ mm
4 Radius of one alveolus =
2
diameter
= __________ mm2
5 Volume of one alveolus = 4/ 3πr3
= __________ mm3
6 Surface area of one alveolus = 4πr2
= __________ mm2
To find out the surface area of all the alveoli that can fit into the two ‘sphere’ lungs work out:
7 The number of alveoli that will fit into both of the lungs
= 3
3 m alveolus/m one of volume lungs/mm of volume =
= __________ alveoli
8 Surface area of the alveoli that will fit inside the lungs
= surface area of one alveolus × number of alveoli = __________ × __________
= __________ mm2 Comparing the two:
9 Surface area of the two 3 dm3 spheres = __________ mm2
10 Surface area of all the alveoli in the two spheres = __________ mm2
Salters-Nuffield Advanced Biology Resources
Activity 2.5 Student SheetQuestions
Q1 What assumptions have you made when estimating the surface area of the lungs in this activity?
Q2 The actual surface area of a typical pair of human lungs is 60–80 m², but can be as much as 140 m². This maximum lung surface area is closest to which of the following? Circle the correct answer.
a a large dining table
b the floor of a small room
c a tennis court
d a football pitch.
Q3 Does your estimate give a reasonably accurate value for lung surface area? Explain your answer.
Purpose
To work out how the surface area of the lungs is greatly increased by the presence of numerous alveoli.
To establish an approximate total surface area for the lungs by calculating volume and surface area of spheres.
Notes on the procedure
This interactive activity allows students to compare the surface area of lungs with and without alveoli to reinforce the idea that the presence of alveoli increases the gas exchange surface area. This is a mathematical activity, which some students may find challenging. The interactive tutorial takes students through the activity in steps and automatically completes several of the more difficult
calculations. Alternatively, students can complete the Student Sheet without referring to the interactive tutorial.
Answers to calculations
1 99 538 mm2
2 199 076 mm2
3 0.25 mm
4 0.125 mm
5 0.0082 mm3 or 8.2 × 10–3, to two significant figures because the diameter of the alveolus is given to two significant figures.
6 0.20 mm2
7 = 3 6
10 2 . 8
10 6
= 7.3 × 108 alveoli
8 0.20 × 7.3 × 108 = 1.5 × 108 mm2
9 199 076 mm2 (or 0.199 m2)
10 1.5 × 108 mm
Salters-Nuffield Advanced Biology Resources
Activity 2.5 Teacher SheetAnswers to questions
Q1 Assumptions include:
The entire lung volume is filled with alveoli (there are also airways and blood vessels, etc. present).
he alveoli spheres pack together closely, so there is no wasted space (not possible with spheres).
Alveolar size remains the same (it will vary during ventilation). Each lung is spherical with a volume of 3 dm3.
Q2 c A single tennis court is about 195 m². So this is the nearest approximate area.
Q3 It is about double what it should be but, taking into account the assumptions that have been made, this is not an unreasonable estimate.
Q4 Walls of alveoli one cell thick – thin barrier to diffusion increases rate of diffusion. Walls of alveoli irregular shape – indentations increase surface area, so increase rate of diffusion.
Blood vessels present – blood supply to alveoli increases the diffusion gradient for gas exchange between alveoli and the blood.
Purpose
To describe the structure of an amino acid.
To explain the formation of polypeptides and proteins.
To explain the significance of a protein’s primary structure in determining its 3D structure.
To describe the types of bonds involved in maintaining protein structure.
Procedure
Complete the interactive tutorial accompanying this activity and then complete this worksheet.
Amino acids
Proteins are polymers made up of different combinations of up to 20 different amino acids.
Q1 What is a polymer? ………..
……….………….……
……….………….……
Q2 Annotate this general structure of an amino acid (see Figure 1) with the name and description of the groups that make it up.
Figure 1 General formula of an amino acid.
Salters-Nuffield Advanced Biology Resources
Activity 2.6 Student SheetJoining amino acids
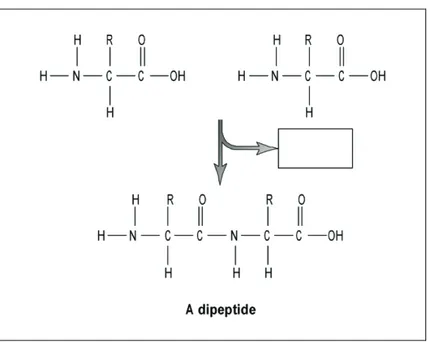
Two amino acids join to form a dipeptide. The bond joining the two amino acids is called a peptide bond.
Q4 Draw a ring around the atoms in Figure 2 that are removed when two amino acids are joined. Write the chemical formula of the molecule that they form in the box.
Figure 2 Formation of a dipeptide.
Q5 The reaction that joins two amino acids is called:
……….………….……..
Q6 Label the peptide bond in Figure 2.
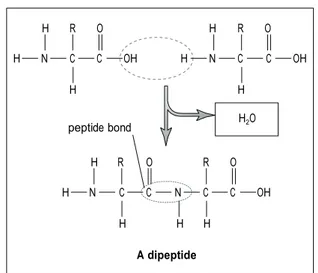
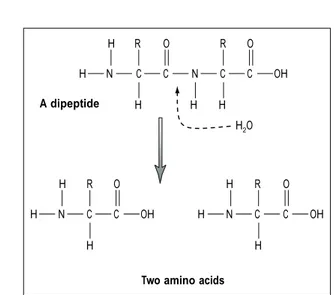
Splitting the peptide bond
A dipeptide bond can be broken down by the addition of water. The breaking of peptide bonds is catalysed by protease enzymes.
……….………….……..
Making a protein
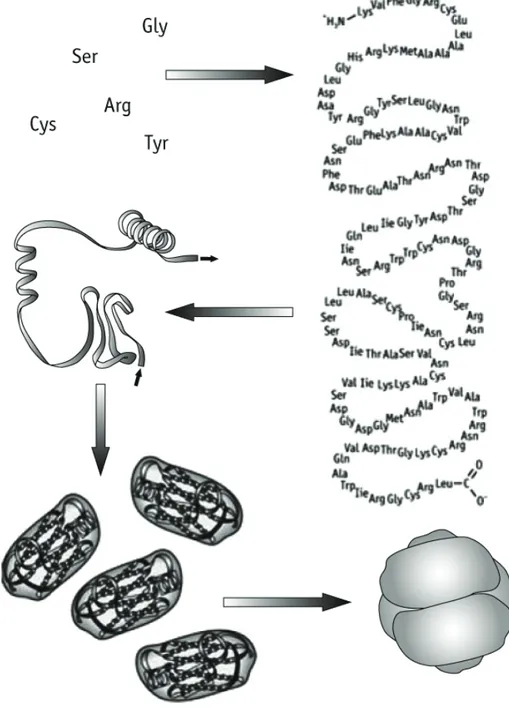
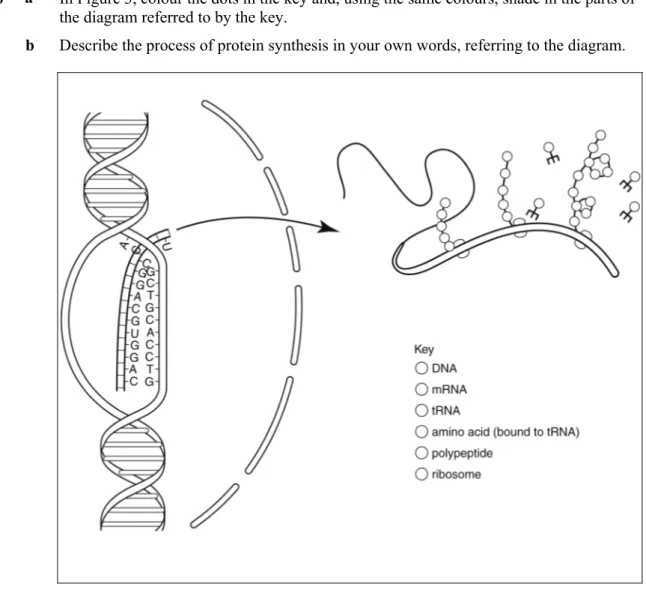
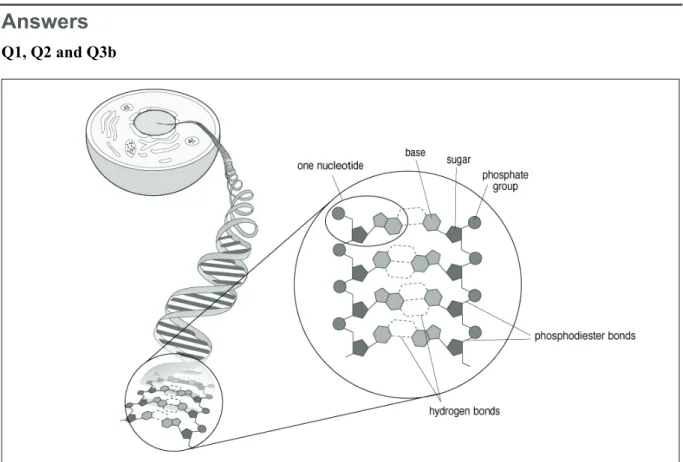
Q9 The flowchart in Figure 4 below shows the sequence of events involved when amino acids join to make polypeptides, which then combine to make a protein. Annotate the diagram with a description of what happens at each stage; include the types of bonds involved at each stage.
Salters-Nuffield Advanced Biology Resources
Activity 2.6 Student SheetQ10 Explain how the sequence of amino acids in a polypeptide chain determines the three-dimensional shape of a functional protein.
……….………….……
……….………….……
……….………….……
……….………….……
……….………….……
……….………….……
……….………….……
Q11 What is the importance of the following in protein folding:
a hydrogen bonds?
……….………….
……….………….
……….………….
……….………….
b water-repelling and water-attracting amino acid side groups?
……….………….
……….………….
……….………….
Purpose
To describe the basic structure of an amino acid.
To explain the formation of polypeptides and proteins.
To explain the significance of a protein’s primary structure in determining its 3D structure.
To describe the types of bonds involved in maintaining protein structure.
Students complete the interactive tutorial or read the Student Book (pages 63–65), and then complete the worksheet.
Answers
Amino acids
Q1 A long molecule made up of small molecules. These may be all the same or a variety of different molecules.
Q2
Figure 1 General formula of an amino acid.
Q3
Figure 2 An amino acid when dissolved in water.
Joining amino acids
Q4
Figure 3 Formation of a dipeptide.
H H O
H+ N+ C C H R O–
H R O H R O
H N C C OH H N C C OH
H H
peptide bond
H R O R O
H N C C N C C OH
H H H
A dipeptide
Salters-Nuffield Advanced Biology Resources
Activity 2.6 Teacher SheetQ5 Condensation.
Q6 See Figure 3.
Splitting the peptide bond
Q7
Figure 4 Splitting of a dipeptide.
Q8 Hydrolysis.
Making a protein
Q9
Figure 5 Flowchart showing the making of a protein from amino acids.
Amino acids ‘link’ by peptide bonds in condensation reactions. A polypeptide (a chain of amino acids) forms. This is the primary structure of the protein.
Several folded units may join together; this is the quaternary structure. The quaternary structure is held together by bonds including those that form between R groups on adjacent chains. Interactions between
the side chains of the amino acids cause the chain to coil and twist to form secondary structures. The secondary structure is held together by hydrogen bonds.
The protein folds tightly to form the tertiary structure. This is held together by bonds between R groups, including disulfide bonds, hydrogen bonds and ionic bonds.
amino acids
α-helix
β-pleated sheet H R O R O
H N C C N C C OH
A dipeptide H H H H2O
H R O H R O
H N C C OH H N C C OH
H H
water. The sequence of amino acids determines the order in which the side groups occur and hence which type of bonds form and which hydrophobic interactions take place.
Q11 a When the chain twists to form an α-helix or a β-pleated sheet, hydrogen bonds form between the carboxylic acid group and the amino group of different amino acids holding the structure in place. When the protein folds to form the tertiary structure, hydrogen bonds form between amino acids and help maintain the 3D shape.
Salters-Nuffield Advanced Biology Resources
Activity 2.7 Student SheetTHE FLUID MOSAIC MODEL
Purpose
To describe the structure and properties of cell membranes including their 3D nature.
To explain how theoretical models of cell membrane structure are interpretations of scientific data and are used to develop scientific explanations.
To appreciate how these theoretical models have developed and changed over time as new data become available.
To appreciate that several theoretical models might co-exist.
To create a 2D or 3D model of a membrane.
Procedure
You are going to be using resources originally developed by the University of Leeds. There are several different sheets that you need to access in order to complete this activity successfully. These can be printed or viewed on screen.
1 Open ‘The fluid mosaic model Resources 1’ PDF.
2 Read page 2, OHT B0.1, which outlines the aims of the lesson.
3 Read the content summary below and then work through tasks 1 and 2.
Page 3 (Sheet B1.1) details the tasks you must complete. The tasks direct you to other sheets in the pack, which present pieces of evidence.
Page 4 (Sheet B1.2) describes when the scientific evidence was obtained.
Pages 5 and 6 (Sheets B1.3 and B2.1) present scientific evidence.
Pages 7 and 8 (B2.2 and B2.3) present the models that were suggested by various researchers.
4 Open ‘The fluid mosaic model Resources 2’ PDF and use pages 1 to 3 (B3.1, B3.2 and B3.3) to complete task 3.
5 Read the Student Book section on ‘Cell membrane structure’, pages 65 to 69.
6 Using any suitable materials available, make your own model of a membrane. Clearly showing the phospholipid bilayer, integral and peripheral proteins and the asymmetric nature of the membrane. You could use modelling clay, straws, wool, foam or any other suitable materials in your model.
B
THEORETICAL MODELS: CELL MEMBRANES
This is a lesson aimed at helping students to develop their understanding of the
role of theoretical models in science, using models of the structure of cell
membranes as an example.
Resources for students
Downloaded from www.nuffieldfoundation.org/aboutscience
OHP B0.1 Aims of the lesson
Sheet B1.1 Structural models of cell membranes
Sheet B1.2 Time line
Sheet B1.3 Lipid layer evidence
Sheet B2.1 Electronmicrograph evidence
Sheet B2.2 Danielli and Davson model
Sheet B2.3 Robertson model
Sheet B3.1 Freeze fracture electronmicrograph evidence
Sheet B3.2 NMR and X-ray diffraction evidence
Sheet B3.3 Singer and Nicholson model
Sheet B3.4 Plasticine model
Teachers’ notes (separate download)
Download from www.nuffieldfoundation.org/aboutscience
by Andy Hind, John Leach, and Jim Ryder: University of Leeds
T
EACHING
A
BOUT
S
CIENCE
OHT B0.1
B
THEORETICAL MODELS: CELL MEMBRANES
Aims of the lesson
In this lesson you are learning about the following.
•
When scientists produce theoretical models, they use
their imagination and creativity to think about data in new
ways. The theoretical models that they produce are
therefore more than careful descriptions of the data.
•
Because the models go beyond the data, more than one
theoretical model can be supported by the available
evidence.
•
In some cases new evidence is gathered which shows
S
TRUCTURAL MODELS OF MEMBRANES
In this lesson you will respond to a number of pieces of evidence which will be
provided in the sequence in which they were discovered.
The time line will help you to see the order of events as they actually happened.
You will need to respond to the questions using all the evidence you have been
provided with at each stage.
Task 1
You should have a copy of sheet B1.3 ‘Lipid layer evidence’.
1.1
From looking at the data in the table, would you agree with the conclusions
of Gorter and Grendel?
1.2
What aspects of the membrane structure is there no evidence for in this data?
Task 2
You should have been given sheet B2.1‘Electronmicrograph evidence’ and a
description of two different models.
2.1
For each of the models, state how the evidence you have supports or
undermines the model.
2.2
Describe what you think led to each model being devised.
Task 3
You should now also have sheets:
B3.1 ‘Freeze fracture electronmicrograph evidence’,
B3.2 ‘NMR and X-ray diffraction evidence’ and
B3.3 ‘Singer and Nicholson’s model’.
The time line will help you see the order these pieces of evidence and models
came in.
3.1
How is each of the models, including Singer and Nicholson’s, supported or
undermined by all the evidence now available?
T
EACHINGA
BOUTS
CIENCES
HEETB1.2
B
T
HEORETICAL MODELS
: C
ELL MEMBRANES
T
IME
L
INE
Gunther Blobel receives a Nobel Prize for his pioneering work on the
mechanisms by which proteins integrate with the membrane (1999)
Singer and Nicholson publish fluid mosaic model (1972)
NMR and X-ray diffraction techniques are developed sufficiently to provide
evidence about the movement of lipids in the membrane
Freeze etching techniques developed giving images of membrane faces
The structure of a protein (haemoglobin) was identified for the first time (1959)
J.D. Robertson proposes his model based on Danielli and Davson’s
Danielli and Davson publish a revised version of their model (1954)
First electronmicroscope images of cell membranes produced
Danielli and Davson propose their original model of the membrane (1935)
Gorter and Grendel publish their paper indicating the possibility of a bilayer
of lipids (1924)
1920
1930
1940
1950
1960
1970
1980
1990
L
IPID
L
AYER
E
VIDENCE
Data from the experiment which laid the foundations for a model of membrane
structure is summarised in the table below. Gorter and Grendel obtained the
membranes of red blood cells. They calculated the area of the red blood cell
membrane and then extracted the lipids that were present. These were dissolved in
petroleum ether and allowed to spread into a layer one molecule thick on a surface of
water and the area was measured.
Animal Total surface area of the red blood cell membrane (A)
Surface area occupied by the lipids extracted (B)
Factor B/A Sq. µ Sq. µ
Dog 31.3 62 2
6.2 12.2 2 Sheep 2.95 6.2 2.1
2.65 5.8 2.2 Rabbit 5.46 9.9 1.8 5.46 8.8 1.6 0.27 0.54 2 0.49 0.96 2
4.9 9.8 2
4.9 9.8 2
Guinea-pig 0.52 1.02 2 0.52 0.97 1.9 Goat 0.33 0.66 2
0.33 0.69 2.1 3.34 6.1 1.8 3.34 6.8 2 0.33 0.63 1.9 Man 0.47 0.92 2
0.47 0.89 1.9
From these results they concluded:
‘It is clear that all our results fit in well with the supposition that the erythrocytes (red blood cells) are covered by a layer of fatty substances that is two molecules thick.’
T
EACHINGA
BOUTS
CIENCES
HEETB2.1
B
T
HEORETICAL MODELS
: C
ELL MEMBRANES
E
LECTRONMICROGRAPH EVIDENCE
During the late 1930s and early 1940s, electronmicroscopy techniques were developed
which provided much more detailed resolution of the structure of a cell. Early micrographs
were obtained by staining a very thin section of tissue with heavy metal salts. These are
absorbed in different amounts by different parts of the cell, giving contrasting degrees of
electron scattering. The parts that take up the most stain appear the darkest on the image.
Electron microscope images of the cell membrane such as this one give us clues as to its
basic structure.
Reprinted from Gomperts, BD (1977) The plasma
membrane: models for structure and function.
D
ANIELLI AND
D
AVSON MODEL
Danielli and Davson proposed their initial model in 1935 and refined it as in the
diagram below in 1954.
The model consists of
A lipid bilayer where two layers of polar lipid molecules are arranged with their
hydrophilic heads outward.
A layer of protein covering the surfaces of the membrane. Note that the protein
layer is embedded in the layer of lipids, holding them in place.
In this model, the lipids are not free to move around.
T
EACHINGA
BOUTS
CIENCES
HEETB2.3
B
T
HEORETICAL MODELS
: C
ELL MEMBRANES
R
OBERTSON
M
ODEL
The model proposed by J.D. Robertson in 1959 is a development of the Danielli
and Davson model with the following exceptions.
The protein layer is formed from a monolayer of polypeptide chains rather
than whole protein molecules. (Polypeptides are the long chain molecules that
proteins are made from.)
The polypeptide layer is on the exterior of the membrane. It is not embedded
in it so the lipids are not held in place.
Robertson proposed that the inner layer could be either polypeptide or
polysaccharide (a long chain sugar molecule).
lipid bilayer
polypeptide layer
F
REEZE FRACTURE ELECTRONMICROGRAPH EVIDENCE
In the freeze fracture technique, the sample is frozen and then cut with a
microtome knife to split the cell. This exposes the membrane’s layered structure
showing the outer and inner layers.
The second picture shows
a similarly treated cell that
has first had 70% of the
protein removed.
There are very few of
the globular structures
that appear in the
membrane of the
untreated cell.
Reprinted from Gomperts, BD (1977) The plasma membrane:
models for structure and function.
chapter 2, page 55, by permission of the publisher, Academic Press
inner
membrane
surface
outer membrane surface
globular particles
This electron micrograph image shows a red blood cell treated in this way.
Note the presence of globular particles on the top surface of the inner
membrane layer which would be within the intact membrane.
100 nm
T
EACHINGA
BOUTS
CIENCES
HEETB3.2
B
T
HEORETICAL MODELS
: C
ELL MEMBRANES
NMR
AND
X-
RAY DIFFRACTION EVIDENCE
NMR stands for Nuclear Magnetic Resonance. By exposing the molecules of the
membrane to a static and an oscillating magnetic field, scientists have been able
to show that the lipids in the membrane, which have a characteristic magnetic
‘spin’, move over distances of up to 50 nm during the duration of the
measurement (5 to 10 seconds).
S
INGER AND
N
ICHOLSON MODEL
Singer and Nicholson’s ‘fluid mosaic model’ (1972) was again a development of Danielli
and Davson’s model but with more significant differences than in the Robertson model.
The key differences are as follows.
The proteins do not form a structural layer holding the lipids in place so the
lipid component of the membrane is not rigid but fluid.
The proteins are not attached to the outside of the lipid layer but embedded
within it, in some cases extending through the thickness of the membrane.
protein molecule
T
EACHINGA
BOUTS
CIENCET
EACHERS’
RESOURCE SHEETB3.4
B
T
HEORETICAL MODELS
: C
ELL MEMBRANES
P
LASTICINE MODEL
In pilot studies, student feedback suggested that a simple model was helpful in
understanding the evidence presented on the freeze fracture sheet.
In freeze fracture preparation, the sample is frozen and then cut with a microtome
knife in a way which exposes the interior of cell organelles.
In the electronmicrographs shown on sheet B3.1, the membrane has been
fractured in a way which exposes the interior of the membrane bilayer.
The simple model described here helps to illustrate this.
Roll out a flattened doughnut of plasticine and superimpose it on
a roughly circular sheet of a contrasting colour.
This surface represents
the outer face of the
inner layer of the
membrane.
This surface represents
the
outer
face
of
the
upper
layer of the membrane
Current membrane research
Studies of cell surface protein receptors in T-cells has shown a link between
tumour necrosis factor (TNF), which attacks cancer cells, and the ageing process. (1999)
Work on molecules that bind with specific receptors on membranes is enabling
Purpose
To describe the structure and properties of cell membranes including their 3D nature.
To explain how theoretical models of cell membrane structure are interpretations of scientific data and are used to develop scientific explanations.
To appreciate how these theoretical models have developed and changed over time as new data becomes available.
To appreciate that several theoretical models might co-exist. To create a 2D or 3D model of a membrane.
Procedure
Students use resources originally developed by the University of Leeds. The SNAB Student Activity Sheet provides an introduction to the Teaching about Science resources, guiding students through the different sheets that are used in this activity. Detailed teacher notes can be found in the Teacher Guidance cell membranes file that accompanies the activity. This activity can be carried out independently by students, or completed as a guided learning activity.