Acceptance and Commitment Therapy as
a Well-Being Focused Mental Health Treatment Approach:
An Investigation of the Association between Mindfulness and Well-Being in Older Adults Jana Marhoferova
Leiden University, The Netherlands j.marhoferova@umail.leidenuniv.nl
Thesis supervisor: Maartje Witlox
Abstract
According to the dual continua model, mental health consists of the two related but independent continua of distress and well-being. Flourishing, the highest well-being level, has been positively associated with better physical and mental functioning (Keyes, 2013; Lamers et al., 2015). Acceptance and Commitment Therapy (ACT) is a treatment approach, which utilizes mindfulness to improve mental health, including well-being. Older adults appear to be a particularly suitable population for mindfulness-based treatment approach, such as ACT. However, little is known about the association between mindfulness, its individual facets and well-being in this population. With this study, we sought to examine the association between dispositional mindfulness and the dual continua model based mental health categories in older adults. Additionally, the unique incremental validity of the individual mindfulness facets in the prediction of well-being was investigated. A cross-sectional online survey of a mixed clinical and community sample of 569 older adults revealed that dispositional mindfulness significantly differentiated purely flourishing older adults from all of the other categories, including older adults who were flourishing with mental distress. Moreover, the facets Describe, Act-Aware, and Non-React significantly predicted well-being, while the facets Observe and Non-Judge did not. We discuss the results in light of the age-related enhanced emotion regulation abilities in older adults and consider the implications for treatment practice and future research. We conclude that older adults might benefit from an adapted ACT focused specifically on increasing well-being.
Acceptance and Commitment Therapy as a Well-Being Focused Mental Health Treatment Approach:
An Investigation of the Association between Mindfulness and Well-Being in Older Adults Improvements in health care in the last century have led to a steady increase in life expectancy (“Mental health of older adults”, 2017). Consequently, the proportion of older adults around the world is predicted to double in the coming 30 years. Prevalence studies on mental health disorders in older adults produce inconsistent results. Some show that mental health disorders tend to decrease with age (Scott et al., 2008). However, many of the prevalence studies limit the age of the sample to a maximum of 75. Recently, a U-shaped prevalence pattern was found using a longitudinal design in a sample without the maximum age specification (Jokela et al., 2013). The prevalence of mental health disorders decreased after age 50, but increased considerably again in population older than 75. Worryingly, the study also revealed that the utilization of mental health treatments tends to decrease in adults older than 55. It is thus important to gain insights into mental health treatment approaches, which could be attractive and suitable for this population.
Importance of Well-Being for Mental Health
represents the highest level of well-being with no distress; Pure Languishing represents the absence of both, well-being and distress; Pure Moderate Well-Being represents intermediate levels of well-being with no distress. Additionally, Flourishing, Languishing, and Moderate Well-Being can each occur while the symptoms of mental distress are also present. In the present study, mental distress is defined as the presence of moderate to severe symptoms of anxiety and/or depression, representing the most common psychological complaints. The current comprehensive definition of well-being combines two important philosophical traditions: hedonic and eudaimonic (Diener et al., 2003; Keyes, 2013; Ryff, 2014). The hedonic tradition reflects the striving for happiness and positive emotions or in other words, emotional well-being. The eudaimonic tradition reflects the striving for excellence in functioning as an individual and as part of society or in other words, psychological and social well-being.
A growing body of evidence shows that Flourishing, as opposed to the other categories, is positively related to a number of desirable outcomes (Huppert, 2009; Keyes, 2010, 2007, 2005 a, b; Lamers et al., 2015; Trompetter et al., 2017). For example, Keyes (2005a, b) found that purely flourishing individuals (i.e. Flourishing without Mental Distress) reported the lowest prevalence of a variety of chronic illnesses and had the best psychosocial functioning in comparison to individuals in the other categories. The evidence also suggests that low levels of well-being without the presence of mental distress could be as risky for health and functioning as the presence of mental distress. In addition, Lamers et al. (2015) used a longitudinal design to demonstrate that high levels of well-being protected from future increase in mental distress.
promotion of well-being should play an increasingly relevant role in mental health research and practice. Moreover, in light of the continuing stigmatization of mental distress in our society (Rössler, 2016), well-being-focused treatment approach might provide a more attractive alternative for older adults than distress-focused treatment approach. This direction can be seen in the so-called third wave of psychological treatments, such as Acceptance and Commitment Therapy (ACT). These treatments incorporate mindfulness, a concept originating in Buddhism, with the traditional behavioral and cognitive techniques (Chiesa & Malinowski, 2011). Importantly, the focus does not lie solely on the treatment of distress, but also on increasing well-being.
Suitability of ACT for Older Adults
Main sources of distress for older adults are loss experiences, declines in physical and cognitive functioning, and role loss (e.g. after retirement). This group might therefore particularly benefit from mindfulness-based treatment, such as ACT, due to its focus on increasing psychological flexibility (Petkus et al., 2010; Witlox et al., 2018). Psychological flexibility refers to “the ability to fully and openly experience the present moment (including the negative or painful aspects) and to behave in a way that is in accordance with personal values” (Witlox et al., 2018, p.2). To promote psychological flexibility ACT makes use of the mindfulness-based processes of acceptance, cognitive defusion, self-as-context, and contact with the present moment, alongside stimulating the identification of and the commitment to personal values. In contrast, the traditional cognitive treatments are aimed at contesting the validity of distressing thoughts (Petkus et al. 2010).
to younger adults (Keyes & Westerhof, 2012). Unexpectedly, but in line with the capitalization model, this finding provides an additional support for mindfulness-based treatments being particularly suitable for this group. Specifically, the high prevalence of flourishing amongst older adults is consistent with research showing that older adults report higher emotional well-being in comparison to younger adults (Prakash et al., 2014; Turk Charles, 2010; Urry & Gross, 2010). The relationship between age and emotional well-being is thought to be partly mediated through enhanced emotional regulation. Evidence indicates that emotion regulation also mediates the association between mindfulness and well-being (Coffey et al., 2010). Therefore, it appears that older adults have a natural bias towards improved emotion regulation, further making this group particularly suitable for mindfulness-based treatments such as ACT. Indeed, older adults responded better to ACT for chronic pain than to Cognitive Behavioral Therapy in comparison to younger adults (Wetherell et al., 2016). Although, to our knowledge there is currently no general review published on the effectiveness of this treatment specifically in older adults
Defining and Measuring Mindfulness
awareness of the present moment are considered as the key-elements of mindfulness. In contrast, other definitions of mindfulness emphasize an interplay of various elements, although the consensus on which elements are central is lacking (Bishop et al., 2004; Hölzel et al., 2011; Leary & Tate, 2007).
Furthermore, the Western conceptualization of mindfulness as a trait-like capacity is criticized by some as deviation from the original Buddhist conceptualization of mindfulness as a practice (Grossman & Van Dam, 2011). Nevertheless, research shows that variability exists in the naturally occurring mindfulness capacity in people with no experience of mindfulness (Brown & Ryan, 2003). For example, dispositional mindfulness in older adults was found to be associated with lower distress and higher vitality (Fiocco & Mallya, 2015; Prakash et al., 2015; Visser et al., 2015). Such research shows that conceptual differences between Buddhist tradition and Western science might not be inherently problematic (Baer, 2018). Instead, the differences can lead to useful insights applicable in the Western culture. At the same time and in line with basic scientific values, it is also important to continuously scrutinize the validity of the instruments used to assess the concept. A large proportion of the research linking mindfulness to distress or well-being in older people employs the MAAS as measurement of mindfulness. However, recent evidence questions the validity of this instrument, suggesting that the MAAS might be measuring lapses of attention rather than mindfulness (Grossman & Van Dam, 2011; Van Dam et al., 2010).
conceptualization allows for detection of unexpected findings, which could otherwise remain obscured. The model emerged as a result of a factor analysis of pooled items from the existing scientifically best-established mindfulness questionnaires and is measured by the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006). The facet Observe assesses the ability to consciously control attention to external and internal stimuli; the facet Describe assesses the ability to verbally label the current experience; the facet Act- Aware assesses the ability to act reflectively instead of reflexively; the facet Non-Judge assesses the ability to forgo the appraisal of inner experience; and the facet Non-React assesses the ability to let the inner experience come and go without reacting (Hölzel et al., 2011). The core mindfulness-based processes from ACT are also reflected in this measure: self as context parallels observing; contact with the present moment parallels acting with awareness; acceptance parallels non-judgment; and cognitive defusion parallels non-reaction.
Individual Mindfulness Facets and Well-Being
Research shows that when mindfulness is applied in order to increase cognitive functioning in older adults, particularly attentional control is improved (Geiger et al., 2016). Yet, studies into the incremental validity of mindfulness facets show that the component ‘observe’ (representing attentional control within mindfulness) does not predict well-being in a community sample, relative to the other facets (Baer et al, 2008). An improved attentional control might thus be less relevant than the other facets in relation to well-being. If this is the case, placing stronger focus on the other aspects of mindfulness could potentially improve the effects of mindfulness-based treatment aimed at the enhancement of well-being.
Continuum-Short Form. However, they only looked at bivariate correlations, rather than the incremental validity of the facets. Bivariate correlations, just as the term suggests, only examine the relation of each individual facet with well-being. In this way, the unique contribution of each facet, relative to the rest of the facets, in the prediction of well-being remains hidden. Examining the incremental validity of mindfulness facets in predicting well-being, Cash & Whittingham (2010) found that none of the mindfulness facets significantly predicted well-being, measured by Personal Well-Being Index (PWI). In contrast, Baer et al. (2008) found that Describe, Act Aware, Non-Judge, and Non-React were all predictors of psychological well-being, measured by Ryff’s psychological well-being scale (PWB), while Observe was not. Although the different measures of well-being might account for the discrepancy (Cash & Whittingham, 2010). PWI measures satisfaction in more materialistic domains, such as standards of living or health. On the other hand, PWB assesses more abstract domains, such as self-acceptance or positive social relationships. The studies mentioned above employed student, community, or clinical samples. None has focused specifically on older adults, which is surprising given the notion that mindfulness-based treatment might be particularly suitable for older adults (Petkus et al., 2010; Prakash et al., 2014). Moreover, high levels of well-being have been shown to serve as a resource for healthier aging in terms of survival rates, physiological, and cognitive outcomes (Allerhand et al., 2014). It might thus be useful to examine the association of mindfulness and well-being in older adults.
The Present Study
evidence-based adaptation of ACT into a novel treatment approach focused specifically on the enhancement of well-being. A cross-sectional online survey of a mixed clinical and community sample of older adults was employed to examine if dispositional mindfulness, conceptualized as a five-facet construct, discriminated the dual continua model based mental health categories in older adults. We expected that purely flourishing older adults would significantly differ in their dispositional mindfulness score from older adults who were languishing with mental distress. Additionally, we investigated which individual facets of mindfulness were associated to flourishing in older adults. We expected that all individual mindfulness facets, apart from the facet Observe, would positively predict well-being in older adults.
Methods Participant Characteristics and Procedure
Patient Health Questionnaire (PHQ-9); 5. having received psychological or psychopharmacological treatment (with the exception of stable use of benzodiazepines or SSRIs) within the last three months; 6. severe role impairment, indicated by a score equal or higher than 8 on two of the three sub-scales of the Sheeran Disability Scale (SDS). The data used in the present study was collected using online questionnaires. For further details on the procedure, see Witlox et al. (2018).
Community sample data was obtained from a thesis study of a Leiden University student, investigating the moderating role of mindfulness on the relationship between stressful life events and mental health in older adults. During September and October 2018, various organizations in Netherlands, where older adults are members, were asked to distribute an online survey amongst their members. Adults aged 55+, with access to internet were recruited through an invitation e-mail from the participating organizations. The data used in the present study was collected using online questionnaires.
Measures
Well-being. Well-being was measured with the Dutch version of The Mental Health
Distress. Distress was measured with the Dutch version of the General Anxiety Disorder Questionnaire (GAD-7; Spitzer et al., 2006) and the Dutch version of the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001).
Anxiety was measured with GAD-7: a 7-item self-report questionnaire assessing the severity of anxiety symptoms. Each item is rated on a 4-point scale ranging from 0 (=not at all) to 3 (= nearly every day), based on the frequency of symptoms experienced in the past two weeks (e.g. “Over the last 2 weeks, how often have you been bothered by: feeling nervous, anxious, or on edge?”). The total score ranges from 0 to 21 and scores of 5, 10, and 15 represent the cut-off points for mild, moderate, and severe anxiety symptoms, respectively. Psychometric properties of GAD-7 are adequate and the reliability and validity of a web-based Dutch version have been established (Donker et al., 2011; Kroenke et al., 2010).
Depression was measured with PHQ-9: a 9-item self-report questionnaire assessing the severity of depressive symptoms. Each item is rated on a 4-point scale ranging from 0 (=not at all) to 3 (= nearly every day), based on the frequency of symptoms experienced in the past two weeks (e.g. “Over the last 2 weeks, how often have you been bothered by: depressed or hopeless?”). The total score ranges from 0 to 27 and scores of 5, 10, 15, 20 represent cut-off points for mild, moderate, moderately severe, and severe depressive symptoms, respectively. Psychometric properties of PHQ-9 are adequate and the reliability and validity were established (Kroenke et al., 2010; Löwe et al., 2004).
Act-Aware assessed by 5 items, Non-Judge assessed by 5 items, and Non-React assessed by 5 items. The five factor structure was confirmed in Dutch population (Bohlmeijer et al., 2011). Each item is rated on a 5-point scale ranging from 1 (= never or very rarely true) to 5 (= very often or always true), based on the general degree of the agreement with the statements. The total score ranges from 24 to 120. Psychometric properties of FFMQ-SF are adequate and the reliability and validity were established with a sample of Dutch adults (Bohlmeijer et al., 2011).
Demographics. Demographic variables were assessed by two questions asking for the participants’ age and gender.
Analysis
4 points) or mild (5 to 9 points) to be considered as absence of distress. Symptoms of anxiety, depression, or both had to be moderate (10 to 14 points) or severe (15+ points) to be considered as presence of distress. On this basis the following mental health categories were created:
Pure Flourishing = one of the three hedonic well-being symptoms (items 1-3) felt
“everyday” or “almost everyday” + six of the eleven positive functioning symptoms (items 4-14) felt “everyday” or “almost everyday” in the past month + GAD7 and PHQ9 score lower than 10.
Pure Languishing = one of the three hedonic well-being symptoms (items 1-3) felt
“never” of “once or twice” + six of the eleven positive functioning symptoms (items 4-14) felt “never” or “once or twice” in the past month + GAD7 and PHQ9 score lower than 10.
Pure Moderate Well-Being = neither Pure Languishing nor Pure Flourishing + GAD7
and PHQ9 score lower than 10.
Flourishing with Mental Distress = Pure Flourishing with GAD7 and/or PHQ9 score
equal to or higher than 10.
Languishing with Mental Distress = Pure Languishing with GAD7 and/or PHQ9 score
equal to or higher than 10.
Moderate Well-Being with Mental Distress = Pure Moderate Well-Being with GAD7
and/or PHQ9 score equal to or higher than 10.
Languishing with Mental Distress are ordered as the first and the last category, respectively. The categories in between were considered as unordered, as it is not clear if, for example Pure Languishing ranks above or below Moderate Well-Being with Mental Distress. MLR is a technique that can be applied for analysis of three or more categorical dependent variables (Petrucci, 2009). It allows for differentiation between mutually exclusive groups and estimates the probability of belonging to a specific group on the basis of one or more categorical or continuous predictors. An advantage is that by using a reference category, MLR computes the estimates for each category of the dependent variable. The category “Pure Flourishing” was used as reference category. Moreover, MLR performs well for non-normally distributed data. The significance level was one-tailed and set at p < .05. The likelihood ratio test (χ2), and Hosmer-Lemeshow statistic were used to evaluate the
improvement of the MLR model over the intercept-only model (Petrucci, 2009). Additionally, Nagelkerke’s pseudo R2 was used to indicate the effect size.
evaluate the improvement of the LR model over the intercept-only model (Peng et al., 2002). Additionally, Nagelkerke’s pseudo R2 was used to indicate the effect size.
Power analysis was performed in R, with one-tailed effect size of 0.2 (Bohlmeijer et al. 2011), alpha set at 0.01 and power of 80%. This analysis indicated that a sample size of just over 500 participants is needed for the present study. The sample for this study consists of 569 participants, which enabled us to conduct the multiple test analysis with reasonable confidence.
Results Descriptives and Preliminary Analyzes
The sample included 569 participants of from which 56.2% were females. Age ranged from 55 to 98 years with a mean of 67.2. There were no missing data. and no outliers (i.e. an individual score that differed by more than 3 standard deviations from the mean). The MHC-SF displayed an excellent internal consistency for the present sample, with Cronbach’s Alpha of .91. The GAD-7 and PHQ-9 displayed a good internal consistency for the present sample, with Cronbach’s Alpha of .89 and .83, respectively. The FFMQ-SF displayed an acceptable internal consistency in the present sample, with Cronbach’s Alpha of .79.
Mindfulness and the Dual Continua Model of Mental Health
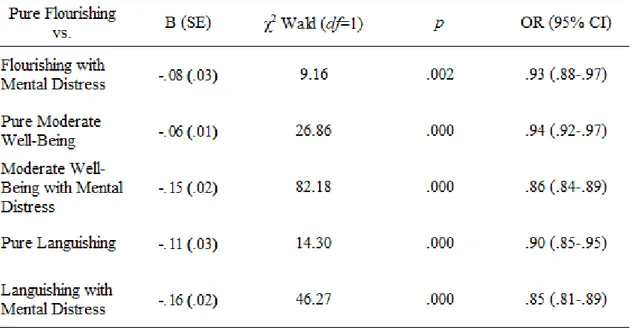
Multinomial logistic regression revealed that adding mindfulness to an intercept-only model significantly improved the model fit, χ2 (5, N = 569) = 138.25, Nagelkerke R2 = .23, p
< .001. The Hosmer and Lemeshow Test was not significant for the model including the dispositional mindfulness as predictor, further indicating a good fit. The parameter estimates,
Table 2. Multinomial regression parameter estimates contrasting the Pure Flourishing category with the other categories as a function of mindfulness
with Pure Flourishing as reference group, are shown in Table 2. Mindfulness significantly differentiated all of the mental health categories, when compared to the Pure Flourishing category. Purely flourishing older adults were significantly more likely to have higher dispositional mindfulness scores than older adults in all of the other mental health categories. The Differential Relationship of Individual Mindfulness Facets with Well-Being
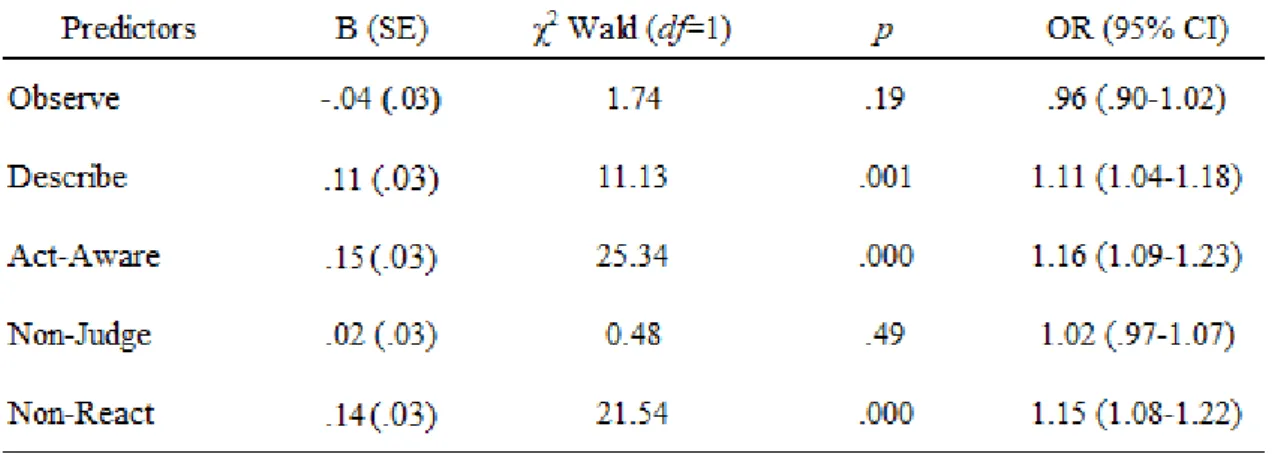
The tolerance and variance inflation factor values indicated that there was no multicollinearity between the predictors. Hierarchical logistic regression revealed that adding the five mindfulness facets to an intercept-only model significantly improved the model fit, χ2
(5, N = 569) = 101.65, Nagelkerke R2 = .22, p < .001. The Hosmer and Lemeshow Test was
not significant for the model including the mindfulness facets, further indicating a good fit for the data. The parameter estimates are shown in Table 3. The facets Observe, and Non-Judge
were not significant predictors of well-being, relative to the other mindfulness facets. The facets Describe, Act-Aware, and Non-React positively predicted well-being. Flourishing older adults were significantly more likely to have higher scores on the facets Describe. Act-Aware, and Non-React than older adults who were less than flourishing.
Discussion
The present study examined whether dispositional mindfulness, conceptualized as a multifaceted construct, discriminated the dual continua model based mental health categories in a mixed community and clinical sample of older adults. We hypothesized that purely flourishing older adults would significantly differ in their mindfulness score from older adults who were languishing with mental distress. As predicted, dispositional mindfulness significantly differentiated purely flourishing older adults from older adults who were languishing with mental distress. Dispositional mindfulness also significantly differentiated purely flourishing older adults from all of the other categories, including older adults who were flourishing with mental distress. Taken together with the evidence that Flourishing is associated with a number of desirable outcomes (Keyes, 2013; Lamers et al., 2015), our finding indicates that older adults might benefit from mindfulness-based treatment focused specifically on promotion of well-being. Moreover, our finding is consistent with previous studies showing an association of mindfulness with well-being or distress in older adults (Fiocco & Mallya, 2015; Prakash et al., 2015; Visser et al., 2015).
partly corroborates the finding from previous research (Baer et al., 2008). In line with Baer et al., the facets Describe, Act-Aware and Non-React were significant predictors of well-being, while the facet Observe was not. In contrast to Baer et al., the facet Non-Judge was not a predictor of well-being, when all the other facets were taken into account. It is plausible, that the facets Observe and Non-Judge might be essential for the development and implementation of the other facets and their association with well-being might be indirect.
On the other hand, the discrepancy in the findings of the present study and those of Baer et al. (2008) might have arisen due to the differences in the assessment of well-being. The present study measured being as consisting of three sub-scales: emotional well-being and psychological functioning, which includes psychological and social well-well-being. To reflect the importance of the various domains to the overall well-being, we also assessed the being categorically. In contrast, Baer et al. (2008) assessed only psychological well-being and as a continuous variable. It is possible that different facets have incremental validity in the prediction of the different well-being sub-scales or that some information was lost due to the different assessment approaches.
suggested to represent a form of an emotion regulation strategy, namely reappraisal (Hölzel et al., 2011). Consequently, the finding that Non-Judge does not hierarchically predict well-being in older adults could be consistent with SAVI. Older adults with different well-well-being levels might not differ in their ability to reappraise.
Hölzel et al. (2011, p. 539) characterize the facet Non-React as an emotion regulation
strategy which facilitates “exposing oneself to whatever is present in the field of awareness; letting oneself be affected by it; refraining from internal reactivity”. The ability to let the inner experience come and go without reacting might thus also contribute to decreases in experiential avoidance. In summary, an increased ability to Describe, Act-Aware, and Non-React, could plausibly differentiate older adults who are flourishing from those who are less than flourishing via the impact on experiential avoidance. In this line, the result of the present study would be in accordance with Hayes (2006), who proposed that experiential avoidance could be detrimental to well-being.
In addition, when interpreting the results of the present study, some methodological limitations should be kept in mind. First, the present study was cross-sectional, and of correlational nature. Causality thus cannot be inferred. An alternative interpretation, that high levels of well-being in older adults lead to an increased ability to Describe, Act-Aware and Non-React, is possible. Yet, our interpretation is grounded in previous research and theoretical accounts demonstrating that increases in mindfulness levels lead to increases in well-being (for example: Bohlmeijer et al., 2015; Brown & Ryan, 2003). Second, only self-report measures were used for data collection, potentially introducing biases. For example, participants might be answering in terms of their desired rather than actual behaviors or the semantic interpretation of the items might vary across participants (Van Dam, 2011). Moreover, the questions about the validity of the FFMQ-SF, as well as the debate over the definition of mindfulness remain (for example: Coffey et al., 2010; Grossman & Van Dam, 2011). Therefore, we cannot be certain to what extent the FFMQ-SF actually represents dispositional mindfulness. Development of objective measures which mitigate these issues would improve future studies. Third, we did not assess the previous meditation experience of the sample. Quality of observing, which can change with meditation experience, has been found to affect the association between the facet Observe and psychological outcomes, including well-being (Baer et al., 2008, 2018; Desrosiers et al., 2014). Assessing previous mindfulness experience in future research should provide a more accurate picture of mindfulness.
References
Allerhand, M., Gale, C. R. & Deary, I. J. (2014). The dynamic relationship between cognitive
function and positive well-being in older people: A prospective study using the
English longitudinal study of aging. Psychology and Aging, 29(2), 306-318. doi:
10.1037/a0036551
Baer, R. A. (2018). Assessment of mindfulness by self-report. Current Opinion in
Psychology, 28, 42-48. doi: 10.1016/j.copsyc.2018.10.015
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S.,...Williams, J.
M. G. (2008). Construct validity of the Five Facet Mindfulness Questionnaire in
meditating and nonmeditating samples. Assessment, 15(3), 329-342. doi:
10.1177/1073191107313003
Baer, R. A., Smith, G., T., Hopkins, J., Krietemeyer, J. & Toney, L. (2006). Using self-report
assessment methods to explore facets of mindfulness. Assessment, 13(1), 27-45. doi:
10.1177/1073191105283504
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L. Anderson, N. D., Carmody, J.,...Devins, G.
(2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science
and Practice, 11(3), 230-241. doi:10.1093/clipsy/bph077
Bland J. M. & Altman D. G. (1995). Multiple significance tests: the Bonferroni method.
Biomedical Journal, 310, 170.
Bohlmeijer, E. T., Lamers, S. M. A., & Fledderus, M. (2015). Flourishing in people with
depressive symptomatology increases with Acceptance and Commitment Therapy.
Post-hoc analyzes of a randomized controlled trial. Behavior Research and Therapy,
Bohlmeijer, E. T., ten Klooster, P. M., Fledderus, M., Veehof, M. & Baer, R. (2011).
Psychometric properties of The Five Facet Mindfulness Questionnaire in depressed
adults and development of a short form. Assessment, 18(3), 308-320. doi:
10.1177/1073191111408231
Brown, K. W. & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role
in psychological well-being. Journal of Personality and Social Psychology, 84(4),
822-848. doi: 10.1037/0022-3514.84.4.822
Cash, M. & Whittingham, K. (2010). What facets of mindfulness contribute to
psychological well-being and depressive, anxious, and stress-related
symptomatology? Mindfulness, 1, 177-182. doi: 10.1007/s12671-010-0023-4
Chiesa, A. & Malinowski, P. (2011). Mindfulness-based approaches: Are they all the
same? Journal of Clinical Psychology, 67(4), 404-424. doi: 10.1002/j clp.20776
Coffey, K. A., Hartman, M. & Frederickson, B. L. (2010). Deconstructing mindfulness and
constructing mental health: Understanding mindfulness and its mechanisms of action.
Mindfulness, 1, 235-253. doi: 10.1007/s12671-010-0033-2
Desrosiers, A., Klemanski, D. H. & Nolen-Hoeksema, S. (2013). Mapping mindfulness facets
onto dimensions of anxiety and depression. Behavior Therapy, 44, 373-384.
Desrosiers, A., Vine, V., Curtiss, J. & Klemanski, D. H. (2014). Observing nonreactively: A
conditional process model linking mindfulness facets, cognitive emotion regulation
strategies, and depression and anxiety symptoms. Journal of Affective Disorders, 165,
31-37. doi: 10.1016/j.jad.2014.04.024
Diener, E., Napa Scollon, C. & Lucas, R. E. (2003). The evolving concept of subjective
well-being: the multifaceted nature of happiness. Advances in Cell Aging and Gerontology,
Donker T., Van Straten A., Marks I. & Cuijpers P. (2011). Quick and easy self-rating of
generalized anxiety disorder: validity of the Dutch web-based GAD-7, GAD-2 and
GAD-SI. Psychiatry Research, 188, 58–64. doi:10.1016/j.psychres.2011.01.016
Fiocco, A. J., & Mallya, S. (2015). The importance of cultivating mindfulness for cognitive
and emotional well-being in late life. Journal of Evidence-Based Complementary &
Alternative Medicine, 20(1), 35–40. doi: 10.1177/2156587214553940
Geiger, P. J., Boggero, I. A., Brake, C. A., Caldera, C. A., Combs, H. L., Peters, J. R. & Baer,
R. A. (2016). Mindfulness-based interventions for older adults: A review of the
effects on physical and emotional well-being. Mindfulness, 7(2), 296-307. doi:
10.1007/s12671-015-0444-1
Grossman, P. & Van Dam, N. T. (2011). Mindfulness, by any other name…: trials and
tribulations of sati in western psychology and science. Contemporary Buddhism,
12(1), 219-239. doi: 10.1080/14639947.2011.564841
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A. & Lillis, J. (2006). Acceptance and
Commitment Therapy: Model, processes and outcomes. Behavior Research and
Therapy, 44, 1–25. doi: 10.1016/j.brat.2005.06.006
Hayes, S. C., Strosahl, K., Wilson, K. G., Bissett, R. T., Pistorello, J., Toarmino,
D.,...McCurry, S. M. (2004). Measuring experiential avoidance: A preliminary test of
a working model. The Psychological Record, 54, 553-578.
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R. & Ott, U. (2011).
How does mindfulness meditation work? Proposing mechanisms of action from a
conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537–
Huppert, F. A. (2009). Psychological well-being: Evidence regarding its causes and
consequences. Applied Psychology and Well-being, 1(2), 137-164. doi:
10.1111/j.1758-0854.2009.01008.x
Huppert, F. A. & Whittington, J. E. (2003). Evidence for the independence of positive and
negative well-being: Implications for quality of life assessment. British Journal of
Health Psychology, 8, 107-122.
Jokela, M., Batty, G. D. & Kivimäki. M. (2013). Aging and the prevalence and treatment of
mental health problems. Psychological Medicine, 43, 2037-2045. doi:
10.1017/S0033291712003042
Kazdin, A. E. (2017). Research Design in Clinical Psychology Fifth Edition. Boston:
Pearson.
Keyes, C. L. M. (2005a). Chronic physical conditions and aging: Is mental health a potential
protective factor? Aging International, 30, 88–104.
Keyes, C. L. M. (2005b). Mental illness and/or mental health? Investigating axioms of the
complete state model of health. Journal of Consulting and Clinical Psychology, 73(3),
539-548. doi: 10.1037/0022-006X.73.3.539
Keyes, C. L. M. (2007). Promoting and protecting mental health as flourishing: A
complementary strategy for improving national mental health. American
Psychologist, 62(2), 95-108. doi: 10.1037/0003-066X.62.2.95
Keyes, C. L. M. (2013). Promotion and protection of positive mental health: Towards
complete mental health in human development. In I. Boniwell, S. A. David & A. C.
Ayers (Eds.), Oxford Handbook of Happiness. Retrieved from
Keyes, C. L. M., Dhingra, S. S., & Simoes, E. J. (2010). Change in level of positive mental
health as a predictor of future risk of mental illness. American Journal of Public
Health, 100, 2366–2371
Keyes, C. L. M. & Westerhof. G. J. (2012). Chronological and subjective age differences in
flourishing mental health and major depressive episode. Aging & Mental Health,
16(1), 67-74. doi: 10.1080/13607863.2011.596811
Kroenke K., Spitzer R. L. & Williams J. B. (2001). The PHQ-9: validity of a brief depression
severity measure. Journal of General Internal Medicine, 16(9), 606–613.
Kroenke K., Spitzer R. L., Williams J. B. & Lowe B. (2010). The patient health questionnaire
somatic, anxiety, and depressive symptom scales: a systematic review. General
Hospital Psychiatry, 32(4), 345–359. doi:10.1016/j.genhosppsych.2010.03.006
Lamers, S. M. A., Westerhof, G. J., Glas, C. A. W. & Bohlmeijer, E. T. (2015). The
bidirectional relation between positive mental health and psychopathology in a
longitudinal representative panel study. The Journal of Positive Psychology, 10(6),
553-560. doi: 10.1080/17439760.2015.1015156
Lamers S. M., Westerhof G. J., Bohlmeijer E. T., ten Klooster P. M. & Keyes C. L. (2011).
Evaluating the psychometric properties of the mental health continuum short form
(MHC-SF). Journal of Clinical Psychology, 67(1), 99–110.
Leary, M. R. & Tate, B. (2007). The multi-faceted nature of mindfulness. Psychological
Inquiry, 18(4), 251-255. doi: 10.1080/10478400701598355
Löwe B., Unutzer J., Callahan C. M., Perkins A. J. & Kroenke K. (2004). Monitoring
depression treatment outcomes with the patient health Questionnaire-9. Medical
Mental health of older adults. (2017, December 12). Retrieved from
http://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults
Peng, C. Y., Lee, K. L., & Ingersoll, G.M. (2002). An introduction to logistic regression
analysis and reporting. Journal of Educational Research, 96(1), 3-14.
Petkus A. J., Wetherell J. L.. (2013). Acceptance and commitment therapy with older adults:
rationale and considerations. Cognitive and Behavioral Practice, 20(1), 47–56.
Petrucci, C. J. (2009). A primer for social worker researchers on how to conduct a
multinomial logistic regression. Journal of Social Service Research, 35(2), 193-205.
doi: 10.1080/01488370802678983
Prakash, R. S., De Leon, A. A., Patterson, B., Schirda, B. L., & Janssen, A. (2014).
Mindfulness and the aging brain: a proposed paradigm shift. Frontiers in Aging
Neuroscience, 6. doi: 10.3389/fnagi.2014.00120
Prakash, R. S., Hussain, M. A., & Schirda, B. (2015). The role of emotion regulation and
cognitive control in the association between mindfulness disposition and stress.
Psychology and Aging, 30(1), 160–171. doi: 10.1037/a0038544
Rosch, E. (2007). More than mindfulness: When you have a tiger by the tail, let it eat you.
Psychological Inquiry, 18(4), 258-264. doi: 10.1080/10478400701598371
Rössler, W. (2016). The stigma of mental disorders. Science & Society, 17(9), 1250-1253.
doi: 10.15252/embr.201643041
Ryff, C. D. (2014). Psychological well-being revisited: Advances in the science and practice
of eudaimonia. Psychotherapy and Psychosomatics, 83, 10-28. doi:
10.1159/000353263
Scott K. M., Von Korff M., Alonso J., Angermeyer M., Bromet E. J., Bruffaerts R.,...
disorders with and without physical co-morbidity. Psychological Medicine, 38, 1659–
69.
Spinhoven, P., Drost, J., de Rooij, M., van Hemert, A. M., & Penninx, B. W. (2014). A
longitudinal study of experiential avoidance in emotional disorders. Behavior
Therapy, 45, 840-850. doi:
Spitzer R. L., Kroenke K., Williams J. B. & Lowe B. (2006). A brief measure for assessing
generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 166(10),
1092–1097. doi: 10.1001/archinte.166.10.1092
Trompetter, H. R., de Kleine, E. & Bohlmeijer, E. T. (2017). Why does positive mental
health buffer against psychopathology? An exploratory study on self-compassion as a
resilience mechanism and adaptive emotion regulation strategy. Cognitive Therapy
and Research, 41, 459-468. doi: 10.1007/s10608-016-9774-0
Turk Charles, S. (2010). Strength and vulnerability integration (SAVI): A model of
emotional well-being across adulthood. Psychological Bulletin, 136(4), 1068-1091.
doi:10.1037/a0021232
Urry, H. L. & Gross, J. J. (2010). Emotion regulation in older age. Current Directions in
Psychological Science, 19(6), 352-357. doi: 10.1177/0963721410388395
Van Dam, N. T., Earleywine, M,. & Borders, A. (2010). Measuring mindfulness? An item
response theory analysis of the mindful attention awareness scale. Personality and
Individual Differences 49(7), 805–810. doi:10.1016/j.paid.2010.07.020
Visser, P. L., Hirsch, J. K., Brown, K. W., Ryan, R., & Moynihan, J. A. (2015). Components
of sleep quality as mediators of the relation between mindfulness and subjective
vitality among older adults. Mindfulness, 6(4), 723–731. doi:
Wetherell, J. L., Petkus, A., J., Alonso-Fernandez, M., Bower, E. S., Steriner, A. R. W.,
Afari, N. (2016). Age moderates response to Acceptance and Commitment
Therapy vs. Cognitive Behavioral Therapy for chronic pain. International Journal of
Geriatric Psychology, 31, 302-308. doi: 10.1002/gps.4330
Witlox, M., Kraaij, V., Garnefski, N., de Waal, M. W. M., Smit, F., Hoencamp, E.,…
Spinhoven, P. (2018). An Internet-based Acceptance and Commitment Therapy
intervention for older adults with anxiety complaints: study protocol for a cluster