A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
110 | P a g e
“EFFECTIVENESS OF TOOTH BRUSHING SKILLS INTERVENTION
AMONG CHILDREN WITH INTELLECTUAL DISABILITY
INVOLVING PARENTS”
Sanjay Sevak1, Dr. Rakesh Ghildiyal2, Dr. Prabha Dasila3
1Ph D Nursing Scholar, MGM University of Health science, Navi Mumbai, 2 Professor and H.O.D. Department of Psychiatry, M. G. M. Medical College, Kamothe,
Navi - Mumbai.
3Professor and Director, M. G. M. Institute University Department of Nursing, Kamothe,
Navi - Mumbai.
ABSTRACT
Intellectual disability is a term used for children with deficits in adaptive behavior, limitations in mental functioning and in poor skills in self-care, decision making,
communication and academic performance. Aim: To assess effectiveness of tooth brushing
skills intervention among children with intellectual disability. Method: A Quasi experimental
non randomized control group design was used to assess effectiveness of tooth brushing skills
intervention among children with intellectual disability residing at Navi Mumbai and Thane
district. A total number of 20 children with intellectual disability were selected by
non-probability convenient sampling technique. The reliability of the tool was 0.996 determined
by Cronbach’s Alpha method. The tooth brushing skills intervention conducted with the help
of model, charts and demonstration Pre intervention assessment of children was done and
posttest was conducted after 12 weeks. The mean scores obtained by the samples in the
pre-test were 37.5 and in the post-pre-test it increased to 46. The calculated p-value is <0.05, which
indicates that there is a significant improvement in the tooth brushing practices compared to
baseline tooth brushing habits and this improvement is statistically significant, Hence we can
reject null hypothesis, therefore It can be concluded that tooth brushing interventions were
effective in improving tooth brushing practices among children with intellectual disability.
Keywords :, Effectiveness, Tooth brushing skills intervention, Children with intellectual
disability, Parents.
International Research Journal of Human Resources and Social Sciences Vol. 4, Issue 5, May 2017 Impact Factor- 5.414
ISSN(O): (2349-4085) ISSN(P): (2394-4218)
© Associated Asia Research Foundation (AARF)
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
111 | P a g e 1. INTRODUCTION
Intellectual disability affects about 2–3% of the general population. Around 75-90% of the children affected by mild intellectual disabled.[1] According to National Sample Survey Organization report estimated 18.49 million disabled persons in the India, out of that 0.44 million individuals are mentally disabled.[2] Previously the term mental retardation was used in Diagnostic and Statistical Manual (DSM)-IV. Moreover, a federal statue in the United States (Public Law 111-256, Rosa’s Law) replaces the term “mental retardation” with intellectual disability.[3] Intellectual disability are lifelong conditions and it is a highly prevalent in developing country like India. According to American Association of Mental Deficiency (1983) Mental retardation refers to significantly sub-average general intellectual functioning resulting in or associated with concurrent impairments in adaptive behavior and manifested during the developmental period.[4]
A study by Nagarkar A. stated intellectual disability affects the communication, academic and activities of daily living, which make the child more dependent on the caregiver as compared with a normal child.[5] When child once he/she has delayed in milestones or been diagnosed with intellectual disability many parents became panic because of sense of helplessness and lack of understanding about disability. A study conducted by Venkatesan & Das (1994) reported that the type of burden reported by care takers and family members may including from difficulties in management of behaviour problems, self-care deficit, disruption of their daily routine, social and economical burden.[6] Hornby G, Singh NN (1984) conducted a study on Behavioural group training with parents of mentally retarded children. A pre-test and posttest experimental design was used on several parents of moderately mentally retarded children. Result shows that maximum parents feedback indicated that the group training was helpful and positive changes in parent child interactions at home were also observed.[7] Baker and McCurry (1984) conducted a parent training program among group of mothers. The program consisted of classroom observation, active learning, and video recordings. The result revealed significant improvements of self-care among children .[8]
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
112 | P a g e revealed that prevalence of dental caries 63.5% and periodontal diseases 13.6%. Also prevalence is higher among females children. These results shows majority of the Indian children of this age group are prone to develop dental caries and also requires special intervention to improve their oral hygiene.[9] Kashima KJ, Baker BL and Landen conducted a review study states that media based programme for parents of mentally retarded children regarding self- help skill teaching. Result revealed that live training increased parent’s knowledge of behavioural principles more than the media- based training.[10] A study conducted by Dennis Fauiks, Martine Hennequin on evaluation of oral health program by caretakers of children with intellectual disabilities. The main purpose of this programme is to educate the caretakers about dental disease, prevention, and to improve the oral hygiene among children with special needs. The result shows the impact of the program in terms of change teeth cleaned more than once from 24% to 52% (p < 0.05). Both posterior and anterior teeth increased from 24% to 60% (p < 0.05), and tooth cleaning increased from 36% to 60%.[11] The tooth brushing skills intervention will be enable them to have independent life in future rather than a burden on their parents, relatives and society.
The conceptual framework for this study is based on the review of literature and
clinical experience of the investigator. The present study is particularly intended to assess effectiveness of the tooth brushing interventions among children with intellectual disability. The investigator identified E. Kings Goal Attainment Theory suitable for this study. A model is used to denote the symbolic representation of the concept. Imogene King’s goal attainment theory is based on the personal and interpersonal system including interaction, perception, communication, transaction.[12]
The objectives of the study -
• To assess the tooth brushing practices among children with intellectual disability. • To compare the Tooth brushing practices among children with intellectual disability
before and after tooth brushing skills intervention in study and control group.
• HYPOTHESES –
• H0: There will be no significant difference in tooth brushing practices among children
with Intellectual disability before and after tooth brushing skills intervention. • H1: There will be significant difference in tooth brushing practices among children
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
[image:4.595.75.542.42.440.2]A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
114 | P a g e 2. RESEARCH METHODOLOGY
• Quasi experimental non randomized control group design was used. Total 20 samples (10 samples study group and 10 samples control group) were selected as per the sampling criteria, living in Navi Mumbai. The population of the present study is comprised of pair of children with intellectual disability and their parents/caretakers. The reliability of the tool was 0.996 determined by Cronbach’s Alpha method. Convenient sampling technique was used. A structure questionnaires and interview schedule was prepared and used for data collection. A tooth brushing intervention administered by the investigator for children with intellectual disability along with caretakers/parents. The tooth brushing skills intervention conducted with the help of Model, flash cards, charts and demonstration. The posttest was conducted after 12 weeks.
Study instruments used by the researcher consisted of: Structured questionnaire, which had two sections. Section I – Demographic variables
Age, gender, type of family, education of father and mother, monthly income of the family and types of intellectual disability.
Section II – Structure questionnaire related to tooth brushing practices.
DESCRIPTION OF VARIABLES
Independent variables: Tooth bushing skills intervention
Dependent variables: Tooth brushing practices
Extraneous variables: Extraneous variables are gender, type of intellectual disability, education of parents/care takers, socio economic status etc.
Inclusion criteria – Children with intellectual disability
o Both genders
o Children in the age group between 6-18 years.
o Who can understand Marathi or Hindi or English language.
o Who are present at the time of data collection. - Exclusion criteria
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
115 | P a g e
o Who are already gone through similar kind of training/sessions
o Who are having mental illness.
o Children with severe and profound intellectual disability.
3. RESULT AND DISCUSSION
[image:6.595.70.542.172.762.2]SECTION I- DESCRIPTION OF SAMPLE CHARACTERISTICS
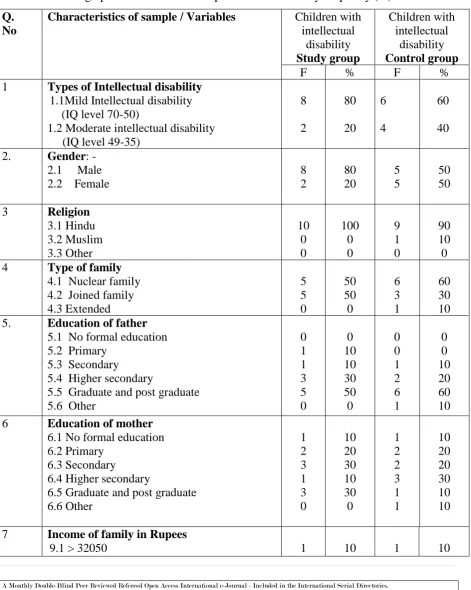
TABLE 1: Demographic distribution of samples characteristics by frequency (%) n = 20 Q.
No
Characteristics of sample / Variables Children with intellectual disability Study group Children with intellectual disability Control group
F % F %
1 Types of Intellectual disability 1.1Mild Intellectual disability (IQ level 70-50)
1.2 Moderate intellectual disability (IQ level 49-35)
8 2 80 20 6 4 60 40 2. Gender: -
2.1 Male 2.2 Female
8 2 80 20 5 5 50 50 3 Religion
3.1 Hindu 3.2 Muslim 3.3 Other 10 0 0 100 0 0 9 1 0 90 10 0 4 Type of family
a. 4.1 Nuclear family 4.2 Joined family 4.3 Extended 5 5 0 50 50 0 6 3 1 60 30 10 5. Education of father
5.1 No formal education 5.2 Primary
5.3 Secondary
5.4 Higher secondary
5.5 Graduate and post graduate 5.6 Other
0 1 1 3 5 0 0 10 10 30 50 0 0 0 1 2 6 1 0 0 10 20 60 10 6 Education of mother
6.1 No formal education 6.2 Primary
6.3 Secondary
6.4 Higher secondary
6.5 Graduate and post graduate 6.6 Other 1 2 3 1 3 0 10 20 30 10 30 0 1 2 2 3 1 1 10 20 20 30 10 10 7 Income of family in Rupees
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
116 | P a g e 9.2 16020 – 32049
9.3 12020 – 16019 9.4 8010 - 12019 9.5 4810 – 8009 9.6 1601 – 4809
4 2 2 1 0
40 20 20 10 0
3 3 2 1 0
30 30 20 10 0 The data presented in table no. 1: Demographic distribution of samples characteristics by
frequency and percentage (%)
Study group
Control group
80
60
20
40
P
erc
en
ta
ge
DISTRIBUTION OF CHILDREN ACCORDING TO TYPE OF DISABILITY
Mild Intellectual disability Moderate intellectual disability
Figure no. 2 Bar diagram showing types of disability among children.
[image:7.595.76.538.112.375.2]The data presented in table no. 1 and figure no. 2 reveal that in study group 80 % children were mild intellectual disability while in control group 60 % children had mild intellectual disability.
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
[image:8.595.76.543.139.353.2]117 | P a g e The data presented in table no. 1 and figure no. 3 revealed that majority 80 % children in study group were male whereas in control group consisted of 50% male children and 50% female children participation in study.
Figure no. 4 Bar diagram showing distribution of children according to types of religion
The data presented in table no. 1 and figure no. 4 reveal that in study group all samples were belonging to Hindu religions while in control group 90% samples were Hindu and 10% belonged to Muslims.
[image:8.595.71.528.483.742.2]A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
[image:9.595.117.483.141.356.2]118 | P a g e The data presented in table no. 1 and figure no. 5 reveals that all samples in study group were equally belong to Joint and nuclear family while in control group 60% samples from joint family, 30% from nuclear family and remaining 10% were belonging to extended family.
Figure no. 6 Bar diagram showing distribution of sample according to father’s education
The data presented in table no. 1 and figure no. 6 illustrates that in both study group and control group maximum samples father educated was up to graduate/post graduations.
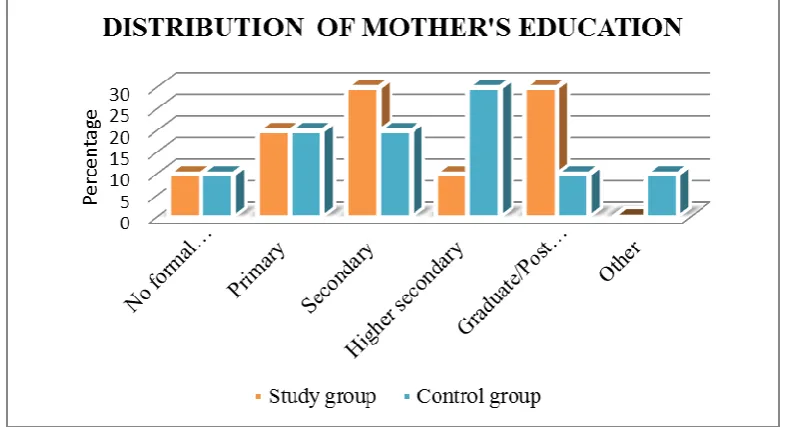
Figure no. 7 Bar diagram showing distribution of sample according to mother’s
[image:9.595.101.496.470.683.2]A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
[image:10.595.111.487.140.332.2]119 | P a g e The data presented in table no. 1 and figure no. 7 reveals that in study group maximum i.e. 30% mothers were educated up to secondary and 30% as graduates/post graduates while in control group 30% sample’s mother educated up to higher secondary.
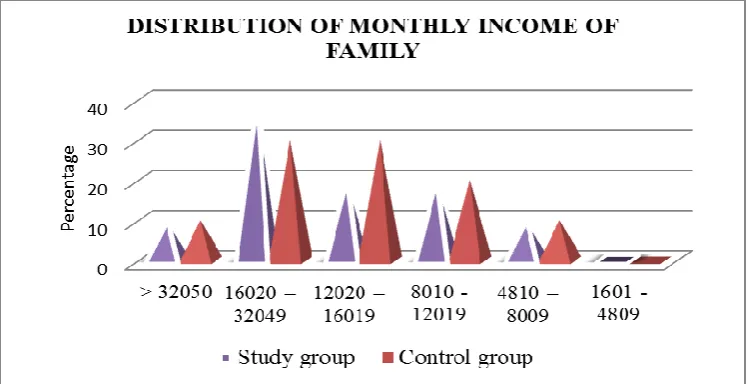
Figure no. 8 Bar diagram showing distribution of sample according monthly income of
family
The data presented in table no. 1 and figure no. 8 presents in study group majority 40% samples monthly family income ranged between Rs. 16020 – 32049 while in control group 30% samples monthly family income ranged between Rs. 16020 – 32049 and other 30% in ranged between Rs. 12020 16019.
SECTION II – TOOTH BRUSHING PRACTICES AMONG CHILDREN WITH
INTELLECTUAL DISABILITY BEFORE AND AFTER INTERVENTION IN STUDY
GROUP AND CONTROL GROUP
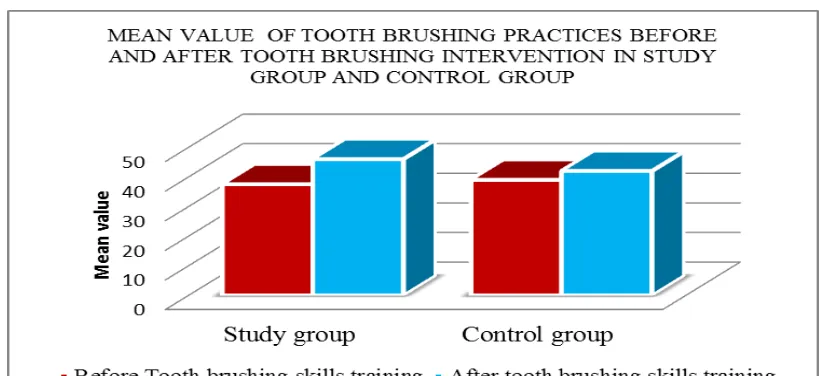
TABLE 2: Mean scores of tooth brushing practices among children with intellectual
disability before and after intervention in study group and control group n = 20
Phase Study group Control group
Before tooth brushing skills intervention 37.5 39
[image:10.595.78.528.606.677.2]A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
[image:11.595.91.503.31.219.2]120 | P a g e Figure no. 9 Bar diagram showing Mean value of tooth brushing practices before and
after tooth brushing intervetion in study group and control group
Figure no. 10 Mean scores of tooth brushing practices after tooth brushing skills improved as 11.33% (8.5) in study group while it improved by 4% (3) in control group.
SECTION III –COMPARISON OF TOOTH BRUSHING PRACTICES AMONG
CHILDREN WITH INTELLECTUAL DISABILITY BEFORE AND AFTER TOOTH
[image:11.595.71.555.436.525.2]BRUSHING INTERVENTION
TABLE 3: Significance differences in tooth brushing practices among children with
intellectual disability before and after the tooth brushing intervention. n = 20
Phase Mean score S.D Z p-value
Pre-test 37.5 8.6 2.81 0.005
Post-test 46 11.2
* P<0.05
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
121 | P a g e DISCUSSION
The study was intended to assess effectiveness of tooth brushing skills intervention
among children with intellectual disability. The results of the present study showed that p-value is <0.05level of significant, which indicates that there is a significant improvement in the tooth brushing practices among children with intellectual disability.
Similar study conducted by R. D. Horner and I. Keilitz on training of mentally retarded adolescent to tooth brushing. This study conducted on eight mentally retarded adolescents, in two groups, training included through role play, verbal instruction, flash card, and physical assistance. In that one group of four samples received token plus social reinforcement and other second received only social reinforcement. These findings suggested that all eight samples showed improved tooth brushing practices when compared to baseline. Six of the eight subjects correctly performed all tooth brushing steps in two of three consecutive sessions. Justification for the study was based on the fact that tooth brushing interventions were effective in improving tooth brushing practices among children with intellectual disability.
CONCLUSION
Children especially with intellectual disability predominated to dental caries. Oral hygiene is the most priority area and dental care is the greatest unattended health need among disabled children [14] A person with intellectual disabilities are left behind and allowed to lead a dependable life.
Approximately majority and more then 3/4th children with intellectual disability are in the mild category and they can often adequate self-help skills if adequate intervention or training is provided. They can become fairly self-sufficient and in some cases live independently when appropriate and consistent social, family and community supports provided. The above results also revealed that majority of children have poor in personal care and activities of daily living. Therefore it is important to identify various skills deficiencies and practices faced by children with intellectual disability and train as early as possible.
4. IMPLICATIONS
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
122 | P a g e intellectual disability are not identified until they enter school and sometimes not until they lacks in various life skills. According to the above studies oral hygiene cannot be maintained without proper tooth brushing interventions. The rate at which children with Intellectual disability acquire new leaning and self-care skills is well below that of typically developing children. In this situation family plays an important role as a trainer. In family children exposed with more with other members who allow them to learn self-care skills i.e. instructing the child that when he/she sees a familiar person while performing tooth brushing. The findings of the study have implication for mental health nursing practice and nursing education.
Mental Health Nursing Practice
Nurses working in special schools, psychiatric settings come across various children with intellectual disability. It is essential for children with disabilities to be taught activities of daily living eg. Tooth brushing, feeding, hair care, dressing and toilet training in order to be successful both at school and in life. The early childhood years constitute a critical window of opportunity for children to learn these skills. Children develop a sense of independence as they learn to do things for themselves.
Nursing Education
We are training nurses to achieve an international standard. To achieve high level of educational standards nursing education needs to be raised to a greater height. This will be achieved if all the aspects of health needs are considered as a whole. The education curriculum must include different developmental disabilities in syllabus, which will expose students to the various disabilities including intellectual disability to help the children, family and society. Similarly, early sign and symptom, preventive modalities, alternative therapies and skill training can be included in the nursing education curriculum.
RECOMMENDATIONS
Keeping in view the findings of the study, the following recommendations are made.
• It is suggested that the study may be replicated using a larger population of children with intellectual disability.
• Comparative Study of tooth brushing practices between Cerebral Palsy and children with intellectual disability.
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
123 | P a g e • Differences in tooth brushing intervention between school going and non-going
children with intellectual disability.
REFERENCES
1. Mental retardation ratio (online) 2001 April Available from URL:http://wikipedio.org. 2. National Sample Survey Organization. Disabled persons in India. NSS Report No.
485 (58/26/1), New Delhi. 2003.
3. www.DSM5.org. Highlights of Changes from DSM-IV-TR to DSM-5
4. Shreevani R. A guide to mental health and psychiatric Nursing. First edition, Japee publications, New Delhi. p. no. 151 - 170.
5. Nagarkar A, Sharma JP, Tandon SK, Goutam P. The clinical profile of mentally retarded children in India and prevalence of depression in mothers of the mentally retarded. Indian J Psychiatry. 2014;56:165–70.
6. Venkatesan S & Das A K. Reported burden on the family members in receiving/ implementing home based training programs for children with mental handicaps. Journal of Psychological Researches 1994, 38, 39-45.
7. Hornby G, Singh NN (1984) “Behavioral group training with parents of mentally retarded children. Ment Defic Res. 1984 Mar;28 (pt1) :43-52.
8. Baker, B. L., & McCurry, M. C. (1984). School based training: an alternative for parents predicted to demonstrate low teaching proficiency following group training. Education and Training of the Mentally Retarded, 19(4), 261–267.
9. M. Ghanashyam Prasad, A. Naga Radhakrishna, Halaswamy V. Kambalimath, Shalini Chandrasekhar, B. Deepthi, J. Ramakrishna. J Int Soc Prev Community Dent. 2016 May-Jun; 6(3): 213–218. Published online 2016 May 30. doi: 10.4103/2231-0762.183102
10.Kashima KJ, Baker BL and Landen SJ “Media based versus professionally led training for parents of mentally retarded children,” American J. of mental retar. v2, P. 209 – 217, Sep 1988.
11. Faulks, D. Jnd Hennequin, M. (2000), Evaluation of a long-term oral health program by carers of children and adults with intellectual disabilities. Special care in dentistry, Volume 20, Issue 5, September 2000, Blackwell Publishing Ltd, p. 199–208.
A Monthly Double-Blind Peer Reviewed Refereed Open Access International e-Journal - Included in the International Serial Directories.
International Research Journal of Human Resources and Social Sciences (IRJHRSS)
124 | P a g e 13. R. D. Horner, I. Keilitz. Training mentally retarded adolescents to brush their teeth, J.
apply behav. Anal. 1975, Fall; 8(3): 301-309 doi: 10.1901/jaba.1975.8-301 PMCID: PMC1311855.