The
use
of
admissions simulation
to
stabilize
ancillary
workloads
Walton M. Hancock
Department
of Industrial andOperations Engineering
University
ofMichigan
IOE
Building,
1205 Beal Avenue AnnArbor,
Michigan
48109Paul F. Walter Walter Software
Engineering
3692 Valentine Road
Whitmore
Lake,
Michigan
48189WALTON M. HANCOCK is Professor of Industrial and Operations
Engineering
and Professor ofHospital
Administration at The Univer-sityof Michigan.
His main area of interest is the use ofcomputer-aided
systems to reduce the costs of operating
hospitals.
His most recentmajor
publications
are The &dquo;ASCS’; The Inpatient AdmissionsScheduling
and Control System, and Advanced Work Measurement. He has three
degrees,
including
a Doctor ofEngineering
from The JohnsHopkins
University.
PAUL F. WALTER received his BSE from The University of
Michigan
College
of Engineering inapplied
mathematics in 1973.Following
ayear of software
development
for process control systems at AnnAr-bor Computer Corporation, he
joined
the staff of The Department ofHospital
Administration in the School of Public Health at The University ofMichigan.
There heparticipated
in the research anddevelopment
of an admissionscheduling
and control system, a nursestaffing
system,and other management information systems for
hospitals.
In 1982 he left the University but continued his efforts in thedevelopment
andimplementation
ofhospital
cost containment systems as the ownerof Walter Software Engineering. Mr. Walter is the coauthor of four
published
papers, more than a dozen reports and the book The &dquo;ASCS&dquo;Inpatient
Scheduling
and Control System.ABSTRACT
As part of the
planning
of a newhospital,
ananalysis
wasper-formed to determine the number of
procedures
that would beperformed
in each of nineteenancillary departments
on aday
of the week basis. Because the
planned
occupancy was not the maximumpossible,
attempts were madeusing
simulation to smooth thedaily ancillary
loadsby
varying
the admissionday
of
elective,
urgent
inpatient
andoutpatient
loads. Themethodology,
sample
outputs, and main conclusions arepresented.
Keywords: hospital
admissions,
hospital
occupancy,simulation
INTRODUCTION
As part of the
planning
process for a newhospital facility,
ques-tions aroseregarding
therelationship
betweenpatient
flows-both
inpatient
andoutpatient -
theexpected
load and thevariation in load
by day
of the week on theancillary
facilities.Earlier work made it
possible
to determine bedcapacities
ofeach clinical unit via simulation after
having
firstpredicted
thechanges
in thepatient
arrival rates andlength
of staydistribu-tions from the base year (1976) to the
planning
year (1990) and then to simulate thepatient
flows to determine the numberof beds for each service.b The Admission
Scheduling
andCon-trol
System
Simulator (ASCSS) allowedsimulating
patient
flows under a number of scenarios and with extensions, to determinethe average number of
procedures
that theancillary
depart-ments of interest would have to
perform
on adaily
basis. Thiswork was
accomplished
by
construction of several models: aninpatient
load model based onpatient flow,
and anoutpatient
procedures loading
model,
and a combinedinpatient
andout-patient
model.To pursue the
quantification
andinvestigation
of thepatient
flow
ancillary
demandrelationship,
the first model was struc-tured so as to allowanalysis
ofancillary
usage as a functionof two factors. The first
factor,
thepatient flows,
was to be de-rived from the ASCSSassuming
thatinpatient
decision rules based on the ASCSS would befunctioning
in thehospital.&dquo;’
The secondfactor,
theancillary
activity
generated by
agiven
inpatient,
was determinedby
assuming
that apatient
of agiven
type
(clinic
and type ofadmission)
would generate the sametotal
quantity
ofancillary
demand in 1990, as in 1976, but thatit would be distributed over the
predicted
shorterlength
of stay.By structuring
theinpatient
model in the manner describedabove,
answers are obtainable to thefollowing
questions:
How does the mean level of
ancillary activity,
due toin-patient demand,
varyby day
of week? andday
ofstay?
How should
patient
flows be altered to smooth demand ofancillary
services?What
type
of trade-offs occur whenpursuing
theobjec-tives to maximize average
occupancy?
or minimizeancillary
For the
outpatient loading
of theancillary
services,
1976out-patient
data were used toproject
the 1990 demand. Theassumption
was made that the distribution ofoutpatient
de-mand would remain the same for each
day
of the week butwould increase
by
amultiplying
factor. The combinedinpa-tient/outpatient
ancillary
serviceactivity
was then determinedby adding
the demands.By
analyzing
the results of the threeoutputs
(inpatient load, outpatient load,
and the totalload)
thefollowing
questions
could be answered:How much
impact
wouldinpatient
flow have on the overall demand for eachancillary
service?What would be the best method of
smoothing
ancillary
de-mand for eachancillary
serviceby manipulation
ofinpatient
flows? or
by manipulation
ofoutpatient
scheduled visits?or
by
both?How would overall demand vary
by day
of the week foreach of the
ancillary
services?The
following
assumptions
were made inperforming
thisstudy:
(1) The elective schedules could be
changed
toaccomplish
the
manipulation
ofinpatient flows;
the rationale was thatthe introduction of the Admission
Scheduling
and ControlSystem
decisionalgorithms
would cause this tohappen
anyway. The authors have
experience
ingetting
surgeonsto
change
theirscheduling
practices
provided
that the samenumber or more
procedures
can be done on an annualbasis and that the number of elective cancellations can be
reduced
sharply.
Also,
since thehospital’s operating
room(OR) utilization was
comparable
to the average for thein-dustry (approximately
55%)e
shifts in schedules werepossible
withoutincurring
a need to increase ORcapacity.
(2) The
outpatient
loading
could bechanged
if necessary toL
accomplish
theobjectives.
In 1976, there was atendency
to have more
outpatient
activity
early
in the week because of a desire to admit thepatient,
if necessary, in time to getdiagnostic
servicesperformed
before the weekend.How-ever, the
hospital
was very concerned about thelength
ofstay and its
inability
toexplain why
it was over twodays
longer
than that ofcommunity hospitals. Thus,
thehospital
wanted to assess the level ofstaffing
on weekends in orderto reduce
length
of stay.Proper
weekendstaffing
wouldrender the constraint of
seeing outpatients
earlier in the week nolonger
necessary.(3) That even
though
there would be resistance tochange,
the combination ofbuilding
a newhospital
and the fact that a newhospital
would have asubstantially
reduced bedcapacity
over an oldhospital
would cause manychanges;
the
analyses
shouldprovide
a best direction forchange
andnot be constrained
by
present
attitudesconcerning
OR andoutpatient scheduling.
PREVIOUS WORK
The
methodology presented
in this paper isunique;
it is basedon the
premise
thatancillary
load is drivenby
the type andfrequency
ofpatients
servicedby
ahospital.
By merging
pa-tient demand data with the accounts receivable computer
files,
one can
provide good
estimatesof ancillary
loads once the typeand number of
patients
to be admitted are forecasted.More traditional methods treat each of the
ancillary
depart-ments as
separate
entities and base estimates ofchanges
inan-cillary
demand on much more grossfigures
ofpatient activity
such as
patient
days
and/or admissions for the totalhospital.’
Other simulations of
inpatient
flows have been doneby
Dumasand
Stap!eton/
but their work has not been extended toan-cillary
loads.THE DATA
USED
All data collected in the bed
determining
process’
was usedincluding
admissiondata,
type ofadmission,
service ofadmis-sion, transfer
dates,
transferservices,
anddischarge
date.In-formation about each fee code record
generated
by
the pa-tientsdischarged
from thehospital during
the 1976 calendar year was obtained as well as fee code datagenerated
by
alloutpatients
in 1976. Aftereliminating
data which was notnecessary for the
ancillary departments
underconsideration,
sets of data items for each of the
24,698
error free records ofinpatients
were constructed. The data included thefollowing
items:
(1 ) Patient
registration
number(2) Admission and
discharge
dates(3)
Age
(4) Sex
(5)
Billing
zip
code(6)
Type
of admission(7)
Discharge
status(8) Total
length
of stay(9) Number of
days
on pass(10) Codes for up to six
diagnoses
explaining
admission(11) Codes for up to six
operative
procedures
including
dates of occurrence(12)
Discharge
service(13)
Lengths
of stay and clinical servicescorresponding
to eachof up to six rooms in which the
patient
stayed
(14) Fee code data:· Fee code number
· Account number
. Insurance code
· Quantity
of serviceprovided
. Service date.
Additionally,
a set of data items was constructed for137,886
outpatients
seen at thehospital during
the 1976 calendar yearwho used the
ancillary
departments
of interest. This set included thefollowing
data items for eachpatient:
(1) Patient
registration
number(2) Fee code data:
· Fee code number
. Account number
.
Quantity
of serviceprovided
,
. Service date
. Location
code,
indicating
clinical unit of fee codeorigin.
MODEL CONSTRUCTION
Briefly,
the ASCSS uses a Monte Carlotype
simulator. Simula-tion models were constructed based onanalysis
of historicaldata
providing
for the definition ofpatient
arrival rates,crossflows between clinical units and all associated
length
of stay distributions for each type of admission for each clinicaladmissions and also restores census with
patients
called in fromwaiting
lists of urgentpatients
asdischarges
occur.In essence, the model is a
study
in networkanalysis
ofpatient
flows mto, outof,
and between each of the model’s clinics withassigned
bedcapacities.
Patient flows are vectors and arede-fined
by
their arrival rates, cumulativelength
of stay distribu-tions and thehospital
policies constraining
their use. Thesim-ulator can handle up to 16 clinical units in one model. Some
simulation
models,
especially teaching hospitals,
may have upto 200 random number generators and cumulative
probability
distributions. Simulation
objectives
consist ofmaximizing
modeloccupancy within
predefined
ranges of constraints oncancella-tion of scheduled admissions and times when beds are not
available for emergency arrivals. The
simulator,
written in PL/I andassembly language,
isoperational
on theUniversity
ofMichigan’s
Amdahl computer under the MTSoperating
system.To construct the
inpatient
output,
patient
flows were simulatedand the
ancillary
services’ demands associated with thein-dividually
simulatedpatients
were tabulated based on eachpa-tient’s clinical unit of
residence,
type ofadmission,
day
ofad-mission,
andday
ofstay.
For theoutpatient
output, it wasnecessary to determine the level of demand for each
ancillary
activity
and tabulate the demands based on the totalexpected
number of
outpatient
visits for eachday
of the week in theplan-ning
year of 1990. The tabulated demands from bothinpatient
andoutpatient
outputs were then usedtogether
to form thecombined model and
produce
the final result.UNIQUE
MODEL ASSUMPTIONS
Since the data available for
analysis
was from calendar year1976 and the output was to reflect the 1990
expected activity,
analysis
was based on twounique assumptions.
The first wasthat in 1990
ancillary
services rendered perpatient
would be the same as in 1976, except that the rate perday
would beincreased due to the
predicted
shorter averagelength
of stay(LOS). After
adjusting
for factors determined to reduce LOS suchas
changes
inpatient
mix,
preadmissions testing
andoutpa-tient surgery,
length
of stay wasprorated
so that overall LOSwould be 8.9
days
ascompared
to the 1976 LOS of 10.3days.
A
major
implication
of thisassumption
was thatancillary
ser-vice &dquo;turnaround&dquo; time would thus be shortened
by
the ratioof the 1990 to 1976 LOS.
The second
assumption
was thatancillary
load data reflectedthe load
imposed
on theancillary
servicesby
the clinicalser-vices. In the
ancillary
database,
the date recorded included the&dquo;day
of request orday
of service.&dquo;Ideally,
we would haveliked to have used
only &dquo;day
ofrequest&dquo;
as the basic measureof load. Since the
day
of service was theday
service wasini-tiated,
in the vastmajority
of cases, exceptpossibly
requestsmade on
weekends,
theday
ofrequest
andday
of service wereassumed to be the same. Since the same amount of
ancillary
work was to be
accomplished
with fewerinpatient
days,
ascheme had to be devised to redistribute the
ancillary
activitiesto the
appropriate
days
in 1990.Briefly,
this wasaccomplished
by:
(1)
Generating
an intermediate data set(2)
Redistributing
theancillary
services to the 1990predicted
length
of stayby
a linear transform for eachpatient
in the1976 data base
(3)
Developing
a summary matrix ofancillary
loadby
clinical service, type of admission(elective,
emergent, urgent,
ortransfer),
day
of stay, andancillary department.
COMPUTER PROGRAMS
AND
ORDER
OF PROCESSING
In order to
perform
theanalysis
ofancillary
activity
due toin-patient flow,
it was necessary tomodify
the ASCSS so that itcould
produce
patient
flow matrices based on ASCSS modelsimulations. These
modifications,
though
notextensive,
weretime-consuming given
theexisting
complexities
of the simulator and its model support routines. The modifications includedad-ding
thecapability
to record andtally
eachpatient
within themodel for each
day
of stay thepatient
was in the model as well as thepatienfs
admission and transfer statistics. These data hadto be tallied on the basis of the clinical unit with which the
patient
was associated as well as the admissiontype
by
which thepatient
was admitted to thehospital.
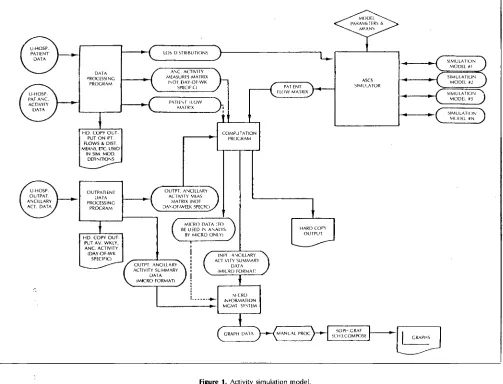
Figure
1 is agraphical
representation
of themethodology
usedto
produce
theancillary activity
models. In the upper left cor-ner is the &dquo;DataProcessing Program&dquo;
which used bothpatient
data andancillary
activity
data asinput.
A number ofinpatient
data items used
by
other programs weregenerated:
(1) All arrival rates and distributions needed to define and build the ASCSS models
(2) The
inpatient
portion
of theancillary
activity
measuresmatrix
(3) The
patient
flow matrix used in theproduction
of a runreflecting
the way thehospital operated
in 1976.The lower left-hand corner of
Figure
1 shows the program thatprocessed
the outpatientancillary
activity
data. It too was amultipurpose
program andproduced:
(1) The
outpatient portion
of theancillary
activity
measuresmatrix
(2) Hard copy
figures
detailing
the numbers ofoutpatients
par-ticipating
in theancillary
activities understudy
(3) A MICRO formatted data set of
outpatient ancillary
activ-ity
to be usedeventually
in theproduction
ofgraphs.
The ASCSS(upper
right-hand
corner ofFigure
1) functionedin the
following
manner: For each scenario ofpatient
flowunder
study,
a separate model was constructed. Each modelwas simulated as many times as necessary until the simulation statistics reflected the desired
hospital
setting.
A
computation
program(upper
middle ofFigure
1) was runusing
a differentpatient
flow matrix each time to beintegrated
with the
inpatient
ancillary
activities measures matrix topro-duce MICRO formatted data sets with hard copy
statistics.’
Aggregation
ofgraph
data resulted from the use of the MICROformatted data sets in
conjunction
with the MICROInforma-tion
Management
System.
From this program and theformat-ted
data,
approximately
400 different sets of data werepro-duced. Further
manipulation
was necessary before theSOPH:GRAF and the SCH3:COMPOSE canned programs were
used to
produce
the 67graphs
andcomposite
graphs
of thestudy.
RESULTS
AND
CONCLUSIONS
(1 )
Day
OfStay
Graphical
Summaries. For each of the 19an-cillary
departments
ofinterest,
graphical
summaries wereproduced
thatdisplayed
the effect ofday
of stay onan-cillary
load.Figure
2 is anexample
of theinpatient
pro-cedure load on the
Biochemistry Laboratory
as a functionFigure 1. Activity simulation model.
a
relatively higher
load the first fewdays
of stay. Otherlaboratories such as
Physical
Therapy (Figure
3) exhibiteda
procedure
load that washigher
as theday
of stayin-creased. Of the 19 laboratories of
interest,
14 exhibitedFigure 2. Average daily ancillary load for Biochemistry Laboratory.
higher
loads the first fewdays
ofstay (Table
1). Thisobser-vation is somewhat
misleading,
as discussedlater,
becausethe
impact
ofhigher
loads was found to beconsiderably
dampened by
the&dquo;steady
state&dquo; loads that had to be metevery
day.
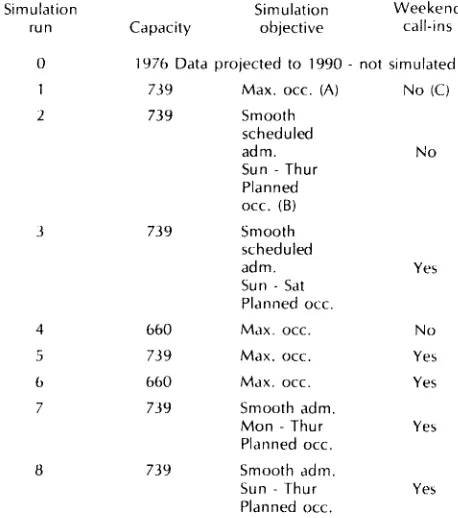
(2) The Effect Of
Varying Inpatient
Patient Flows. Table 2 de-fines theexperimental
scenarios for the simulation runs.The
analysis
wascomplicated by
the use of two bedca-pacities.
At thispoint
in theplanning
process, the number of beds that thehospital
administration had decided to buildwas 739. The minimum number needed to care for the
pre-dicted
patient
demand under maximum average occupancyconsiderations was determined to be 660. The
higher
number (739) gave much moreflexibility regarding
whenscheduled elective
patients
could beadmitted,
whereas thelower number (660) gave no
flexibility
except whether ornot urgent elective
patients
were to be admitted on theweekends.
Thus,
all except runs 4 and 6 used the 739 bedcapacity.
The &dquo;Smooth Scheduled Admissions&dquo; was an at-tempt to smooth the workload ori theancillary
services.It was chosen as an
approach
because so many of thean-cillary departments
(14 of 19) hadhigher procedure
loadsFigure 3. Average daily ancillary load for Physical Therapy.
Table 1. A list of the laboratories having higher procedure loads the first few
days of stay.
Approximate ratio of first or
second
day procedure
rate to--
the average of the
following
18a simulation but as the 1976 admission data transformed (LOS, admissions rate) to the 1990
planning
year, so thatthe
hospital
administration could compare any newadmis-sions
policies
with thosethey
wereusing
in 1976.The weekend call-ins factor was included to show the ef-fect of the presence or absence of urgent elective
admis-sions on weekends because some third party reimbursers
were not
paying
for urgent electivepatients
admitted onweekends.
(3) The
Graphical
Output.
Themajor
output
of the effort was a series of threegraphs
for each of theancillary
depart-ments : averageinpatient
procedure
load,
the averageout-patient procedure load,
and the combined averagepro-cedure load.
Examples
of thesegraphs
arepresented
using
the
Biochemistry
Laboratory
as anexample
(Figures
4, 5,and 6). In these
figures
the average number ofprocedures
isplotted
for eachday
of week for each of the simulationruns. The numbers
superimposed
on thegraphs
are thesimulation run numbers of Table 2. For the
inpatient
and totalloads,
a relative scale ispresented along
theright
sidewith 100
being
the lowestpoint,
so that one can get anidea of the relative
change
in load fromday
today,
whichis
presumed
to be related to staff size.The
following
items represent our conclusionsconcerning
thetotal
ancillary
loads:A. The variation in average load
by day
of week was differentfor each of the
ancillary departments. Thus,
nosingle
in-patient
admissionpolicy
wouldprovide
a stable workloadfor all 19
departments.
B.
Outpatient
loads tended to mask and dominate variation in load due toinpatient policies. Thus, outpatient
clinicscheduling
was a critical aspect of thestability
forancillary
demands.
C. Maximum
occupancies
at theplanned
capacities
(739beds)
gave much
higher
loads (runs 1 and 5) than loadsimposed
by projected
occupancies. Thus,
if 739 beds were to bebuilt,
ancillary
capacities
should be based on maximumoccupancy conditions not
planned
occupancy conditions.D. The differences in
inpatient
admissionspolicies
wereprimarily
reflected in total loads onSaturday
andSunday
when
outpatient
demand was the lowest.Table 2. A scenario of the inpatient simulation runs.
Note: (A) Max. occ. is where
hospital
beds would be used tomaximum extent
subject
to scheduled admission cancellations and no beds for emergencycon-stramts. This gives an upper bound to the use of
ancillary
tacilities.(B) Planned occ. is the
planned
occupancy for 1990.(C) Weekend call-ins &dquo;no&dquo; is where urgent electives
[image:5.606.322.551.359.618.2]Figure 4. Average number of inpatient procedures versus day of the week for Biochemistry Laboratory (for the simulation runs of Table 2).
E. The
generally higher
activity
of theoutpatient
departments
on
Monday
andTuesday
versusWednesday, Thursday
andFriday
wasgenerally
reflected in the total load curves.Thus,
if at all
possible,
outpatient activity
needed to be reducedon
Monday
andTuesday
and increased onWednesday,
Thursday,
andFriday
to smooth the total load.F.
Preventing
weekend urgent elective call-ins onFriday
andSaturday
decreasedancillary
loads onFriday
andSaturday,
but
substantially
raised them onSunday,
so that in manyancillary departments, Sunday
had thehighest
load of anyday
of the week.G. Most of the
ancillary departments
are labor intensive sothat the number of
procedures
areprobably linearly
related to the staffsize,
both on an absolute and a relative basis.Thus,
staffing
on adaily
basis could be determinedusing
the data of this
methodology
plus
the labor hours perpro-cedure data for any
given ancillary
department.
Using
thefollowing
data as anexample
ofstaffing
for theBiochemistry
Laboratory:
(i) Let the load
predicted by
simulation run #8 be theplanned
load and the loadpredicted by
run #5 be themaximum load
(ii) Assume an average time per
procedure
of 5.0 minutes(iii)
Assume a 450.0 minuteworking day.
Table 3
gives
therequired
staffsby
day
of the week. Please note thehigh staffing required
onSaturday
andSunday
andthe differences between
planned
and maximum averageloads.
(4)
Outputs
versus Present Practice. A cursory examination ofthe
staffing
patterns
indicatedby
run 0(1976
policies)
and the actual staff used in thehospital
revealed atendency
to
substantially
understaff on weekends and to overstaffon
Fridays.
Thesepractices
probably:
~
Substantially
raised theancillary
loads onMonday
andTuesday,
which in many cases werealready relatively
high
due tooutpatient
policies.
if this demand is to bemet with full-time
staff,
overstaffing
toward the end of the week will occur if the units arecorrectly
staffeddur-ing
the first part of the week.~
Substantially
increased LOS due to thedelay
ofservic-ing
of requests for service on the weekends.~ Caused
physicians
to minimize treatment on weekendsbecause of the poor
ancillary
response.(5) Predictions of Weekend
Staffing
By Department.
Examina-tionof Table
4,
which comparesMonday
toFriday
loadsversus
Saturday
andSunday
loads,
reveals that the [image:6.605.308.548.326.693.2]staff-ing
on the weekend issurprisingly high.
This result is dueFigure 5. Projected average number of procedures caused by outpatient
Figure 6. Total average number of procedures (inpatient plus outpatient) for
Biochemistry Laboratory.
Table 3. Predicted average daily staff at planned and maximum average load for the Biochemistry Laboratory.
to the
&dquo;Steady
State Load&dquo; of many of theancillary
servicesafter the first few
days
ofstay
and to theassumption
thatwas made that the number of
procedures
for apatient
wasdue to the type of
patient
and theday
of stay, not to theday
of the week. Thisassumption
wasjustified
on the basisthat there was great interest in
reducing
the LOS ofpatients
and that one of the ways to do this was to
provide
the same intensive service on weekends asduring
the week. Ifstaff-ing
is relatedlinearly
toload,
then thepercent
figures
give
an indication of the
Saturday
andSunday
staff. Thefollow-ing
is observed:.
Saturday
toSunday
staff varied betweenancillary
depart-ments, but in all cases needed to be
higher
thananticipated.
Table 4. A companson of the Saturday and Sunday average ancillary load with the Monday through Fnday load using simulation run #8 (from Table 2).
. Overall average is 80% on
Sunday
and 74% onSatur-day indicating
the weekend staffs needed to beroughly
three-fourths of the staffduring
the week. This issubstan-tially
different than thepresent
staffing
of thehospital.
REFERENCES
1 DOWLING, W.
"Converting Demand Forecast into Facility Requirements." Cost Control in
Hospitals, Section 11.3. Health Administration Press, Ann Arbor, Michigan
(1976) 70-89.
2 DUMAS, B M. and STAPLETON, C. J.
"Hospital Bed Planning Via Computer Simulation." Simulation in Health Care
Delivery Systems. The Proceedings of the Conference on Simulation in Health
Care Delivery Systems, Simulation Councils, Inc., La Jolla, California (1983),
13-20.
3 GRIFFITH, J. R.; HANCOCK, W. M.; and MUNSON, F. C.
"Admission scheduling and control systems," Cost Control in Hospitals, Sec-tion III.2. Health Administration Press, Ann Arbor, Michigan (1976), 150-185. 4 HANCOCK, W. M.; JOHNSON, C.; MAGERLEIN, D.; MARTIN, J.; and
WALTER, P.
Replacement Bed Size for University Hospital : Determination and Final Results. Report No. 78-1. Management Information Systems Group of the
Department of Hospital Administration, The University of Michigan, Ann
Ar-bor (May 1978).
5 HANCOCK, W. M. and WALTER, P. F.
The "ASCS" Inpatient Admission Scheduling and Control System. AUPHA Press,
Ann Arbor, Michigan (1983). 6 HANCOCK, W. M. and WALTER, P. F.
University Ancillary Services Project. Report 80-1, Management Information
Systems Group of the Department of Hospital Administration, University of Michigan (January 1980).
7 KAHN, M. A.; RUMELHART, D. L., and BRONSON, B. L.
Micro Information Management System Reference Manual. Institute of Labor
and Industrial Relations, The University of Michigan, Ann Arbor, Michigan
(October 1977).
8 ROBINSON, G. H.; WING, P.; and DAVIS, L. E.
"Computer Simulation of Hospital Patient Scheduling Systems." Health
[image:7.603.319.549.69.311.2]