pISSN 2320-1770 | eISSN 2320-1789
Research Article
Clinical study of post operative wound infections in obstetrics and
gynaecological surgeries in a tertiary care set up
Amrita R. Bhadauria*, Chella Hariharan
INTRODUCTION
Despite advances in operative techniques and a better understanding of the pathogenesis of wound infection and wound healing, post operative wound infection (surgical site infections) continue to be a major source of morbidity and mortality for patients undergoing operative procedures. The overall incidence of wound sepsis in India is from 10%-33%. However, the incidence of wound complications in the obstetric population varies with rates ranging from 2.8% to 26.6%.1-3 Surveillance of post operative wound infection or surgical site infection (S.S.I.) is useful tool to demonstrate the magnitude of the
problem. By keeping the above points in mind, the present study was conducted for early recognition of the problem so that early intervention can be done for better management of postoperative wound infections in our problem.
METHODS
The prospective study of wound infection was carried out in Acharya Vinoba Bhave Rural Hospital in the department of Obstetrics and Gynaecology from August 2011 to August 2013 after the approval from the Ethical Department of Obstetrics & Gynecology, Jawaharlal Nehru Medical College, DMIMS, Sawangi (Meghe), Wardha, Maharashtra, India
Received: 19 October 2013
Accepted: 27 October 2013
*Correspondence:
Dr. Amrita R. Bhadauria,
E-mail: dr.amrita.b87@gmail.com
© 2013 Bhadauria AR et al. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Background: The study was performed with the aim to find out the incidence of post-operative wound infection among the elective and emergency obstetrics and gynaecological abdominal surgeries in the Dept. of OBGY, A.V.B.R.H., Sawangi (Meghe), Wardha with the objectives to identify the risk factors and most common causative micro-organism and to study the preventive aspects.
Methods: This prospective observational study was carried out in the Dept. of Obstetrics and Gynaecology at Acharya Vinoba Bhave Rural Hospital, Sawangi (Meghe), Wardha, India from August 2011 to August 2013.
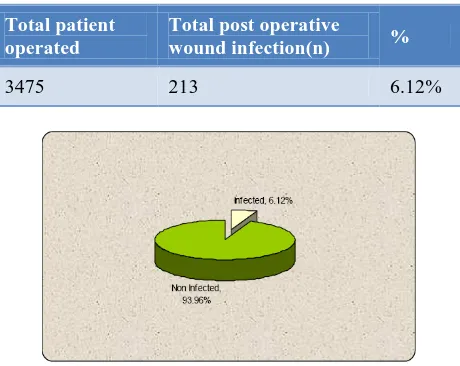
Results: During this period a total of 3475 patients underwent major abdominal surgeries, out of which 213 cases develop post operative wound infections with rate being 6.12%.The rate was found to be higher among the emergency obstetric case (51.17%) with the common risk factors being anaemia, advanced age and diabetes among gynaecological surgeries and prolonged rupture of membranes and previous LSCS and multiparity among obstetric cases. The common causative organism was found to be E. coli (36.15%).
Conclusion: The merit of this study was to start the active surveillance of surgical site infections based on standard definitions and methods to be maintained by cooperation of infection control practitioners and surgical team. Identification of risk factors for surgical site infections to encourage the development of recommendations for prevention of SSI in order to achieve the setting goal to reduce the SSI.
Committee. The study population consisted of 3475 patients who underwent surgery in the A.V.B.R.H.
Inclusion criteria
1. Surgery done in this hospital.
2. Occurs within 30 days after the operation. 3. Involves only the skin or subcutaneous tissue.
Exclusion criteria
1. All patients who were not operated in A.V.B.R.H. 2. Patient coming with wound infection after
getting discharge from the hospital.
All these patients were thoroughly examined and investigated on admission and prepared for operative procedures through abdominal approach, either elective or emergency. Patients who underwent surgeries were grade 3 or less than grade 3 according to ASA score.4 Operated patients were followed up regularly, during the post operative period. The wound was checked on 4th post-operative day routinely and earlier and later according to the complaint of the respondents.
Wound swabs were sent for culture and sensitivity where discharge from the wound was present. Severity of the post operative wound infection were graded according to the Southampton wound grading system (Bailey IS et al).5 Micro-organisms were identified and their antibiotic sensitivity were done. Treatment was started in accordance with the culture sensitivity report. Patient’s progress and the response to drug treatment were monitored. If needed secondary suturing was done and noted. Complications and their cause were identified thereby providing a clue to their successful prevention.
RESULTS
The present study was undertaken in Department of OBGY, Jawahar Lal Nehru Medical College and Acharya Vinoba Bhave Rural Hospital Sawangi (Meghe) Wardha from August 2011 to August 2013 after approval from the Ethical Committee. The study population consisted of 3475 patients who underwent major abdominal surgeries in the A.V.B.R.H. In present study based on our inclusion criteria, total 3475 operated patients were eligible for analysis (2782 elective surgery and 693 emergency surgery) who underwent surgery in A.V.B.R.H. Post operative wound infection (SSIs) was found in 213 patients out of 3475 patients with an overall post operative wound infection rate of 6.12%. Age of the population ranges from 20-70years, being the patient of obstetrics and gynaecology, all were females. Majority of the population was housewives. Regarding the educational status one quarter of the patients were illiterate. Types of surgery done among the wound infected population were caesarean section, total abdominal hysterectomy and laparotomy. The wound infection rate was found to be more amongst the
emergency cases (16.01%) as compared to elective (3.67%) and that too amongst emergency obstetric cases (51.17%). The total number of cases were graded according to the Southampton wound grading system and was found to be higher among grade I(124) and lowest among grade V(4). Of 118 obstetric cases of wound infection; performed both in elective and emergency hours; 35(29.66%) cases underwent caesarean section for previous c-section and 26(22.03%) cases were due to prolonged rupture of membranes(>4 hrs). Anaemia 45 (21.13%), Advanced Age 41(19.72%) and Multiparity 70(59.32%) were found to be the other common risk factors involved in wound infection. In 74.19% (158) of patients the wound discharge appeared after 4thpost operative day. E. coli (36.62%) was the most common organism found in wound swab culture. Out of 213 cases, 83(38.97%) were sterile. Sensitivity for amoxyclav (39.44%) was found to be more. Other drugs found to be sensitive were gentamicin (20.66%) and cefotaxime (27.72%). Amikacin (10.80%) was sensitive commonly for grade IV(5.16%) and V(1.88%). Grade I and II had minor complications like fever, while in grade III, IV and V had major complications like gaping. Out of 213 patients of post operative wound infection, 179(83.10%) patients of grade I, II and III were managed conservatively and surgical management was required in 34(16.90%) of grade III, IV and V. Morbidity of post operative wound infected patients in terms of average hospital stay was more in grade V( mean=36.75 days) as compared to grade I(mean=11.53 days).
Table 1: Post operative wound infection rate in surgical patients.
Figure 1: Post operative wound infection rate in surgical patients.
rates between the two subgroups by type of surgery was statistically significant (P ≤0.0001, RR1.11 with CI: 675-1.08-1.15), being 3.67% (102/2782) for the Elective, 16.01% (111/693) for the Emergency. This difference was statistically significant with P ≤0.0001.
Table 2: Post operative wound infection rate in type of surgery.
Type of Surgery
Total patients operated
Total post operative wound Infection (n)
%
Elective
Patients 2782 102 3.67
Emergency
Patients 693 111 16.01
(P =<0.0001, Significant, RR =1.11, with CI =1.08-1.15)
Figure 2: Post operative wound infection rate in type of surgery.
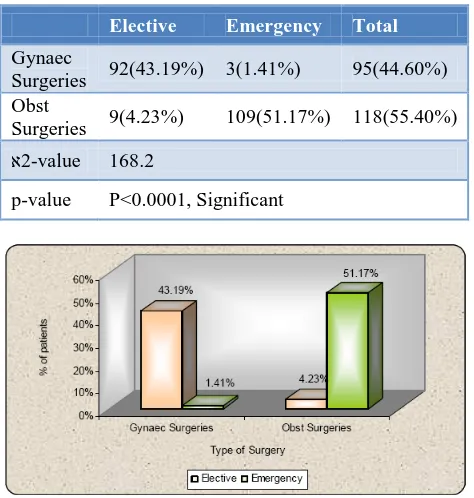
Table 3: Post operative wound infection rate among different surgeries.
Elective Emergency Total
Gynaec
Surgeries 92(43.19%) 3(1.41%) 95(44.60%) Obst
Surgeries 9(4.23%) 109(51.17%) 118(55.40%) א2-value 168.2
p-value P<0.0001, Significant
Figure 3: Post operative wound infection rate among different surgeries.
In the present study, the post operative wound infection was studied in two different sub groups. The total number of infected patients were 118(55.40%) amongst obstetric cases. Amongst gynaec cases, the total number of infected patients were 95(44.60%). The infection rate was slightly higher among obstetric cases and that too among those which were done in emergency {109, (51.17%)}.
Table 4: Post operative wound infection according to Southampton Wound Grading System.
Grade No. of post operative wound infected patients(213 Patients)
I 124 58.2%
II 52 24.4%
III 22 10.3%
IV 11 5.2%
V 4 1.9%
Total 213 100.00%
Source: Bailey IS, Karran SE, Toyn K, Brough P, Ranaboldo C, Karran SJ. Community surveillance of complications after
hernia surgery. BMJ 1992;304 (6825): 469-71.
Figure 4: Post operative wound infection according to Southampton Wound Grading System. From table no.4 it was observed that postoperative wound infected patients were maximum in grade 1 (58.20%) as compare to other grades according to Southampton Wound Grading System.
Table 5: Indications of LSCS.
Indications Elective Emergency
PROM 0(0%) 26(22.03%)
Previous LSCS 6(5.08%) 29(24.58%)
Fetal Distress - 16(13.56%)
NPOL - 14(11.86%)
Failed Induction - 1(0.85%)
Twin - 4(3.39%)
Breech - 15(12.71%)
BOH - 7(5.93%)
Figure 5: Indications of LSCS. Table 6: Risk factor in post operative wound
infection patients.
Risk Factors
No. of P.O. wound infected patients
%
Advanced Age 42 19.72
Diabetes 18 8.45
Obesity 29 13.62
Hypertension 10 4.69
Anaemia 45 21.13
Multiparity 70 59.32
No risk factor 55 25.82
From table no.6 it was observed that among all groups of infected patients anaemia 45 (21.13%), advanced age 41(19.72%) and multiparity 70(59.32%) were found to be common risk factors.
We analyzed the data by multiple logistic regression and found that after stepwise adjustment certain factors like Type of surgery, Nature of surgery, Anaemia, PROM, Obesity, and Diabetes were most significant factors in the present study as compared to others.
Figure 6: Risk factor in post operative wound infection patients.
Table 7: Logistic regression analysis.
Parameter P value
Clean + Contaminated 0.000,S,p<0.05
Complications 0.400,NS,p>0.05
Obesity 0.000,S,p<0.05
Diabetes 0.000,S,p<0.05
Advanced Age 0.045,S,p<0.05
Anemia 0.000,S,p<0.05
PROM 0.000,S,p<0.05
Previous LSCS 0.04,S,p<0.05
Length of stay 0.029,S,p<0.05
*S- significant at P< 0.05 NS- Not Significant at p<0.05
From table 8 it was concluded that E. coli (36.62%) was the most common organism found in wound swab culture. Out of 213 cases, 83 were sterile.
From table 9 it was observed that sensitivity for amoxyclav was found to be more. Other drugs found to be sensitive were gentamycin and cefotaxime. Amikacin was sensitive commonly for grade IV and V.
Out of 213 patients of post operative wound infection,179(83.10%) patients of grade I, II and III were managed conservatively and surgical management was required in 34(16.90%) of grade III, IV and V.
From table 11 it was observed that morbidity of post operative wound infected patients in terms of average hospital stay was more in grade V ( mean=36.75 days) as compare to grade I (mean=11.53 days).
signifies that the source of infection was from hospital ward or attendants etc.
Table 8: Distribution of antibiotics in relation to causative microorganism in post operative wound infection.
Antibiotics
Causative Microorganism
T
o
ta
l
% Per
ce
nta
g
e
E
-C
o
li
E
-C
o
li+
Kleb
siella
Kleb
siella
Stap
h
y
lo
co
cc
u
s
au
reu
s
Ps
eu
d
o
m
o
n
as
Ster
ile
MRS
A
Amikacin 8 6 3 2 2 1 1 23 10.80
Cefotaxime 24 5 5 5 4 16 59 27.70
Amoxyclav 28 3 3 2 6 42 84 39.44
Gentamicin 16 1 1 2 24 44 20.66
Doxycycline 2 1 3 1.41
Total 78 14 13 10 14 83 1 213 100
Percentage 36.62 6.57 6.10 4.69 6.57 38.97 0.47
א2
-value=56.006, p-value=0.000, Significant
Table 9: Distribution of antibiotics as per Southampton wound grading system in post operative wound infection.
Grade Antibiotics as per Southampton wound grading system
Amikacin Cefotaxime Amoxyclav Gentamicin Doxycycline No %
I 1 29 55 38 1 124 58.22
II 4 22 19 6 1 52 24.41
III 7 5 9 1 22 10.33
IV 7 3 1 11 5.16
V 4 4 1.88
Total 23 59 84 44 3 213 100
% 10.80 27.72 39.44 20.66 1.41 100
א2
-value=107.29, p-value=0.000, Significant
Figure 8: Distribution of antibiotics as per Southampton wound grading system in post operative
wound infection.
Table 10: Management of post operative wound infection.
Management
Grade
Total %
I II III IV V
Conservative 124 52 3 - - 179 83.57
Surgical - - 19 11 4 34 16.43
Total 124 52 22 11 4 213 100
א2-value 189.99
p-value 0.000,S,p<0.05
Figure 9: Management of post operative wound infection.
Table 11: Association of hospital stay with respect to Southampton wound grading system in post operative
wound infection.
Grade Average Hospital stay (days) SD
I 11.53 7.50
II 12.80 3.48
III 22.40 9.58
IV 29.90 9.67
V 36.75 2.06
Total 18.56 10.80
F-Value 35.91
p-value 0.000, Significant
Figure 10: Association of hospital stay with respect to Southampton wound grading system in post operative
wound infection.
Table 12: Day on which post operative wound infection noted.
Gynaec Obstetrics
Elective Emergency Elective Emergency <4
days 29(13.62%) 0(0.00%) 0(0.00%) 26(12.21%) >4
days 63(29.58%) 3(1.41%) 9(4.23%) 83(38.97%) Total 92(43.19%) 3(1.41%) 0(0.00%) 109(51.17%) Mean 5.35 6.33 5.33 5.31
SD 1.46 1.52 0.70 1.26
Figure 11: Day on which post operative wound infection noted.
DISCUSSION
Jahanara Rahman.7 Mean age group was found to be 42 among gynaecological surgeries. No co-relation with wound infection among obstetric cases. Incidence of post operative wound infection (S.S.I.) was more in emergency obstetric patients (51.17%) and clean contaminated nature of surgery patients (15.87 %) and it is quite comparable with the study performed by Jahanara Rahman et al.7 The incidence of wound infection in obstetric surgeries was found to be higher among the previous c-section (24.58%) and prolonged rupture of membranes (>4hrs) (22.03%). Other indications are found to be less contributing towards the post operative wound infection among obstetric surgeries. Anaemia (21.13%), advanced age (19.72%) and multiparity (59.32%) were overall common risk factors in post operative wound infected patients. Uncontrolled Diabetes and anaemia delay wound healing, and causes tissue breakdown which leads to post operative wound infection (SSIs). Fat in subcutaneous plane (obesity) causes lipolysis in fatty patients which contributes in SSIs as serous discharge. The incidence of prolonged rupture of membrane, prolonged labour, repeated internal examination in labour, trial of labour at home invites bacterial invasion and increases the chance of wound infection. Six factors significantly associated with wound infection, which were identified by univariate analysis, were put into multiple logistic regression for further analysis. After analyzing and stepwise adjustment certain factors like Type of surgery, nature of surgery, anaemia, PROM, obesity, and diabetes were most significant factors in the present study as compared to others (p=0.000). This study also found, the occurrence of post-operative wound infection was more in multiparous women (70) than in primiparous (47) and possibly malnutrition and anaemia due to repeated childbirth acted as the predisposing factors. Another author mentioned similar picture Jahanara Rahman et al.7 This study shows 21.13% of the populations were anaemic, though severe and moderate anaemia was found in a negligible number of the patients. There was a strong relationship between anaemia and wound infection (P=0.000) in our study as was found by Zaman F (2011)8 in her study. Diabetes was found in 8.45% of patients who underwent surgery which is found to be statistically significant when compared in univariate analysis which is quite comparable with the Dhaka study group.7
The study showed the appearance of infection between 6 and 10 post-operative days in more than half of the population. Similar result (8±2 day post operatively) was found in a study by Matin ASMR (1981)12.9 Haddad V and Macon WLN (1980)10 showed in their studies that the occurrence of wound infection was on an average of 6.8 post-operative days which was also similar to that of ours(5.33-6.33).The time of appearance of wound infection in majority of the cases (6 to10 days) indicates that the source of infection was not from the operation theatre, rather from patients’ surroundings like, patients’ ward, attendance etc. Escherichia coli is the most
common cause of SSI, accounting for 36.62% of cases. It originates from fecal flora that colonize the periurethral area (ascending infection). Klebsiella (6.10%) and pseudomonas (6.57%) species cause most of the remaining cases. Gram-positive organisms, particularly Staph. aureus, are also clinically important pathogens, contributing 4.69% of the infections. Urea-splitting bacteria including Proteus, Klebsiella, Pseudomonas, and coagulase negative Staphylococcus alkalinize the urine and may be associated. S. aureus from the exogenous environment or the patient's skin flora is the usual pathogen, whereas, in other categories of surgical procedures, the polymicrobial flora closely resembling the normal endogenous microflora of the surgically resected organ are the most frequently isolated pathogens (Nichols, 1991)11 (Wassef et al)12.
Only single strain of MRSA was found in the study. This study correlates with the study of Anila Ansar (2010-2012)13 and Wassef et al (2012)12. Once a diagnosis of wound infection has been confirmed and antibiotic sensitivities identified, appropriate management regimens should be considered, with a high priority given to reducing the risk of cross infection.
In present study the antibiotic sensitivity for all the organisms isolated by swab culture was studied and the drugs of choice for each organism were identified and given. It was observed that sensitivity for amoxyclav (39.44%) was found to be more. Other drugs found to be sensitive were gentamycin (20.66%) and cefotaxime (27.72%). Amikacin (10.80%) was sensitive commonly for grade IV and V.
It was observed that in grade I, II minor complications like fever is more common, while in grade III, IV and V major complications like gaping is more common.
Therefore, out of 213 patients of post operative wound infection,179(83.10%) patients of grade I, II and III were managed conservatively and surgical management was required in 34(16.90%) of grade III, IV and V.
In conservative management, we managed the wound with daily sterile povidone-iodine (Betadine) dressing along with antibiotic coverage and found it effective measure.
In surgical management, after obtaining swab culture for microorganisms and repeated daily dressings, secondary suturing was done. In secondary suturing refreshing of skin edges with excision of fibrosed granulation tissue was done after achieving haemostasis.
Thus conservative treatment was common mode of treatment as compare to surgical treatment in our study.
(36.75 days) as compare to grade IV (29.90), III (22.40), II (12.80) and I (11.53 days.) according to Southampton Wound Grading System.
CONCLUSION
Surgical site infections determine the final outcome of an operation apart from the morbidity and mortality they cause. Though surgical care is very important to prevent wound infection, but some pre and post operative steps surgical operation, as infection in a post operative wound increases the length of stay in the hospital. The cost of antibiotics, and increased duration of antibiotic therapy further adds on to the cost of treatment. If we can eradicate anaemia in pregnancy, control diabetes, avoid prolonged labour, use potent antibiotics in cases of rupture of membrane, do timely intervention, provide well equipped obstetrics ward with clean environment, then incidence of wound infection can be lowered. The merit of the study was to start the active surveillance of surgical site infections based on standard definitions and methods to be maintained by cooperation of infection control practitioners and surgical team. Identification of risk factors for surgical site infections has encouraged the development of recommendations for prevention of SSI in order to achieve the setting goal to reduce the SSI.
Funding: None
Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethical Committee
REFERENCES
1. Myles TD, Gooch J, Santolaya J. Obesity as an independent risk factor for infectious morbidity in patients who undergo cesarean delivery. Obstet Gynecol 2002; 100:959–964.
2. Naumann RW, Hauth JC, Owen J, et al. Subcutaneous tissue approximation in relation to wound disruption after caesarean delivery in obese women. Obstet Gynecol 1995;85:412–416.
3. Chelmow D, Huang E, Strohbehn K. Closure of the subcutaneous dead space and wound disruption after
cesarean delivery. J Matern Fetal Neonatal Med 2002;11:403–408.
4. Owens WD, Felts JA, Spitznagel EL. ASA physical status classifications: A study of consistency of ratings. Anesthesiology 1978; 49: 239-243.
5. Bailey IS, Karran SE, Toyn K, Brough P, Ranaboldo C, Karran SJ. Community surveillance of complications after hernia surgery. BMJ 1992: 304(6825): 469-71.
6. Mishriki SF, Law DJ, Jeffery PJ. Factors affecting the incidence of postoperative wound infection. J Hosp Infect. 1990 Oct; 16(3):223-30.
7. Rahman Jahanara, Sultana Nasreen, Hasan Munir, Begum Hosne Ara, Factors of post-operative wound infections in abdominal surgeries of Obstetrics and Gynaecology, Dept; Journal of Dhaka Medical College Hos. 2011;18(01):39-42.
8. Zaman F. Profile of wound infection following caesarean section delivery at Institute of Child & Mother health, Matuail, Dhaka. (Dissertation), Bangladesh College of Physicians and Surgeons, 2011.
9. Matin ASMR. Wound Infection in Planned Abdominal Surgery. (Dissertation), Bangladesh College of Physicians and Surgeons, 1981.
10. Haddad V, Macon WLN. Abdominal Wound Dehiscence and Evisceration: Contributing factors and improved mortality, Br J Surg. 1980;16:508-13. 11. Nichols. Ronald Lee, Elsevier B.V., Nosocomial
infections, Cross infection American Journal of Medicine, Health care industry 0002-9343, 1991. 12. Wassef MA, Hussein A., Abdul Rahman E. M., and
El-Sherif RH. A prospective surveillance of surgical site infections: Study for efficacy of preoperative antibiotic prophylaxis; African Journal of Microbiology Research Vol. 6(12), pp. 3072-3078, 30 March, 2012.
13. Ansar Anila, Surgical Site Infection in Obstetrics Practice, Department of Obstetrics and Gynaecology, Islam Teaching Hospital Sialkot, from September 2010 to October 2012; Journal of Surgery Pakistan (International) 18 (2) April - June 2013;68-73.
14. Bowler P, Duerden B, Armstrong D. Wound microbiology and associated approaches to wound management. Clin Microbiol Rev 2001; 14(2): 244-69.
15. Kothuis BJ. The effect of povidone-iodine on postoperative wound infection in abdominal surgery. Neth J Surg 1981;33(4):186-9.
DOI: 10.5455/2320-1770.ijrcog20131228