Sadik Taju, Workayehu Kebede. Ethiop Med J, 2017, Vol 56, No. 1 ORIGINAL ARTICLE
CAUSES OF CRANIAL NERVES III, IV AND VI PARALYSIS AMONG ETHIOPIAN
PATIENTS PRESENTED AT MENELIK II HOSPITAL
Sadik Taju, MD1, Workayehu Kebede, MD2
ABSTRACT
Introduction: Causes and clinical features of third, fourth and sixth cranial nerve palsy showed variation among previous studies and cases were analyzed regarding final causal diagnosis.
Method: A cross sectional study was performed among112 patients with third, fourth, and sixth nerve palsy who
were consecutively seen at the neuro-ophthalmic clinic of the Ophthalmology Department of Menelik II Hospital. Data was collected prospectively and the etiology and results of ocular examination on each visit were reviewed. A multivariate logistic regression analysis using SPSS version 17.0 was performed to identify independent factors associated with the etiology.
Results: The sixth cranial nerve was affected most frequently (n=60 (53.6%) and head trauma (n=48 (42.9%) was
the most common etiology. The mean age at presentation was 34.3 (± 2.54) years. Involvement of the left eye (p= 0.010) and head trauma (p=0.02) as the etiology were statistically significantly associated with sixth nerve cranial palsy.
Conclusion: Sixth cranial nerve is the commonest affected nerve and head trauma is the main cause of cranial nerve paralysis.
Keywords: cranial nerve; palsy; clinical features, Menelik II; Ethiopia
1
Addis Ababa University, College of Health Science, Department of Ophthalmology * Corresponding author: [email protected]
INTRODUCTION
Oculomotor (cranial nerve III), trochlear (cranial nerve IV) and abducens (cranial nerve VI) contain the lower motor neuron, which innervates the six extra ocular and levator palpebral muscles. The coor-dinated activities of the extra-ocular muscles produce the normal conjugate movement of the eyes; the con-traction of the levator palpebral muscles elevates the eye lids (1,2).
A palsy of any one of three motor cranial nerves (CNs) presents with double vision, droopy lid and, less frequently, awareness of an enlarged pupil or blurred monocular vision at near range (3). Most studies reviewing the causes of oculomotor nerve palsies do not distinguish isolated from non-isolated palsies, nor do they list causes by location. A large number of cases is recorded as “undetermined” cause and, still a larger proportion of presumed ischemic origin, remains of uncertain location (3,4).
Some of the best information regarding the incidence of acquired fourth nerve palsy can be found in the Mayo Clinic series (5). In the most recent series, the etiology remained undetermined in 26% of the cases, and was due to head trauma in 20%, vascular in 17%, neoplastic in 14%, aneurysm in 7%, and other sources in 15%. These series are not typical of a gen-eral ophthalmology experience, because they re-viewed cases treated at a large referral center by oph-thalmologists, neurologists, and neurosurgeons. Nev-ertheless, the scope of these series provides impor-tant data on the etiology and classification of CN palsies (6,7).
The study on the causes of paralysis involving the third nerve involving 290 cases by Rush and Young in 1981 showed a large number of cases had no iden-tifiable causes. Among those with known associated diseases 60 had vascular disorders, of which 25 had diabetes mellitus, 22 had hypertension, and 10 had atherosclerosis compared with Rucker’s report where only minor differences were noted (3,8).
patients showed that sixth nerve palsy was the lead-ing cause of cranial nerve paralysis. But due to lack diagnostic instruments like computerized tomogra-phy (CT) and magnetic resonance imaging (MRI), the etiology was not determined in 22% of the case (unpublished). Available evidence shows that the clinical features of cranial nerve palsy vary and analysis of the underlying causes is limited. The pur-pose of this study was to determine the causes of paralysis of cranial nerves III, IV and VI among Ethiopian patients seen at a hospital in Addis Ababa.
PATIENTS AND METHODS
A cross sectional study with prospective data collec-tion was conducted among all consecutively seen outpatients that were referred by ophthalmologists practicing primary health facilities to the neuro-ophthalmic clinic at ophthalmology Department of Menelik II Hospital with cranial nerves III, IV and VI palsy during the period February 2013 to May 2014. A data collection form was developed consist-ing patient’s socio-demographic characteris2tics, type and duration of onset of complaints, and previ-ous medical history. The degree of ocular motor re-striction in the worst motion direction, the deviation angle at each visit, the presence of other related oph-thalmic or neurological signs, and the results of sero-logic, hematologic and neuroradiological tests were recorded.
Deviation angle was measured with the simultaneous prism and cover test in the primary position at dis-tance fixation. As in the Mayo Clinic series, cases were categorized into six etiological groups: vascu-lar, trauma, neoplasm, aneurysm, undetermined, or ‘other’ (1-3,8). Vascular cases were defined as hav-ing at least one vascular risk factor (diabetes, hyper-tension, ischemic heart disease, or peripheral vascu-lar disease) without trauma history or evidence of aneurysm or neoplasm on image studies. ‘Other’ or miscellaneous causes included complications of neu-rosurgical procedures and other systemic syndromes or diseases related to the cranial nerve function. Con-ditions that mimic cranial nerve palsy, such as myas-thenia gravis and thyroid orbitopathy were excluded from the study. For the cranial nerve IV palsy,
his-tory of head tilt dating back to infancy, definite facial asymmetry, amblyopia in the palsied eye, large verti-cal fusional amplitudes more than 10 prism dioptres (PD) were considered to be signs of congenital palsy. Data was checked for completeness edited, cleaned and entered into SPSS version 15.0 software for any association between baseline characteristics of the patients with types of cranial paralysis using either the X2 or Fisher Exact test and P-values below 0.05 were considered statistically significant.
Ethical clearance to conduct the study was obtained from Research and Publication Committee of Depart-ment of Ophthalmology, Medical Faculty Addis Ababa University. Similarly, verbal consent was ob-tained from each participant and subjects had the right to withdraw from the study at any time.
RESULTS
Of the 987 total neurophthalmic patients seen at dur-ing the study period 112 (11.6%) were found to have motor paralysis involving cranial nerves III, IV and VI in combined and isolated forms. A total of 112 patients were included in the study and all of them were Ethiopian and 61.1% of them came from the capital city, Addis Ababa. Sixty, 39 and two patients were found to have isolated cranial nerve III, IV and VI palsy, respectively, and the rest (11 patients) were found to have multiple cranial palsy of various com-bination. For the entire 112 patients, the average age of onset was 34.3 (±2.54) years and age ranged from 1 to 76 years. Sixty-one were men and 51 women. (Table 1).
Table 1. Distribution of age by sex of patients with paralysis of cranial nerves III, IV & VI seen at Menelik Hospital, February 2013 - May 2014
Table 2. Distribution of patients with cranial nerve III, IV and VI palsy by age, gender, laterality, time presentation time, and etiology, Menelik II Hospital, Feb 2013-May 2014.
Sex Total N (%)
Male Female
Age Group
<10 3 (4.9%) 5 (9.8%) 8 (7.2%)
11-20 16 (26.2%) 7 (13.7%) 23(20.5%)
21-30 9 (14.8%) 12 (23.5%) 21(18.8)
31-40 15 (24.6%) 10 (19.6%) 25(22.3%
41-50 6 (9.8%) 7 (13.7%) 13(11.6%)
51-60 5 (8.2%) 7 (13.7%) 12(10.7%)
>60 7 (11.5%) 3 (5.9%) 10(8.9%
Total 61 (100%) 51 (100%) 112(100%)
Socio demographic Variables Affected Cranial Nerve Total N (%)
Age Group
III IV VI Multiple
<10 2 2 3 1 8 (7.2
11-20 5 0 15 3 23(20.5)
21-30 5 0 14 2 21(18.8)
31-40 14 0 8 3 25(22.3)
41-50 3 0 9 1 13(11.6)
51-60 5 0 7 0 12(10.7)
>60 5 0 4 1 10 (8.8)
Sex
Male 21 0 33 7 61(54.5)
Female 18 2 27 4 51(45.5)
Laterality
LE 14 2 41 7 64(57.1)
RE 25 0 19 4 48(42.9)
Time
<4Wks 12 0 27 3 42 (37.5)
5-12Wks 8 0 15 0 23 (20.5)
13-24Wks 4 1 4 1 10 (8.9)
25-52Wks 6 1 5 6 18 (16.1)
>52Wks 9 0 9 1 19 (17)
Causes
Head Trauma 13 0 32 3 48 42.8)
Vascular 14 0 20 1 35 (31.3)
Neoplasm 2 0 3 3 8 (7.1)
Undetermined 3 0 3 1 7 (6.3)
Po. Com. A 1 0 0 0 1 (0.9)
Other 6 2 2 3 13 (11.6)
Total 39 2 60 11 112
Radio imaging was indicted for 73% of the patients; 22.3% of the patients didn’t afford to have this done. Among those who underwent neuroimaging investi-gation, different lesions were detected in 29% of the cases.
Cranial Nerve VI: Paralysis of the cranial nerve III was the most frequently, 60(53.6%), encountered palsy; left eye involvement seen in 41 patients. Thirty-three of the affected cases were males making male to female ratio of 1.2:1. The mean age was 33.3 (±2.89) years. One-half (28) of the patients presented with a compliant of in deviation of the eye while the next common compliant was diplopia. Seventy per-cent of the patients came within one three months
Figure 1: Distribution of age by cause among patients with cranial nerve VI palsy, Menelik II Hospital, Feb 2013-May 2014
Associated visual loss in the form of optic atrophy was found in four (6.7%) of the cases due to head trauma and neoplasm (lymphoma and metastatic breast cancer), two patients each. Forty-two (70%) of the patients with cranial nerve VI palsy presented within three months after the onset of the palsy. In-volvement of the left eye (p= 0.010) and head trauma (p=0.02) as an etiologic agent were statistically sig-nificantly associated with cranial nerve cranial VI palsy.
Cranial Nerve III: Thirty-nine (25 right and 14 left eyes) , (21 male and 18 female) patients had isolated cranial nerve III palsy. The mean age was 39.2 (±3.21) years. The most common presenting symp-tom was lid ptosis, seen in 22 (56.4%) of the pa-tients; 8 (20.5%) had out deviation of the eye. Other symptoms included diplopia and decreased vision. More than one-half (51.3%) of the patients presented
three months after the onset of symptoms. Clinical examination revealed that 61.5% of the patients had pupil involving cranial nerve III palsy, 58.3% of them in right eye and among 13 patients with trau-matic third nerve palsy 12(92.3%) had pupillary ab-normality. Complete paralysis of the cranial nerve III was present in 34 eyes (87.2%).
Neuroimaging (MRI or CT) was performed for 19 (48.7%) of the patients and revealed an abnormality in 10 (52.6%) of the cases, including aneurysms (one case), intracranial tumors (two cases), tuberculoma (three cases) increased intracranial pressure (two cases), subarachnoid hemorrhage (one) and one case of superior orbital wall fracture. For nine (23.1%) of the patients neuroimaging was considered but patient could not afford. The causes of paralysis in 39 pa-tients with cranial nerve III are given in Figure 2.
Fourteen 35.9%) of cases had vascular disorders; seven of them had diabetes mellitus, four had hyper-tension and two had both diabetes and hyperhyper-tension. All of the patients presented with isolated cranial nerve III palsy secondary to diabetes were identified during evaluation and all of them were having pupil sparing cranial nerve palsy. Only two patients secon-dary to hypertension of vascular cause had pupil in-volving palsy. Trauma was the second leading cause accounting for 33.3% and out of 13 cases 11 were due to car accident and eight of them were in the age range of 20-40 years. Posterior communicating artery aneurysm was seen only in one of the patient.
Fourth Cranial Nerve: Two female patients below the age of 10 years with isolated cranial nerve IV palsy were seen in the study. One patient presented with face turn while the other one came with poor vision. Congenital cranial IV palsy was considered in both of the patients.
Combined cranial nerves III, IV and VI: Eleven patients with multiple cranial palsy were seen during the study period. The mean age was 28.3 (±2.67)
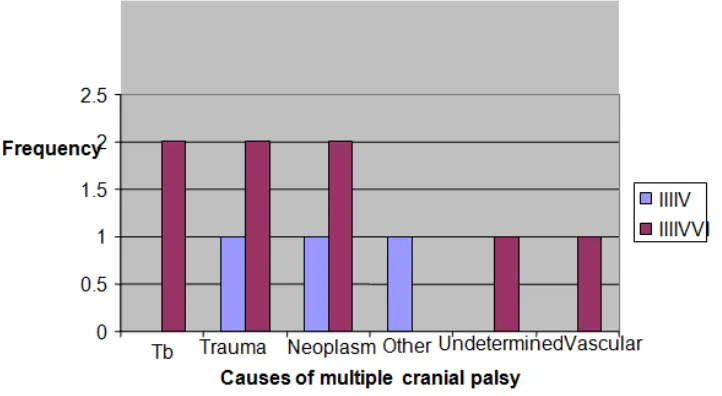
years of age and seven of them were males. Five of the patient complained droopy lid and seven patients (63.6%) came after six months of onset of the com-pliant. Only four (33.6%) of the patients came within here months after the onset of palsy. There were eight patients, (72.7%), with combined cranial nerve III, IV and VI paralysis and the rest three presented with combined cranial nerves III and IV palsy. Infrat-entorial neoplasm was the most frequent cause (Figure 3). Seven of the patients with combined cra-nial nerves III, IV and VI palsy affected the left eye. Metastatic tumors (lymphoma, nasophryngeal carci-noma) and arachdonic cyst were the causes in 3 of 11 cases and car accidents in 3/11 cases, respectively. Four patients had a variety of causes including tuber-culoma (two) and raised intracranial pressure from HIV encephalitis and one patient with superior or-bital fissure syndrome. Nine patients (81.8%) with acquired multiple cranial nerve palsy had docu-mented neuroimaging (either CT or MRI). Visual loss was observed in six cases due to optic atrophy secondary to increased intracranial pressure.
Figure 3. Type of multiple cranial palsy by causes among patients seen at Menelik II Hospital, Feb 2013 - May 2014
DISCUSSION
This is the first study (cross sectional) with prospec-tive data collection from Ethiopian patients with cra-nial nerve paralysis. Compared with reports by Rucker (1956), Rucker (1963) and Rush and Younge (1981), which involved retrospective data in some
Cranial nerve VI was affected frequently in our se-ries, which is comparable with that reported by the other studies. (6-8). The commonest cause for cranial nerve VI palsy among those less than twenty years of age was head trauma, 14/18 (77.8%), but Lee MS et al. reported neoplasm as the leading etiology (45%) of cranial nerve VI paralysis in this age group (9). Among adults between 15 to 50 years of age trauma remains the most frequent (45%) of the causes. In contrast, Moster ML, et al. in a cross sectional study with prospective data collection, reported vasculopa-thy as the most common cause of cranial nerve VI palsy in this age group (10). Similar to the pediatric age group, in our series, head trauma is the leading causes of cranial nerve VI palsy in the whole age group, but Rush et al. reported undetermined causes top on the list whereas Park UC. reported vascular causes as the major underlining etiology of cranial nerve VI palsy (8,11,12). In contrast, Peter J. et al. reported neoplasm as the leading cause of paralysis of cranial nerve VI (13).
Generally, the trend in the cause of cranial nerve VI palsy shifted from undermined causes in the Mayo Clinic series from the 1950’s to 1980’s, to the recent studies, where vascular disorder is becoming the commonest disorder. The possible reasons for the largest undermined causes in the earlier time could be lack of investigative modalities like CT/MRI. In our series, head trauma was common and this could be due to the prevailing figure of the youngest seg-ment of cases as compared to other studies. In our study, the cranial nerve III was the next most com-monly involved affected 39 (34.8%). This is compa-rable to a magnitude of 23.3% to 36% reported be-fore (6,7,8,12), and there was no cranial nerve III palsy with bilateral involvement. Blepharoptosis was observed in 87.2% of the patients with cranial nerve III paralysis, which is com-parable to the percentage (89.3%) quoted by Tabassi AR (14),
Pupilary involvement in cranial nerve III palsy in our study of 61.5% was higher than a report from Farabi Eye Hospital in Tehran, Iran during 2001-2002, which was 50% (14). Among our patients with cra-nial nerve III palsy associated with diabetes mellitus, there was no case of pupillary involvement, which is different result from 38% reported by Daniel M. (15). The possible reason for a relatively higher fig-ure of pupillary involvement in cranial nerve III pa-ralysis in our series could be due to high prevalence of trauma as the etiologic cause, while vascular causes were the commonest from Tabassi AR’s re-port. The majority causes of cranial nerve III palsy due to vascular causes are pupil sparing. As to the etiology of cranial nerve III palsy, undetermined
causes were the commonest cause from the earlier reports by Rucker and Rush, ranging from 23.1% to-25.6%. Previous reports, including report from Ethio-pia and India have shown that an undetermined etiol-ogy of cranial nerve palsy was in the order of 18%-30% (6-8,11). Whereas in our study we have seen vascular pathologies constituting 35.9% of causes of cranial nerve III palsy, which concurs the range re-ported by others: 34.9% from Kyoto Hospital, Japan (16), 35.4% from Korea (11)and 42.8% from Farabi Eye Hospital, Tehran, Iran (14).
Of the 39 patients with third nerve palsy in our study around 27(70%) of them were above the age of 40 years and vascular disorders were re common in this age group. Several studies, performed over the last four decades, reported cranial nerve IV palsy was less common than oculomotor or abducens palsies (6,7,8,11). We have seen similar trend in our series (1.8%). The highest prevalence of cranial nerve IV palsy was reported by Park UC. from Seoul National University of 22.3% (12).
Multiple cranial nerve palsies accounted for 9.8% of all cases. This figure is comparable with that reported by Rush (8),Rucker (2), 11.9% and 12.7%, respec-tively. It was however lower than that reported by Menon V and Rucker, 17.3% and 18.9%, respec-tively (2,11).The frequency of combined cranial nerves III, IV and VI palsy is higher as compared to a report by Rush (45.4%). Neoplasm(3), head trauma (3) and CNS tuberculosis (2) were the leading causes of multiple cranial palsy in our series is in agreement with other earlier reports by Rush (8) and Menon V. (11).
REFERENCES
1. M. J. G. Harrison .Contemporary Neurology. Third edition .1983.Butter Worth
2. Jack J. Kanski. Clinical ophthalmology a systemic Approach. Fifth edition 2003 Butter Worth -Heinmsnn pub-lisher chapter 18: 631-8.
3. Duane TD Neuro ophthalmology. Cranial nerve palsies. Chapter 19. Vol. 2. revised edition.1990. Lippincott Williams & Wilkims co. Philadelphia.
4. Reinecke RD and Mansour AM. Central Trochlear palsy A review survey. Ophthalmol. 1986;30:279-97. 5. Balkan R and Hoyt CS. Associated neurologic abnormalities in congenital III nerve palsy. AJO 1984;97:315-9 6. Rucker CW. Paralysis of the third, fourth, and sixth cranial nerves. Am J Ophthalmol 1958; 46:787–94. 7. Rucker CW. The causes of paralysis of the third, fourth, and sixth cranial nerves. Am J Ophthalmol 1966;
61:1293–298.
8. Rush JA and Younge BR. Paralysis of cranial nerves III, IV and IV cause and prognosis in 1000 cases. Arch Ophthalmol. 1981: 99:76-9.
9. Lee MS, Galetta SL, Volpe NJ, Liu GT. Sixth nerve palsies in children. Pediatr Neurol 1999; 20:49-52. 10. Moster ML, Savino PJ, Sergott RC, Bosley TM, Schatz NJ. Isolated sixth-nerve palsies in younger adults.
Arch Ophthalmol 1984; 102: 1328–30.
11. Menon V, Singh J, Prakash P. Aetiological patterns of ocular motor nerve palsies. Indian J Ophthalmol 1984;32:447-53
12. U-C Park, S-J Kim, J-M Hwang and YS Yu. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye 2008;22,691–6.
13. Peter JS; Jan K.; Gary H. Norman J. Schatz. Chronic Sixth Nerve Palsies Are They Really Harbingers of Seri-ous Intracranial Disease? Arch Ophthalmol 1982; 100:1442-4.
14. Tabbasi AB, Dehghani AL. Etiology of Oculomotor Nerve Paralysis . J Ophthalmic Vis Res. 2006;1:1. 15. Daniel M., Jacobson. Pupil Involvement in Patients With Diabetes-Associated Oculomotor Nerve Palsy Arch
Ophthalmol. 1998;116(6):723-727. doi:10.1001/archopht.116.6.723