Anna Sadakierska-Chudy
1, Jan Skóra
2, Piotr Barć
2, Dagmara Baczyńska
3,
Urszula Kasprzykowska
4, Artur Pupka
2, Marek Ussowicz
5, Piotr Szyber
2,
Tadeusz Dobosz
1Angiogenic Therapy for Critical Lower Limb Ischemia
Angiogenna terapia w leczeniu krytycznego niedokrwienia
kończyn dolnych
1 Molecular Techniques Unit, Department of Forensic Medicine, Wroclaw Medical University, Poland 2 Department and Clinic of General and Vascular Surgery and Transplantology, Wroclaw Medical University,
Poland
3 Institute of Biochemistry and Molecular Biology, Department of Cell Pathology, Wroclaw Medical University,
Poland
4 Department of Microbiology, Wroclaw Medical University, Poland
5 Department of Pediatric Bone Marrow Transplantation, Oncology, and Hematology, Wroclaw Medical
University, Poland
Abstract
Background. In several preclinical and clinical studies, VEGF gene therapy has proven successful in the treatment of critical limb ischemia (CLI). CLI is estimated to develop in 500–1000 individuals/million/year. It is a severe disease associated with a high risk of amputation and mortality. Therapeutic angiogenesis is a novel concept con-sisting of the use of proangiogenic growth factors to promote collateral artery development in ischemic tissues. To test a potential clinical application of this method, the authors prepared a nonviral expression vector encoding VEGF165 protein.
Objectives. The purpose of this study was to construct a functional expression vector encoding isoform VEGF165
which can be used for therapeutic angiogenesis in no-option patients with critical limb ischemia.
Material and Methods. Total RNA was extracted from vein and RT-PCR was used to prepare a cDNA sequence for cloning into the plasmid vector. The naked pcDNA3/VEGF165 plasmid was administered alone (group I) or
combined with mononuclear cells (group II) directly into the skeletal muscle of the ischemic lower limb.The vec-tor’s ability of expression in mammalian cells, clinical outcome, serum level of VEGF protein, and endothelial cell proliferation in muscle tissue were evaluated.
Results. pcDNA3/VEGF165 was expressed in transfected CHOPro5 cells. Due to the gene transfer, 9 of 24 patients
did not require amputation. A higher serum VEGF concentration was observed than in healthy controls and the level of cytokine increased on day 14 and decreased on day 90 after plasmid administration. Histological and immunohistochemical analysis of the muscles derived from amputated limbs revealed the presence of VEGF pro-tein and signs of new blood vessel formation.
Conclusions. This therapy is safe, but a single intramuscular gene transfer of VEGF165 is insufficient to promote
angiogenesis efficiently. Better results were observed when combined therapy was used (Adv Clin Exp Med 2010, 19, 3, 347–359).
Key words: angiogenic cytokine, isoform VEGF165, expression vector, gene transfer, critical lower limb ischemia.
Streszczenie
Wprowadzenie. Wiele badań przedklinicznych i klinicznych udowodniło, że terapia genowa z wykorzystaniem genu VEGF może być z powodzeniem stosowana w leczeniu krytycznego niedokrwienia kończyn. Szacuje się, że niedokrwienie kończyn rozwija się u 500–1000 osób na 1 milion w ciągu roku. Choroba niesie ze sobą duże ryzy-ko amputacji i śmiertelności. Nowym sposobem leczenia może być terapeutyczna angiogeneza z wyryzy-korzystaniem proangiogennych czynników wzrostu, które pobudzają rozwój naczyń obocznych w niedokrwionej tkance. Aby zbadać możliwość klinicznego zastosowania tej metody, przygotowano niewirusowy wektor ekspresyjny kodujący białko VEGF165.
Adv Clin Exp Med 2010, 19, 3, 347–359 ISSN 1230-025X
ORIGINAL PAPERS
Critical limb ischemia (CLI) is estimated to develop in 500 to 1000 individuals per million per year [1]. Nowadays, chronic lower limb ischemia treatment is based on pharmacotherapy and inva-sive techniques. However, results from these tra-ditional treatment procedures are unsatisfactory, especially in severely ill patients suffering from critical ischemia. The latest scientific discoveries have brought about a completely new era of lower limb ischemia treatment. These new methods of treatment including modern stent construction, coating stents with substances attenuating epi-thelial hyperplasia and preventing restenosis, new drugs, and, raising the greatest hopes, using genes encoding proteins to affect disease process (gene therapy) and administering multipotential bone marrow cells (cell therapy) [2–8]. It seems that intramuscular injections of angiogenic cytokine genes may be a supplement or even an alterna-tive to conventional treatment. The purpose of the treatment is to induce collateral small blood ves-sel formation, which become bypasses around the blocked arteries [9–11].
Gene therapy, especially with the application of plasmids, has already received certain recog-nition around the world. A series of successful studies has been conducted, both on animals and in humans, most often with the use of vascular endothelial growth factor (VEGF) [12–14]. VEGF belongs to the VEGF/PDGF supergene family and is a key regulator of angiogenesis. VEGF increases vascular permeability and induces the migration and proliferation of endothelial cells [15]. The biological activities of VEGF are mediated by two endothelial cell-specific transmembrane receptors: VEGFR1, also known as Flt1 (fms-like tyrosine kinase receptor), and VEGFR2, also known KDR (kinase insert domain-containing receptor) [16].
VEGF exists in nine isoforms ranging from 121 to 206 amino acids due to alternative splicing [16]. VEGF165, the predominant isoform, is secreted,
but a significant fraction remains bound to the cell surface and ECM (extracellular matrix). This isoform is released in a diffusible form by heparin, heparinase, or by plasmin cleavage, which gener-ates a bioactive fragment [17]. VEGF165 has strong
biological potency and optimal characteristics of bioavailability.
Many studies indicated that the
administra-tion of VEGF165 significantly augments the
devel-opment of collateral vessels in animal models [17]. Nowadays, viral and non-viral systems for gene transfer are used for therapeutic angiogenesis. Viral systems are more effective than non-viral but they are less safe. Some kinds of viruses can inte-grate into the host cell genome and their insertion may lead to mutagenesis [18]. Moreover, viral vec-tors can initiate an immune response of patients, which leads to the elimination of therapeutic cells [19]. Non-viral gene transfer has several advantag-es over recombinant viral vectors. It is relatively non-immunogenic, non-infectious, can transfer a large DNA plasmid, and may be easily produced on a large scale. Non-viral delivery systems such as cationic liposomes, polymers, and naked DNA offer attractive alternatives in gene therapy. This therapy is safe, since after intramuscular or intra-venous injection, the gene locates to striated and non-striated muscles, where it can survive for up to 3 months, during which time it is responsible for promoting angiogenesis [12–14].
The aim of this study was to assess the expres-sion ability of pcDNA3/VEGF165 plasmid in mammalian cells, its clinical effects in patients with critical lower limb ischemia, and the safety of gene therapy.
Cel pracy. Konstrukcja funkcjonalnego wektora ekspresyjnego kodującego izoformę VEGF165, który mógłby być
wykorzystany w terapii angiogennej u pacjentów z krytycznym niedokrwieniem niemających innej możliwości leczenia.
Materiał i metody. RNA całkowite izolowano z żyły, sekwencję cDNA, którą wklonowano w wektor, przygoto-wano, wykorzystując reakcję RT-PCR. Bezpośrednio do mięśni szkieletowych niedokrwionej kończyny podawano albo nagi plazmid pcDNA3/VEGF165 (grupa I), albo komórki jednojądrzaste szpiku kostnego inkubowane z
pla-zmidem (grupa II). W tym badaniu autorzy oceniali zdolność wektora do ekspresji w komórkach ssaczych, wynik kliniczny, stężenie białka VEGF w surowicy oraz proliferację komórek śródbłonka w tkance mięśniowej.
Wyniki. Wykazano zdolność plazmidu pcDNA3/VEGF165 do ekspresji w transfekowanych komórkach jajnika
cho-mika chińskiego (CHOPro5). Po podaniu genu lub genu i komórek szpiku 9 z 24 pacjentów nie wymagało ampu-tacji. Zaobserwowano większe stężenie cytokiny VEGF w surowicy u pacjentów z niedokrwieniem w porównaniu z osobami zdrowymi z grupy kontrolnej, stężenie zwiększyło się w 14. dniu, a zmniejszyło się w 90. dniu po zastoso-waniu terapii. Badanie histologiczne i immnohistochemiczne mięśni z amputowanych kończyn wykazało obecność białka VEGF i ślady tworzenia nowych naczyń krwionośnych.
Wnioski. Przeprowadzone badanie wykazało, że terapia jest bezpieczna, pojedynczy domięśniowy transfer genu
VEGF165 okazał się jednak niewystarczający do wydajnego pobudzenia angiogenezy. Lepsze wyniki uzyskano, gdy
zastosowano terapię łączoną (Adv Clin Exp Med 2010, 19, 3, 347–359).
Słowa kluczowe: cytokina angiogenna, izoforma VEGF165, wektor ekspresyjny, transfer genu, krytyczne
Material and Methods
RT-PCR
RT-PCR was used to prepare VEGF165 cDNA
and total RNA was extracted from vein based on the Chomczynski method [20]. For the reverse-transcriptase (RT) reaction, 5 μl of RNA template was used for cDNA synthesis with oligo(dT) primer using the Super-ScriptTMIII First-Strand Synthesis
System for RT-PCR (Invitrogen, USA). cDNA was
amplified with specific primers for VEGF carrying
the HindIII and EcoRI restriction sites (Table 1).
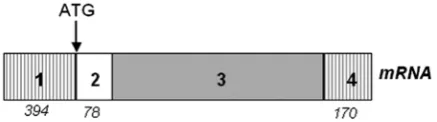
This VEGF fragment has an included 5’-UTR
with IRES sequence and protein leader sequence (to allow efficient translation and active secretion from intact cells), the exon sequences, and also part of the 3’-UTR region (Fig. 1).
A proofreading AccuPrimeTM Pfx DNA
Polymerase (Invitrogen, USA) was used for the PCR. The cDNA sequence is available at GenBank with accession number NM_003376. The primers
of the housekeeping gene GAPDH were used as
a positive control in RT-PCR (Table 1).
Cloning and Preparation
of Plasmid DNA
The PCR products were digested with HindIII
and EcoRI restriction enzymes, then purified using
a SpinPrepTM Clean-Up Kit (Novagen, USA). The
resultant products were ligated with the pcDNA3 plasmid (Invitrogen) in the presence of T4 Ligase (Amersham, U.K.). This is a simple eukaryotic expression vector which contains an MCS site (multiple cloning site), a strong CMV promoter, and other elements for efficient expression in mammalian cells. The recombinant plasmid was
named pcDNA3/VEGF165.
Viable E. coli DH5alpha cells were
trans-formed using the ligation mixture and the bac-teria were inoculated on LB medium containing ampicillin (100 μg/ml). To select the appropriate
plasmid containing the VEGF165 isoform, plasmid
DNA from ampicillin-resistant clones were iso-lated using a QIAGEN Plasmid Mini Kit (Qiagen, Germany) and cut by HindIII and EcoRI restriction
enzymes to confirm the insert sequence of VEGF165
gene. The digestion products were separated by electrophoresis on 1% agarose gel with ethidium bromide (0.5 μg/ml). It was also sequenced with T7 and Sp6 primers in an ABI Prism 310 genetic analyzer (Applied Biosystems).
Table 1. Nucleotide primer sequences used for the RT-PCR, sequencing and expression detection
Tabela 1. Sekwencja nukleotydowa starterów użytych do reakcji RT-PCR, sekwencjonowania i wykrywania ekspresji Gene
(Gen) Sequence 5’ → 3’ (Sekwencja 5’ → 3’) PCR product size (Wielkość produktu PCR) Aim (Cel) VEGF_F
VEGF_R GACGHind III AAGCTTCGTCGCACTGAAACTTTTCGT GACGAATTCGCAGAGTCTCCTCTTCCTTCA
Eco RI
VEGF121 – 1024 bp
VEGF145 – 1096 bp
VEGF165 – 1156 bp
VEGF189 – 1228 bp
insert amplification
GAPDH_F
GAPDH_R TGAAGGTCGGAGTCAACGGATTTGGT CATGTGGGCCATGAGGTCCACCAC 983 bp RT-PCR positive con-trol T7
Sp6 AATACGACTCACTATAGGGA GCATTTAGGTGACACTATAG VEGF165 – 1249 bp sequencing VEGF _F
Sp6 GACGHind III AAGCTTCGTCGCACTGAAACTTTTCGT GCATTTAGGTGACACTATAG
VEGF165 – 1233 bp expression detection
Fig. 1. Structure of the cloning mRNA VEGF frag-ment. (1) 5’-untranslated region (5’-UTR) contains the IRES sequence, (2) leader protein sequence, (3) exon sequences, (4) 3’-untranslated region (3’-UTR), ATG – start codon. Numbers below mRNA structure are the numbers of base pairs
Ryc. 1. Struktura wklonowanego fragmentu mRNA
Large-Scale Preparation
of Plasmid
Plasmid was prepared on a large scale from cultures of pcDNA3/VEGF165-transformed E. coli
DH5alpha according to the instructions of the EndoFree Plasmid Mega Kit (QIAGEN, Germany). Briefly, after cell lysis the plasmid DNA was pre-cipitated by addition of isopropanol, washed with 70% ethanol, and air dried. The purified plasmid DNA was dissolved in sterile water, stored in vials, and pooled for quality control (absorbance at wave-lengths of 260 and 280 nm to document a ratio between 1.70 and 1.75, a limulus amebocyte lysate (LAL) using a Pyrochrome Chromogenic Test Kit (Charles River)for the detection and quantification of bacterial endotoxin levels, microbial cultures, and agarose gel electrophoresis with ethidium bro-mide to confirm that the nucleic acid was in closed circular supercoiled form). The LAL test was per-formed at the Medical Microbiology Laboratory, Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, Wroclaw.
In vitro
Transfection
and Expression VEGF
165Chinese Hamster Ovary cells (CHOPro5) were cultured on OPTI-Mem (Gibco BRL) con-taining 10% bovine serum (Gibco BRL) and 2 mM glutamine (Gibco BRL). Transfection of CHO cells
with pcDNA3/VEGF165 was performed in
serum-free medium using LipofectamineTM 2000 (Roche)
according to the manufacturer’s protocol. To con-firm the expression of VEGF165, 72-h CHOPro5
cells were harvested and total RNA was extracted using an RNA Easy Midi Kit (Qiagen, Germany).
The presence of pcDNA3/VEGF165 transcript of
transgene was evaluated by RT-PCR assay with
sense VEGF165 primer within cDNAand antisense
Sp6 promoter primer within the pcDNA3 vec-tor (Table 1). The primers of the housekeeping gene GAPDH were used as a positive control in RT-PCR.
Preparation of Bone Marrow
Mononuclear Cells
Bone marrow was harvested by multiple aspi-ration from iliac crests under general anesthe-sia using a bone marrow collection set (Baxter). Mononuclear cells were separated from the har-vested marrow with an albumin-primed blood cell separator (Baxter Fenwall CS 3000 plus) according to the manufacturer’s protocol. The final volume
of the mononuclear cell concentrate was 120 ml. The CD34+ cell content was determined by flow cytometry according to ISHAGE recommenda-tions. The median final number of prepared mono-nuclear cells was 1.58×109 (range: 0.77–3.83×109).
The median number of collected CD34+ cells was 1.7×107 (range: 0.12–4.25×107).
Patients
Twenty-four patients with critical ischemia of the lower limb due to atherosclerosis obliterans were enrolled in the clinical study and randomized into groups according to the method of treatment. Of the 24 patients, 12 were treated using gene trans-fer only (group I) and 12 received stem cells and recombined plasmid (group II). Group I consisted of 3 women and 9 men, age range 32–78 years, and group II 4 women and 8 men, age range 31–53 years. Fourteen patients had a history of unsatis-factory peripheral femoropopliteal by-pass; in 8 cases the procedure was carried out twice. Six patients had undergone a failed endovascular pro-cedure. In 2 cases both failed endovascular proce-dure and occlusion of femoropopliteal by-pass was recorded. Only 2 patients did not have any history of vascular surgery or endovascular intervention. All patients were qualified for thigh-level lower limb amputation on the grounds of poor clinical state (non-healing ischemic ulcers in 17 and gan-grene in 7 limbs) before joining the study. Patient assessment included evaluation of clinical state of the ischemic limb, pain intensity, ankle-brachial index (ABI), and VEGF cytokine blood concentra-tion level. CT-angiography was performed before and after a three-month follow-up study in all participating patients. Patients with proliferative retinopathy, evidence or history of malignancy, unstable angina pectoris, terminal renal failure, advanced hepatic dysfunction, anemia, tuberculo-sis, diabetes mellitus, or other severe diseases were excluded. Written informed consent was obtained from all patients. The Study Protocol was approved by the Ethics Committee of the Wroclaw Medical University, approval No. KB-926/2003.
Intramuscular Injection
of pcDNA3/VEGF
165injections were performed using 12-gauge needles, without local anesthesia. After the injections, the patients were observed to check for any immediate adverse reactions.
Intramuscular Injection
of Mononuclear Cells
and pcDNA3/VEGF
165The mononuclear cells were incubated with
pcDNA3/VEGF165 for two hours and then the
concentrate was injected intramuscularly into the ischemic lower limb below the knee level. The injection sites to the calf muscles were based on a previous study of the present authors and litera-ture data [1, 21]. The volume of each injection was 1.5 ml (approximately 80 injections to calf mus-cles, each 2 cm deep). The time of the injections did not exceed 7 hours after bone marrow harvest-ing because the intention was to eliminate possible loss of stem cells caused by extracorporeal stor-age of bone marrow cells and to avoid prolonged exposure of plasmid to enzymatic degradation by nucleases from monocytes present in the mono-nuclear cell solution.
Serum VEGF Concentration
Serum VEGF concentrations were measured at baseline and 7, 14, 28, and 90 days after the
pcDNA3/VEGF165 plasmid injection. Samples were
collected in sodium citratetubes and centrifuged
and the serum was stored at –20oC until analysis.
The serum VEGFconcentration was determined
by ELISA using a kit from R&D Systems accord-ing to the manufacturer’s protocol.
Muscle Samples
The muscle specimens near the site of gene injection were retrieved from amputation limbs. Tissue fragments were fixed and assessed at the Wroclaw Medical University Anatomical Pathology Institute. Biopsy specimens were evalu-ated histologically (hematoxylin and eosin stain), and immunohistochemically in order to reveal factor VII and VEGF.
Statistical Analysis
All data are expressed as the mean ± SD and the data were analyzed by the Wilcoxon test and the Friedman test was used for comparisons between groups. A P value of less than 0.05 was considered statistically significant.
Results
Transformant Selection
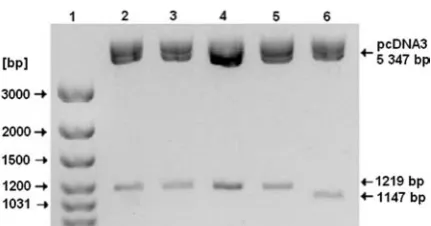
The digestion analysis of the obtained five clones revealed the 165- and 189-amino-acid
iso-forms of VEGF gene (Fig. 2). As sequencing
analy-sis also confirmed the presence of these isoforms,
the VEGF165 isoform was chosen for further study
due to its strong proangiogenic potential.
Expression of VEGF Gene
in CHOPro5 Cells
RT-PCR was performed to determine that CHOPro5 cells expressed the transgene. To show that the only product of the transgene would be
amplified, a sense primer within VEGF cDNA and
an antisense primer within the Sp6 promtor of pcDNA3 were used. A band of the predicted size of 1233 bp was present in the transfected CHO cells, but absent in the control cells (Fig. 3). This result
confirmed that the recombinantplasmid showed
the capacity to express VEGF165 gene.
Change in Clinical Status
The intramuscular injections of bone
mar-row mononuclear cells with pcDNA3/VEGF165
or pcDNA3/VEGF165 alone were well tolerated
by most patients. No major complications were noted; mild and transient limb edema occurred in 11 patients. The edema regressed in the course of a few days and did not require any medical Fig. 2. Electrophoretic separation of digestion plas-mids extracted from five transformant clones. Lane 1: GeneRuler TM100bp DNA ladder plus, lanes 2–5:
transformants containing isoform VEGF189, product
size: 1219 bp, lane 6: transformant contains isoform
VEGF165, product size: 1147 bp
Ryc. 2. Rozdział elektroforetyczny produktów trawienia plazmidów wyizolowanych z 5 transformantów. Ścieżka 1: standard wielkości GeneRuler TM100bp DNA ladder
plus, ścieżki 2–5: transformaty zawierające izoformę
VEGF189 – wielkość produktu 1219 pz, ścieżka 6:
intervention. Fever, leukocytosis, side effects, and other reactions were not observed in the patients during the course of the study. The therapeutic
benefit in the patients of group I (receiving naked plasmid) was demonstrated in 3 of the 12 (25%) patients by regression of resting pain in the isch-emic limb. These patients had ischisch-emic ulcers; after gene transfer their wounds were completely healed and limb amputation were not necessary (Figs. 4a-c). In the remaining 9 patients (75%) the results were not as satisfactory and all required surgical intervention; these patients underwent calf-level amputation. In this group, none of the patients „saved” their limbs longer than 3 months and necrotic foot lesions persisted as well as and lower limb ulcerations also showed no healing. During the study, 2 patients died; both belonged to the group in which plasmid administration did not improve clinical status and calf-level amputation was necessary. The first patient died of ischemic heart disease and the second patient’s death was due to sepsis and multi-organ failure in the course of massive ischemic lesions of the lower limb.
More satisfactory results were observed among the patients treated by combined therapy (cell and gene therapy). Limb amputation was performed in 6 patients because of advanced critical ischemia, with large ulceration or necrosis of the foot with severe wound infection. In the other 6 patients the therapy caused rest pain recession, and total healing of chronic foot ulcerations occurred up to Fig. 3. Agarose gel electrophoresis of VEGF165 product
separation from non- and transfected CHOPro5 cells. Lane 1: GeneRuler TM 100-bp DNA ladder plus; lanes 2–3:
NT – nontransfected cells (control), lanes 4–5: T – trans-fected cells. The product sizes expected for GAPDH and VEGF165 are 983 bp and 1233 bp, respectively
Ryc. 3. Elektroforeza na żelu agarozowym produk-tów PCR z transfekowanych i nietransfekowanych komórek CHOPro5. Ścieżka 1: standard wielkości GeneRuler TM100bp DNA ladder plus; ścieżki 2–3: NT
– komórki nietransfekowane (grupa kontrolna), ścieżki 4–5: T – komórki transfekowane. Oczekiwana wielkość produktów 983 pz i 1233 pz odpowiednio dla GAPDH i VEGF165
Fig. 4. Limb salvage in patent who underwent intra-muscular gene transfer of naked plasmid encoding VEGF165: (a) before treatment, (b) 6 weeks after gene
transfer, (c) 12 weeks after gene transfer
Ryc. 4. Ocalona kończyna u pacjenta po podaniu nag-iego plazmidu kodującego VEGF165: (a) przed
12 weeks after the administration of mononuclear cells with VEGF gene (Figs. 5a-d).
Change in the Ankle-Brachial
Index
The mean ankle-brachial index (ABI) increased in group I from 0.11 ± 0.05 at baseline to 0.16 ± 0.03 (in 3 cases with healed ulcerations) by day 30 after gene delivery. The ABI was 0.17 ± 0.02 on day 90, but the difference was not significant (P > 0.05). In group II, ABI increased significantly from 0.27 ± 0.20 before treatment to 0.41 ± 0.32 (P < 0.001) 4 weeks after bone marrow cell and gene administration. At the end of the study (i.e. after 3 months) the index increased significantly to 0.50 ± 0.22. The increase in ankle-brachial index was observed exclusively in 8 patients with com-pletely healed lower limb ulcerations or gangrene.
Blood Levels of VEGF
Mean blood concentrations of VEGF in the patients with critical lower limb ischemia were sig-nificantly higher than in the healthy controls. The serum level of VEGF protein in group I increased non-significantly 2 weeks after gene injection (P > 0.05). However, on day 90 the cytokine
concen-tration decreased and the differences between the 14th and 90th days were statistically significant (P
< 0.05). The increase in VEGF serum level from 238 ± 85 pg/l before treatment to 387 ± 76 pg/l on day 14 after stem-cell/gene injection was noted in group II, but it was statistically insignificant (P > 0.05). Moreover, on day 90 the concentration of the cytokine decreased and statistical analysis showed non-significant differences (P > 0.05) between day 14 and day 90. The serum level of VEGF increased slightly more 2 weeks after therapy in the patients with clinical status improvement than in the remaining patients. In these patients the level of the cytokine also decreased insignificantly on day 90. This trial demonstrated an increase in serum VEGF concentration between the 2nd and 4th weeks
of cell and/or gene therapy.
Histological,
Immunohistochemistry
Analysis
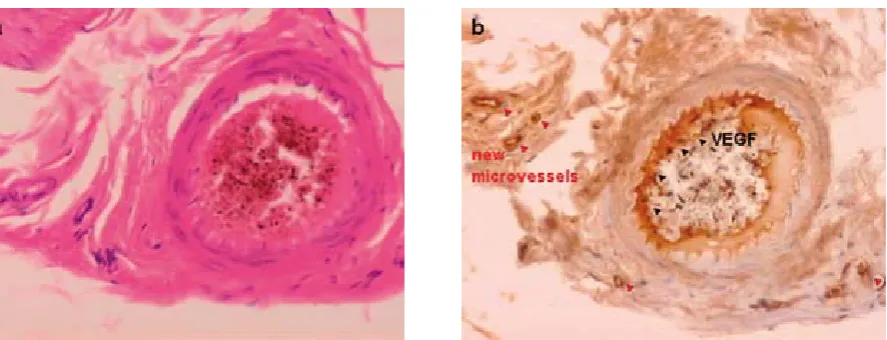
The 13 samples from amputated limbs were evaluated histologically and immunohistochemi-cally in order to visualize foci of endothelial cell proliferation, VEGF protein, and vascular net-works. The histological assay illustrated typical findings of microcirculation of muscle in critical
Fig. 5. Limb salvage in patent who underwent combine cell/gene transfer of naked plasmid encoding VEGF165: (a, b) before treatment,
(c, d) 3 months after therapy
Ryc. 5. Ocalona kończyna u pacjenta po podaniu jednojądrzastych komórek szpiku kostnego i nag-iego plazmidu kodującego VEGF165: (a, b) przed
limb ischemia. A number of capillaries, both arte-rial and venous, were occluded by partially recana-lized thrombus (Fig. 6).
Discussion
The present study describes the construction of a plasmid DNA expressing the 165-amino-acid isoform of VEGF and gene transfer into the isch-emic limb. It has been demonstrated that gene expression of VEGF is regulated at the level of mRNA stability and the 3’-UTR (untranslated region) has been identified as essential for
stabi-lization [16]. Furthermore, VEGF expression can
be regulated at the translation level; the 5’-UTR contains two internal ribosome entry sites (IRES) that initiate cap-independent translation and ensure efficient production of VEGF protein even under hypoxic conditions [22]. VEGF pro-tein required posttranslational modification, such as glycosylation into the endoplasmic reticulum (ER) [23]. The signal peptide is crucial for pro-tein translocation into the ER and also for suc-cessful secretion into the extracellular medium. It is well known that VEGF increases vascular permeability and is a specific angiogenic protein for endothelial cells [24, 25]. Transient edema in treated patients may suggest that VEGF can aug-ment vascular permeability [9, 26]. The cellular and molecular mechanism of VEGF-induced vascular permeability is not clear. Dvorak et al. found that vascular leakage could be attributed to transendothelial transport by means of a novel cytoplasmic organelle termed the vesicular-vacuolar organelle [27]. Another study reported VEGF-induced ultrastructural features consistent
with endothelial fenestration [28]. The vasodilat-ing effects of VEGF are stimulated for the release of nitric oxide and together with vasoactive metabolites released from ischemic tissues may participate in this effect [29–31].
The patients who received pCK-VEGF165 gene
transfer showed improvement in resting pain [32]. Other studies have demonstrated improvement in symptoms of sensory neuropathy in patients with PAD following intramuscular injection of
phVEGF165 [33, 34]. In the present study the ABI
increased after therapy to 0.17 and 0.50 in groups I and II, respectively. Specifically, the ankle-bra-chial index increased significantly in 8 patients (of group II) with successfully healed ulcerations. Unfortunately, at the same time no improvement was documented in 4 patients who required limb amputation. The stage of microcirculation dam-age in the affected limbs in these cases seemed to be too advanced to be improved by therapeutic angiogenesis induced by stem and gene therapy [21, 35].
Previous studies with phVEGF165 showed that
the ABI scores were 0.15, 0.14, and 0.19; the pres-ent study produced similar results [9, 26, 36]. The present study found no significant relationship between clinical outcome and ABI score. The ABI is probably not an optimal measurement reflect-ing physiological changes. This index is based on the blood pressure in the distal posterior and anterior tibial artery and an increased ABI reflects an improvement in the potency of inflow [37]. Increased vascularity was mainly caused by small side branches, most often proximal to the ankle level, and consequently less effective in terms of increasing ABI. In the future, transcutane-ous oxymetry or magnetic resonance perfusion Fig. 6. Thepresence of VEGF protein and angiogenesis in tissue specimens revealed by histology and immunohis-tochemistry staining: (a) capillary occluded by thrombus, (b) signs of VEGF protein and new microvessels
imaging might be more sensitive measurements. CT-angiography showed new collateral vessel for-mation; wider and more regular posterior tibial artery (PTA) were observed in this study than in the first examination.
Like other authors, the present authors found higher serum VEGF level in patients with criti-cal lower limb ischemia compared with healthy controls [15]. This situation seems to result from a considerably increased but instable production of VEGF by critically ischemic muscles in the affected limb [21, 38]. The present study found increased concentration of the cytokine on day 14 in both groups of patients, but this increase was not sta-tistically significant (P > 0.05). Shyu et al. reported that mean plasma levels of VEGF increased sig-nificantly two weeks after gene therapy; the pres-ent results were differpres-ent [36], but the results of another two studies are ambiguous: one of them could not detect elevated levels of blood VEGF [32] and in the second study, in which the plasma level of VEGF after intramuscular gene injection was rose for seven days (38 to 41 pg/ml, P < 0.05), it was not different from baseline on days 14, 21, and 28 [39]. In the present study the prolonged
high level of VEGF between the 2nd and 4th week
after treatment seems to be related to increased production of cytokine by transfected muscle cells in injection sites and also by transfected stem cells from bone marrow cells [1, 21, 40]. The present study showed a significant drop in VEGF level in all patients on day 90 after administration. It must be noted that at this time more than half of the treated patients (15 of 24) underwent amputation, thus eliminating the ischemic area which stimu-lated the production of native VEGF [15]. It is well known that endothelial cells can synthesize VEGF under hypoxic conditions and they create addi-tional sources of secretion [41]. However, in most of these patients the amputation was performed at the calf level, and not below the knee, as previously planned.
The present authors believe that their therapy proved insufficient for a number reasons. First, the efficiency of transfection was too low to sus-tain a high level of VEGF protein or the period of gene expression was too short. However, even if VEGF gene expression is limited to a few cells, the paracrine effects of the product may be sufficient to achieve a biological effect [42]. The results of preclinical studies suggested that if the gene prod-uct is limited to less than 30 days, repeated admin-istration is necessary [43]. According to Kim et al., multiple injections with low doses would be more effective than a few infections at high doses [32]. The optimum dose and frequency of plasmid DNA administration should be established.
Second, VEGF isoforms are capable of bind-ing to two tyrosine kinase receptors (Flt1/VEGFR1 and KDR/VEGFR2) on the surface of endothelial cells and both receptors are important in con-trolling the effects of VEGF on angiogenesis. Waltenberger et al. showed that KDR/VEGFR2 is functionally upregulated in response to hypoxia; in fact, the mRNA level is decreased but the pro-tein level is augmented in an uncharacterized post-transcriptional manner [44]. Other investigators have suggested that hypoxia induced the produc-tion of the factor by vascular smooth muscle cells and vascular endothelial cells, which is capable of upregulating KDR/VEGFR2 protein on the endothelial cell surface [45]. The present authors hypothesize that the expression of a small num-ber of VEGF receptors on the cell surface can lead to a lack of response to VEGF and consequently a lack of therapeutic effect.
Third, non-viral vectors have limited efficacy and short duration of gene expression because they encounter the diffusional and metabolic barriers of the cytoplasm and nucleus [46]. Only a small amount of intact plasmid DNA can reach the nucleus and its metabolic instability may con-tribute to the low gene transfer efficiency [47]. In contrast to plasmids, viruses overcome these bar-riers and can sufficiently infect the host cells and enter the nucleus [48]. The adenovirus capsid has a specific protein which can bind to a nuclear pore complex and ensure the nuclear uptake of viral DNA [49, 50]. Viral vectors could probably ensure better effects of therapeutic angiogenesis, but they have altered the cellular structure and show severe disadvantages, such as immunogenicity and cytotoxity [51]. On the other hand, non-viral vec-tors are less effective but safer tools than viruses for delivering therapeutic angiogenic genes. The new generation of synthetic delivery systems (e.g. diverse liposomal formulations, basic proteins and polymers) have improved transgene expres-sion [52]. Nowadays, many studies focus on in
vivo intramuscular electroporation as a promising
method to augment gene expression [53–55]. Fourth, angiogenesis is a very complex process involving many factors, including growth factors, integrin cell surface receptors, matrix proteins, and
other components [56, 57].This process requires
alone may be insufficient to induce the matura-tion of capillaries [59, 60]. Masaki et al. found that a higher concentration of VEGF in ischemic muscle without a sufficient level of FGF2 can be toxic [60]. Another study reported that Ang-1 in conjunction with VEGF gene therapy can enhance arteriogenesis and angiogenesis [61]. Thus it is possible that administration in the appropriate order of a few proangiogenic genes might result in therapeutic angiogenesis.
Fifth, the formation of new blood vessels requires bone marrow-derived endothelial pro-genitor cells (EPCs) [62, 63]. The hemangioblast progenitor cells are capable of generating blood cells as well as endothelial cells [64, 65]. VEGF can mobilize endothelial cells and their progenitors from the bone marrow into the blood circulation [66]. Previous studies have shown that the number of EPCs and their neovascularization capacity are greatly limited in patients with several cardiovas-cular risk factors [67–69]. Therefore it is possible that the therapy applied in the present study did not lead to significant angiogenesis due to a lack of effector cells essential in this process. Many authors propose applying cell and gene therapy simultaneously or tend to use new genes [7, 15, 70, 71]. The present results confirmed this suggestion: 50% of the patients in group II compared with 25% in group I salvaged their limb.
The results of the present study demonstrated improvement in clinical symptoms in the patients
which cannot be attributed to a placebo effect [21, 35, 72]. It seems that the large amount of VEGF and the increased number of microvessels in biop-sy samples from three amputated limbs might be additional proof of neoangiogenesis induced by the combined method of treatment.
This study has shown that intramuscular gene therapy or combined cell/gene therapy with plas-mid encoding human VEGF165 is safe; no side effects
were observed besides slight, self-regressing edema of the treated calf. In this trial, 9 of 24 patients had clinical state improvement, the ischemic ulcers were healed, and the patients also saved their limbs from amputation. The authors suppose that the very advanced stage of the disease among the patients made therapy difficult; further investigations are needed to assess the effectiveness and usefulness of cell and/or gene therapy precisely. Due to the unsatisfactory clinical effects, the search for more effective methods to augment transgene expression should continue, for example using some transfec-tion factors and/or more than one angiogenic gene. The authors conclude that combined therapy is a more promising method of treatment in patients with chronic critical limb ischemia than exclu-sive administration VEGF plasmid. They suggest that future research should be focused on various aspects of the combined method, for example with more effective methods of cell transfection and/or using more than one angiogenic gene as well as the timing and duration of the treated period.
References
Creager MA:
[1] Medical management of peripheral arterial disease. Cardiol Rev 2001, 9, 238–245.
Dormandy JA:
[2] Therapeutic advances in critical limb ischemia. International Congress and Symposium Series No 195, 1992 May 2, Dublin.
Simons M, Bonow RO, Chronos NA, Cohen DJ, Giordano FJ, Hammond HK, Laham RJ, Li M, Pike M, Sellke [3]
FW, Stegmann TJ, Udelson JE, Rosengart TK: Clinical trials in coronary angiogenesis: issues, problems, consen-sus an expert panel summary. Circulation 2000, 102, e73–e86.
McLaren M, Newton DJ, Khan F, Belch JJ:
[4] Vascular endothelial growth factor in patients with critical limb ischemia before and after amputation. Int Angiol 2002, 21, 165–168.
Fam NP, Verma S, Kutryk M, Stewart DJ:
[5] Clinician guide to angiogenesis. Circulation 2003, 108, 2613–2618.
Fuchs S, Satler LF, Kornowski R, Okubagzi P, Weisz G, Baffour R, Waksman R, Weissman NJ, Cerqueira M, [6]
Leon MB, Epstein SE: Catheter-based autologous bone marrow myocardial injection in no-option patients with advanced coronary artery disease. J Am Col Cardiol 2003, 10, 1721–1724.
Hill JM, Zalos G, Halcox JPJ, Schenke WH, Waclawiw MA, Quyyumi AA, Finkel T:
[7] Circulating endothelial
progenitor cells, vascular function, and cardiovascular risk. N Eng. J Med 2003, 348, 593–600.
Clauss M, Gerlach M, Gerlach H, Bert J, Wang F, Familletti PC, Pan YC, Olander JV, Cionnolly DT, Stern D: [8]
Vascular permeability factor: A tumor-derived polypeptide that induces endothelial cells and monocyte procoagu-lant activity and promotes monocyte migration. J Exp Med 2004, 172, 1535–1545.
Baumgartner I, Pieczek A, Manor O, Blair R, Kearney M, Walsh K, Isner JM:
[9] Constitutive expression of
phVEGF165 after intramuscular gene transfer promotes collateral vessel development in patients with critical limb ischemia. Circulation 1998, 97, 1114–1123.
Rajagopalan S, Mohler E, Lederman RJ, Saucedo J, Mendelsohn FO, Olin J, Blebea J, Goldman C, Trachtenberg [10]
JD, Pressler M, Rasmussen H, Annex BH, Hirsch AT: Regional angiogenesis with vascular endothelial growth factor (VEGF) in peripheral arterial disease: Design of the RAVE trial. Am Heart J 2003, 145, 1114–1118.
Urbich C, Dimmeler S:
Iwaguro H, Yamaguchi J, Kalka Ch,
[12] Murosawa S, Masuda H, Hayashi S, Silver M, Li T, Isner JM, Ashara T:
Endothelial progenitor cell vascular endothelial growth factor gene transfer for vascular regeneration. Circulation 2002, 105, 732–738.
Heeschen Ch, Lehmann R, Honold J, Assmus B, Aicher A, Walter DH, Martin H, Zeiher AZ, Dimmeler S: [13]
Profoundly reduced neovascularization capacity of bone marrow mononuclear cells derived from patients with chronic ischemic heart disease. Circulation 2004, 109, 1615–1622.
Ozawa CR, Banfi A, Glazer NL, Thurston G, Springer ML, Kraft PE, Donald M, McDonald DM, Blau HM: [14]
Microenvironmental VEGF concentration, not total dose, determines a threshold between normal and aberrant angiogenesis. J Clin Invest 2004, 113, 516–527.
Choksy S, Pockley AG, Wajeh YE, Chan P:
[15] VEGF and VEGF receptor expression in human chronic critical limb
ischaemia. Eur J Vasc Endovasc Surg 2004, 28, 660–669.
Takahashi H, Shibuya M:
[16] The vascular endothelial growth factor (VEGF)/VEGF receptor system and its role
under physiological and pathological conditions. Clin Sci 2005, 109, 227–241.
Ferrara N:
[17] Vascular endothelial growth factor: basic science and clinical progress. Endocrine Rev 2004, 25, 581– 611.
Schagen FHE, Rademaker HJ, Fallaux FJ, Hoeben RC:
[18] Insertion vectors for gene therapy. Gene Ther 2000, 7,
271–272.
Mitrovic T:
[19] Gene transfer systems. Med Biol 2003, 10, 101–105.
Chomczynski P:
[20] A reagent for the single-step simultaneous isolation of RNA, DNA and proteins from cell and tissue samples. Biotechniques 1993, 15, 536–537.
Skóra J, Sadakierska-Chudy A, Pupka A, Biegus J, Barć P, Baczyńska D, Janczak D, Zacharska S, Ugorski M, [21]
Dobosz T, Szyber P: Application of VEGF165 plasmid in treatment of critical lower limb ischemia. Pol Merk Lek 2006, 20, 655–659.
Xie K, Wei D, Shi Q, Hung S:
[22] Constitutive and inducible expression and regulation of vascular endothelial growth
factor. Cytokine Growth Factor Rev 2004, 15, 297–324.
Bates DO, Hillman NJ, Williams B, Neal CR, Pocock TM:
[23] Regulation of microvascular permeability by vascular
endothelial growth factor. J Anat 2002, 200, 581–597.
Keck PJ, Hauser SD, Krivi G, Sanzo K, Warren T, Feder J, Connolly DT:
[24] Vascular permeability factor, an
endothelial cell mitogen related to PDGF. Science 1998, 246, 1309–1312.
Leung DW, Cachianes G, Kuang WJ, Goeddel DV, Ferrara N:
[25] Vascular endothelial growth factor is a secreted
angiogenic mitogen. Science 1998, 246, 1306–1309.
Baugmartner I, Rauch G, Pieczek A, Wuensch D, Manger M, Kearney M, Schainfeld R, Isner JM:
[26]
Lower-extremity edema associated with gene transfer of naked DNA encoding vascular endothelial growth factor. Ann Intern Med 2000, 132, 880–884.
Dvorak HF, Nagy JA, Feng D, Brown LF, Dvorak AM:
[27] Vascular permeability factor/vascular endothelial growth
factor and significance of microvascular hyperpermeability in angiogenesis. Curr Top Microbiol Immunol 1999, 237, 97–132.
Roberts WG, Palade GE:
[28] Increased microvascular permeability and endothelial fenestration induced by vascular
endothelial growth factor. J Cell Sci 1995, 108, 2269–2279.
Laitinen M, Zachary I, Breier G, Pakkanen T, Hakkinen T, Luoma J, Abedi H, Risau W, Soma M, Laakso M, [29]
Martin JF, Ylä-Herttula S: VEGF gene transfer reduce intimal thickening via increased production of nitric oxide in carotid arteries. Hum Gene Ther 1997, 8, 1737–1744.
van der Zee R, Murohara T, Luo Z,
[30] Zollman F, Passeri J, Lekutat C, Isner JM: Vascular endothelial growth
fac-tor/vascular permeability factor augments nitric oxide release from quiescent rabbit and human vascular endothe-lium. Circulation 1997, 95, 1030–1037.
Ylä-Herttuala S, Martin JF:
[31] Cardiovascular gene therapy. Lancet 2000, 355, 213–222.
Kim HJ, Jang SY, Park J,
[32] Byun J, Kim DI, Do YS, Kim JM, Kim S, Kim BM, Kim WB, Kim DK: Vascular
endothelial growth factor-induced angiogenic gene therapy in patients with peripheral artery disease. Exp Mol Med 2004, 36, 336–344.
Simovic D, Isner,JM, Ropper AH, Pieczek A, Weinberg DH:
[33] Improvement in chronic ischemic neuropathy
after intramuscular phVEGF165 gene transfer in patients with critical limb ischemia. Arch Neurol 2001, 58,
761–768.
Isner JM, Ropper A, Hirst K:
[34] VEGF gene transfer for diabetic neuropathy. Hum Gene Ther 2001, 12, 1593–
1594.
Stewart DJ, Hilton JD, Arnold JM, Gregoire J, Rivard A, Archer SL, Charbonneau F, Cohen E, Curtis M, [35]
Buller CE, Mendelsohn FO, Dib N, Page P, Ducas J, Plante S, Sullivan J, Macko J, Rasmussen C, Kessler PD, Rasmussen HS: Angiogenic gene therapy in patients with nonrevascularizable ischemic heart disease: a phase 2 randomized, controlled trial of AdVEGF(121) (AdVEGF121) versus maximum medical treatment. Gene Ther. 2006, 13(21), 1503–1511.
Shyu KG, Chang H, Wang BW, Kuan P:
[36] Intramuscular vascular endothelial growth factor gene therapy in
patients with chronic critical leg ischemia. Am J Med 2003, 114, 85–92.
Mäkinen K, Manninen H, Hedman M, Matsi P, Mussalo H, Alhava E, Ylä-Herttuala S:
[37] Increased vascularity
Kalka C, Masuda H, Takahashi T, Kalka-Moll WM, Silver M, Kearney M, Li T, Isner JM, Asahara T: [38]
Transplantation of ex vivo expanded endothelial progenitor cells for therapeutic neovascularization. Proc Natl Acad Sci USA 2000, 97, 3422–3427.
Freedman SB, Vale P, Kalka C, Kearney M, Pieczek A, Symes J, Losordo D, Isner JM:
[39] Plasma vascular
endothe-lial growth factor (VEGF) levels after intramuscular and intramyocardial gene transfer of VEGF-165 plasmid DNA. Hum Gene Ther 2002, 13, 1595–1603.
Kusumanto YH, van Weel V, Mulder NH, Smit AJ, van den Dungen JJ, Hooymans JM, Sluiter WJ, Tio RA, [40]
Quax PH, Gans RO, Dullaart RP, Hospers GA: Treatment with intramuscular vascular endothelial growth factor gene compared with placebo for patients with diabetes mellitus and critical limb ischemia: a double-blind random-ized trial. Hum Gene Ther 2006, 17(6), 683–691.
Namiki A, Brogi E, Kearney M, Wu T,
[41] Couffinhal T, Varticovski L, Isner JM: Hypoxia induces vascular
endothe-lial growth factor in cultured human endotheendothe-lial cells. J Biol Chem 1995, 270, 31189–31195.
Isner JM, Pieczek A, Schainfeld R, Blair R, Haley L, Ashara T, Rosenfield K, Razvi S, Walsh K, Symes J:
[42] Clinical
evidence of angiogenesis after arterial gene transfer of phVEGF165 in patient with ichaemic limb. Lancet 1996, 348,
370–374.
Tsurumi Y, Takeshita S, Chen D, Kearney M, Rossow ST, Passeri J, Horowitz JR, Symes JF, Isner JM:
[43] Direct
intramuscular gene transfer of naked DNA encoding vascular endothelial growth factor augments collateral devel-opment and tissue perfusion. Circulation 1996, 94, 3281–3290.
Waltenberger J, Mayr U, Pentz S, Hombach V:
[44] Functional upregulation of the vascular endothelial growth factor
receptor KDR by hypoxia. Circulation 1996, 94, 1647–1654.
Brogi E, Schatteman G, Wu T, Kim. EA, Varticovski L, Keyt B, Isner JM:
[45] Hypoxia-induced paracrine regulation
of vascular endothelial growth factor receptor expression. J Clin Invest 1996, 94, 469–476.
Lechardeur D, Lukacs G:
[46] Intercellular barriers to non-viral gene transfer. Curr. Gene Ther 2002,2, 183–194.
Neves C, Escriou V, Byk G, Scherman D, Wils P:
[47] Intracellular fate and nuclear targeting of plasmid DNA. Cell
Biol Toxicol 1999, 15, 193–202.
Seisenberger G, Reid M, Enderss T,
[48] Büning H, Hallek M, BräuchleCh: Real-time single-molecule imaging of
the infection pathway of an adeno-associated virus. Science 2001, 294, 1929–1932.
Harel A, Forbes DJ:
[49] Welcome to the nucleus: can I take your coat? Nat Cell Biol 2001, 3, E267–E269.
Trotman L, Mosberger N, Fornerod M, Stidwill R, Greber U:
[50] Import of adenovirus DNA involves the nuclear
pore complex receptor CAN/Nup214 and histone 1. Nat Cell Biol 2001, 3, 1092–1100.
Zaiss A, Muruve D:
[51] Immune response to adeno-associated virus vectors. Curr Gene Ther 2005, 5, 323–331.
Lechardeur D, Lukacs GL:
[52] Nucleocytoplasmic transport of pasmid DNA: perilous journey from the cytoplasm to
the nucleus. Hum Gene Ther 2006, 17, 882–889.
Ho SH, Hahn W, Lee HJ, Kim DS, Jeong JG, Kim S, Yu SS, Jeon ES, Kim S, Kim, JM:
[53] Protection against
collagen-induced arthritis by electrotransfer of an expression plasmid for the interleukin-4. Biochem Biophys Res Commun 2004, 321, 759–766.
Heller LC, Ugen K, Heller R:
[54] Electroporation for targeted gene transfer. Expert Opin Drug Deliv 2005, 2, 255–
268.
Kuroda T, Maruyama H, Shimotori M, Higuchi N, Kameda S, Tahara, H, Miyazaki J, Gejyo F:
[55] Effects of viral
interleukin 10 introduced by in vivo electroporation on arthrogen-induced arthritis in mice. J Rheumatol 2006, 33, 455–462.
Carmeliet P:
[56] Angiogenesis in health and disease. Nat Med 2003, 9, 53–60.
Simons M:
[57] Integrative signaling in angiogenesis. Mol Cell Biochem 2004, 264, 99–102.
Polverini JP:
[58] Angiogenesis in health and disease: insights into basic mechanisms and therapeutic opportunities. J Dent Educ 2002, 66, 962–975.
Engler DA:
[59] Use of vascular endothelial growth factor for therapeutic angiogenesis. Circulation 1996, 94, 1496– 1498.
Masaki I, Yonemitsu Y, Yamashita A, Sata S:
[60] Angiogenic gene therapy for experimental critical limb ischemia.
Acceleration of limb loss by over expression of vascular endothelial growth factor 165 but not fibroblast growth factor-2. Circ Res 2002, 90, 1–11.
Siddiqui AJ, Blomberg P, Wardell E, Hellgren I, Eskandarpour M, Islam KB, Sylven C:
[61] Combination of
angio-poietin-1 and vascular endothelial growth factor gene therapy enhances arteriogenesis in the ischemic myocar-dium. Biochem Biophys Res Common 2003, 310, 1002–1009.
Crosby J, Kaminski WE, Schatteman G, Martin PJ, Raines EW, Seifert RA, Bowen-Pope DF:
[62] Endothelial cells
of hematopoietic origin make a significant contribution to adult blood vessel formation. Circ Res 2000, 87, 728– 730.
Tateishi-Yuyama E, Matsubara H, Murohara T, Ikeda U, Shintani S, Masaki H, Amano K, Kishimoto Y, [63]
Yoshimoto K, Akashi H, Shimada K, Iwasaka T, Imaizumi T: Therapeutic angiogenesis for patients with limb ischemia by autologous transplantation of bone-marrow cells: pilot study and a randomised controlled trial. Lancet 2002, 360, 427–435.
Choi K, Kennedy M, Kazarov A, Papadimitriou JC, Keller G:
[64] A common precursor for hematopoietic and
endothelial cells. Development 1998, 125, 725–732.
Green AR:
Ashara T, Takahashi T, Maruda H, Kalka C, Chen D, Iwaguro H:
[66] VEGF contributes to postnatal
neovasculariza-tion by mobilizing bone marrow-derived endothelial progenitor cells. EMBO J 1999, 18, 3964–3972.
Golledge J:
[67] Lower-limb arterial disease. Lancet 1997, 350, 1459–1465.
Heilmann CAU, Attmann T, Thiem A, Haffner E, Beyersdorf F, Lutter
[68] G: Gene therapy in cardiac surgery:
intramyocardial injection of naked plasmid DNA for chronic myocardial ischemia. Eur J Cardiothorac Surg 2003, 24, 785–793.
Dzau VJ, Gnecchi M, Pachori AS, Morello F, Meloand LG:
[69] Therapeutic Potential of Endothelial Progenitor Cells
in Cardiovascular Diseases. Hypertension 2005, 46, 7–18.
Neil PF, Subodh V, Kutryk M, Stewart DJ:
[70] Clinician guide to angiogenesis. Circulation 2003, 108, 2613–2618.
Yang Y, Jiang-Yong M, Rana JS, Ke Q, Cai J, Chen Y, Morgan JP, Yong-Fu Xiao YF:
[71] VEGF enhances
func-tional improvement of postinfarcted hearts by transplantation of ESC-differentiated cells. J Appl Physiol 2002, 93, 1140–1151.
Isner JM, Baumgartner I, Rauh G, Schainfeld R, Blair R, Manor O, Razvi S, Symes JF:
[72] Treatment of
throm-boangiitis obliterans (Buerger’s disease) by intramuscular gene transfer of vascular endothelial growth factor: preliminary clinical results. J Vasc Surg 1998, 28(6), 964–973; discussion 73–75.
Address for correspondence:
Anna Sadakierska-Chudy Institute of Pharmacology Polish Academy of Sciences Smętna 12
31-343 Kraków Poland
Tel.: +48 12 66 23 389
E-mail: [email protected]
Conflict of interest: None declared