Copyright © 2007, American Society for Microbiology. All Rights Reserved.
Analysis of Changes in Recent Tuberculosis Transmission Patterns
after a Sharp Increase in Immigration
䌤
Jesu
´s In
˜igo,
1Darı´o Garcı´a de Viedma,
2Araceli Arce,
1Elia Palenque,
3Noelia Alonso Rodrı´guez,
2Elena Rodrı´guez,
1Marı´a Jesu
´s Ruiz Serrano,
2Sandra Andre
´s,
2Emilio Bouza,
2and Fernando Chaves
3*
Consejerı´a de Sanidad y Consumo, Comunidad de Madrid,1Servicio de Microbiologı´a Clı´nica y Enfermedades Infecciosas,
Hospital Gregorio Maran˜o´n,2and Servicio de Microbiologı´a, Hospital Doce de Octubre,3Madrid, Spain
Received 8 August 2006/Returned for modification 1 October 2006/Accepted 5 November 2006
We conducted a population-based molecular epidemiological study of tuberculosis (TB) in Madrid, Spain (2002 to 2004), to define transmission patterns and factors associated with clustering. We particularly focused on examining how the increase in TB cases among immigrants in recent years (2.8% in 1997 to 1999 to 36.2%
during the current study) was modifying transmission patterns.Mycobacterium tuberculosisisolates obtained
from patients living in nine districts of Madrid (1,459,232 inhabitants) were genotyped. The TB case rate among foreign-born people was three to four times that of Spanish-born people, and the median time from arrival to the onset of treatment was 22.4 months. During the study period, 227 (36.3%) patients were grouped in 64 clusters, and 115 (50.7%) of them were in 21 clusters with mixed Spanish-born and foreign-born patients. Three of the 21 mixed clusters accounted for 21.1% of clustered patients. Twenty-two of 38 (57.9%) immigrants in mixed clusters were infected with TB strains that had already been identified in the native population in 1997 to 1999, including the three most prevalent strains. Factors identified as independent predictors of clustering
were homelessness (odds ratio [OR], 2.3; 95% confidence interval [95% CI], 1.2 to 4.5;Pⴝ0.011) and to be
born in Spain (OR, 1.8; 95% CI, 1.2 to 2.6;P ⴝ0.002). The results indicated that (i) TB transmission was
higher in Spanish-born people, associated mainly with homelessness, (ii) that foreign-born people were much less likely to be clustered, suggesting a higher percentage of infection before arriving in Spain, and (iii) that an extensive transmission between Spanish- and foreign-born populations, caused mainly by autochthonous strains, was taking place in Madrid.
The burden of tuberculosis (TB) disease is greater in poor countries, but even within wealthy countries, deprived areas tend to have higher rates of TB incidence (1). As long as economic differences have prevailed between industrialized countries and the rest of the world, human migration has been an unavoidable phenomenon that has contributed substantially to change TB epidemiology in industrialized countries (2, 23). Unlike in neighboring countries, in Spain, immigration had little influence on TB prior to 2000 (11). Since 2000, important demographic changes have taken place in the country; for instance, in Madrid the percentage of the immigrant popula-tion rose from 1.9% in 1996 to 12.2% in 2003. During the last decade, significant changes in the epidemiology of TB in Ma-drid have occurred. Between 1994 and 1998, the TB rate de-creased from 48.5 per 100,000 to 26.8. Since 1998, the inci-dence of TB has decreased slowly, reaching 23.3 in 2003. Over a 10-year period, the percentage of TB cases coinfected with human immunodeficiency virus (HIV) decreased from 55.9% in 1994 to 14.3% in 2003, whereas TB cases in foreigners increased from 2.6% in 1994 to 33.7% in 2003 (14).
The new epidemiological scenario, with these recent socio-demographic changes in Madrid, gives us the opportunity to study in depth the epidemiology and transmission patterns of
TB and to compare these results with those obtained from a previous molecular epidemiology study performed in Madrid between 1997 and 1999, when 2.8% of TB cases were found to occur in foreign-born people (13). Understanding the factors that contribute to the incidence of TB is critical in defining new strategies and reinforcing the TB control program. We con-ducted a population-based molecular epidemiological study of TB in Madrid to define transmission patterns and predictors associated with being in a cluster. We particularly focused on determining whether or not the increase in cases of tubercu-losis among immigrants in recent years was modifying recent transmission patterns in Madrid.
MATERIALS AND METHODS
Design and study population.A prospective population-based molecular and epidemiological study of patients diagnosed with TB was conducted in nine urban districts in the south of Madrid (Spain) during 2002 to 2004. These districts have an official population of 1,459,232, and their largest providers of specialized
care are Hospital Doce de Octubre and Hospital Gregorio Maran˜on.
From 1 January 2002 to 31 December 2004, 1,155 tuberculosis cases were diagnosed in the study area and reported to the Regional Registry of TB in Madrid. For all patients, information was collected using a standardized proto-col. Data were assigned to the following sets of variables: demographic charac-teristics (age, sex, country of origin, number of years of residence in Madrid or elsewhere in Spain, and district of residence), clinical characteristics (date of symptom onset, date of diagnosis, site of disease, and previous TB), risk factors for TB (homelessness, injection drug use, presence of HIV infection, previous imprisonment, diabetes, silicosis, gastrectomy, and malignant disease), and in-formation from contact investigations. Additional inin-formation on HIV status was obtained by cross-matching the Regional Registry of Tuberculosis with the AIDS
* Corresponding author. Mailing address: Servicio de Microbiolo-gı´a, Hospital Universitario Doce de Octubre, Avenida de Cordoba sn, Madrid 28041, Spain. Phone: (34) 91-3908239. Fax: (34) 91-5652765. E-mail: [email protected].
䌤Published ahead of print on 15 November 2006.
63
on May 16, 2020 by guest
http://jcm.asm.org/
Regional Registry. All variables were measured in categories, except for age, which was measured as a continuous variable.
Microbiology.Primary isolation and culture of mycobacterial isolates were performed in the mycobacteriology laboratories of the two hospitals involved in the study. Susceptibility testing with isoniazid, rifampin, streptomycin, and ethambutol was performed using a mycobacterial growth indicator tube strepto-mycin-isoniazid-rifampin-ethambutol system (Becton Dickinson, Sparks, MD).
DNA fingerprinting with the insertion sequence IS6110was performed as
de-scribed previously (25). Computer-assisted analysis of IS6110fingerprints was
carried out using Bionumeric 4.0 software (Applied Maths, Kortrijk, Belgium).
Supplementary spoligotyping (15) was performed on all isolates which hadⱕ5
copies of IS6110and which shared identical restriction fragment length
poly-morphism (RFLP) patterns. Patients were included in clusters if their RFLP
patterns contained (i)ⱖ6 IS6110bands in an identical pattern or (ii)ⱕ5 identical
IS6110bands and an identical spoligotyping pattern.
Epidemiological investigation.Patients were interviewed and the contact trac-ing was done by the primary health care physicians. They sent the questionnaires to the Regional Registry of TB in Madrid, where this information was analyzed by two epidemiologists from our research group. We examined every case for contact with another TB patient in the 2 years prior to symptom onset and checked for the inclusion of any contacts in the Regional Registry of Tubercu-losis cases. For clustered patients, medical records were reviewed and general practitioners were questioned in order to obtain supplementary information about previous exposure to other cases of TB. An epidemiological link was defined as sharing a residence, place of employment, social activity, or family relationship with a case patient.
Statistical analysis.All tuberculosis patients diagnosed by culture in the study area were included. For all study patients, information concerning demographic characteristics, clinical characteristics, and risk factors for TB were collected using a standardized protocol based on the Regional Registry of Tuberculosis cases in Madrid. The time-related changes in the incidence of TB were estimated by Poisson regression. In order to identify risk factors for clustering, univariate
analysis was performed using thettest for continuous variables and the2or the
Fisher exact test for categorical variables. Factors that were significantly associ-ated with clustering were analyzed by multiple logistic regression, using a step-wise approach to identify factors that were independent predictors of clustering.
RESULTS
During the study period, 1,155 cases of TB were reported (1,090 in the general population and 65 cases diagnosed in prison). Among them, 887 (76.8%) were bacteriologically con-firmed as culture positive. The incidence rates in the general population were 23.5 per 100,000 in 2002 (332 cases), 26.3 in 2003 (384 cases), and 25.1 in 2004 (374 cases) (P⫽0.399 for trend). The incidence rates among the Spanish-born population were 18.9 in 2002 (241 cases), 19.6 in 2003 (251 cases), and 17.5 in 2004 (223 cases) (P⫽0.408 for trend). Among the foreign-born peo-ple, the incidence rates were 66.7 in 2002 (91 cases), 74.6 in 2003 (133 cases), and 70.8 in 2004 (151 cases) (P⫽0.727 for trend).
Demographic and clinical characterizations of the study
population.A total of 621 (70%) culture-proven cases were
molecularly characterized and included in the final univariate and multivariate analysis. The study population with molecular data available did not significantly differ with regard to demo-graphic and clinical characteristics from the total number of tuberculosis patients diagnosed in the south of Madrid during the 3-year study, with the exception that a greater proportion of pulmonary rather than extrapulmonary isolates was avail-able for fingerprinting (79.5% versus 71.3%;P⬍0.001).
Two hundred twenty-five patients (36.2%) were foreign-born individuals from 35 different countries, including 127 patients from South and Central America (56.4%), 40 from European countries (17.8%), 33 from the Magreb region of Africa (14.7%), 22 from sub-Saharan Africa (9.8%), and three from Asian countries (1.3%). The single most frequent country
of origin was Ecuador (n ⫽62 persons, 27.6%), followed by Morocco (n ⫽ 32, 14.2%), Romania (n ⫽ 26, 11.1%), Peru (n⫽24, 10.7%), Bolivia (n⫽14, 6.2%), and Colombia (n⫽
12, 5.3%). Information on date of arrival was available for 124 (55.1%) foreign-born cases. Among them, 65 (52.4%) were diagnosed within the first 2 years of residence, 37 (29.8%) between 2 and 5 years, and 22 (17.7%) after more than 5 years after arrival. The median time from arrival to the onset of treatment was 22.4 months (25th percentile [P25] toP75, 7.8 to
44.6).
Foreign-born patients were likely to be younger than Span-ish-born TB patients (Table 1). One hundred forty-eight (65.8%) of the foreign-born patients were younger than 35 years, compared to 134 (33.8%) of Spanish-born patients (P⬍
0.001). The median age of foreign-born TB patients was 29 years (P25toP75, 24 to 38), whereas it was 41 years (P25toP75,
[image:2.585.299.546.89.484.2]31 to 64) in Spanish-born cases (P⬍0.001). The proportion of TABLE 1. Comparison of sociodemographic risk factors among
Spanish-born and foreign-born TB patients
Characteristic
No. (%) of population with characteristic
Pvalue
Spanish-born patients
(n⫽396)
Foreign-born patients
(n⫽225)
Sex
Male 280 (70.7) 150 (66.7) 0.34
Female 116 (29.3) 75 (33.3)
Age (yr)a
1–14 10 (2.5) 17 (7.6) 0.006
15–34 124 (31.3) 131 (58.2) ⬍0.001
35–54 131 (33.1) 66 (29.3) 0.38
ⱖ54 123 (31.1) 8 (3.6) ⬍0.001
HIV status
Positive 87 (22.0) 23 (10.2) ⬍0.001
Negative/unknown 309 (78.0) 202 (89.8)
Injection drug use
Yes 77 (19.4) 12 (5.3) ⬍0.001
No/unknown 319 (80.6) 213 (94.7)
Homelessness
Yes 32 (8.1) 16 (7.1) 0.78
No/unknown 364 (91.9) 209 (92.9)
Localization of TBb
Pulmonary 313 (79.0) 181 (80.4) 0.75
Extrapulmonary/unknown 83 (21.0) 44 (19.6)
TB diagnosed in prison
Yes 37 (9.3) 8 (3.6) 0.012
No 359 (90.7) 217 (96.4)
Resistance to any drugc
Yes 40 (11.0) 25 (12.1) 0.82
No 322 (89.0) 182 (87.9)
Resistance to isoniazidc
Yes 26 (7.2) 19 (9.2) 0.49
No 336 (92.8) 188 (90.8)
a
Age was unknown in 11 cases. Each category was compared to the rest of the age groups.
b
Localization of TB was unknown in eight cases.
c
Available for 569 clinical isolates.
on May 16, 2020 by guest
http://jcm.asm.org/
HIV-seropositive TB patients was significantly lower in immi-grants (10.2% versus 22.0%;P⬍0.001). Among the foreign-born population, the proportion of HIV-infected patients was higher for people from sub-Saharan Africa (27.3%). Similar proportions of sputum smear-positive cases were seen among the foreign-born population (64.4%) and the Spanish-born population (60.9%) (P⫽0.46).
To examine the potential contribution of immigration to drug resistance, we analyzed strain data from the 569 (91.6%) patients for whom resistance information was available. Sixty-five (11.4%) were resistant to any first-line drug, 45 (7.9%) were resistant to isoniazid, and nine (1.6%) were multidrug resistant (i.e., resistant to both rifampin and isoniazid). Resis-tance did not change over time. The proportions of resistant cases were similar among immigrants (12.1%) and the Span-ish-born population (11.0%) (P⫽0.82). We also found similar proportions of isoniazid resistance among foreign-born and Spanish-born populations (9.2% versus 7.2%, respectively;P⫽
0.49) and similar proportions of multidrug resistance among both populations (1.9% versus 1.4%;P⫽0.73).
Cluster analysis and factors associated with clustering.
IS6110DNA fingerprinting and spoligotyping determined that 227 of the 621 patients (36.3%) were grouped in 64 clusters. Significantly more Spanish-born than foreign-born TB patients belonged to strain clusters (41.9% versus 27.1%;P⬍0.001). The genetic clusters were relatively small in size; 36 (56.3%) clusters contained only two people, 19 clusters (29.7%) tained three to five people, and nine clusters (14.1%) con-tained six or more people. Of the 227 clustered TB patients, 115 (50.7%) were in 21 clusters with mixed Spanish-born and foreign-born patients, 89 (39.2%) were in 33 clusters contain-ing only Spanish-born patients, and 23 (10.1%) were in 10 clusters containing only foreign-born patients (seven clusters contained members who all came from the same country).
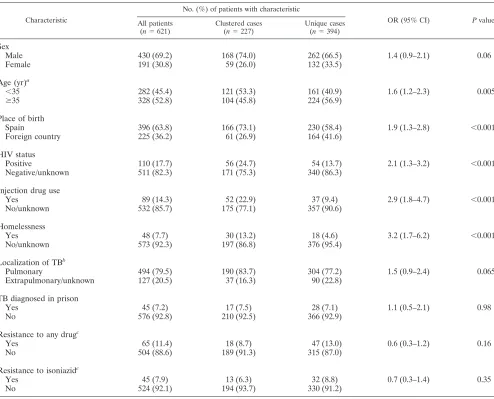
[image:3.585.46.540.79.478.2]Characteristics significantly associated with clustering ac-cording to the univariate analysis (Table 2) were age of⬍35 TABLE 2. Characteristics of patients with tuberculosis in Madrid (2002 to 2004) and their association with cluster status
Characteristic
No. (%) of patients with characteristic
OR (95% CI) Pvalue
All patients
(n⫽621)
Clustered cases
(n⫽227)
Unique cases
(n⫽394)
Sex
Male 430 (69.2) 168 (74.0) 262 (66.5) 1.4 (0.9–2.1) 0.06
Female 191 (30.8) 59 (26.0) 132 (33.5)
Age (yr)a
⬍35 282 (45.4) 121 (53.3) 161 (40.9) 1.6 (1.2–2.3) 0.005
ⱖ35 328 (52.8) 104 (45.8) 224 (56.9)
Place of birth
Spain 396 (63.8) 166 (73.1) 230 (58.4) 1.9 (1.3–2.8) ⬍0.001
Foreign country 225 (36.2) 61 (26.9) 164 (41.6)
HIV status
Positive 110 (17.7) 56 (24.7) 54 (13.7) 2.1 (1.3–3.2) ⬍0.001
Negative/unknown 511 (82.3) 171 (75.3) 340 (86.3)
Injection drug use
Yes 89 (14.3) 52 (22.9) 37 (9.4) 2.9 (1.8–4.7) ⬍0.001
No/unknown 532 (85.7) 175 (77.1) 357 (90.6)
Homelessness
Yes 48 (7.7) 30 (13.2) 18 (4.6) 3.2 (1.7–6.2) ⬍0.001
No/unknown 573 (92.3) 197 (86.8) 376 (95.4)
Localization of TBb
Pulmonary 494 (79.5) 190 (83.7) 304 (77.2) 1.5 (0.9–2.4) 0.065
Extrapulmonary/unknown 127 (20.5) 37 (16.3) 90 (22.8)
TB diagnosed in prison
Yes 45 (7.2) 17 (7.5) 28 (7.1) 1.1 (0.5–2.1) 0.98
No 576 (92.8) 210 (92.5) 366 (92.9)
Resistance to any drugc
Yes 65 (11.4) 18 (8.7) 47 (13.0) 0.6 (0.3–1.2) 0.16
No 504 (88.6) 189 (91.3) 315 (87.0)
Resistance to isoniazidc
Yes 45 (7.9) 13 (6.3) 32 (8.8) 0.7 (0.3–1.4) 0.35
No 524 (92.1) 194 (93.7) 330 (91.2)
aAge was unknown in 11 cases.
bLocalization of TB was unknown in eight cases.
cAvailable for 569 clinical isolates. We found three clusters with two patients each resistant to isoniazid.
on May 16, 2020 by guest
http://jcm.asm.org/
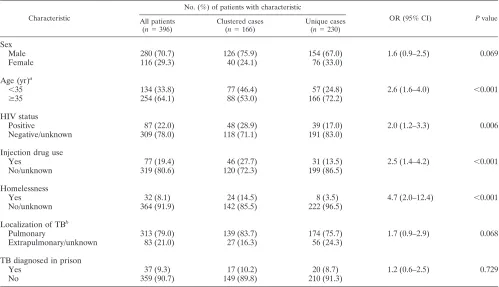
years (odds ratio [OR], 1.6; 95% confidence interval [95% CI], 1.2 to 2.3;P⫽0.005), to be born in Spain (OR, 1.9; 95% CI, 1.3 to 2.8;P ⬍ 0.001), intravenous drug use (OR, 2.9; 95% CI, 1.8 to 4.7;P⬍0.001), HIV infection (OR, 2.1; 95% CI, 1.3 to 3.2;P⬍0.001), and homelessness (OR, 3.2; 95% CI, 1.7 to 6.2; P ⬍ 0.001). In the logistic regression analysis, factors identified as independent predictors of clustering were home-lessness (OR, 2.3; 95% CI, 1.2 to 4.5;P⫽0.011) and to be born in Spain (OR, 1.8; 95% CI, 1.2 to 2.6;P⫽0.002). A separate analysis was performed to evaluate predictors of clustering in Spanish-born (Table 3) and in foreign-born (Table 4) persons. In the logistic regression model, the only factor identified as an independent predictor for clustering among Spanish-born per-sons was homelessness (OR, 3.5; 95% CI, 1.5 to 8.4; P ⫽
0.004).
Analysis of the 115 TB patients in 21 mixed clusters indi-cated that 77 (67%) of the TB patients were Spanish-born patients and 38 (33%) were foreign-born patients from 14 different countries. Three mixed clusters, which contained 17, 17, and 14 cases, accounted for 21.1% of clustered patients. We compared the DNA fingerprints of the isolates from the foreigners with a database from a previous study performed in Madrid between 1997 and 1999 (13). Twenty-two of 38 (57.9%) immigrants in mixed clusters were infected with TB strains that had already been identified in the native popu-lation, including the three most prevalent strains. We did not find immigrants with unique RFLP patterns or in clus-ters with only immigrants matching with those in the 1997 to 1999 database. The comparison between immigrants in
mixed clusters and the rest of the immigrants with TB showed that the first group had a higher proportion of intravenous drug users (13.2% versus 3.7%;P⫽0.034). Of the 38 foreign-born TB patients in mixed clusters, there was information on date of arrival for 21. For 12 patients (57.1%), TB was diagnosed within 2 years of arrival; for three patients (14.3%), TB was diagnosed from 2 to 5 years after arrival; and for six patients (28.6%), TB was diagnosed
⬎5 years after the person arrived in Spain. No differences could be found for the moment of diagnosis after arrival when comparing foreign TB patients (i) in mixed clusters, (ii) in foreign clusters, or (iii) unclustered.
[image:4.585.43.542.81.368.2]Epidemiologic connections were established for 50 (22%) of the 227 clustered TB cases, for 30 (18.1%) of the 166 Spanish-born patients in clusters, and for 20 (32.8%) of the 61 foreign-born TB clustered patients (P⫽0.03). Epidemi-ologic links were established for 20 (17.4%) of 115 patients in mixed clusters, for 20 (22.5%) of 89 TB patients in clusters containing only Spanish-born patients, and for 10 (43.5%) of 23 TB patients in clusters containing only for-eign-born persons. Overall, of the 20 relationships estab-lished through the 50 clustered TB patients with epide-miologic connections, possible TB transmission between Spanish-born persons occurred in 11 (55%) relationships, from foreign-born to foreign-born persons in seven (35%) relationships, from foreign-born to Spanish-born persons in one (5%) relationship, and from Spanish-born to foreign-born persons in one (5%) relationship.
TABLE 3. Risk factors for clustering in patients born in Spain (2002 to 2004)
Characteristic
No. (%) of patients with characteristic
OR (95% CI) Pvalue
All patients
(n⫽396)
Clustered cases
(n⫽166)
Unique cases
(n⫽230)
Sex
Male 280 (70.7) 126 (75.9) 154 (67.0) 1.6 (0.9–2.5) 0.069
Female 116 (29.3) 40 (24.1) 76 (33.0)
Age (yr)a
⬍35 134 (33.8) 77 (46.4) 57 (24.8) 2.6 (1.6–4.0) ⬍0.001
ⱖ35 254 (64.1) 88 (53.0) 166 (72.2)
HIV status
Positive 87 (22.0) 48 (28.9) 39 (17.0) 2.0 (1.2–3.3) 0.006
Negative/unknown 309 (78.0) 118 (71.1) 191 (83.0)
Injection drug use
Yes 77 (19.4) 46 (27.7) 31 (13.5) 2.5 (1.4–4.2) ⬍0.001
No/unknown 319 (80.6) 120 (72.3) 199 (86.5)
Homelessness
Yes 32 (8.1) 24 (14.5) 8 (3.5) 4.7 (2.0–12.4) ⬍0.001
No/unknown 364 (91.9) 142 (85.5) 222 (96.5)
Localization of TBb
Pulmonary 313 (79.0) 139 (83.7) 174 (75.7) 1.7 (0.9–2.9) 0.068
Extrapulmonary/unknown 83 (21.0) 27 (16.3) 56 (24.3)
TB diagnosed in prison
Yes 37 (9.3) 17 (10.2) 20 (8.7) 1.2 (0.6–2.5) 0.729
No 359 (90.7) 149 (89.8) 210 (91.3)
aAge was unknown in eight cases.
bLocalization of TB was unknown in five cases.
on May 16, 2020 by guest
http://jcm.asm.org/
DISCUSSION
Immigration from countries with high rates of TB to coun-tries with lower rates is a phenomenon which has affected different European and North American countries for quite some time (6, 8, 12, 16–18, 22). This obviously has an impact on the epidemiological features of TB of the host countries, and therefore the recent transmission patterns of TB are expected to be affected. However, in many cases it is difficult to measure this impact because most molecular epidemiology studies are not performed at the time when changes in the patterns of TB due to immigration are occurring. Our study fulfills the two aspects required to define a good epidemiological model for understanding the questions previously discussed, which are (i) to fit the time of analysis of recent transmission to the time when TB cases among immigrants are increasing (in our study, up to 36.2% of total cases) and (ii) to have a reference study of the situation before the sharp increase in immigration (in our case, a study between 1997 and 1999, when only 2.8% of the cases involved foreigners) (13). This combination of parame-ters in a “local” study converts our study into a good model for helping to understand a “global” issue: the role of immigration on changing the patterns of tuberculosis and recent transmis-sion of the host countries.
In this special epidemiological context, we have found a
much higher case rate of TB among the foreign-born than among the Spanish-born population, a lower percentage of clustered patients in the foreign-born population, and a high percentage of Spanish and foreign-born patients involved in mixed clusters. These results suggest that there are three epi-demiological patterns of tuberculosis occurring simultaneously in the city: the first in the Spanish-born population, the second in the foreign-born population, and the third between the two populations, all contributing with different weights to the cur-rent incidence of TB in Madrid. Each one of these epidemio-logical patterns could have special characteristics, risk factors, and mechanisms to develop active TB. Understanding these patterns of development will help us to design strategies for TB control.
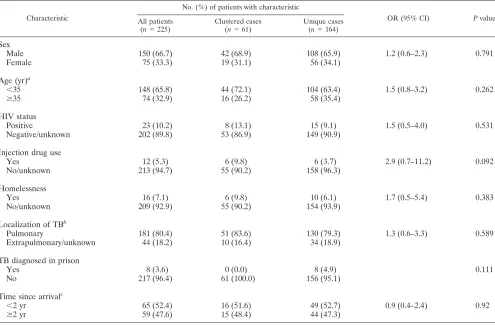
[image:5.585.45.540.81.406.2]This study shows that in the Spanish-born population the incidence of TB for the study period ranged from 17.5 to 19.6 cases per 100,000, significantly lower than the 30 cases per 100,000 reported for the period from 1997 to 1999 (13, 14). However, the percentage of clustered cases for the previous study was 44.8%, similar to the 41.9% for the Spanish-born population group reported in this study. In spite of the impor-tant decrease in the prevalence of HIV infection and intrave-nous drug use observed in the last 10 years, risk factors for clustering are similar in both studies. The study performed TABLE 4. Risk factors for clustering in foreign-born patients (2002 to 2004)
Characteristic
No. (%) of patients with characteristic
OR (95% CI) Pvalue
All patients
(n⫽225)
Clustered cases
(n⫽61)
Unique cases
(n⫽164)
Sex
Male 150 (66.7) 42 (68.9) 108 (65.9) 1.2 (0.6–2.3) 0.791
Female 75 (33.3) 19 (31.1) 56 (34.1)
Age (yr)a
⬍35 148 (65.8) 44 (72.1) 104 (63.4) 1.5 (0.8–3.2) 0.262
ⱖ35 74 (32.9) 16 (26.2) 58 (35.4)
HIV status
Positive 23 (10.2) 8 (13.1) 15 (9.1) 1.5 (0.5–4.0) 0.531
Negative/unknown 202 (89.8) 53 (86.9) 149 (90.9)
Injection drug use
Yes 12 (5.3) 6 (9.8) 6 (3.7) 2.9 (0.7–11.2) 0.092
No/unknown 213 (94.7) 55 (90.2) 158 (96.3)
Homelessness
Yes 16 (7.1) 6 (9.8) 10 (6.1) 1.7 (0.5–5.4) 0.383
No/unknown 209 (92.9) 55 (90.2) 154 (93.9)
Localization of TBb
Pulmonary 181 (80.4) 51 (83.6) 130 (79.3) 1.3 (0.6–3.3) 0.589
Extrapulmonary/unknown 44 (18.2) 10 (16.4) 34 (18.9)
TB diagnosed in prison
Yes 8 (3.6) 0 (0.0) 8 (4.9) 0.111
No 217 (96.4) 61 (100.0) 156 (95.1)
Time since arrivalc
⬍2 yr 65 (52.4) 16 (51.6) 49 (52.7) 0.9 (0.4–2.4) 0.92
ⱖ2 yr 59 (47.6) 15 (48.4) 44 (47.3)
aAge was unknown in three cases.
bLocalization of TB was unknown in three cases.
cTime since arrival was known in 124 cases.
on May 16, 2020 by guest
http://jcm.asm.org/
between 1997 and 1999 showed that clustered patients were younger than patients with a uniqueMycobacterium tuberculo-sisRFLP pattern and were more likely to be intravenous drug users and to have a history of previous imprisonment. The current study (2002 to 2004) showed that in addition to an age of⬍35 years, HIV infection, and injection drug use, homeless-ness is a new risk factor contributing to the transmission of tuberculosis in Madrid among Spanish-born people. Similar findings have been described in other studies (9, 12, 19). We believe there is an important margin for reducing the burden of TB in this population. It is necessary to intensify the mea-sures for TB control in these particular groups and the places where the TB transmission occurs.
In regard to the foreign-born population, the TB case rate for the study period ranged from 66.7 to 74.6 cases per 100,000, three to four times higher than the case rate for Spanish-born people. Most of these patients had recently migrated to Spain from countries with a high incidence of TB. Furthermore, an important epidemiological fact is that 82.4% of immigrants develop TB in the first 5 years of living in Spain. This percent-age is greater than those determined over the same time period in studies of other countries, i.e., 58.1%, 51.5%, and 40% in Germany (7), the United States (23), and Canada (5), respec-tively. Our molecular epidemiology study showed that foreign-born people were much less likely to be in the clustered group, and this could mean a higher percentage of infection before arriving in Spain. As the percentage of reported TB cases among foreign-born people continues to grow, the control of TB in Madrid will depend increasingly on TB case findings, tracing the contacts, and screening people at high risk for infection among this population (7, 10, 20).
Finally, in regard to TB dynamics among the autochthonous and foreign populations, we interestingly found that 50.7% of clustered patients were in clusters that resulted from transmis-sion ofM. tuberculosisbetween the two populations. We have epidemiologic evidence of transmission from one population to the other and vice versa. Furthermore, we found that 57.9% of immigrants in mixed clusters were infected with TB strains that had already been identified in the native population. Our study shows a more extensive transmission between the two populations in Madrid than other authors have shown previ-ously (3, 9, 22), even taking into account that in Madrid the period from arrival to the time of diagnosis of active TB was shorter than the parallel period in those studies. Probably, the sociocultural characteristics of immigrants coming to Spain, many of them sharing a common language with Spanish-born people, facilitate interactions between foreign-born people and the native population. With foreign-born cases, the possibility of recent transmission of TB after arrival is supported by the role of autochthonous strains in the recent transmission events of some of the TB cases in immigrants (those sharing risk factors with autochthonous cases, such as intravenous drug use), which clearly supports acquisition in the host country. We are probably underestimating the percentage of foreign-born people involved in transmission chains due to difficulties in accessing all foreign cases in a population with high mobility and also since this is a time when many foreigners reside illegally in Spain, which could make it difficult for the public health system to capture all TB cases.
Our study has some limitations. First, we were able to
iden-tify RFLP patterns for only 70% of all culture-positive cases and this lack of isolates may introduce a sampling bias (21). Higher capture of cases in Madrid could have identified more links. However, the analysis of disease characteristics did not reveal significant differences between those patients whose iso-lates were available for fingerprinting and the total population, other than the availability of a higher proportion of pulmonary isolates in the first group. Second, we found a low percentage of epidemiological links among clustered cases. This is a gen-eral limitation in molecular epidemiological studies (4, 9). In our study, although tuberculosis case registry and contact trac-ing information were examined, we did not carry out more-detailed interviews for all clustered cases than what is done routinely. Doing that might have aided in identifying more patient-to-patient links (24). Thus, the inference that we can make on cases that have molecular, demographic, and geo-graphic links but not documented case-to-case links is limited. Our molecular epidemiology study constitutes a model to describe the impact of sharp sociodemographic changes on the patterns of TB transmission at a time when these changes are occurring. To further control TB in Madrid, there must be an intensification of measures focused on improving the identifi-cation of contacts among Spanish-born and foreign-born peo-ple with homelessness and drug abuse. In addition, data ob-tained in this study also support the need for a strategy of screening for TB infection and case finding among the foreign-born population in their first contact with the health system in Spain. This strategy will allow us to decrease incidence rates, but global TB control will be required to advance towards the elimination of the disease in western Europe.
ACKNOWLEDGMENTS
We thank Antonia Martı´n and Mar Aguilera for excellent technical assistance.
This study was financed partially by grants from Fondo de Investi-gaciones Sanitarias (02/0572, 02/1307, 02/0882, and 03/0654). N.A.R. received a grant from Consejerı´a de Educacio´n de la Comunidad de Madrid and the European Social Fund (7580/2003).
REFERENCES
1.Bates, I., C. Fenton, J. Gruber, D. Lalloo, A. Medina Lara, S. B. Squire, S. Theobald, R. Thomson, and R. Tolhurst.2004. Vulnerability to malaria, tuberculosis, and HIV/AIDS infection and disease. Part 1: determinants
operating at individual and household level. Lancet Infect. Dis.4:267–277.
2.Broekmans, J. F., G. B. Migliori, H. L. Rieder, J. Lees, P. Ruutu, R. Loddenkemper, and M. C. Raviglione.2002. European framework for tu-berculosis control and elimination in countries with a low incidence—rec-ommendations of the World Health Organization (W. H. O.), International Union Against Tuberculosis and Lung Disease (IUATLD) and Royal Neth-erlands Tuberculosis Association (KNCV) Working Group. Eur. Respir. J.
19:765–775.
3.Chin, D. P., K. DeRiemer, P. M. Small, A. P. de Leon, R. Steinhart, G. F. Schecter, C. L. Daley, A. R. Moss, E. A. Paz, R. M. Jasmer, C. B. Agasino, and P. C. Hopewell.1998. Differences in contributing factors to tuberculosis incidence in U.S.-born and foreign-born persons. Am. J. Respir. Crit. Care
Med.158:1797–1803.
4.Clark, C. M., C. R. Driver, S. S. Munsiff, J. R. Driscoll, B. N. Kreiswirth, B. Zhao, A. Ebrahimzadeh, M. Salfinger, A. S. Piatek, J. Abdelwahab, et al.
2006. Universal genotyping in Tuberculosis Control Program, New York
City, 2001–2003. Emerg. Infect. Dis.12:719–724.
5.Cowie, R. L., and J. W. Sharpe.1998. Tuberculosis among immigrants: interval from arrival in Canada to diagnosis. A 5-year study in southern
Alberta. Can. Med. Assoc. J.158:599–602.
6.Dahle, U. R., P. Sandven, E. Heldal, and D. A. Caugant.2003. Continued low
rates of transmission ofMycobacterium tuberculosisin Norway. J. Clin.
Mi-crobiol.41:2968–2973.
7.Diel, R., S. Ru¨sch-Gerdes, and S. Niemann.2004. Molecular epidemiology of tuberculosis among immigrants in Hamburg, Germany. J. Clin. Microbiol.
42:2952–2960.
on May 16, 2020 by guest
http://jcm.asm.org/
8.Ellis, B. A., J. T. Crawford, C. R. Braden, S. J. N. McNabb, M. Moore, S. Kammerer, et al.2002. Molecular epidemiology of tuberculosis in a sentinel
surveillance population. Emerg. Infect. Dis.8:1197–1209.
9.El Sahly, H. M., G. J. Adams, H. Soini, L. Teeter, J. M. Musser, and E. A. Graviss.2001. Epidemiologic differences between United States- and
for-eign-born tuberculosis patients in Houston, Texas. J. Infect. Dis.183:461–
468.
10.Geng, E., B. Kreiswirth, C. Driver, J. Li, J. Burzynski, P. DellaLatta, A. LaPaz, and N. W. Schluger.2002. Changes in the transmission of
tubercu-losis in New York City from 1990–1999. N. Engl. J. Med.364:1453–1458.
11.Grupo de Trabajo de los Talleres de 2001 y 2002 de la Unidad de Investi-gacion en Tuberculosis de Barcelona.2003. Prevencio´n y control de las
tuberculosis importadas. Med. Clin. (Barcelona)121:549–557.
12.Hernandez-Garduno, E., D. Kunimoto, L. Wang, M. Rodrigues, R. K. Elwood, W. Black, S. Mak, and J. M. FitzGerald.2002. Predictors of clus-tering of tuberculosis in greater Vancouver: a molecular epidemiologic
study. Can. Med. Assoc. J.167:349–352.
13.Inigo, J., A. Arce, J. M. Martin-Moreno, R. Herruzo, E. Palenque, and F. Chaves.2003. Recent transmission of tuberculosis in Madrid: application of capture-recapture analysis to conventional and molecular epidemiology. Int.
J. Epidemiol.32:763–769.
14.Inigo, J., A. Arce, E. Rodrı´guez, D. Garcı´a de Viedma, E. Palenque, M. J. Ruiz Serrano, L. Cabello, and F. Chaves.2006. Tuberculosis trends in Ma-drid (1994–2003): impact of immigration and HIV infection. Int. J. Tuberc.
Lung Dis.10:550–553.
15.Kamerbeek, J., L. Schouls, A. Kolk, M. van Agterveld, D. van Soolingen, S. Kuijper, A. Bunschoten, H. Molhuizen, R. Shaw, M. Goyal, and J. D. A. van Embden.1997. Simultaneous detection and strain differentiation of Myco-bacterium tuberculosisfor diagnosis and epidemiology. J. Clin. Microbiol.
35:907–914.
16.Kulaga, S., M. Behr, K. Musana, J. Brinkman, D. Menzies, P. Brassard, D. Kunimoto, T. N. Tannenbaum, L. Thibert, L. Joseph, J. F. Boivin, and K. Schwartzman.2002. Molecular epidemiology of tuberculosis in Montreal.
Can. Med. Assoc. J.167:353–354.
17.Kunimoto, D., K. Sutherland, K. Wooldrage, A. Fanning, L. Chui, J. Manfreda,
and R. Long.2004. Transmission characteristics of tuberculosis in the for-eign-born and the Canadian-born populations of Alberta, Canada. Int. J.
Tuberc. Lung Dis.8:1213–1220.
18.Lillebaek, T., Å. B. Andersen, J. Bauer, A. Dirksen, S. Glismann, P. de Haas, and A. Kok-Jensen.2001. Risk ofMycobacterium tuberculosistransmission in a low-incidence country due to immigration from high-incidence areas.
J. Clin. Microbiol.39:855–861.
19.Luka´cs, J., V. Tubak, J. Mester, S. Da´vid, Z. Ba´rtfai, T. Kubica, S. Niemann, and A. Somosko¨vi.2004. Conventional and molecular epidemiology of tu-berculosis in homeless patients in Budapest, Hungary. J. Clin. Microbiol.
42:5931–5934.
20.Maguire, H., J. W. Dale, T. D. McHugh, P. D. Butcher, S. H. Gillespie, A. Costetsos, H. Al-Ghusein, R. Holland, A. Dickens, L. Marston, P. Wilson, R. Pitman, D. Strachan, F. A. Drobniewski, and D. K. Banerjee.2002. Molec-ular epidemiology of tuberculosis in London 1995–7 showing low rate of
active transmission. Thorax57:617–622.
21.Murray, M., and D. Alland.2002. Methodological problems in the molecular
epidemiology of tuberculosis. Am. J. Epidemiol.155:565–571.
22.Sharnprapai, S., A. C. Miller, R. Suruki, E. Corkren, S. Etkind, J. Driscoll, M. McGarry, and E. Nardell.2002. Genotyping analyses of tuberculosis cases in U.S.- and foreign-born Massachusetts residents. Emerg. Infect. Dis.
8:1239–1245.
23.Talbot, E. A., M. Moore, E. McCray, and N. J. Binkin.2000. Tuberculosis
among foreign-born persons in the Unites States, 1993–1998. JAMA284:
2894–2900.
24.van Deutekom, H., S. P. Hoijng, P. E. de Haas, M. W. Langendam, A. Horsman, D. van Soolingen, and R. A. Coutinho.2004. Clustered tubercu-losis cases: do they represent recent transmission and can they be detected
earlier? Am. J. Respir. Crit. Care Med.169:806–810.
25.Van Embden, J. D. A., M. D. Cave, J. T. Crawford, J. W. Dale, K. D. Eisenach, B. Gicquel, P. Hermans, C. Martin, R. McAdam, T. M. Shinnick, and P. M. Small.1993. Strain identification ofMycobacterium tuberculosisby DNA fingerprinting: recommendations for a standardized methodology.
J. Clin. Microbiol.31:406–409.