INFORMATION
ARCHITECTURE
IMPROVING
AWARENESS OF
AVAILABLE DATA,
INFORMATION AND
INTELLIGENCE
Report and recommendations
August 2012
TABLE OF CONTENTS
1 Summary ... 2
2 Introduction ... 4
3 Stakeholder requirements ... 5
4 Product development ... 8
5 Recommendations for improving data, information and intelligence11 6 Conclusions ... 16
1
SUMMARY
The Department of Health (DH), as part of the wider Education and Training Reform
Programme to support a safe transition to the new health system, commissioned
the Centre for Workforce Intelligence (CfWI) to develop a set of products which would
support workforce planners and education commissioners by improving awareness
of relevant sources of data, information and intelligence, to inform decision
making.
Our approach was to engage with a range of stakeholders and partner organisations to establish the information requirements of those responsible for workforce planning and education commissioning at a national, regional and local level. This informed the development of:
• a knowledge bank detailing validated sources of data, information and
intelligence
• an electronic signposting tool to enable user-friendly access via the CfWI
website.
This report summarises the CfWI’s approach to this project, describes the
engagement with stakeholders and partners and explains how these discussions informed developments. It highlights some areas for improvement in the way data is collected and shared and links these to initiatives which are already being
implemented to address gaps and support more effective workforce planning and decision making in the future.
Key messages
• Stakeholders confirmed that an electronic signposting tool could benefit their work and that this should :
o be interactive and offer a search function
o provide summary information categorised as raw data, information and intelligence.
• There was general consensus that the tool would be relevant and useful to a
wide range of end users at national, regional and local level.
• There is significant demand for a more comprehensive and sophisticated
web-based tool which would improve awareness of data sources; what they
do and don’t provide and to provide enhanced functionality for the user to maximise shared learning between users.
• Senior leaders, strategic workforce planners and education commissioners support actions to address the further improvement needed to the
Next steps
• Develop and implement a communications strategy to raise awareness of
the electronic signposting tool using existing networks and communications channels and promote the benefits of use (tool to be launched September 2012).
• Monitor and evaluate how the tool is accessed and used by the different
end user groups, gathering feedback on the functionality and content
(Autumn 2012).
• Collate feedback from stakeholders regarding the tool. If appropriate, hold discussions on whether it would be beneficial to commission a scoping report that sets out the infrastructure, investment required and benefits in developing a more comprehensive, web-based tool in the future (December 2012).
• Continue to work with lead organisations across the health and social care system to inform further improvements to data integrity and to the way data is collected and made accessible to support effective workforce planning and education commissioning.
• Feed information about data gaps and areas for improvement into the
2
INTRODUCTION
This report summarises the CfWI’s 2012 Workforce Information Architecture (WIA) project which, at a time of significant change across the health system, aims to improve awareness of available data, information and intelligence. This project does this by:
• exploring the current and future information requirements of workforce planners and education commissioners
• developing a robust, user-friendly signposting product to enable greater awareness of data sources information and intelligence and what they do and don’t do
• identifying issues and recommendations for future improvements to the way
data is collated and accessed.
This work builds on a CfWI project in 2010 which undertook an in-depth analysis of data sources and produced a static ‘map’ showing where workforce data was
collected and housed. An accompanying report, Review of Information Architecture,
CfWI (2010) http://www.cfwi.org.uk/intelligence/projects/information-architecture-1 provided a detailed summary of each of the sources and highlighted the gaps and issues affecting access.
The DH commissioned the CfWI to review information requirements and develop an updated and interactive version of the earlier ‘map’. This was primarily to ensure planners and commissioners are able to locate and, where appropriate, access data in the new system and also to understand what individual data sources provide and do not provide. It is important to note that the CfWI is not a data repository and does not hold workforce data.
This CfWI project is an important element of the wider DH WIA workstream. The aim of the over-arching workstream is to further develop the workforce information architecture to bring about improvements in the quality of data and in the way workforce planning data and information is made available and accessible.
3
STAKEHOLDER REQUIREMENTS
The CfWI engaged with over 50 stakeholders at national, regional and local level and from different parts of the health and social care sector to understand their requirements and inform the product development. This included engagement with:
• workforce planners and education commissioners in Strategic Health
Authorities (SHAs), deaneries, NHS trusts, local authorities, social enterprise and primary care organisations
• workforce and policy leads at the DH, Medical Education England (MEE), Professional Advisory Bodies and Royal Colleges
• providers of data, information and intelligence e.g. Skills for Care (SfC), Skills for Health (SfH) and the Health and Social Care Information Centre (HSCIC). Details of contributors to this project can be found at Annex 1.
A series of semi-structured telephone interviews were conducted to gather views on common information requirements and data sources, explore the key issues affecting access to consistent and high quality data, information and intelligence. They also sought to identify potential end users for the products, together with the key features and functionality which would be of most benefit to users.
Two facilitated workshops were held to focus specifically on:
• understanding common information requirements and data sources
• identifying and prioritising who would be ‘end users’ for the proposed tool • establishing the core functionality required and ranking this by importance • reviewing early mock-ups of two products and obtaining feedback on the
extent to which these might meet the identified needs.
Combined stakeholder feedback from the interviews and workshops indicated that: • the proposed tool would be beneficial to a range of end users
• all potential end users would have broadly the same requirements for the tool
• potential end users could be grouped into the following categories, set out in the following table.
Potential end users Examples of existing and emergent organisations by category
National bodies Department of Health (DH), Public Health England (PHE), Health Education England (HEE), the CfWI
Local workforce planning and education commissioning bodies
Local authorities, strategic health authorities (SHAs), deaneries, local education and training boards (LETBs) Providers of health and social care services NHS, independent, voluntary and
community Providers of education and training
services
Higher education, further education, private providers
Service commissioners Clinical commissioning groups, local authorities.
Critical requirements identified by stakeholders included:
• The terminology used must be consistent and understood by a wide range
of potential end users (not just those in a workforce planning role). • The tool needs to be easily accessible and user friendly.
• Information provided must be kept up to date to ensure users have confidence in the tool.
• The tool must have the ability to do multiple searches. • The tool needs to have the ability to save and edit searches.
• The tool must be carefully marketed and communicated to manage
expectations and encourage use by a wide group of stakeholders .
• There must be a facility to provide feedback on the tool itself and the information contained within the tool.
Important requests included:
• The tool would ideally be an integrated web based solution. • It would be useful to include key regional sources.
The CfWI’s research to develop the tool also highlighted that stakeholders and partners have some concerns about data gaps and the consistency and quality of
information available to support effective workforce planning. They suggested a
number of key issues which need to be addressed to maximise the benefits that the signposting tool can bring to the health and social care sectors in the future. For a more detailed discussion of these issues, please refer to Chapter 5 below.
A consistent message from stakeholders was that an interactive PDF tool would not meet their requirements, as this could not provide a facility to search, sort or filter the information in a variety of ways in order to reach summary information on the most appropriate sources.
As a result, following discussions with the DH, the CfWI were able to revise the project brief to produce an electronic Excel-based signposting tool to provide greater functionality than an interactive PDF. The revised solution meets the critical need for stakeholders to search, sort and filter the information using multiple parameters. This facility provides both a free text search and a specific search using drop down options in order to find summary information on the most appropriate sources. In addition, the CfWI has provided the DH with the benefits and indicative costings for
a more comprehensive, web-based tool that could be developed in the future and
would meet some of the additional stakeholder requirements such as access to reviews of the most popular searches. If feedback from users indicates significant demand to further develop the tool into an on-line web-based solution, a detailed scoping exercise would be required to agree the functional requirements, costings and funding arrangements.
4
PRODUCT DEVELOPMENT
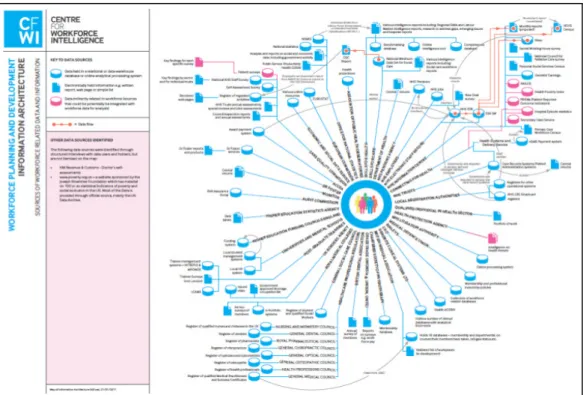
The initial aim of the project was to update an existing diagram (Figure 1) which maps where workforce data is collected and housed and to develop this into an interactive version of the current PDF.
Download a PDF version of the Information Architecture map
http://www.cfwi.org.uk/intelligence/projects/information-architecture-1/files/information-architecture-map.
Figure 1: Information Architecture Map produced by CfWI in 2010
The first stage was to compile a spreadsheet-based ‘knowledge bank’. This contains over 100 sources of data and information relevant to health and social care
workforce planning. Each entry shows whether a particular source: • captures raw data,such as the NHS Electronic Staff Record (ESR) • makes available information, for example the Health and Social Care
Information Centre (HSCIC)
• provides intelligence by adding value to raw data and information, as in the case of the CfWI and Sector Skills Councils (SSCs).
Each lead organisation with responsibility for an entry has been given the
opportunity to verify the description on the entry, with a 99 per cent response rate to date. This includes:
• level of coverage across England • availability and access
• type of information e.g. age, gender, demographic • web page link
• contact details for further information
• known issues from a workforce planning perspective and suggested
improvements.
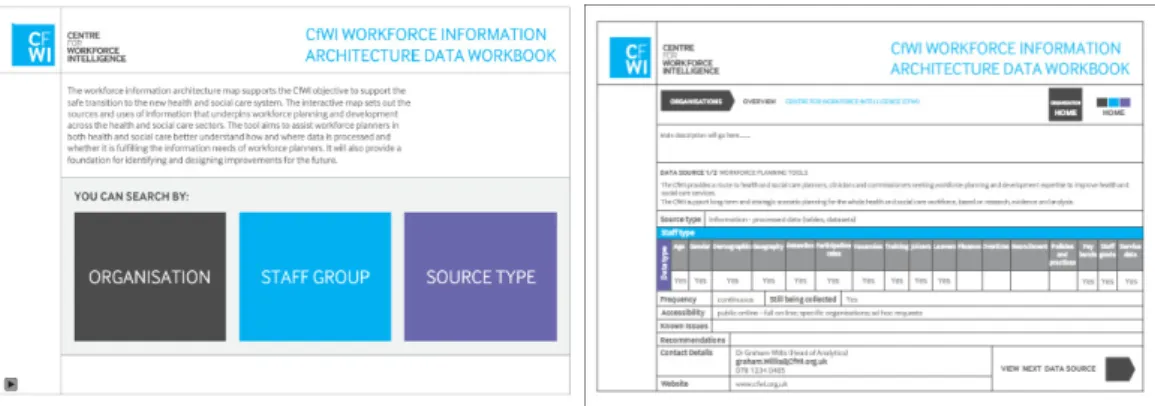
This knowledge bank was designed to provide the content for an interactive
version of the PDF ‘map’ through which users could access summary information
for each source.
Figure 2: Examples of mock up screens for interactive PDF
As a result of stakeholder engagement, it became clear that a tool of this nature could not provide the level of functionality being requested by the majority of potential end users and that some of the requirements could only be met by a more sophisticated web-based solution.
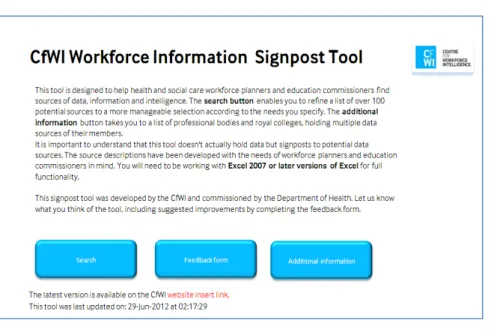
Following a technical analysis of the options available to provide an appropriate solution, the project brief was adapted to focus on developing, within the same financial envelope and timeline, an electronic Excel-based signposting tool. This option:
• provides more enhanced functionality than an interactive PDF • meets the most critical requests from stakeholders
• could form the basis of a more comprehensive, web-based solution in the future.
Figure 3: Screen shot of the CfWI workforce information signposting tool
The CfWI has provided the project sponsor, the DH, with a summary of the high level requirements of stakeholders and the extent to which these have been met by the current project. This includes indicative costings for a more comprehensive, web-based tool that could be developed in the future and would meet more of the stakeholder requirements.
As significant change to data sources is infrequent, updating of the tool content will take place on a continuous basis as the CfWI become aware of changes (both
through our own work and via feedback from others). Core information contained within the tool, for example contact names, will be checked every six months. The tool will include the opportunity for users to provide feedback and suggested improvements. These comments will be collated and presented to the DH for further discussion (autumn 2012). It is also suggested that this is supported by a small number of structured telephone interviews with stakeholders and partners to gather feedback on the content, functionality and usability of the tool.
User testing of the signposting tool will be essential to gather feedback on functionality and content, to inform future development and improvements, for example:
• indicating whether sources include information which could help to track the movement of health professionals
• adapting the language and terminology to make the tool more appropriate for a wider audience
• additional interactive functionality to enable users to learn from each other and how they have used the sources available (this would require a web-based solution).
5
RECOMMENDATIONS FOR IMPROVING
DATA, INFORMATION AND INTELLIGENCE
This section of the report outlines recommendations being made by the CfWI on ways in which data, information and intelligence could be improved to support more effective workforce planning and education commissioning. These
recommendations are a result of stakeholder feedback and from the core work of the CfWI including development of the workforce information signposting tool. We focus on five key areas that the CfWI believes require improvement and which would help to create a more flexible data system, able to respond to the needs of the emerging LETBs.
It is vital that workforce planners and service commissioners have access to data which has the right level of granularity and is aligned to the way education and training is commissioned. This will help to inform workforce planning more
effectively, particularly for highly specialised professions. A more flexible data system of this sort will also help provide the information workforce planners and service commissioners need to understand the likely quality outcomes and financial implications of their plans and decisions.
Addressing gaps and issues for improvement will require a concerted effort over time by a range of organisations within the health and social care sector. The CfWI
acknowledges that a number of initiatives to support improvement are already underway, including the DH WIA workstream of which this project is one element. The DH is also working closely with the Health Education England transition team and a range of partners, including the CfWI, to review the current education and training planning cycle, identify areas for improvement and develop guidance to support the emerging LETBs.
The overarching theme for improvement relates to data quality and data granularity and the top four priority areas which emerged from the CfWI WIA project are:
• supporting the programme to improve data quality through the NHS Electronic
Staff Record
• availability of core workforce information across all qualified providers of NHS funded services
• an agreed standardised approach to data and information collection by regulators, royal colleges and professional bodies
• improved access to raw data and information to enable analysis and benchmarking
A key challenge in taking forward these developments will be to balance the need for better quality workforce data against the desire not to add to the burden of data collection across the sector. While recognising this constraint, we consider that
much can be achieved through better coordination and cooperation. There is also scope in some areas for streamlining and simplification.
1. Supporting the programme to improve data quality through the NHS
Electronic Staff Record
Having a central Electronic Staff Record (ESR) system has brought many advantages and streamlined the collection of workforce information from the hospital and community health sector. The need to collect data once has replaced a burdensome central collections system and provided vital information which can support effective workforce planning. The current contract for the provision of the NHS Electronic Staff Record comes to an end in August 2014 and users have been involved in developing future requirements. We urge LETBs to engage in the consultation on re-procurement of ESR so their future needs are considered. The emerging LETBs will be reliant on access to comprehensive and accurate data to inform their workforce strategies and plans.
The CfWI considers that greater clarity is needed on where future responsibility will sit for assuring the quality of data at a local level in the new system, and in particular, whether LETBs will have a quality assurance role for the data they use in their
workforce strategies and plans.
As part of the Health and Social Care Act (2012) the Health and Social Care
Information Centre (HSCIC) has been given a lead role on data quality across health and social care. In 2011 the HSCIC implemented a revised data quality process for ESR data so that a single data quality report is sent to individual provider
organisations on a monthly basis. This highlights any issues relating to specific fields within ESR and summary reports are also sent to SHAs
The CfWI supports the continued development of the ESR system and the HSCIC’s ongoing programme to improve data quality. We recommend that the focus should continue to be on improving the integrity and completion of data and the work with NHS providers to increase the use and accuracy of ESR fields and benchmarking tools.
Other improvements which would be beneficial include:
• The recording of data with greater granularity on medical sub-specialism. Establishing methods to improve the coding of medical sub speciality
categorisation published by the HSCIC in December 2011. It is important that this is updated in ESR as individual roles change.
• The continued drive to improve coding as workforce titles change for example in healthcare sciences, in line with the latest defined Modernising Scientific Careers roles and specialisms.
• The continued improvement in the granularity of recording data on some
Stakeholders and partner organisations highlighted particular challenges in obtaining robust and timely data for the primary and community workforce. The CfWI
recommends that consideration is given to ways in which the level and quality of data available through the ESR for the workforce in the primary care and community sectors can be improved to help inform local planning and commissioning.
2. Availability of core information across all qualified providers of NHS funded services
Gaining access to high-quality, robust data across all parts of the healthcare
workforce is a significant challenge. Currently, education commissioning cannot take full account of the needs of the independent sector yet decisions on commissioning the future NHS workforce have an impact on both NHS funded and independent organisations.
More complete information will help improve supply and demand forecasts across all of health and social care, which will in turn improve workforce planning. The need for more robust workforce data and a better understanding of workforce requirements across both sectors is likely to become more important as the system shifts to provide more integrated care and staff currently employed in the NHS are employed in different organisations, for example, local authorities and social enterprises. There is therefore an increasing need for all providers of healthcare services to provide basic workforce planning information to the system. We recognise the concerns regarding the sharing of data with competitors and the need to explore: • whether there could be a mandated collection for all NHS qualified providers
• how the competitiveness of providers could be protected when they provide
such data to the wider system.
This could be achieved through the national minimum dataset strand of the DH WIA workstream which is already well advanced in establishing a core workforce data set for all qualified providers of NHS services. The case needs to be made to all health and social care providers of the benefits to them of providing high quality workforce data to inform local education and training commissioning.
3. An agreed standardised approachto data and information collection by
regulators, royal colleges and professional bodies
The professional bodies currently invest a great deal of time and effort in collecting profession-specific data. This data has been, and will continue to be, valuable in informing workforce planning at a local, regional and national level. It also informs education commissioning and investment planning. However the nature and frequency of the data collected varies considerably, as do the definitions used.
The CfWI recommends that a minimum dataset for all royal colleges and professional bodies should be developed, to enable valid comparisons across the professions. Our on-going work with royal colleges and professional bodies suggest support for this. It would be of great benefit to the system if all regulators and/or medical royal colleges had a standardised approach to capturing data, based on agreed definitions. If all regulators could agree a minimum data set so that comparisons can be made across professions, each part of the system could then embark on developing comparative plans based on agreed data.
We also recommend that all regulators should also specifically include the clinical status of registrants i.e. clinically active or not.
In addition, it is important to obtain better information on the geographical and longitudinal migration of doctors. This could be achieved by ensuring a unique identifier for each individual member of a royal college or professional body (e.g. GMC or NMC number) as well as employer information, which could be reported and triangulated.
It would be important to keep this information up-to-date, to ensure information about movement to different roles and retirement is captured. We suggest
agreement will be needed on the frequency of collecting and reviewing this data. It would also be important to make sure that this data is fully available, securely and safely, to the relevant organisations for planning and reporting purposes.
The DH and GMC have work in progress that will allow improved forecasts of trainee attrition, recruitment and specialty training choices. The improvement of medical workforce planning is also being considered by the Joint Working Group for Specialty Training Numbers (JWG) through a commission to review local and national
information sources in England. The review will recommend a way to use the evidence and data available to the JWG to improve system wide intelligence.
4. Improved access to raw data and information to enable analysis and benchmarking
The CfWI recommends that the following measures are adopted to improve transparency and access to key information:
• Organisations which collect and/or hold data to develop data sharing protocols which will allow the safe, secure and responsible sharing of anonymised data in a fast and efficient manner. This should include open publication and linkage of
specified data sets to facilitate greater transparency in the context of the review of information protection and sharing being led by Dame Fiona Caldicott1. • Continued support to keep the information architecture mapping up to date,
including contributing to the HSCIC ‘inventory of the wealth of data collected by other parts of the health and social care system’2
• Links to workforce-related data sources could be included in the Department of Health’s proposed comprehensive online ‘portal’3. This may also be the
appropriate central repository for different benchmarks such as clinician: population ratios for all professions where available.
• The NMDS-SC database to be made available to workforce planners in health care
services to enable workforce commissioning across local authority and
commissioning group areas. This could be through a network of authorised users with an understanding of how the data has been collected, defined and analysed so that it can be applied to their particular area or issue.
• A method should be established to link training status deanery data to the wider system workforce information as deaneries do not have access to ESR. This should create a consistent dataset across regions and allow comparison with other workforce datasets.
1
http://www.dh.gov.uk/health/2012/02/dame-fiona-caldicott-to-lead-confidentiality-review/
2
Department of Health, ‘The Power of Information’, June 2012, page 99. URL: http://informationstrategy.dh.gov.uk/
3
6
CONCLUSIONS
The CfWI WIA project and development of the workforce information signposting tool has established that:
• There is an appetite within the workforce planning and education
commissioning community for practical tools and products which signpost users from health and social care organisations to reliable sources of data, information and intelligence.
• The WIA signposting tool which has been developed meets the most critical stakeholder requirements and a key benefit of the Excel tool is the ability to search, sort and filter by multiple parameters to find the most appropriate sources available. This would not have been available through the interactive PDF originally commissioned.
• User-testing of the signposting tool will be essential to gather feedback on functionality and content and inform any further development, for example:
o Indicating whether sources include information which could help to track the movement of health professionals.
o Adapting the language and terminology to make the tool more
appropriate for a wider audience.
o Improving the functionality and user experience.
• A web-based tool could offer some additional benefits including access to a single updated live version of the tool, providing statistics on use of the tool and the capability to review the most popular searches. There is also potential to include user feedback on specific sources to maximise shared learning across the system. A detailed assessment of the benefits and investment will be necessary to inform future decisions on further development of the tool. • A comprehensive communications and marketing plan will be put in place to
ensure a wide range of strategic and operational bodies have an awareness of the signposting tool, its benefits and any future developments.
• There is a need for continued improvement to the quality and consistency of information available to workforce planners and education commissioners. There are a number of initiatives already being progressed by the DH and HEE to address these issues and support the emerging LETBs.
It is essential that during and beyond transition to the new system, national and regional organisations continue to work together to improve the quality and availability of information which supports health and social care workforce planning at all levels.
ANNEX 1 CONTRIBUTORS
Name Title and organisation
Kate Anderson Chair of the Social Services User Service Group
The Health and Social Care Information Centre
David Bennett Workforce Information Architecture Workstream Manager, DH
Jonathan Booker Head of Workforce Intelligence and Modernisation
Leeds Teaching Hospitals NHS Trust Dale Brown Senior Workforce Analyst
Lancashire Care NHS Foundation Trust Ian Bullard Workforce Section Head
The Health and Social Care Information Centre
Mike Burgess Assistant Director Workforce Strategy NHS North West SHA
Nigel Burgess Workforce and Education Commissioning Strategy Manager,
Guys and St Thomas Hospitals NHS Foundation Trust
Damian Byrne Head of Workforce Planning & Resourcing 5 Boroughs Partnership NHS Foundation Trust
Duncan Campbell Senior Information Analyst London SHA
Tracey Carstairs Education Commissioning and Contract Manager
East Midlands SHA
Nancy Cooke Strategic Workforce Development Manager East Midlands SHA
Mary Currie Associate Director: Workforce Planning Kings Hospital Foundation Trust Liz Edelman Head of Leadership & Workforce
Outer North East London NHS Trust Wendy Egerton Head of Workforce Information, Planning
and Assurance DH
Jacqui Ellis Head of Workforce and Development NAViGO Health and Social Care Community Interest Company
Michelle Featherstone Workforce Manager
Central Manchester University Hospitals NHS Foundation Trust
Joan Fletcher DH
David Foster Deputy Chief Nursing Officer, Department of Health
Professor Simon Gregory Post Graduate Dean
NHS East of England Multi-Professional Deanery
David Griffiths Workforce Intelligence Project Manager (Analysis)
Skills for Care Alastair Henderson Chief Executive
Academy of Medical Royal Colleges
Lisa Hughes Co-Chair, National Allied Health Professional Advisory Board, DH
Shereen Hussein Senior Research Fellow
Social Care Workforce Research Unit King's College London
Dr Keith Ison Head of Medical Physics, Guy's and St Thomas' NHS Foundation Trust
Zoe Johnston Adults & Joint Commissioning Adult Social Care & Health
Bracknell Forest Council
Andrew Jones Associate Director of HR & Workforce East Cheshire NHS Trust
Kathryn Jones Workforce Planning & Transformation Manager
Bridgewater Community Healthcare NHS Trust
National Care Forum
Jonathan King Senior Workforce Information Analyst East Midlands SHA
Trish Knight Deputy Director of Workforce East Midlands SHA
Mary Lewis Strategic Workforce Planner South Central SHA
Jackie Livesey Strategic Workforce Planning Manager Pennine Acute Hospitals NHS Trust Derek Marshall Head of Workforce Intelligence
North East SHA
Joanne Marvell Transition Programme Manager NHS Equality and Adult Social Care, DH Patrick Mitchell Director of National Programmes – Medical
Education DH
Nigel Moloney Bolton NHS Foundation Trust
Peter Nightingale President, Royal College of Anaesthetists Paul Niblett Social Care Dissemination Section Head
The Health and Social Care Information Centre
Tony Overd Head of Workforce Intelligence South West SHA
Adrian Price Workforce Lead Staff Survey Department of Health Mike Purvis Postgraduate GP Dean
Yorkshire and the Humber SHA Saba Razaq Workforce Analyst
North West SHA
Professor David Sowden Director Medical Education (England) Medical Education England
Liz Thomas Senior Workforce Analyst North West SHA
Ian Thornber Sector Head, Primary Care Workforce, The Health and Social Care Information Centre
Learn to Care
Ian Wheeler Head of Research and LMI Skills for Health
Adrian Whittle Head of Human Resources and Organisational Development
Cambridgeshire and Peterborough County Workforce Group
Simon Williams Information Analyst Hampshire County Council
DISCLAIMER
The Centre for Workforce Intelligence (CfWI) is an independent agency working on specific projects
for the Department of Health and is an operating unit within Mouchel Management Consulting Limited.
This report is prepared solely for the Department of Health by Mouchel Management Consulting Limited, in its role as operator of the CfWI, for the purpose identified in the report. It may not be used or relied on by any other person, or by the Department of Health in relation to any other matters not covered specifically by the scope of this report.
Mouchel Management Consulting Ltd has exercised reasonable skill, care and diligence in the compilation of the report and Mouchel Management Consulting Ltd only liability shall be to the Department of Health and only to the extent that it has failed to exercise reasonable skill, care and diligence. Any publication or public dissemination of this report, including the publication of the report on the CfWI website or otherwise, is for information purposes only and cannot be relied upon by any other person.
In producing the report, Mouchel Management Consulting Ltd obtains and uses information and data from third party sources and cannot guarantee the accuracy of such data. The report also contains projections, which are subjective in nature and constitute Mouchel Management Consulting Ltd's opinion as to likely future trends or events based on i) the information known to Mouchel
Management Consulting Ltd at the time the report was prepared; and ii) the data that it has collected from third parties.
Other than exercising reasonable skill, care and diligence in the preparation of this report, Mouchel Management Consulting Ltd does not provide any other warranty whatsoever in relation to the report, whether express or implied, including in relation to the accuracy of any third party data used by Mouchel Management Consulting Ltd in the report and in relation to the accuracy, completeness or fitness for any particular purposes of any projections contained within the report.
Mouchel Management Consulting Ltd shall not be liable to any person in contract, tort (including negligence), or otherwise for any damage or loss whatsoever which may arise either directly or indirectly, including in relation to any errors in forecasts, speculations or analyses, or in relation to the use of third party information or data in this report. For the avoidance of doubt, nothing in this disclaimer shall be construed so as to exclude Mouchel Management Consulting Ltd’s liability for fraud or fraudulent misrepresentation.
www.cfwi.org.uk
The Centre for Workforce Intelligence produces quality intelligence to inform better workforce planning that improves people’s lives