INSTRUMENTAL VARIABLE METHODS IN THE COMPARATIVE EFFECTIVENESS OF OSTEOPOROSIS MEDICATIONS IN POST-MENOPAUSAL OSTEOPOROSIS WOMEN
Jane Susan Der
A dissertation submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Epidemiology in the
Gillings School of Global Public Health.
Chapel Hill 2019
iii ABSTRACT
Jane Susan Der: Instrumental Variable Methods in the Comparative Effectiveness of Osteoporosis Medications in Post-menopausal Osteoporosis Women
(Under the direction of M. Alan Brookhart)
Background: Safety warnings from the Food and Drug Administration regarding long-term use of bisphosphonates (BP) have led to increasing interest in the comparative effectiveness of osteoporosis (OP) medications. Studying post-menopausal women, a population at high risk for developing OP, in healthcare claims databases is valuable but confounding by indication is a concern. Instrumental variable (IV) methods may control for unmeasured confounding. Identifying the prescribing physician in
databases may be essential but often there is no consistent physician identifier (ID) available.
Methods: Women 55+ initiating a BP or other OP medication were identified in the United Healthcare (UH) database (2008-2011) and followed for incident osteoporotic fracture (Fx). IVs were defined by the prescribing physician’s preference (IV=BP vs. Other OP) determined by the most recent prior prescription (Rx) (Day_IV) and all Rxs in the previous year (Year_IV). Using the two-stage IV framework, we computed differences in risk of osteoporotic Fx divided by IV strength between medication groups (IV estimator). We developed a gold standard measure for the co-occurrence between two physician IDs. We used regression models to evaluate the association between characteristics of outpatient claims and the probability that the provider was the prescriber on a proximal pharmacy claim.
Results: The strength of Day_IV was 0.15 (0.14, 0.16). Imbalances in confounders between treatment groups were slightly improved by the IV. The strength of the IV varied moderately over a few covariates. Analyses for Year_IV yielded similar results. IV estimator values ranged from -1.66 to 1.29 and all 95% confidence intervals included 0. Family and general practitioner, hospitalist, and OP
iv
Conclusions: The analysis does not allow us to rule out a substantial difference between BP and other OP groups. Our algorithms were good at identifying matches for the prescribing physician
v
For my mother and father who have loved and supported me through the years. And for my brother, who always appreciated the best in me and who continues to inspire me to live, to love, and to make a
vi
ACKNOWLEDGEMENTS
I would like to express my deepest gratitude to my doctoral advisor, Alan Brookhart, for his steadfast mentorship and for being a model of the kind of dynamic scholar and leader I aspire to become. I am thankful for the times when he challenged me and for when he encouraged me as well. With his guidance, I have grown considerably as a professional and as a person.
I am also sincerely grateful to the rest of my committee - Charlie Poole, Gary Koch, Jenny Lund, and Margaret Gourlay - who have each mentored me in their own ways. I am appreciative of the long
conversations and the honest advice. I would like to give special thanks to Charlie for graciously stepping in as my dissertation chair when we needed him. And especially I want to thank Dr. Koch, who has guided me throughout my program and whose extraordinary scholarship and caring mentorship have been inspiring. I am honored to have received his scholarship and to be counted as a student of the Biostatistics Consulting Lab.
I also would like to acknowledge financial support (I.e., stipend and research support for dissertation) from Amgen, Inc. It was during an internship with the company, when I worked with Fei Xue and Cathy Critchlow, that some of the ideas for this dissertation work were started.
vii
I am also incredibly grateful to Dr. Daniel Clarke-Pearson and the team of doctors and nurses at UNC Hospital and Dr. T.G. at Duke for all of their help and my prayers go out to all of the patients who are hoping for another day.
viii
TABLE OF CONTENTS
LIST OF TABLES ……….………… xi
LIST OF FIGURES ………..……… xiii
LIST OF ABBREVIATIONS ……… xiv
CHAPTER I. INTRODUCTION AND SPECIFIC AIMS ……… 1
A. Introduction ……… 1
B. Statement of Specific Aims ……….………… 2
References ……….……… 4
CHAPTER II. REVIEW OF THE LITERATURE ……… 6
A. Overview of osteoporosis ……… 6
B. Osteoporosis medications ………...…… 9
i. Bisphosphonates ………..………… 10
ii. Other osteoporosis medications ……… 12
C. Safety of bisphosphonates ……… 17
D. Comparative effectiveness of osteoporosis medications ……….……… 17
i. Clinical trials ………..……… 17
ii. Observational studies ………..……… 18
E. Instrumental variable methods ………...……….….……… 19
References ………..……… 22
CHAPTER III. METHODS ………...………… 27
A. Study population ……….……… 27
B. Data sources ………...……… 28
C. Study design ……… 28
D. Significance and innovation ………..……… 28
ix
F. Independent variable definitions ………..… 30
G. Statistical analysis for Aim 1 ……….……… 32
H. Statistical analysis for Aim 2 ……….…… 33
I. Statistical analysis for Aim 3 ……….……… 35
References ………..……… 37
CHAPTER IV. RESULTS: Identifying the Prescribing Physician in U.S. Healthcare Claims data …. 38 A. Introduction ………..… 38
B. Methods ……… 39
C. Results ………..… 41
D. Discussion ……… 43
E. Tables and figures ………..…… 45
References ………..……… 50
CHAPTER V. RESULTS: Preference-based Instrumental Variable Methods in Comparative Effectiveness Analyses of Osteoporosis Medications in Women with Postmenopausal Osteoporosis ………..……….… 52
A. Introduction ………..……… 52
B. Methods ……… 54
C. Results ………..……… 58
D. Discussion ……… 59
E. Tables and figures ………..……… 64
References ………..……… 75
CHAPTER VI. RESULTS: Time-to-event analysis of osteoporotic fracture using two-stage Instrumental Variable approach ……….….…….. 78
A. Introduction ………...………...…… 78
B. Methods ……… 79
C. Results ………..……… 81
D. Discussion ……… 82
E. Tables and figures ………..…… 83
x
CHAPTER VII. DISCUSSION ………..……… 92
A. Summary of findings ……...……….……… 92
B. Public Health Implications ………..……….…… 94
C. Strengths ……… 96
D. Limitations ………..……… 97
E. Future directions ………...……… 98
F. Conclusions ………...……… 99
References ……….………...……… 101
xi
LIST OF TABLES
Table 2.1. Summary of commonly prescribed bisphosphonates which are used
to treat osteoporosis ……….. 14 Table 2.2. Summary of commonly prescribed other osteoporosis medications
(non-bisphosphonates) which are used to treat osteoporosis ……….… 15
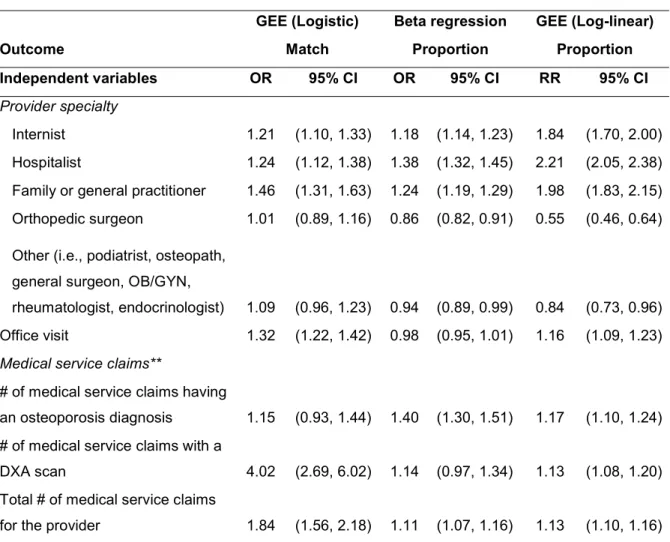
Table 4.1. Odds ratios from generalized estimating equation (GEE) logistic model and beta regression and relative risk estimates from GEE log-linear
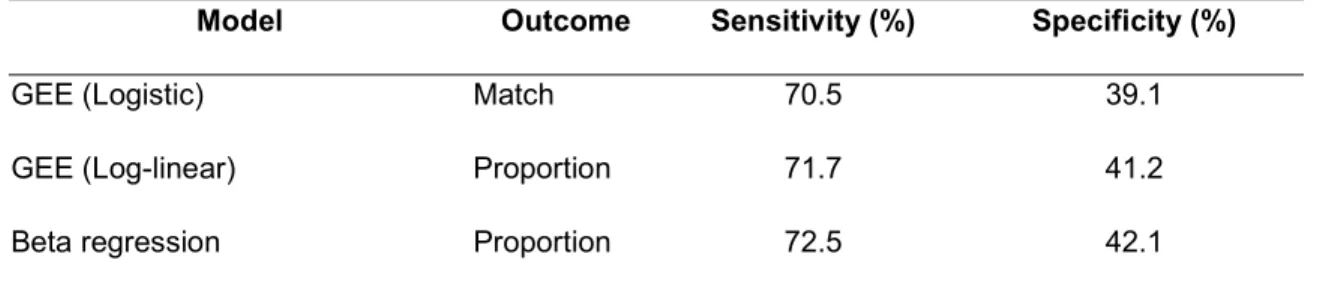
model ……….… 48 Table 4.2. The sensitivity and specificity of the generalized estimating equation
(GEE) logistic and log-linear models and the beta regression model ……….…… 49 Table 5.1. Prevalence of diagnoses, medication prescriptions, and conditions
of the Charlson Comorbidity Score among treatment and instrumental variable (Day IV) groups during the baseline period of 12 months prior to the
index date……….………...………….. 65 Table 5.2. Incidence rates and incidence rate ratios of osteoporotic fracture for
treatment and instrumental variable (Day IV) groups ……… 67 Table 5.3. Heterogeneity of treatment effect: instrument strength of physician
preference IV based on most recent prior new prescription (Day IV) in strata defined by the presence of medical conditions or prescriptions assessed during the baseline period (i.e., 12-month period prior to the index date) and by the
Charlson Comorbidity score ………..……… 68 Table 5.4. Prevalence of diagnoses, medication prescriptions, and conditions
of the Charlson Comorbidity Score among treatment and instrumental variable (Year IV) groups during the baseline period of 12 months prior to the index
date ………..……….. 70 Table 5.5. Incidence rates and incidence rate ratios of osteoporotic fracture for
treatment and instrumental variable (Year IV) groups ………...…… 72 Table 5.6. Heterogeneity of treatment effect: instrument strength of physician
preference IV based on most recent prior new prescription (Year IV) in strata defined by the presence of medical conditions or prescriptions assessed during the baseline period (i.e., 12-month period prior to the index date) and by the
Charlson Comorbidity score ………..……… 73
Table 6.1. Prevalence of diagnoses, medication prescriptions, and conditions of the Charlson Comorbidity Score among treatment groups during the
baseline period of 12 months prior to the index date with calculated prevalence
differences and 95% confidence intervals ………...……… 85 Table 6.2. Prevalence of diagnoses, medication prescriptions, and conditions
of the Charlson Comorbidity Score among instrumental variable (IV) groups
xii
Table 6.3. Number of fractures, risk of fracture (95% CI), difference in risk of fracture between IV (instrumental variable) groups (95% CI) by IV group, and difference in risk of fracture between IV groups divided by IV strength (95% CI)
for each IV at 1, 2, and 3 years after the index date ………..… 89 Table A (Appendix). Osteoporosis Diagnosis and Medication Codes and Case
Algorithm ……….……… 103 Table B (Appendix). Diagnosis Codes and Algorithm for Osteoporotic
xiii
LIST OF FIGURES
Figure 2.1. Directed acyclic graph of IV, treatment, confounders and outcome
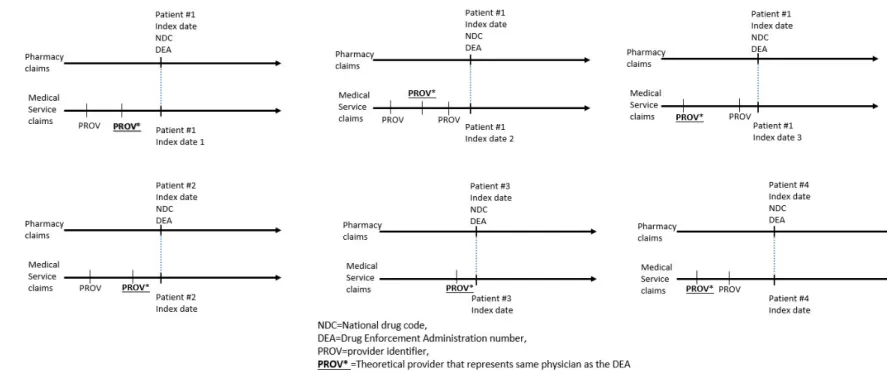
illustrating the main assumptions of IV methods ……… 20 Figure 4.1. The “proportion” statistic ………..……….……… 45 Figure 4.2. Pharmacy and medical service claims in administrative healthcare
claims databases ………...………..……… 46 Figure 4.3. The match between the provider identifier (ID) and Drug
Enforcement Administration number (DEA) variable in the United
Healthcare database ……….………….. 47 Figure 5.1. Physician preference instrumental variables (IVs) constructed in
the United Healthcare database ……… 64 Figure 6.1. Cumulative risk of fracture for Day IV (instrumental variable), Year IV,
Day IV without refills, and Year IV without refills by IV group (i.e., BP, other OP) ………...…… 83 Figure 6.2. Cumulative risk of fracture by index drug (i.e., bisphosphonate,
other OP (osteoporosis) medication ……….……… 84
xiv
LIST OF ABBREVIATIONS
AHFS American Hospital Formulary Service BMI body mass index
BP(s) bisphosphonate(s) CI confidence interval
DEA(s) Drug Enforcement Administration number(s) DXA dual energy x-ray absorptiometry
ER emergency room
FDA Food and Drug Administration Fx(s) fracture(s)
GEE generalized estimating equation GLM generalized linear model
HCPCS Healthcare Common Procedure Coding System ID(s) identifier(s)
ICD International Classification of Diseases IRR incidence rate ratio
IV(s) instrumental variable(s) NDC(s) National Drug Code(s) OB/GYN obstetrician/gynecologist OLS ordinary least squares OP osteoporosis
PDR prevalence difference ratio PM post-menopausal
PMO post-menopausal osteoporosis Rx(s) prescription(s)
1
CHAPTER I. INTRODUCTION AND SPECIFIC AIMS
A. Introduction
Osteoporosis (OP) is a disease characterized by reduced bone mineral density, deterioration of bone microarchitecture, and an increased risk of fracture (Fx).1 Currently, approximately 8 million women and 2 million men in the United States (US) have OP2 and the incidence of OP is projected to increase in coming decades.3 Osteoporotic Fxs, particularly of the vertebrae and hip, are associated with prolonged disability and an increased risk of death. Post-menopausal (PM) women are especially at risk for
developing OP4 and it is estimated that 30% of these women have OP (PMO);5 40% of PMO women will experience one or more osteoporotic Fxs in their remaining lifetime.6
2 B. Statement of Specific Aims
None of the commonly used confounding-adjustment methods, such as stratification, covariate adjustment, weighting, propensity score methods, and inverse probability treatment weighting adjust for unmeasured confounding. IV analysis is a method of controlling for unmeasured confounding in observational studies. These methods have been widely used in econometrics9 and are becoming increasingly used in pharmacoepidemiologic research. Previous IV studies in pharmacoepidemiology have used geographic location,10 history of comorbidity or co-prescriptions,11,12 hospitals classified by availability of technology,13 facility-level dosing practice,14 physician preference15, 16, 17 and calendar time18, 19 as instruments. Because the OP medications differ greatly in their route and frequency of administration and are associated with different potential adverse events, and received FDA approval at different times it is likely that physicians have preferences for OP medications (i.e., beyond formulary choices), making physician preference a viable instrument in studies of the comparative effectiveness of OP medications.
AIM 1: In databases with access to data from health maintenance organizations and private medical practices, develop methods to identify the physician responsible for prescribing the OP medication to patients in the PMO cohort.
1. In the UH database, assess the use of the Drug Enforcement Administration number (DEA) in the pharmacy claims and provider ID (PROV) in medical service claims to identify the prescribing physician for the analyses.
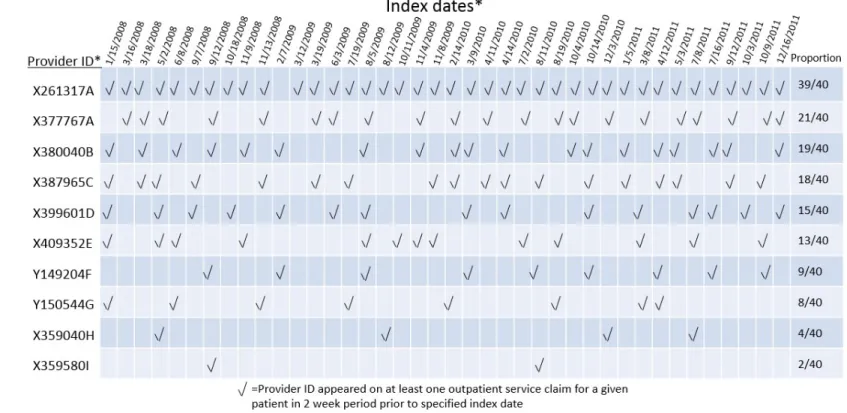
2. Link outpatient service claims to pharmacy claims data to evaluate the co-occurrence of provider ID in medical service claims with DEA in pharmacy claims. Compute a “gold standard” proportion as the number of times a provider ID appears at least once in medical service claims in the two weeks prior to a new OP Rx as appearing in pharmacy claims for each DEA associated with our PMO cohort.
3. Construct predictive models using generalized estimating equation (GEE) logistic and log-linear models and beta regression with characteristics of the medical service claims with the outcome of the proportion “gold standard” statistic.
3
AIM 2: Evaluate the assumptions of the IV methods in the comparative effectiveness of BPs (alendronate, ibandronate, risedronate, zoledronic acid) versus other OP medications (teraparatide, calcitonin, raloxifene) in reducing the risk of OP Fxs (I.e., fragility Fxs) in PMO women. Assumptions: (1) The IV is associated with the treatment received, (2) Covariate values do not differ by the level of IV (independence assumption), and (3) The IV does not predict the outcome except through its influence on the treatment (exclusion restriction). An additional consideration is to test for the heterogeneity (or monotonicity) of treatment effect since the IV analysis may be biased if the instrument strength differs by covariate strata. Evaluate different ways of identifying preference (i.e., last prescription [Rx] or proportion of recent Rxs) of each IV with respect to how strongly the IVs are associated with treatment and balance covariates.
1. In the United Healthcare (UH) database, construct the preference instrument. Obtain the prescribing history for each physician or provider associated with the cohort. Construct physician
preference instruments based on the last Rx or the proportion of Rxs in the year prior to the index date of each patient for BPs or other OP medications.
2. Evaluate the assumptions of the IVs.
3. Evaluate the heterogeneity of treatment effect.
AIM 3: Apply the IV methods using a two-stage approach to estimate the effect of the treatment of BP versus other OP medications on osteoporotic Fxs using time-to-event analyses in the UH database.
1. Construct Kaplan Meier models to obtain estimates of the survival and hazard functions for the treatment groups and physician/provider preference instrument groups.
2. To compute the IV estimate, use Kaplan Meier estimates to calculate the risk difference between IV groups (numerator) and scale this by the difference in the expected value of exposure in the IV groups (denominator). Compare IV estimates to differences in risk between treatment groups.
3. Compute risk of Fx at 1, 2, and 3 year time points for IV and treatment groups.
4 REFERENCES
1. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis Prevention, Diagnosis, and Therapy. J Am Med Assoc. 2001;285:785-95.
2. Reginster JY. Burlet N. Osteoporosis: A still increasing prevalence. Bone. 2006;38: S4-S9. 3. Gullberg B, Johnell O, Kanis JA. Worldwide projections for hip fracture. Osteoporosis Int. 1997;7:407-13.
4. National Osteoporosis Foundation. Fast facts on osteoporosis. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm . Accessed on 31 August 2010.
5. Melton III LJ, Chrischilles EA, Cooper C, Lane AW, Riggs BL: Perspective: How many women have osteoporosis? J Bone Miner Res. 1992;7:1005-10.
6. Randell A, Sambrook PN, Nguyen TV, Lapsey H, Jones G, Kelly PJ, Eisman JA. Direct clinical and welfare costs of osteoporotic fractures in elderly men and women. Osteoporosis Int. 1995;5:427-32. 7. Whitaker M, Guo J, Kehoe T, Benson G. Bisphosphonates for Osteoporosis – Where do we go from here? N Engl J Med. 2012; 366:2048-2051.
8. Yasothan U, Kar S. Osteoporosis: overview and pipeline. Nature Reviews Drug Discovery. 2008; 7, 725-726.
9. Sargan JD. The estimation of economic relationships using instrumental variables. Econometrica. Jul 1958; 26(3):393-415.
10. Earle CC, Tsai JS, Gelber RD, Weinstein MC, Neumann PJ, Weeks JC. Effectiveness of
chemotherapy for advanced lung cancer in the elderly: instrumental variable and propensity analysis. J of Clinical Oncology. Feb 15 2001; 19(4):1064-1070.
11. Groenwold RHH, Hak E, Klungel OH, Hoes AW. Instrumental variables in influenza vaccination studies: mission impossible?! Value in Health. 2010; 13(1): 132-7.
12. Yoo BK, Frick KD. The instrumental variable method to study self-selection mechanism: a case of influenza vaccination. Value in Health. 2006; 9(2): 114-122.
13. McClellan M, McNeil BJ, Newhouse JP. Does more intensive treatment of acute myocardial infarction in the elderly reduce mortality? Analysis using instrumental variables. 1994; 272(11):859-866. 14. Bradbury BD, Brookhart MA, Winkelmayer WC, Critchlow CW, Kilpatrick RD, Joffe MM, Feldman HI, Acquavella JF, Wang O, Rothman KJ. Evolving Statistical Methods to Facilitate Evaluation of the Causal Association Between Erythropoiesis-Stimulating Agent Dose and Mortality in Nonexperimental Research: Strengths and Limitations. American J of Kidney Disease. 2009; 54(3): 554-560.
15. Brookhart MA, Rassen JA, Wang PS, Dormuth C, Mogun H, Schneeweiss S. Evaluating the validity of an instrumental variable study of neuroleptics. Med Care. 2007; 45:S116-S122.
5
17. Brookhart MA, Wang PS, Solomon DH, Schneeweiss S. Evaluating short-term drug effects using a physician-specific prescribing preference as an instrumental variable. Epidemiology. May 2006; 17(3): 1-8.
18. Mack CD, Brookhart MA, Glynn RJ, et al. Comparative Effectiveness of Oxaliplatin Versus 5-flourouricil in Older Adults: An Instrumental Variable Analysis. Epidemiology. 2015;26(5):690–699. 19. Gokhale, M, Buse, JB, DeFilippo Mack, C, et al. Calendar time as an instrumental variable in assessing the risk of heart failure with antihyperglycemic drugs. Pharmacoepidemiol Drug
6
CHAPTER II. REVIEW OF THE LITERATURE
A. Overview of osteoporosis
OP is a disease characterized by reduced bone mineral density, deterioration of bone
microarchitecture, and an increased risk of Fx.1 Osteoporosis is considered a “silent epidemic”2 because there are usually no clinical symptoms until a bone Fxs. Currently, approximately 8 million women and 2 million men in the US have OP3 and the incidence of OP is projected to increase in coming decades.4 Osteoporotic Fxs, particularly of the vertebrae and hip, are associated with prolonged disability and an increased risk of death. PM women are especially at risk for developing OP5 and it is estimated that 15.5% (age-adjusted) of US PM women aged 50 and older have OP (PMO) at the femoral neck or lumbar spine, with variation by race/ethnicity;3 40% of PMO women will experience one or more osteoporotic Fxs in their remaining lifetime.5 According to 1995 US estimates, 52% of women aged 80 and older had femoral neck OP. Because of the high cumulative rate of Fxs6 and devastating effects of the disease, OP is a significant public health issue.
The identified safety concerns of BPs7, 8 (e.g., osteonecrosis of the jaw) combined with the introduction of new OP medications9 in recent years have led to increasing interest in assessment of the risk-benefit profile of OP medications among clinicians, patients, the pharmaceutical industry, and regulatory agencies. Few head-to-head clinical trials comparing the relative effectiveness of these drugs have been conducted.10--14 In addition, only a small number of observational studies have directly compared different OP drugs in their effect on Fx risk or other outcomes.15-18 A major limitation of these studies particularly those based on claims or administrative databases, is that important potential confounders, such as bone mineral density, BMI, physical activity, family history of OP and frailty, were not available for analyses.
7
studies of intended drug effects because prescribers’ choice of treatment is likely influenced by the anticipated treatment effect. In addition, when these studies are conducted in administrative insurance claims databases, important potential confounders such as lifestyle factors (e.g., diet, smoking), laboratory test results, and other clinical measurements are often missing or unmeasured. Commonly used methods to adjust for confounding such as covariate adjustment, stratification, weighting, propensity score methods, and inverse probability treatment weighting address confounding by measured variables. IV methods, which have been widely used in econometrics, have been proposed as an innovative
approach to adjust for unmeasured confounding.20 A valid IV is predictive of treatment but not related to the outcome under study except through its effect on treatment. Prior pharmacoepidemiologic studies using IV methods based on administrative databases have used a variety of co-prescriptions,
comorbidities, and other variables as instruments.21-27
IV methods may control for unmeasured confounders but have yet to be applied to the study of comparative effectiveness of OP medications. The decision to prescribe one OP drug over another may depend on a variety of factors such as convenience, drug tolerance, and adherence to dosing
schedules.28-29 Because of these reasons and beyond formulary choices, it is likely that physicians would differ in their Rx preferences for OP medications and hence physician preference for prescribing BP versus other OP medications may be a potential IV. The current project proposed to construct an IV based on physician preference for prescribing BP versus other OP drugs and to evaluate the
assumptions of the IV method in assessing the potential effect of these drugs on risk of osteoporotic Fx in women with postmenopausal osteoporosis (PMO). IV methods were then be applied to time-to-event analyses to compare the effectiveness of BP with other OP medications on osteoporotic Fxs.
Osteoporosis and osteoporotic fractures
Osteoporosis is a disease characterized by low bone mass and deterioration of bone
microarchitecture which may result in an increase in bone fragility and susceptibility to Fx.6 It is estimated that among Caucasians, 50% of women and 20% of men 50 years of age or older will have an
8
Studies have shown that the effect of OP on the skeleton is systemic and that individuals who experience a Fx are more likely to experience another Fx at the same or different sites; in addition, adults with low bone density have a higher risk of sustaining any type of Fx.32 PM women are especially at risk for developing OP5 because the rate of bone loss usually increases at menopause due to a decline in sex hormone production, especially when a lifestyle that is conducive to bone health is not practiced;32-34 40% of PMO women will experience one or more osteoporotic Fxs in their remaining lifetime.4
Osteoporotic, or fragility, Fxs occur from standing height or less and is not the result of a major trauma (e.g., car accident). Hip and spine Fxs are estimated to increase mortality by 10 to 20 percent over the subsequent 6 months.35-36 In addition, Fxs may lead to loss of independence, limited ability to walk, chronic pain, and depression.37-38 In the US, the lifetime risk of a hip, spine, or forearm Fx at the age of 50 years is 40% in women and 13% in men.39 In 2000, 1.6, 1.4, and 1.7 million Fxs for the hip, vertebrae, and forearm were estimated to have occurred worldwide.39 Furthermore, researchers have found that the risk of death is increased in patients who experience osteoporotic Fxs, especially
immediately after the occurrence of the Fx;40 the increase in mortality risk may be related to comorbidities and causally to deaths. The annual costs of all osteoporotic Fxs are approximately $20 billion in the U.S. and about $30 billion in Europe.32
Factors which contribute to bone strength are bone mineral density (BMD), bone size and shape, microarchitecture, the rate of bone turnover, and degree of mineralization.41 Fx risks increases with decreasing BMD. Other factors that contribute to the risk of Fx include previous Fxs, falls, treatment with glucocorticoid, age, sex, BMI, family history, smoking, heavy alcohol use and rheumatoid arthritis.42-44
9 B. Osteoporosis medications
Treatment choices for osteoporosis
A clinician’s decision regarding which treatment to give postmenopausal women for the treatment of OP may be based on the patient’s risk of Fx,48 the efficacy and potential side-effects of the medications to be prescribed, the patient’s severity of disease, age, gender, tolerance, and preferences.49 Treatment choice may also be affected by the patient’s kidney functioning, other risk factors, and reimbursement issues.32 Bisphosphonates are often the first choice for the treatment of OP because several formulations have been shown in randomized trials to prevent both vertebral and non-vertebral Fxs and because insurers commonly require intolerance or failure of prior BP treatment before approval of alternative medications. However, a variety of OP medications, with different mechanisms of action and formulations, are available as treatment options for OP.
The Bone Remodeling Cycle
Bone renews and changes constantly in the bone remodeling cycle that lasts approximately 6 months. Bone remodeling occurs in two stages: (1) resorption, where bone is broken down or removed and cells called osteoclasts dissolve bone tissue and create small cavities and (2) formation, where cells called osteoblasts fill the cavities left by resorption with new bone tissue. In normal bone, resorption and formation occur in sequence and are balanced. However, during menopause in women and aging in both men and women, the bone remodeling cycle may become imbalanced, resulting in bone loss and
eventually this may lead to OP and Fxs.32, 50
Antiresorptive and Anabolic Drugs
10
Teriparatide, an anabolic drug, increases the rate of formation of bone and is in a category of its own among OP medications. It is the only OP medicine approved by the FDA which rebuilds bone.32 BP therapy is a required follow-up to teriparatide in order that anabolic bone density gains be maintained.
i. Bisphosphonates
BPs are the most commonly prescribed medications used to treat OP and similar diseases. These drugs slow bone loss by inhibiting the osteoclasts which break down bone. In addition to treating OP, BPs are also used in the treatment of osteitis deformans (Paget’s disease of the bone), metastasis of the bone, multiple myeloma and other diseases where bones have become fragile.32
Alendronate and risedronate are the most commonly prescribed BPs for the first-line treatment of OP.5 Nitrogen-containing oral BPs, which are currently the most widely used medications in the treatment of OP, are excreted by the kidney and are not recommended by the US FDA for the treatment of OP in patients with stage 4 to 5 chronic kidney disease.
Alendronate Sodium or Alendronate Sodium plus Vitamin D3 (Fosamax or Fosamax Plus D)
Alendronate is approved for the treatment and prevention of OP in PMO women and for the treatment of OP in men. It may also be used to treat glucocorticoid-induced OP, caused by long-term use of steroids, in men and women. Alendronate reduced the loss of bone, increases bone density and has been shown to reduce the risk of hip, spine and other Fxs by approximately 50 % over two to four years.5 Alendronate may be taken daily as a 5 mg tablet or weekly as a 35 mg tablet for prevention. It is taken daily as a 10 mg tablet or weekly as a 70 mg tablet (with or without vitamin D) for treatment.32 Generic alendronate became available in 2008, which may have prompted a surge in Rxs for the drug.
Ibandronate sodium (Boniva)
11
injection of 3 mg every three months by a healthcare professional during an office visit or in other outpatient settings. A daily dose has been approved by the FDA but it is not available in the US.5, 32
Risedronate Sodium or Risedronate Sodium with Calcium Carbonate (Actonel, Actonel with
Calcium and Atelvia)
Risedronate has been approved for the treatment and prevention of OP in PMO women and for the treatment of OP in men. Also, it may be used for the treatment and prevention of glucocorticoid-induced OP in women and men. Risedronate has been shown to reduce the risk of hip and vertebral Fxs by 35 to 45 % over three years. For treatment or prevention, risedronate is taken daily as a 5 mg tablet, weekly as a 35 mg tablet (with or without separate calcium carbonate tablets), twice monthly as a 75 mg tablet (on two days consecutively) or as a 150 mg tablet monthly.5, 32
Zoledronic Acid (Reclast)
Zoledronic acid has been approved for the treatment and prevention of OP in postmenopausal women. It may also be used to increase bone mass in men with OP, to prevent new clinical Fxs in patients with low-trauma hip Fx, and to treat or prevent glucocorticoid-induced OP in women and men.
Zoledronic acid increases bone density and reduces hip, spine, and non-spine Fxs. In one study, zoledronic acid reduced the risk of spine and hip Fxs by 70% and 41%, respectively.5 It has also been shown to reduce the risk additional Fxs in people who have recently had a hip Fx. Zoledronic acid as an IV infusion yearly to treat OP or every two years to prevent OP. Zoledronic acid is delivered in a 5 mg dose in a physician’s office or other outpatient setting.
12 ii. Other osteoporosis medications
Calcitonin (Fortical)
Calcitonin is a hormone involved in the regulation of calcium and metabolism of bone. It is used for treating OP in PMO women who are five or more years beyond menopause. Calcitonin slows the loss of bone and has been shown to reduce the risk of Fxs in the spine but not in other bones. It is delivered by nasal spray (200 IU daily) or injection (varied dosages).5,32 Although intranasal calcitonin has been approved by the FDA for the treatment of postmenopausal OP since 1995, trial data supporting its ability to reduce fracture is lacking. In March 2014, the FDA added new warnings and precautions to the calcitonin label regarding a possible associated increased risk of malignancy.
Raloxifene (Evista)
Raloxifene has been approved for the treatment and prevention of OP in PMO women. It is neither a hormone or an estrogen, but used to be called a selective estrogen receptor modulator (SERM) and is in a class of drugs called estrogen agonists/antagonists, which have been developed to deliver the positive effects of estrogens without the possible disadvantages.
Raloxifene has been shown to reduce the risk of spine Fxs but there is no evidence that it reduces the risk of hip and other non-spine Fxs. It is taken daily as a 60 mg tablet for treatment or prevention.
In addition to treatment for OP, raloxifene has also been shown to decrease the risk of estrogen-dependent breast cancer by 65% over eight years. It is also approved by the FDA to decrease the risk of breast cancer in women with OP and also in women without OP who are at high risk for breast cancer.5,32
Teriparatide Parathyroid Hormone (PTH) (1-34) (Forteo)
13
Clinical studies have found that teriparatide reduces Fxs in the spine and in other bones in PMO women. Patients who have had a Fx due to OP and with very low bone density (T-scores < -3.0) may be the best candidates for teriparatide. It is an option for those who continue to lose bone density or break a bone during treatment with other OP drugs.
Teriparatide is self-administered as a daily injection from a pre-loaded pen and may be taken for a maximum of two years, after which patients may start on an antiresorptive medication to retain the benefits of teriparatide. Teriparatide is usually used for resistant diseases.5,32
Denosumab (Prolia)
Denosumab has been approved by the FDA to treat OP in PMO women who are at high risk of Fx and in women at high risk of Fx who are receiving adjuvant aromatase inhibitor therapy for breast cancer. It may also be used to increase bone mass in men with OP who are at high risk of Fx who may also be receiving androgen deprivation therapy to treat nonmetastatic prostate cancer.
14
Table 2.1. Summary of commonly prescribed bisphosphonates which are used to treat osteoporosis. Listed are generic name, brand name, indication approved for by the Food and Drug Administration, results of from trials, dosing and route of administration.
*OP=osteoporosis, PMO=post-menopausal osteoporosis, mg=milligram
Generic Name Brand Name Approved For Results Dosing/ Route of
administration
Alendronate Fosamax Treatment/prevention of OP in men, PMO women
Reduces risk of hip, spine, other fractures by approximately 50% over 2 to 4 years
5 mg tablet/day or 35 mg tablet/week for prevention. 10 mg tablet/day or 70mg tablet/week for treatment
Ibandronate Boniva Treatment/prevention of
OP in PMO women
Reduces incidence of spine fractures by ~50% over 3 years
IV injection 3 mg/3 months
Risedronate Actonel Treatment/prevention of OP in PMO women, treatment of OP in men
Reduces fracture risk by 35-45% over 3 years
5 mg tablet/day, 35 mg tablet/week, 75 mg tablet/2 weeks, 150 mg
tablet/month
Zoledronic acid Reclast Treatment/prevention of OP in PMO women, men, or those w/ existing low-trauma hip FXs; treatment of bone conditions in CA patients
Reduces risk of spine and hip fractures by 70% & 41%, respectively
IV infusion (doctor's office/outpatient setting) of 5 mg per year for
15
Table 2.2. Summary of commonly prescribed other osteoporosis medications (non-bisphosphonates) which are used to treat osteoporosis. Listed are generic name, brand name, indication approved for by the Food and Drug Administration, results of from trials, dosing and route of administration.
Generic Name Brand Name Approved For Mechanism of
action
Results Dosing/ Route
of
administration
Calcitonin Fortical Treatment of OP in
PMO women 5+ years beyond menopause
Hormone involved in
regulation of calcium & metabolism of bone; slows bone loss
Reduces risk
of Fxs in spine
Nasal spray
(200 IU daily) or injection (varied doses)
Raloxifene Evista Treatment/preventio
n of OP in PMO women; decreases
risk of breast CA in women w/OP or women w/o OP at high risk for breast cancer Selective estrogen receptor modulator (SERM), estrogen agonists/antagonists Reduces risk of spine FXs; reduces risk
of estrogen-dependent breast CA by 65% over 8 years
60 mg tablet/day for treatment/preve
ntion
Teriparatide Forteo Treatment of OP in PMO women, men at high risk of Fx; treatment of OP in both at high risk of Fx because of prolonged steroid use
Rebuilds bone, increases bone density, especially in the spine
Reduces FXs in spine and other bones in PMO women Self-administered daily injection for 2 years maximum, then patients may start
16
*OP=osteoporosis, PMO=post-menopausal osteoporosis, mg=milligram
Denosumab Prolia Treatment of OP in
PMO women at high risk of Fx and women at high risk of Fx who are receiving adjuvant aromatase inhibitor
therapy for breast cancer; increases bone mass in men w/ OP at high risk of Fx receiving androgen deprivation therapy for nonmetastatic prostate CA RANK ligand inhibitor/human monoclonal antibody Reduces risk of broken bones in spine, hip other bones. Reduces incidence of new spine FXs by 8%, hip FXs by 40%, incidence of non-spine FXs by 20% over 3 years
17 C. Safety of bisphosphonates
Concerns have emerged in recent years regarding the safety of BPs. Since 2003, many studies have been published regarding the association between BP therapy and exposed and necrotic bone of the jaw in patients.51 Several hypotheses have been proposed as to the potential mechanisms of this association, including the theory that inhibition of osteoclast functioning can inhibit normal bone turnover such that local damage from normal procedures such as tooth extraction cannot be repaired, ultimately resulting in bone necrosis.52 Other hypotheses are that there is inadequate bone blood supply to the jaw, genetic differences in patients, and metabolic changes due to BP therapy which may produce jawbone necrosis.52 More recently in 2011, reports emerged suggesting that long-term use of BPs may be associated with atypical femoral Fxs8 with recommendations that the therapy for patients on BP for more than five years should be reviewed to decide if treatment should be stopped.53-57
D. Comparative effectiveness of osteoporosis medications
i. Clinical Trials
Few head-to-head clinical trials comparing OP drugs have been conducted.10-14 Luckey et. al. (2004) compared alendronate with raloxifene in the treatment of 456 PMO in a 12-month randomized, double-blind trial. The researchers found that alendronate produced much greater increases in spine and hip BMD and greater reductions in the rate of bone turnover compared to raloxifene over the study period. Both drugs had similar profiles in terms of safety and tolerability among the patients. Recker et. al. (2007) also compared alendronate with raloxifene on Fx outcomes in PMO women; the study found greater increases in BMD at the lumbar spine, femoral neck, and total hip for patients treated with alendronate versus raloxifene.
18
risedronate. Bonnick et. al. (2006) found that the BP drugs alendronate and risedronate both increased BMD and lowered rates of bone turnover in the FACT (Fosamax Actonel Comparison Trial), a randomized multicenter trial enrolling over 1000 PM women with low initial BMD values who were followed for a year of treatment. However, BMD increased more in women who were treated with alendronate relative to those who were treated with risedronate.
ii. Observational studies
In addition, only a small number of non-experimental or observational studies have directly compared different OP drugs in their comparative effectiveness on Fx risk or other outcomes.15-18
Watts et. al. (2004) used administrative claims to study cohorts of new users of risedronate, alendronate, and nasal calcitonin. The study found that risedronate was more effective than calcitonin in reducing the risk of nonvertebral Fxs six months after the start of treatment. In addition, risedronate was found to reduce the risk of nonvertebral Fxs within a year of treatment more effectively than calcitonin or alendronate.
Silverman et. al. (2007) used observational data to compare the incidence of nonvertebral Fxs and hip Fxs between cohorts of users of risedronate and alendronate; the researchers found that patients who received risedronate had lower rates of hip and nonvertebral Fxs during the first year of therapy
compared to patients receiving alendronate.
A major limitation of these studies particularly those based on claims or administrative databases, is that important potential confounders, such as bone mineral density, BMI, physical activity, family history of OP and frailty, were not available for analyses.
Administrative claims-based pharmacoepidemiology
19
Large insurance claims databases can be valuable data sources for studies of rare adverse drug events. Large numbers of observed individuals, often with large amounts of observable follow-up time allow for easier identification of rare events.
Employer-based insurance coverage is the most common insurance state in the U.S., with approximately 49% of the total population being covered by an employer-based health plan in 2010.58 While the UH database represent very large numbers of unique individuals, over 60 million,, from throughout the US, there are limitations to the generalizability of the sample. Employed, insured
individuals tend to be healthier than uninsured individuals59 and therefore studies using these databases are somewhat limited in the generalizability of findings to uninsured or unemployed populations. Also, the employer-based health plans participating in UH tend to be all large employers, without representation from small- or medium-sized employers.60 While the populations that make up these databases are limited somewhat in population-representation, they are still valuable tools for investigating the associations between drugs and diseases.
All claims contained within the UH database resulting from pharmacy dispensing, outpatient services, or inpatient admissions have been paid and adjudicated, ensuring a high level of accuracy and completeness.
Because the primary purpose of the UH data system is to facilitate reimbursement for healthcare provided, data for variables that might be found in a medical chart, but are not used for billing purposes such as height, weight, or smoking, are generally not available. Therefore, observational research based on this data may be plagued by unmeasured confounding.
E. Instrumental variable methods
IV methods61 which may control for these unmeasured confounders and which have been widely used in econometrics,62-63 have yet to be applied to the study of comparative effectiveness of OP medications.
20
instrumental variable (i.e., “instrument”). Prior pharmacoepidemiologic studies using IV methods based on administrative databases have used a variety of co-Rxs, comorbidities, and other variables as instruments.64-69, 25
Generally, the IV estimate is the intent-to-treat estimate of the effect of the IV (numerator) on the treatment on the outcome, weighted by the strength of the IV in predicting received treatment
(denominator).62
where X is received treatment, Y is outcome, and Z is IV.
Figure 2.1. Directed acyclic graph of IV, treatment, confounders and outcome illustrating the main assumptions of IV methods.
IV methods rest on three main assumptions: (1) the IV is associated with the received treatment (i.e., the IV affects the treatment choice or shares a common cause with it), (2) covariate values do not differ by the level of the IV (independence assumption), and (3) the IV does not predict the outcome except through its influence on the treatment (exclusion restriction; no direct effect of the IV on the outcome and no effect of any kind of the outcome on the IV).69
Evidence of physician/provider preference for osteoporosis medications
21
assumes that physicians or groups of providers differ in their preferences for medical treatments or procedures for similar patients.70 Differences in hospital capacity, drug benefit plans or formularies may lead to regional differences in medical decision making among groups of physicians.71 Other factors such as marketing by pharmaceutical companies, a physician’s clinical experience, emerging evidence about safety and efficacy of a drug, patient case mix, drug availability and reimbursement may also influence a physician’s prescribing decision. However, as long as these factors contributing to physician prescribing decisions are not related to patients’ characteristics, the assumptions of the IV are not violated.
Furthermore, for OP medications, a physician’s prescribing preferences may be influenced by patient preference which may depend on affordability,28 potential side effects,72, 73 convenience of dosing schedule,29 and route of administration.74 If these patient preferences are associated with potential confounding variables, the validity of the IV may be compromised.
22 REFERENCES
1. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis Prevention, Diagnosis, and Therapy. J Am Med Assoc. 2001;285:785-95.
2. Laulert L, Almeida MA, Araujo VG, Francisco CM. Osteoporosis: a silent epidemic which will turn public. Rev Bras Enferm. 1995; 48(2):161-7.
3. Melton III LJ, Chrischilles EA, Cooper C, Lane AW, Riggs BL: Perspective: How many women have osteoporosis? J Bone Miner Res. 1992;7:1005-10.
4. Randell A, Sambrook PN, Nguyen TV, Lapsey H, Jones G, Kelly PJ, Eisman JA. Direct clinical and welfare costs of osteoporotic fractures in elderly men and women. Osteoporosis Int. 1995;5:427-32. 5. National Osteoporosis Foundation. Fast facts on osteoporosis. Available at:
http://www.nof.org/osteoporosis/diseasefacts.htm . Accessed on 31 August 2010. 6. Sambrook P, Cooper C. Osteoporosis. Lancet 2006; 367:2010-18.
7. Fellows JL, Rindal DB, Barasch A, et al. ONJ in two dental practice-based research network regions. J Dent Res. 2011;90:433-438.
8. Dell RM, Adams AL, Greene DF, Funahashi TT, Silverman SL, Eisemon EO, Zhou H, Burchette RJ, Ott SM. Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res. 2012;27:2544-50.
9. Rachner TD, Khosla S, Hofbauer L. Osteoporosis: now and the future. Lancet. 2011;377(9773):1276-1287.
10. Bonnick S, Saag KG, Kiel DP, McClung M, Hochberg M, Burnett SM, et al. Comparison of weekly treatment of postmenopausal osteoporosis with alendronate versus risedronate over two years. J Clin Endocrinol Metab. 2006; 91:2631-7.
11. Luckey M, Kagan R, Greenspan S, Bone H, Kiel RD, Simon J, et al. Once-weekly alendronate 70 mg and raloxifene 60 mg daily in the treatment of postmenopausal osteoporosis. Menopause. 2004; 11:405-15
12. Recker RR, Kendler D, Recknor CP, Rooney TW, Lewiecki EM, Utian WH, et al. Comparative effects of raloxifene and alendronate on fracture outcomes in postmenopausal women with low bone mass. Bone. 2007; 40: 843-51.
13. Rosen CJ, Hochberg MC, Bonnick SL, McClung M, Miller P, Broy S, et al. Fosamax Actonel Comparison Trial Investigators. Treatment with weekly alendronate 70 mg compared with once-weekly risedronate 35 mg in women with postmenopausal osteoporosis: a randomized double-blind study. J Bone Miner Res. 2005; 20:141-51.
14. Sambrook PN, Geusens P, Ribot C, Solimano JA, Ferrer-Barriendos J, Gaines K, et al. Alendronate produces greater effects than raloxifene on bone density and bone turnover in postmenopausal women with low bone density: results of EFFECT (Efficacy of FOSAMAX versus EVISTA Comparison Trial). International J Intern Med. 2004; 255:503-11.
23
16. MacLean C, Newberry S, Maglione M, McMahon M, Ranganath V, Suttorp M, Mojica W, Timmer M, Alexander A, McNamara M, Desai S, Zhou A, Chen S, Carter J, Tringale C, Valentine D, Johnsen B, Grossman J. Systematic Review: Comparative Effectiveness of Treatments to Prevent Fractures in Men and Women with Low Bone Density or Osteoporosis. Annals of Internal Medicine. 2008; 148: 197-213. 17. Silverman SL, Watts NB, Delmas PD, Lang JL, Lindsay R. Effectiveness of bisphosphonates on nonvertebral and hip fractures in the first year of therapy: the risedronate and alendronate (REAL) cohort study. Osteoporosis Int. 2007; 18:25-34.
18. Watts NB, Worley K, Solis A, Doyle J, Sheer R. Comparison of risedronate to alendronate and calcitonin for early reduction of nonvertebral fracture risk: results from a managed care administrative claims database. J Manag Care Pharm. 2004; 10:142-51.
19. Signorello LB, McLaughlin JK, Lipworth L, Sorensen HT, Blot WJ. Confounding by indication in epidemiologic studies of commonly used analgesics. Am J Ther. 2002 May-Jun; 9(3):199-205.
20. Brookhart MA, Schneeweiss S. Preference-based instrumental variable methods for the estimation of treatment effects: assessing validity and interpreting results. The International Journal of Biostatistics. 2007; 3(1): Art. 14.
21. Earle CC, Tsai JS, Gelber RD, Weinstein MC, Neumann PJ, Weeks JC. Effectiveness of
chemotherapy for advanced lung cancer in the elderly: instrumental variable and propensity analysis. J of Clinical Oncology. Feb 15 2001; 19(4):1064-1070.
22. Yoo BK, Frick KD. The instrumental variable method to study self-selection mechanism: a case of influenza vaccination. Value in Health. 2006; 9(2): 114-122.
23. Groenwold RHH, Hak E, Klungel OH, Hoes AW. Instrumental variables in influenza vaccination studies: mission impossible?! Value in Health. 2010; 13(1): 132-7.
24. McClellan M, McNeil BJ, Newhouse JP. Does more intensive treatment of acute myocardial infarction in the elderly reduce mortality? Analysis using instrumental variables. 1994; 272(11):859-866. 25. Wong K, Campitelli MA, Stukel TA, Kwong JC. Estimating influenza vaccine effectiveness in community-dwelling elderly patients using the instrumental variable analysis method. Arch Intern Med. 2012; 172(6): 484-491.
26. Brookhart MA, Wang PS, Solomon DH, Schneeweiss S. Evaluating short-term drug effects using a physician-specific prescribing preference as an instrumental variable. Epidemiology. May 2006; 17(3): 1-8.
27. Brookhart MA, Rassen JA, Wang PS, Dormuth C, Mogun H, Schneeweiss S. Evaluating the validity of an instrumental variable study of neuroleptics. Med Care. 2007; 45:S116-S122.
28. McHorney CA, Schousboe JT, Cline RR, Weiss TW. The Impact of osteoporosis medication beliefs and side-effect experiences on non-adherence to oral bisphosphonates. Current Medical Research and Opinion. 2007; 23(12):3137-3152.
29. Reginster J, Rabenda V. Patient preference in the management of postmenopausal osteoporosis with bisphosphonates. Clinical Interventions in Aging. 2006;1(4):4415-423.
24
32. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, and Posey LM. Pharmacotherapy: A Pathophysiologic Approach. New York: McGraw-Hill; 2005.
33. Delmas PD. Treatment of postmenopausal osteoporosis. The Lancet 2002; 359:2018-26. 34. Bartl R, Frisch B. Osteoporosis: Diagnosis, Prevention, Therapy. Berlin Heidelberg: Springer-Verlag; 2009.
35. Riggs BL, Melton LJ 3rd. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone. 1995; 17:505S.
36. Ioannidis G, Papaioannou A, Hopman WM, et al. Relation between fractures and mortality: results from the Canadian Multicentre Osteoporosis Study. CMAJ. 2009; 181:265.
37. Poole KE, Compston JE. Osteoporosis and its management. BMJ. 2006; 333:1251.
38. Adachi JD, Adami S, Gehlbach S, et al. Impact of prevalent fractures on quality of life: baseline results from the global longitudinal study of osteoporosis in women. Mayo Clin Proc. 2010; 85:806. 39. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006; 17:1726.
40. Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jonsson B. Mortality after osteoporotic fractures. Osteoporos Int. 2004; 15:38-42.
41. Ahlborg HG, Johnell O, Turner CH, et al. Bone loss and bone size after menopause. N Engl J Med. 2003; 349:327.
42. Kanis JA. Diagnosis of osteoporosis and assessment of fracture risk. Lancet. 2002; 359:1929. 43. Kanis JA, Johnell O, Oden A, et al. Ten-year risk of osteoporotic fracture and the effect of risk factors on screening strategies. Bone. 2002; 30:251.
44. Kanis JA, Borgstrom F, De Laet C, et al. Assessment of fracture risk. Osteoporos Int. 2005; 16:581.
45. Unnanuntana A, Gladnick BP, Donnelly E, Lane JM. The Assessment of Fracture Risk. J Bone Joing Surg Am. 2010; 92(3):743-753.
46. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser. 1994; 843:1.
47. World Health Organization Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK. FRAX: WHO Fracture Risk Assessment Tool. Available at:
http://www.shef.ac.uk/FRAX/index.aspx?lang=En . Accessed on April 24, 2005.
48. Bates DW, Black DM, Cummings SR. Clinical use of bone densitometry: clinical applications. JAMA. 2002;288(15):1889-1897.
49. Fontenot HB, Harris AL. Pharmacologic Management of Osteoporosis. JOGNN. 2013; 43:236-245.
25
51. Fellows JL, Rindal DB, Barasch A, et al. ONJ in two dental practice-based research network regions. J Dent Res. 2011;90:433-438.
52. Ruggiero SL, Drew SJ. Osteonecrosis of the jaws and bisphosphonate therapy. J of Dental Res. 2007; 86:1013.
53. How Long Should You Take Osteoporosis Drugs? Food and Drug Administration Website 2014. Available at: http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm309688.htm . Accessed on April 22, 2014.
54. FDA Drug Safety Communication: Safety update for osteoporosis drugs, bisphosphonates, and atypical fractures. Food and Drug Administration Website 2010. Available at:
http://www.fda.gov/drugs/drugsafety/ucm229009.htm . Accessed on April 22, 2014.
55. Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-Connor E, Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC, Vogt T, Wallace R, Yates AJ, LaCrix AZ. Effect of Alendronate on Risk of Fracture in Women with Low Bone Density but Without Vertebral Fractures. JAMA. 1998; 280(24):2077-2082.
56. Black DM, Schwartz AV, Ensrud KE, et al. Effects of continuing or stopping alendronate after 5 years of treatment: The Fracture Intervention Trial Long-term Extension FLEX): A Randomized Trial. JAMA. 2006; 296(24):2927-2938.
57. Food and Drug Administration. FDA Drug safety podcast for healthcare professionals: Safety update for osteoporosis drugs, bisphosphonates, and atypical fractures. Available at:
http://www.fda.gov/drugs/drugsafety/drugsafetypodcasts/ucm229800.htm . Accessed on April 24, 2014. 58. Kaiser Family Foundation. Health coverage & uninsured.
http://www.statehealthfacts.org/comparecat.jsp?cat=3&rgn=6&rgn=1. Updated 2010. Accessed on April 21, 2014.
59. Kasper JD, Giovannini TA, Hoffman C. Gaining and losing health insurance: strengthening the evidence for effects on access to care and health outcomes. Medical Care Research and Review. 2000;57(3):298-318.
60. Hansen LG, Chang S. White paper: Health research data for the real world: the Thomson Reuters MarketScan Databases. Thomson Reuters. January 2011.
61. Greenland S. An introduction to instrumental variables for epidemiologists International Journal of Epidemiology. 2000; 29:722-729.
62. Angrist JD, Pischke J. Mostly Harmless Econometrics: An Empiricist’s Companion. Princeton, NJ: Princeton University Press; 2009
63. Angrist JD, Krueger AB. Instrumental variables and the search for identification: from supply and demand to natural experiments. The Journal of Economic Perspectives. 2001; 1(4):69-85.
64. Earle CC, Tsai JS, Gelber RD, Weinstein MC, Neumann PJ, Weeks JC. Effectiveness of
chemotherapy for advanced lung cancer in the elderly: instrumental variable and propensity anslysis. J of Clinical Oncology. Feb 15 2001; 19(4):1064-1070.
26
66. Yoo BK, Frick KD. The instrumental variable method to study self-selection mechanism: a case of influenza vaccination. Value in Health. 2006; 9(2): 114-122.
67. McClellan M, McNeil BJ, Newhouse JP. Does more intensive treatment of acute myocardial infarction in the elderly reduce mortality? Analysis using instrumental variables. 1994; 272(11):859-866. 68. Brookhart MA, Rassen JA, Wang PS, Dormuth C, Mogun H, Schneeweiss S. Evaluating the validity of an instrumental variable study of neuroleptics. Med Care. 2007; 45:S116-S122.
69. Brookhart MA, Wang PS, Solomon DH, Schneeweiss S. Evaluating short-term drug effects using a physician-specific prescribing preference as an instrumental variable. Epidemiology. May 2006; 17(3): 1-8.
70. Brookhart MJ, Rassen JA, Schneeweiss S. Instrumental variable methods in comparative safety and effectiveness research. Pharmacoepidemiology and Drug Safety. 2010; 19:537-54.
71. Cole JA, Norman H, Weatherby LB, Walker AM Drug copayment and adherence in chronic heart failure: effect on cost and outcomes. Pharmacotherapy. 2006; 26: 1157-1164.
72. Papaioannou A, Kennedy CC, Dolovich L, Lau E, Adachi JD. Patient adherence to osteoporosis medications - problems, consequences and management strategies. Drugs Aging. 2007; 24(1): 37-55. 73. Unson CG, Siccion E, Gaztambide J, Gaztambide S, Mahoney Trella P, Prestwood K.
Nonadherence and Osteoporosis Treatment Preferences of Older Women: A Qualitative Study. Journal of Women’s Health. 2003; 12(10):1037-45.
74. Fraenkel L, Gulanski B, Wittink D. Patient treatment preference for osteoporosis. Arthritis Rheum. 2006 Oct 1; 55(5): 729-735.
27
CHAPTER III. METHODS
A. Study population
This retrospective cohort study was conducted in a population of PM women aged 55 years and older participating in commercial health insurance plans and residing in various geographical regions throughout the US from 2008 to 2011. The patient population meeting study criteria was drawn from the UH database from OptumInsight, Inc.
Subject/Patient Eligibility
Inclusion Criteria:
Women who satisfy all the following criteria during the study period were included in the cohorts of women who are PMO treatment initiators:
Reach postmenopausal age (≥55 years).
Have ≥12 months of continuous enrollment in the health plan (with complete medical and pharmacy coverage) without any OP medication Rxs before the index date.
Receive BP or other OP treatment after reaching postmenopausal age.
The index date is defined by the earliest date when the patient satisfied all the 3 cohort criteria during the study period. The 12-month period prior to the index date (including the index date) is defined as the baseline period.
Exclusion Criteria
Women with Paget’s disease (ICD [International Classification of Disease]-9
731.0) or a diagnosis of malignancy (excluding non-melanoma skin cancer) or treatment with
chemotherapy, hormonal therapy or radiation therapy for cancer during the 12-month treatment
28 B. Data sources
This project was a secondary analysis using the UH database. It consisted of fully-adjudicated claims databases of eligibility, pharmacy and medical claims data for patients enrolled in a large U.S. health plan which provides fully-insured coverage for physician, hospital and Rx drug services. The current project included data from January 1, 2008 to June 30, 2011 from the UH database.
C. Study design
Definitions of Time Periods
Study Period
Analysis was conducted using the UH commercial administrative claims databases from January 2008 through the June 2011.
Baseline Period
The 12-month period prior to the index date (including the index date) is defined as baseline period.
Study Follow-up Period
Follow-up began on the index date (excluding index date) and continued until the earliest of disenrollment from the data system, death, Paget’s disease, a diagnosis of malignancy (excluding non-melanoma skin cancer) or treatment with chemotherapy, hormonal therapy or radiation therapy, or end of the study period. The follow-up also ended at the first occurrence of study outcome, i.e., osteoporotic Fx (definition provided Table A of the Appendix).
D. Significance and innovation
Significance
29
medical service claims, which contain provider information, with pharmacy claims, which do not; these methods are of value not only to the current project but also to other studies and databases where this identification and linking is needed to conduct the desired analyses.
In addition, although large pharmacoepidemiologic databases such as UH provide large sample sizes to study rare events, they are often lacking in important potential confounders; therefore, exploring the viability of using IV methods to adjust for unmeasured confounding in studies using these databases consisting of observational data is important. IV methods have not yet been applied to the study of comparative effectiveness of OP medications.
Furthermore, with the recent safety warnings issued by the FDA regarding long-term use of BPs and the introduction of new OP drugs onto the market, understanding the comparative effectiveness of the different OP medications is of value to clinicians, regulators, the pharmaceutical industry, and academia.
Innovation
IV methods have not yet been applied to the study of the comparative effectiveness of OP medications. Previous studies that have compared the effectiveness of these medications using observational data have used conventional methods to address measured confounding but have not addressed the issue of unmeasured confounding.
In addition, the current project used innovative methods to link different parts of the UH database. These methods could be useful in other instances, such as with Medicare data where Parts A (hospital insurance) and B (medical insurance) contains provider or physician information but Part D (Rx drug coverage) does not.
30
provider/physician may be useful in general for studies that seek to evaluate the patterns of physician prescribing and their impact on health-related outcomes.
E. Dependent variable definitions
Outcome definition
Osteoporotic Fx was defined as closed Fx at the hip, spine, pelvis, femur, humerus, radius or ulna, open Fx at the distal radius or ulna, or Fx at the spine based upon an algorithm (Appendix, Table B) comprised of ICD-9 diagnosis codes and procedure codes.1 Fxs associated with an ICD-9 E code for major trauma associated with vehicle accidents, falls, and other accidents (E800-E848, E881-E884, E908-E909, E916-E928) were excluded. To ensure identification of incident cases, there was a
requirement that that there were no claims for the same Fx site within the 6 month period preceding the Fx.
The patient was followed until the first eligible event of osteoporotic Fx was identified or follow-up was censored.
Validity and reliability of outcomes
There is no validation of the ascertainment algorithm for fragility Fx planned in this study.
However, the case ascertainment algorithm of fragility Fx was derived based on Fxs of hip (closed), distal radius/ulna, spine (closed or pathologic), pelvis (closed), other femur (closed), other radius/ulna (closed) and humerus (closed) according to a systematic literature review.1 In this review, the above mentioned Fx sites and types were ranked as 8-9 out of 9 as highly likely to be Fxs because of OP in elderly females.
F. Independent variable definitions
Exposure definition
31
(HCPCS) procedure codes. BPs to be assessed in this study are restricted to those indicated for the treatment of postmenopausal OP, i.e., IV BPs including zoledronic acid infusion (Reclast) and
ibandronate injection, and oral BPs including alendronate sodium, alendronate sodium/vitamin D tablet (Fosamax plus D), ibandronate sodium, risedronate and risedronate sodium/calcium carbonate
(Appendix, Table A). Other OP medications to be assessed include calcitonin injection, teriparatide injection; raloxifene tablet and calcitonin spray (Appendix, Table A).
Covariate information
For the cohorts, covariates were assessed during the baseline period. Covariates were chosen by literature review; in particular, risk factors for osteoporotic Fx in women with PMO as described in Holmberg et. al. (2006)2 and Dontas et. al. (2007)3 were used in this study. These covariates include demographic factors, comorbidities and concomitant medications.
Demographic factors:
Age on the PMO index date
Geographic region
Ethnicity
Length of enrollment in the data system before PMO index date Comorbidities:
Diabetes
Fragility Fx (assessment using same approach as in PMO algorithm)
Osteoporosis (assessment using same approach as in PMO algorithm)
Overweight or obesity
Tobacco use disorders
Rheumatoid arthritis
32 Medications:
Hormone Replacement Therapy
Corticosteroids
Tamoxifen
Immunosuppressants
Anticonvulsants
Antidepressants
Antihypertensives Charlson Comorbidity Index
The calculation of CCI was based on diagnosis received during the 12-month baseline period. Comorbidities for the calculation of CCI include 16 disease categories which are defined using ICD-9 codes. Both inpatient and outpatient data claims were used to calculate the CCI. New Jersey Medicare weights for each category developed by Schneeweiss (2003)4 was applied in the Charlson Comorbidity Index calculation.
G. Statistical analysis for Aim 1
The gold standard “proportion” statistic
The unique DEAs on the index Rxs for women in our cohort were identified. For each DEA, all new Rx fills for any drug during the study period were obtained and the provider IDs on the medical service claims appearing within 14 days prior to each new Rx were identified.
33
Predictive modeling of a match
We used GEE logistic and log-linear models and beta regression with “proportion” or “match” as the outcomes to predict whether a given provider, as identified from the medical service claims, will be the most likely prescriber by relating the characteristics of medical service visits with the probability of a match between the provider ID and DEA variables. Explanatory variables were indicator variables for provider specialty (among the specialties likely to prescribe OP medications) being internist, hospitalist, family or general practitioner, orthopedic surgeon, or other specialty (i.e., podiatrist, osteopath, general surgeon, obstetrician/gynecologist [OB/GYN], rheumatologist, or endocrinologist), office visit, total number of OP diagnoses and the total number of dual energy x-ray absorptiometry (DXA) scans as identified on the medical services claims in the 2-week period prior to an index date, and the total number of medical service claims for a particular provider. The predicted probabilities from this model could be applied to another database such as MarketScan, which has a provider ID variable in medical service claims but no physician ID in pharmacy claims, to predict the most likely prescriber.
To evaluate the performance of the models, we computed sensitivity and specificity for each approach by comparing the provider with the highest “proportion” with the provider with the largest predicted probability as calculated with each model.
H. Statistical analysis for Aim 2
DEA variable in the United Healthcare Database