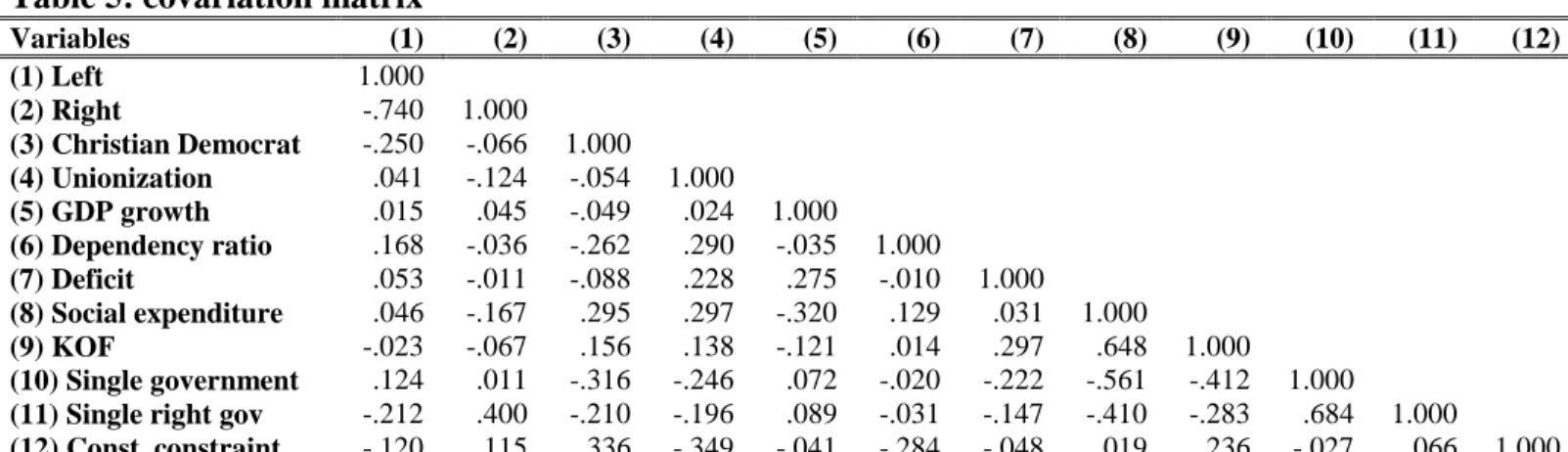
1
The politics of health care: examining the role of
partisanship in health care
Leiden University
Public administration: Economics and Governance Track Master’s
thesis
Name:
Samir Mustafa Negash
Student id: s1280309
Date:
06/11/2018
2
Table of contents
1. Introduction ... 3
2. Theoretical framework ... 7
2.1 Partisan politics and the power resource theory ... 7
2.2 The new politics of the welfare state ... 9
2.3 Health care retrenchment in a social rights perspective ... 12
2.4 Hypotheses ... 18
3. Methodology ... 21
3.1 Case selection and operationalization ... 23
3.2 Dependent variable ... 23
3.3 Independent variable ... 24
3.4 Data ... 29
4. Results ... 30
4.1 Descriptive statistics ... 30
4.2 Inferential statistics ... 32
4.3 New politics models ... 42
4.4 Analysis and discussions ... 51
5. Conclusion ... 53
Literature ... 56
3
1. Introduction
Following the golden-age of the welfare state (1960-1980), welfare scholarship has described the
welfare state as being in a perpetual state of austerity. According to Paul Pierson (1994), the period
after 1980 constitutes a period of permanent austerity and is characterized by welfare retrenchment
and restructuring. The period of welfare expansion ended in most mature western democracies as
countries were confronted with stagflation, i.e., high unemployment and persistent inflation.
Structural changes in the economy exert downward pressures on welfare states to reduce their
social wage, e.g., by reducing social spending and cutting taxes and social contributions in order
to maintain attractive investment climates. As governments are dependent on business and capital
to create jobs and generate revenues for taxes, they are receptive to the demands made by capital,
albeit their receptivity to these claims comes in varying degrees. The implications for the welfare
state are a potential regulatory and welfare ‘race to the bottom’ (Myles & Quadagno, 2002: p. 43).
A range of domestic and international developments have made the financing and delivery
of welfare programs more difficult. On the international front, these changes have been a function
of changes associated with globalisation. Internationalisation of the economy has pushed states
toward fiscal and monetary discipline. This has been the result of increased trade with low wage
countries in the global south, which generates inter-industry competition between developed and
developing countries and has led to offshoring and deindustrialisation. Increased capital mobility – enabled by the removal and reductions in restrictions of capital flows – has also incentivised
states to be more receptive to market forces (Raess & Pontusson, 2015: p. 3; Burgoon, 2001; Autor,
Dorn & Hansen, 2015). Additionally, for European welfare states, membership to the European
Union (EU) and European Monetary Union (EMU) has functioned as another means of fiscal and
monetary constraint on the welfare state. Membership to these institutions has resulted in reduced
autonomy of states to conduct social policy by privileging low deficits and low inflation rates over
full employment or risk-sharing (Brady and Lee, 2014; Korpi, 2003: p. 604).
Domestically, the shift from industrial to post-industrial economies with high employment
rates in the services industry has resulted in lower economic growth rates (Iversen & Cusack,
2000). This shift toward post-industrial economies has also shifted risks across actors in the
economy. This shift has complicated welfare provision by creating additional budgetary pressures
on the welfare state (Korpi, 2003: p. 590). Demographic changes such as population aging, a
4 constellation of the labour market due to the increased participation of women, has increased
pressure on welfare states to adapt. This has resulted in an emphasis on social investment, active
labour market policies and a focus on capacity enhancing services such as child care and education,
rather than providing passive wage replacement. (Busemeyer et al, 2018: p. 802; Esping-Andersen,
1999: p. 182). Long term unemployment or structural unemployment has also become more
prevalent due to technological advances. This has also made funding the welfare state more
difficult and poses another major challenge for contemporary welfare states (Pierson, 2001b;
Schwartz, 2001: p. 19; Korpi, 2003: p. 603).
These developments have constituted pressures on the welfare state as a whole. Their impact
has varied across different policy areas. Health care systems, for example, have experienced cost
pressures uniquely related to developments in the policy area of health care. As with other
components of the welfare state, health care seems to have been subject to the same general pattern:
a golden age of expansion (1960-1980) and a subsequent period of stagnation and restructuring
after 1980s (Freeman & Moran, 2000: p. 37). Health care cost have been rising in all OECD
members, more than doubling in total expenditures since 1970. It is no wonder then that from the
1980s onward, governments in OECD countries began to raise questions regarding the efficiency
of their health care systems. Consequently, mature welfare states started examining the
expenditures on health care and re-evaluated their health care systems in an effort to enhance
efficiency and restrain costs (Mackenbach et al, 2012: pp. 341-342).
This study aims to contribute to the welfare state scholarship by zooming in on developments
in on the field of health care. It seeks to gauge how health care systems of 22 industrialised
democracies have adapted to these pressures. Using a Large-N design and studying the period
1981-2014, this project studies whether there is a relationship between partisanship and various
measures of health care policy output over time. Previous studies on the importance of partisan
makeup of governments for the organizing health care systems have produced mixed results (see
references). It builds on these previous works by expanding the scope of research from the
financing of health care (e.g. Jordan, 2011; Potrafke, 2010) to service provision capacity and
regulation. The research question guiding this study is thus as follows: What effects have different
partisan makeups of governments had on degree of retrenchment in the field of health care?
To answer this question, the explanatory power of the power resource theory (Korpi, 2006;
5 1996; 1994) will be tested. These two theories make competing claims about the role and
importance of partisanship, as well as the likelihood of large scale retrenchment. The power
resource theory holds that the distribution of power resources matters for welfare expansion. It
posits that organizations that help wage earners engage in collective action, e.g. through
unionization or translating their demands into policy via voting for left wing parties, are critical in
understanding outcomes of distributive conflicts. Left and right wing parties have different
preferences and pursue different policies according to the power resource theory. Left parties
favour expansion of the welfare state and pursue higher degrees of redistributions. Right wing
parties pursue retrenchment and restructuring of the welfare state.
The new politics approach’s claims differ from this, as the role of partisanship is more
circumspect according to this theory. Due to differences in the goals and consequences of welfare
expansion and retrenchment, the political logic of retrenchment varies substantially from
expansion. The behaviour of left and right parties becomes more similar according to the new
politics thesis. That is, left wing parties do not or cannot pursue large expansion, right parties by
contrast cannot pursue expansion. The new politics school also holds that large scale retrenchment is unlikely due to the welfare state’s staying power. The existence of the welfare state alters the
political landscape and creates powerful constituencies that will come to the aid of social programs.
Governments can choose from a range of options in response to cost pressures in health
care. The specific responses to these challenges are the often subject of political and distributive
conflicts. Health care can be profoundly political as it concerns an object of collective consumption
with a large role for the state in all mature welfare state (Moran, 2000: pp. 141-142). The chosen
methods may reflect partisan preferences as some previous studies have indicated (Montanari &
Nelson, 2013a; 2013b). Overall, governments have to contend with balancing multiple goals in
organizing health care and making decisions about cost containment. These goals include ensuring
equity and access; having health systems that are efficient and delivering high quality health care
services. (Blank et al, 2007: p. 93). These goals are inherently in conflict as it is impossible to
deliver on all fronts. The choices made could then, to a certain degree, reflect the values and
priorities of the actors involved. This makes them a relevant area of research for politics
researchers.
What is unclear from the existing literature on welfare retrenchment and partisanship is
6 systems systematically vary according to partisan makeup of governments and distribution of other
power resources. The types of administrative changes pursued affect the degree to which health
care services can readily be accessed and the degree to which health care is provided as a social
right. Health care constitutes a crucial element of the social right to citizenship in most mature
welfare states. This study expands the scope of analysis to include these dimensions, in line with
previous research (Montanari & Nelson, 2013a; 2013b; Bambra, 2005). The analysis will examine
how partisan makeup of government affects the range of health care resources available in a
western democracy. Since the 1980s, the private share of health care financing has increased in all
members of the Organisation of Economic Cooperation and Development (OECD). This suggests
some degree of retrenchment in health care. The following sections will argue that financing is not
the only relevant dimension of health care retrenchment. Instead, financing is but one dimension
of health care in which retrenchment can take place. This study hopes to contribute to the welfare
scholarship by examining how partisanship affects health care service provision. It does this by
applying two theories often used to explain developments in cash benefits schemes to services
such as health care which have different underlying logic. In so doing it tries to expand current
scholarship on the determinants of public services as well as the politics underlying services such
as health care.
This thesis is structured as follows: in the next section the power resource theory is
presented and elaborated on. This is followed by a discussion of the new politics thesis. After a
discussion of the power resource theory and the new politics thesis, the politics of health care
retrenchment are discussed. Special attention is paid to the differences between services and
in-kind benefits versus cash benefits. Following this theoretical discussion, the research design is
presented. This study uses time-series data on 21 members of the OECD and performs statistical
analysis using linear regression with panel-corrected standard errors to answer the research
question. After the research design, the results are presented and analysed. The final chapter
7
2. Theoretical framework
2.1 Partisan politics and the power resource theory
One of the main approaches used to study the development of the welfare state is the power
resource theory (Bradley et al, 2003: p. 193). According to scholars in the power resource school
of thought, contemporary welfare states are the product of class-based distributional conflicts.
Socioeconomic class is related to the types of life course risks individuals are exposed to. As such,
the fault lines of distributive conflicts are likely to reflect these class-based differences in risk
exposure. Moreover, socioeconomic class shapes the range of power resources individuals have at
their disposal. Consequently, researchers in the power resource school have argued that welfare
state development mirrors the class-based distributive conflicts and partisan political distribution
of power in different countries (Korpi, 2006: p. 168). Therefore, differences in the distribution of
power resources as well as the types of cross-class coalitions present in individual countries
accounts for the variation in welfare states (Esping-Andersen, 1990, chapter 1).
Power resources reflect the ability of individuals or groups to sanction or reward other
actors (Korpi, 1985: p. 33; Korpi, 2006: p. 172). Their relevance to welfare state development
stems from the fact that they enable wage earners to equalize or erase their inherently
disadvantaged position vis-à-vis employers and business interests e.g. through unionization or
organizing politically in class-based political parties (Korpi, 1985: p. 41; Korpi, 2006: p. 171). The difference between wage earners and capital owners’ position stems from the differences between
physical capital and human capital, i.e., the specific means of production owned by different
groups in society. Employers’ power flows from their ownership of physical capital. Physical
capital lends itself to concentration, is scarcer and is easier to divest or apply as it requires low
mobilization cost. Wage earners on the other hand tend to rely on human capital rather than
physical capital. Labour power is the primary basis of human capital, this is derived from education
and occupational skills for example. This power resource is more difficult to mobilise, is less
scarce and, importantly, harder to concentrate and difficult to divest from its owner. It is their
advantage in numbers that gives their form of power resource its potency. If wage earners do not pool their resources, then employers’ capital derived power resources can be leveraged to bend
distributive conflicts to their will (Bradley et al, 2003: p. 197). For these reasons wage earners
8 favour (Korpi, 1985: p. 34).
The power resources theory is distinctly different from other partisan accounts of welfare
state development. What the power resource account has in common with other non-power
resource-based partisan approaches to studying welfare development is the emphasis they put on
distribution of partisan political power. As such, both the power resource theory and partisan
approaches of welfare state development essentially hold that parties represent different social
constituencies with different needs and interests, that parties’ social profiles mirror the social
preferences of their constituencies and that they are policy-seeking as well office-seeking
(Schmidt, 2010: p. 213). Where they differ though, is that power resource accounts of welfare
development also emphasises other means wage earners have at their disposal to organise
collective action, e.g. unionization, electoral turnout. Moreover, regarding the partisan effects,
power resource scholars have correctly identified Christian democratic parties as playing a large
role in developing welfare states as well. In many western European countries Christian democrats
have been successful in mobilising parts of the working and middle classes by catering to them
with their distinct type of social policy (Van Kersbergen, 1995). Therefore, researchers in the
power resource school not only take into account strength of left parties, but they also take into
consideration the strength of Christian democratic parties (Korpi, 2006: p. 196; Huber & Stephens,
1993; Korpi & Palme, 2003; Esping-Andersen, 1990:).
There is, generally speaking, a substantial amount of support for the power resource
account in the comparative welfare states literature. Especially in the old politics era (i.e. from
the1960s until roughly 1980), a lot of studies confirm that incumbency of left parties is associated
with various indicators of welfare expansion (Korpi and Palme, 2003; Allan & Scruggs, 2004;
reference) For example, Huber and Stephens: (2001: p. 41; 78) find that incumbency of left wing parties and Christian democratic parties lead to distinctly different outcomes with regards to
redistribution, development of social expenditures and transfer payments. They argue that
incumbency of left parties that facilitate the translation of preferences, mobilization and
organization of the working and lower-middle classes generates generous and redistributive
welfare states. This account finds support in other studies as well (Bradley et al, 2003). Social
democracy with strong unions has been linked to expansions of the public economy by expanding
the public sector, greater degrees of decommodification, redistribution and the provision of goods
9 Christian democratic parties tends to result in overall higher expenditures, primarily through higher
transfer payments, Christian democratic governments are less likely to lead spend more on social
expenditures. Christian democracy is also associated with lower degrees of decommodification, as
Christian democrats pursue social policy that reproduces inequality instead of ameliorating or
exterminating it, and Christian democrats are also not associated with expansions of public
economy (Huber et al, 1993: pp. 717-718). In the same vein, Brady and Lee (2014) trace the causes
of cuts or changes in government spending. They find support for the power resources account as
the presence of strong trade unions is associated with lower cuts to government spending.
The main takeaway of these studies seem to be that the different social bases parties
represent affects the social policy they pursue in government. These parties’ ability to achieve their
policy goals is not only determined by their representation in parliament or government, but is also
contingent on workers mobilising outside of parliamentary politics. Moreover, changes or shifts
in the distribution of power resources can thus be expected to affect distributive conflicts (Korpi,
1985: p. 39).
2.2 The new politics of the welfare state
The claims advanced by the new politics of the welfare state perspective contradict those of the
power resource and partisan theories of welfare development. The new politics approach describes
the political logic of welfare development in an age of permanent austerity. According to Pierson
(1994; 1996; 2001), the politics of welfare retrenchment differ markedly from the politics of
welfare expansion. Welfare retrenchment is not simply the mirror image of expansion and the
politics of welfare retrenchment has its own distinctive logic. The differences in goals and political
context make the new politics fundamentally different from the “old politics” of the expansion
period (Pierson, 1996: p. 144). In contrast to could be expected based on the power resource
account, increasing power of the right and declining power of the left and unions does not appear
to have enabled large scale retrenchment of social programs (Pierson, 1996: p. 150).
Welfare state expansion often entailed the enactment of popular policies, conversely,
retrenchment is an exercise in taking away or reducing the generosity of benefits people receive.
As such, politicians enacting new social programs can engage in credit claiming, whereas
politicians advocating for and implementing restructuring or retrenching the welfare state will
10 seek to cut back on programs, they will shy away from visible cuts and retrenchment is only
possible limitedly and they will only enact them in broad based coalitions (Starke, 2006: p. 106).
Enacting cutbacks to social programs is difficult for a variety of reasons: Enacting
retrenchment can be challenging because of social psychological reasons, i.e. taking away is more
difficult than granting benefits and engenders weaker responses. Consequently, recipients and
citizens in general experience cuts more negatively, regardless of how government intends to
compensate citizens. Moreover, another factor that further compounds the challenges inherent to
welfare retrenchment is the logic of collective action: retrenchment typically imposes high and
concentrated cost on a (comparatively) small group of recipients, while promising diffuse and
often uncertain benefits on a larger group of people. Lastly, policy feedback and policy legacies
are additional factors that complicate the process of retrenchment. These factors are more
institutional in nature. They have bearing on the ways in which the welfare state has become part
of the political landscape and how this has altered the basic political calculus of actors in the welfare state. The welfare state’s existence led to the formation of new interest groups and
entrenched constituencies who rely on the welfare state, e.g. pensioner’s rights groups and patients’ rights groups. These groups have become the greatest proponents and protectors of
welfare programs. In so doing they have replaced trade unions as the interest group of greatest
significance, as was the case in the power resource account. Moreover, welfare retrenchment is
also likely to engender opposition from existing clientele due to the double payment problem and constrain government’s capacity to change policy due to lock-in effects and pre-commitments and
associated problems such as double payment. Moreover, formal institutions such as veto players
in the system also make enacting retrenchment more difficult (Pierson, 2001: p. 411-414; Levy,
2010: pp. 554-555).
The implications of the new politics for the relationship between partisanship and welfare
state development are clear: in the new politics era, partisanship is likely to matter less as the
welfare state has changed actors’ political calculus. For left parties it means they cannot, or are
restricted, in their pursuit of their preferred options of expanding existing programs or enacting
new programs. This is largely a consequence of the structural changes to the economy that have
created budgetary pressures on welfare states. For right parties this means that they are restricted
in advancing their preferred policy agenda of welfare retrenchment. As radical retrenchment is not
11 forced to obfuscate their goals or trim social programs around the edges. Therefore, the new
politics thesis would lead to the expectation that left and right parties behave more similarly with
regards to welfare development. It should be noted here that the new politics account provides
explanations for the behaviour of left and right parties. It is worth noting here that this approach
does not provide an account of Christian democrats’ preferences. It unclear whether Christian
democrats would pursue retrenchment and how they would rearrange risks.
Scholars have sought to corroborate the claims made by the new politics theory of welfare
development with overall mixed results. By and large Kittel and Obinger (2003: pp. 33-34) find
support for a declining importance of party politics on welfare state development in the new
politics era. They conclude that partisan effect decreased overt time, and stress that the importance
of partisanship for welfare development declined after 1980s. They claim that a particular type of
catch-up dynamic is unfolding. Generous states are in the process of retrenching or scaling down
their welfare state, while less generous welfare states on the other hand have expanded. As a results
welfare states are converging. Furthermore, they attribute much of the changes in welfare
development to the increasing dependency ratio due to aging and rising unemployment. Kwon and
Pontusson (2010) also argue that partisan differences seem to have disappeared in how
governments compensate domestic workers with welfare in response to globalisation. They argue
however that the rate of decline seems to be mediated by the presence of strong labour unions.
Brooks and Manza (2006: p. 822) provide additional support for the new politics approach. They
argue that welfare state resilience is explained by popular support for the welfare state. This seems
to be unrelated to distribution of power resources. They also find no significant association
between left power or the continued cabinet participation of left parties and welfare state
development in new politics era.
There are studies that find continued support for the power resource account, even in the
new politics age. For example, Allan and Scruggs (2004) test the implications of both the power
resource theory and new politics thesis and find that in the new politics age, right-wing parties
continue to be associated with retrenchment. This seems to disprove the new politics’ account,
according to which right wing parties are constrained in pursuing their preferred goal of
retrenchment. Korpi and Palme (2003: p. 41) also find that compared to secular and conservative
right parties, left-wing parties are more likely to increase, or at least, less likely to reduce the
12 finds that left parties are significantly and positively related to expansions of unemployment
insurance, pension and sick pay replacement rates. Her analysis includes data between 1980 and
2010, and the focus of the analysis is thus new politics period.
2.3 Health care retrenchment in a social rights perspective
Thus far the discussion has centred on the potential effects of partisanship on the development of
the overall welfare state. Authors across multiple disciplines, e.g. economics, sociology and
political science, have honed in on and examined the relationship between partisanship and
retrenchment in the domain of health care (see for example Jordan, 2011; Montanari & Nelson,
2013a; Potrafke, 2010; Herwartz & Theilen, 2010; Herwartz, & Theilen, 2014; Béland, 2010;
Freeman & Moran, 2000; Fervers, Oster & Picot, 2016; Pavolini & Österle, 2013; Companje,
Veraghtert & Widdershoven, 2009). What stands out is the diversity in theoretical perspectives
employed, the methods used and the variables of interest in these studies.
The causes attributed to the rising cost of health care are varied and are the result of
multiple mechanisms. The primary factors commonly cited as explaining increased health
spending are: First of all, increases in per capita gross domestic product (GDP) arguably lead to
increases in health care expenses. GDP per capita has long been a powerful explanatory variable
in explaining rises in aggregate health care expenditures, as health care appears to be a (somewhat)
elastic good (Aron-Dine et al, 2013). This means that consumption of health care increases as
national income increases. This increased consumption will then naturally be reflected in increases
in aggregate spending levels in health care (Hacker, 2004a: p. 699). Secondly, another commonly
cited factor explaining the continued increases in healthcare expenses is Baumol’s disease. Baumol’s disease refers to the limited room for productivity growth in the public sector. The
incomes of employees in the services sector have to keep pace with the incomes of employees in
the non-service sector. Over time, this combination of stagnant productivity and rising wages leads
to higher overall costs in the services sector. Given that health care is a policy field where services
make up a large part of the output, stagnant productivity will thus likely be reflected in higher
expenditures in health care (Baumol, 1967: p. 417). Thirdly, advancements in medical technology
and medicine are another commonly cited factor that could account for rises in health care
spending. These new technologies can improve health, but often come at high financial cost. Once
13 access to these technologies (Barr, 2010: p. 252; Giaimo, 2001: p. 336). Lastly, increased volume
in health care e.g. due to aging population and new treatments being available are other factors
that contribute to the increases in overall healthcare expenditures (Mackenbach, Stronks & Anema,
2012: pp. 343-344). Increases in overall healthcare expenditures are not necessarily problematic.
The increases in healthcare expenditures could simply reflect overall taste for healthcare and could
therefore constitute an entirely legitimate endeavour for governments to spend their money.
Increased healthcare expenditures could also reflect increased need for and use of healthcare
services due to demographic changes. Increased use of health services shows need for these
services and also shows why cutting back on them or otherwise shifting costs could be unpopular
(Freeman & Moran, 2000: p. 39).
Increasing expenditures on health care could nevertheless still be problematic in so far as
increased health care expenditures also constitute an opportunity cost; governments can invest a
euro only once. Spending more on health care essentially walls off, that is, forecloses expenditures
on other facets of the economy or the welfare state. Moreover, the ever-increasing expenses on
health care could have an impact on the overall economy as well. The effect of increases in health
care cost – in instances where employers cover the costs – are potential lower rates of investments.
The effects of rising health expenses in systems where employees bear the burden are potentially
higher marginal tax rates which act as disincentives for labour (Mackenbach et al, 2012: p. p. 343).
This argument finds at least some empirical support, for example by Fervers, Oser and Picot (2016) who extend Burgoon’s (2001) argument that various kinds of trade openness have dissimilar
effects in different policy areas. They examine a range of indicators for globalisation and public
share of health spending and conclude that increased openness does seem to lead to lower growth
in public health care expenses. This indicates that governments are under pressure to reduce public
health care spending to remain competitive in the face of increased international completion.
There are good reasons to assume that efforts at retrenchment in health care will differ from
efforts in other domains of social policy. Government’s health care cost containment strategies can
target the supply side or the demand side. Supply side cost containment strategies could be
agreements with preferred providers, restricting the number of doctors by putting restricting access
to the medical profession. There are also a number of demand side cost containment strategies.
These measures are aimed at making users of health care more conscious of the cost of health care
14 costs. Demand side cost containment can also be achieved through achieving slower rates of rises,
stopping cost rises in real terms or in rare instances reducing real costs (Blank, Burau and
Kuhlmann, 2007: p. 97). Governments will thus tend to shy away from achieving cost-cutting via
imposing costs on health care users. This is also apparent as in practice governments try to pursue
cost containment through stimulating competition, putting restrictions on providers and other
administrative changes. (Freeman & Moran, 2010: pp. 40-42).
Multiple authors have conducted Small-N comparative studies to research various episodes
of health care reform pursued by governments, and explore the politics underlying these reforms
(e.g. Hann, 2007; Gingrich, 2011; Giaimo, 2001). Hacker (2004a) for example examines recent
health care reforms in a couple of wealthy democracies (US, UK, Netherlands, Canada and
Germany). He argues that reform processes have been marked by change without reform and
reform without change. Toth (2010) looked at different waves of reform in health care in multiple
countries. He finds that each wave of reform is followed by a wave of counter reforms where the
effects of the previous reform are (partially) reversed. Interestingly, he notes that ideology seems
to matter in dynamic of reform and counter reform. The starting point of these studies is often the
cost pressures countries face to contain the growing costs of health care. They, however, rarely
examine explicitly the role of partisanship on attempts at implementing cost containment policies,
or the degree to which choice of cost containment strategy is tied to partisan and ideological
differences. So, while they contribute valuable information on the intentions and preferences of
actors in reform episodes, these studies do not allow for systematically quantifying the effects of
left, right or Christian democratic parties on health care.
In addition to the case study approach, numerous studies have attempted to map the long
term patterns in the development of health care expenses and the extent of retrenchment in health
care. These studies have also researched the relationship between partisan distribution of power
and changes in health care. Studies of retrenchment politics and welfare retrenchment have often
looked at cash benefits programs such as pensions or unemployment insurance (e.g.
Esping-Andersen, 1990; Korpi & Palme, 2003; or Allan & Scruggs, 2004). Studies of health care politics
have often emphasized the financing aspect by using the public share of health care expenditures
as the dependent variable. For example, in mapping health care retrenchment, Jordan (2011) tries
to gauge the effects of partisanship on health care retrenchment. His findings suggest that after
15 on the development of the public share of health spending.
In a similar vein, other authors have examined the relationship between partisan makeup
of governments and overall developments of the public share of health spending. These studies
have tended to produce mixed results as well with regards to the relationship between partisanship
and the public share of healthcare. Some find that while the private share of health spending seems
to be increasing in OECD countries (and therefore the public share has to be decreasing), there
does not seem to be an ideological basis for this, i.e. left and right parties seem to behave broadly
similarly, which would seem to disconfirm the partisan accounts (Fervers et al., 2016; Potrafke,
2010).
However, some authors (e.g. Huber and Stephens, 2001: p. 270; Herwartz, & Theilen,
2014) have found evidence of a relationship between the partisan makeup of government and
health care expenditures. The differences in results could in part be explained by differences in
how partisanship is operationalized in those studies and different statistical methods applied.
Potrafke (2010) for example uses government ideology as an explanatory, a variable which ranges
from 1-5 based on the degree of dominance of right wing parties in government. This allows for
identifying differences between left and right parties, but neglects the role of Christian democrats
in accounting for developments of public health care expenditures. Huber and Stephens (2001: p.
53) on the other hand use cabinet portfolio of left and Christian democratic parties as an
explanatory variable. This has the upside of including Christian democrats, however, their
approach also fails to include right parties. This is at least questionable; right wing parties are often
the actors most likely to pursue retrenchment. Excluding right parties from the analysis could
potentially understate the role of partisanship (Alan and Scruggs, 2004: p. 504).
These studies have a number of conceptual limitations. The majority of the studies
reviewed thus far have analysed retrenchment in health care by looking at the shifts in financial
burdens. That is, they have looked at how the public share of health care spending has changed
over time. However, health care as an area of social policy differs significantly from other cash
benefits social programs. The numerous actors involved, the set of regulations in place regarding
remuneration of providers and coverage, the range of services covered by different insurance plans
in addition to the types of health care resources available in a country, are all decisions that could
16 for what services are therefore not the only relevant changes governments make with regards to
health care. This follows from the fact that healthcare is primarily about services, and not about
providing income replacement. This calls for a different approach to studying retrenchment in
healthcare. One that takes a broader view of healthcare and does not relegate itself to looking at
financing.
There are studies that have reckoned with the difference between cash benefits and services. In this regard, Bambra’s (2005) approach to the study of health care politics tries to
elaborate on this distinction. Bambra argues that welfare states differ with regard to how much
value they place on service provision or cash benefits. Some welfare states, notably those that
belong to the social democratic welfare regime, spend more on services and cash benefits, whereas
liberal and conservatives spend comparatively little on services. Unlike other authors
(Esping-Andersen, 1990; Ferreira, 1996) who have classified welfare states based on cash benefits
schemes, she classifies welfare states based on the types of in-kind benefits they provide. Taking
a more indirect approach, some authors have also linked the specific political traditions of
countries to differences in health outcomes. In this line of research, the argument goes as follows:
Belonging to a specific welfare regime implies presence of a particular political tradition, i.e. social
democratic, Christian democratic and liberal traditions. These political traditions in turn structure
social outcomes through the types of welfare arrangements that are likely to be in place. Lastly,
these social outcomes affect health outcomes (Hurrelmann et al., 2011; Eikemo et al., 2008).
This is something Navarro and Shi (2001) argue as well. Examining the significance of
partisanship and policies implemented by parties in government on inequality, and by extension
their [political parties’] impact on health inequalities. They conclude that, political parties in
government affect levels of inequality though redistributive policies they implement. This in turn
affects concrete health outcomes such as infant mortality. They find that social democrats are both
most inclined to redistribute and also associated with the highest scores for health outcome
indicators. Furthermore, the Christian democratic and liberal tradition also differ with regards to
how much they redistribute and the central institutions for delivering and organising health care
(Navarro & Shi, 2001). These studies thus suggest that politics seems to matter not only for
expenditure levels. Instead, politics also has implications for how services are organised and these
choices result in different outcomes. There are thus also qualitative differences between how
17 Esping-Andersen (1990, chapter 2), Korpi and Palme (2003), Korpi (1989; 1998) and others in the
power resource school who also emphasise the social rights accorded by different welfare states.
These qualitative differences have been studied using a social rights perspective. Social
citizenship refers to the rights and duties of individuals in society to benefits and services that
allow them to meet social needs enhance their capabilities and guarantee the resources necessary
to finance them. Social citizenship is based on three values, namely: reciprocity, inclusion and
trust (Taylor-Gooby, 2008: p. 5). Social rights are a critical component of citizenship in most
welfare states. As such, social rights are accorded to individuals as part of their rights as citizens.
Social rights can, however, also be based on employment as is often the case for example with
schemes such as unemployment insurance (Korpi, 1989: p. 310). This is the case with Esping-Andersen’s conception (1990). According to him benefits are provided as social rights, i.e.
decommodifying, when they at least allow for an individual to exit the market freely and not
experience large drop-off in quality of living (Stephens, 2010: p. 512).
Health care can be commodified as well. Social citizenship in health care includes an
entitlement to health care and is fundamentally aimed at eliminating this commodification
(Bambra, Fox and Scott-Samuel, 2006: p. 188). It is conceivable that the forces exerting downward
pressure on welfare states, also result in a reduction in the degree to which health care can be
provided as a social right. To empirically verify this claim, a number of aspects of health care
systems can be studied. Health care systems can be classified along three dimensions: service
provision, financing and regulation. Service provision entails the main health services, i.e.
inpatient and outpatient care, dental care and provision of pharmaceuticals. Financing pertains to
method of financing health care, e.g. social insurance, taxes or private and out of pocket expenses.
Lastly, regulation pertains to coverage, access of users to provider’s services and remuneration of
providers (Böhm et al., 2013: p. 260). These three dimensions can be used to gauge the degree to
which health care is commodified, or decommodified.
Some researchers have tried to map these qualitative differences and tried to find
distinctions in health care policy output. Montanari and Nelson (2013a), for instance, have
examined the role of partisanship in shaping healthcare reform. Approaching the topic via a social citizenship perspective, they focused on service provision. Their approach differs from Bambra’s
18 commodification and decommodification in health care is a function of whether services are
privately or publicly provided, and whether provision is privately or publicly organized. Publicness
indicates collective risk sharing. Bambra equates this with smaller probabilities of exclusion or
being denied important services which could be more prevalent in private schemes. But this is at
odds with studies that find that retrenchment and restructuring is often more probable and severe
in national health systems (NHS) (Giaimo, 2001: pp. 339-340). This effect is likely mediated by
private or public financing. Therefore, the difference between private and public coverage is a
fruitful way to classify health care systems. It is not the most suitable way to study retrenchment
though. Because health care is fundamentally about service provision. Whether services are
organised publicly or privately, whether costs are public or private matters of course. However,
they need not have any bearing on the degree to which health care can be provided as a social right.
Accounting for service provision in research is thus a more promising track.
2.4 Hypotheses
Having argued that studies of retrenchment in health care should incorporate more facets of health
care than financing, the specific expectations to be tested are more ambiguous. There are
theoretically grounded reasons for why partisanship could matter in health care. What is apparent,
though, is that health care is a policy area where partisanship may matter, but in more constrained
ways than in other policy areas. Jensen (2011: p. 913) provides a theoretical account of the different
preferences of left and right wing parties in health care. He posits that health care politics differ
from the politics of other areas of social policy, which have a more direct link to the labour market.
This is a function of generic social risks being correlated with income, whereas health risks are
only weakly correlated with income, and instead, mainly related to life-course risks. Furthermore,
right wing parties practice a form of marketization via compensation. This essentially means that
they will – for electoral reasons – spend roughly as much as the left. Right parties will behave this
way in order to avoid alienating middle class voters who would otherwise be harmed by pure
private provision and financing of health care. However, they will do their best to ensure private
or market based health provision, i.e. through supplementary systems of health care. This has two
advantages: private provision is likely to be used by high incomes and second may instil in the
population a form of market values and loyalties (in some the opposite of broad solidarities
19 healthcare is going to differ to a degree from other policy areas. It will not be based entirely on the
distribution of risks.
Gingrich’s (2011) provides a comparable account of policy preferences of left, right and confessional party’s. According to her, left and right wing parties organise markets for public
services differently in ways that reflect their own relative ideological predispositions. Accordingly,
left parties are more likely to favour linking the fates and risks of individuals in different classes,
so as to engender collective solidarity. Right parties, in contrast, favour more private involvement
and greater competition, less generous schemes and are more likely to pursue reforms that
fragment risks (Gingrich, 2011: pp. 37-38). These changes are often independent of private or
public financing.
Therefore, left wing parties will likely support public provision of health care, public
funding of health care and universal and broad coverage. Confessional and right parties will likely
be more willing to have a larger share of health care financing privately taken care of, be more
willing to introduce and tolerate supplemental systems and more likely to fragment risks where
possible. To test for the results of these different preferences on health care, the impact of partisan
makeup of government on the three dimensions of health care systems will be tested Based on the
following reading, the following hypotheses have been formulated:
The first hypothesis tests the dimension of health care where political contestation should
be most similar to that of other social programs. That is because the financing of health care is
fundamentally also about how risks are shared. To test for the differences between left,
confessional and secular right wing parties on health care financing, the first hypothesis is as
follows:
H1a: Left party cabinet seat shares is associated with increases in the public share of HCE. H1b: Confessional party cabinet seat shares is associated with smaller increases in the public share of HCE.
H1c: Secular and conservative right party cabinet seat shares are associated with stabilisation or small increases in the public share of HCE.
Hypothesis two and three will be used to test for the effects of the partisan makeup of government
on the availability of health care resources, which are critical for ensuring the social right to health
20 Taking Montanari and Nelson (2013a; 2013b) as starting point, and considering what previous
studies have shown about health care regimes, the following hypotheses has been formulated:
H2a: Left and Confessional party participation in cabinets are associated with increases in the number health care resources available.
H2b: Secular and conservative right party cabinet seat share is associated with weaker growth, or even declines in the number of health care resources available.
H 3a: Left parties cabinet seat shares is most strongly associated with increases in employment in health care sector.
H3b: Confessional party cabinet seat share is less so associated with increases in employment in health care sector.
H3c: Secular and conservative right parties are associated with the smallest increase – or potentially even with decreases – in employment in the health care sector.
Hypothesis four tests the effects of partisanship on regulation of access to health care. It extends
the argument from hypothesis one. Specifically assuming that different parties have different
degrees of preference and commitment vis-à-vis types of health insurance coverage. Even if parties
do not differ on how they finance health care, they should care whether or not health insurance is
privately organized or publicly organized. As such, hypothesis 4 is as follows:
H4a: Left party cabinet seat share is associated with the largest share of the population covered and the largest share covered in public schemes.
H4b: Confessional party cabinet shares are associated with smaller shares of the population covered and smaller shares covered in public schemes.
This is expected to be a result of Christian democrats’ commitment to the principle of subsidiarity
and their preference for the social insurance model (Van Kersbergen, 1995: p. 2).
H4c: Secular and conservative right parties are associated with the smallest shares of the population covered and coverage of a smaller share of the population in public schemes.
Hypothesis 5 tests a claim advanced by the new politics theory. It tests whether or not path
dependency explains developments in health care. One of the takeaways from the new politics
thesis is that welfare programs are resistant to change and that they are path dependent. The fifth
hypothesis is thus as follows:
21
H5b: The value of total health care expenditure in 1981 is associated with public share of health care financing in the period analysed.
H5c: The values of health care resources in 1981 are associated with health care resources in the period analysed.
H5d: The value of coverage in 1981 is associated with coverage in the period analysed.
In accordance with the power resource theory, labour unions are assumed to pursue similar
outcomes as left parties. Hence the expected association between trade union density and the
various outcome variables is in the same direction as with left parties.
3. Methodology
The research design used for this study will be a Large-N statistical analysis. The aim of this study
is to test whether the power resource theory or the new politics theory hold up as explanations for
the developments in the health care system of various OECD members. The goal is thus
explanatory in nature. Additionally, this study tries to replicate and test claims advanced by
previous studies for robustness (Leavy, 2017: p. 89). The politics of health care can be studied
using multiple designs, such as Small-N research designs, e.g. by performing single case studies Table 1: Summary of hypotheses
Variable Expected association
Hypothesis 1 Left cabinet share
Christian democratic cabinet share
+ +
Right cabinet share 0/+
Hypothesis 2
Left cabinet share +
Christian democrat 0/+
Right cabinet share -/0
Hypothesis 3 Left cabinet share
Christian democrat cabinet share
+ +
Right cabinet share -/0
Hypothesis 4
Left cabinet share +
Christian democratic cabinet share 0/+
Right cabinet share 0
Hypothesis 5
22 or comparative case study designs. These designs lend themselves to accounting for particular
outcomes, or identifying the motivations of actors involved in the process. For establishing general
patterns, however, Large-N designs are more suitable. This applies to the current study, as the goal
is to gauge whether there is a relationship between partisanship and organization of health care.
To accomplish this, this study compares of a large number of cases on a limited number of relevant
variables across a sufficiently large number of years (Toshkov, 2016: p. 256; Huber & Stephens,
2001: p. 37).
This thesis will analyse pooled data, that is, time-series-cross-sectional (TSCS) data. It
includes 33 time periods and 21 units, which yields (in the most optimal scenario) 735 observed
values per variable. The specific statistical analysis technique used is linear regression. TSCS have
observations on set number of units, in these studies countries are units, for multiple time periods.
Ordinary least squares (OLS) models cannot be carried out, or at least yield inaccurate estimates,
without regard for the fact that time-series data in TSCS likely violates core assumptions of the
OLS models. In particular, the assumptions of homoscedasticity and an absence of correlation of
standard errors in units at different time periods is potentially violated as observations are rarely
independent of each other (Beck and Katz, 1995: pp. 534-636). The use of panel corrected standard
errors (PCSE) helps to account for the heteroscedasticity and autocorrelation in standard errors
(Plümper, Troeger & Manow, 2005: p. 330). Using PCSE with a lagged dependent variable can
counteract these deficiencies of TSCS. However, the inclusion of the lagged dependent variable
as an explanatory variable can also be problematic, as this could artificially reduce the explanatory
power of other independent variables. So all the tests will also be conducted by differencing the
dependent variables. These additional tests serve as a robustness check. (Janoski & Isaac, 1993: p.
33).
The research design applied in this study has the advantage of being highly reliable. The
variables constructed and results produced using this data can be replicated by other scholars. The
data used for this study is freely available from authoritative organizations such as the OECD.
Regarding validity, the results are only generalizable to a set of industrialised democratic countries. So this study’s external validity is limited to the set of countries studied and other similar countries.
Another limitation of TSCS includes the somewhat uncertain validity of inferences across cases.
23 so for other units. This is an innate feature of TCSC and has to be considered when interpreting
results.
3.1 Case selection and operationalization
Cases have been selected for their theoretical relevance and availability of data to conduct analysis.
The analysis includes 21 members of the OECD from 1981 until 2014. This is an appropriate
starting point as the 1970s are often considered the end of the old politics era, signalling the
paradigm shift to the new politics era. The following countries included in the analysis: Australia,
Austria, Belgium, Canada, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Japan, the
Netherlands, New Zealand, Norway, Portugal, Spain, Sweden, Switzerland, United Kingdom and
the United States. These countries are highly comparable on the theoretically relevant dimensions.
This means that all of these countries are industrial welfare states, and all countries were
democracies in the period under analysis. This makes the partisan accounts potentially relevant.
Some scholars prefer to exclude countries such as Portugal, Greece and Spain from the analysis;
they are not mature democracies and thus the dynamics of democratic politics may differ in those
countries (Huber and Stephens, 2001: p. 33). It is conceivable the shift to the new politics context
did not arrive in these countries at the same period in time it did for other OECD countries. As
such, these cases may inflate the effect of the power resource account. A number of other studies
include these countries however. Therefore, in the interest of comparability, the analysis conducted
includes Spain, Greece and Portugal. The tests will also be run excluding Spain, Portugal and
Greece to see if excluding these countries changes the results substantially.
3.2 Dependent variable
In debates about welfare retrenchment or resilience, the exact operationalization of the dependent
variable used could affect the results. Using aggregate or per capita expenditure data, using
replacement rates or net replacement rates yields different results (Allan and Scruggs, 2004;
Green-Pedersen, 2004; Esping-Andersen, 1990; Starke, 2006: p. 112). An examination of the
dependent variable used in studies of retrenchment of health care shows numerous authors using
public share of health care as dependent variable (Jordan, 2011; Potrafke, 2010). The public share
does not incorporate important features such as tax expenditures, subsidies or other more nuanced
24 organized, how costs and risk are distributed and shared (Brady et al, 2016: pp. 356-357).
Therefore, to gauge retrenchment in the financing of health care, the public share of health care
expenditures is used.
It is worth noting that retrenchment in these studies does not mean reductions in total health
care spending. Retrenchment reflects a decline in the public share of total healthcare spending, or
a decline in the public share of health spending as a percentage of GDP. This difference between
the specific ways of measuring it could have consequences: when the public share is expressed as
a share of GDP, the public share of health care may decline or increase irrespective of changes to
health care expenditures. This would not be the case when public health care expenses are
expressed as a share of overall health care expenses. Therefore, to gauge retrenchment in the
financing of health care, the public share of health care expenditures is used for this study. As
health care financing is but one dimension that characterizes the performance of health care
systems, the other two dimensions, regulation and health care provision, need to be accounted for
as well. Montanari & Nelson (2013a: pp. 261-262) operationalized health care provision as an
additive index, which is comprised of: health employment (number of nurses and physicians per
1000 inhabitants), hospital beds and medical technology (additive index of five categories of
medical technology per 1000 inhabitants). For this study, health care resources are operationalized
in the following two things: first, the number of physicians (additive index of nurses and physicians
per 1.000 residents). Second, the number of hospital bed. This is also an additive index comprising
the number curative and hospital beds per 1.000 residents. The variable health employment is also
included to gauge the importance of health care and social employment in the economy. This
variable is expressed as health care and social employment as a share of overall civilian
employment (OECD, 2016). Lastly, for regulation, this study includes an additive index of
coverage in public scheme and overall coverage. The score ranges from 0 to 200. This variable is
meant to give an indication of how accessible the health care system is. As is customary, this study
includes lagged values of all variables to account for time lag between changes in partisan
distribution of power and policy responses (Fervers et al., 2016: p. 365).
3.3 Independent variable
For the main independent variable of interest, partisan power, previous studies have used multiple
25 at cabinet seat shares of left, right and Christian democratic parties. This approach is an
appropriate way of studying power resources. This study will use the cabinet composition as the
main measure of partisanship. However, it is important to note that there are other approaches to
operationalizing this variable. Another method of operationalizing cabinet composition is the
Schmidt index for government ideology. It is a five-point scale indicating dominance of right and
centre parties in government. The value 1 indicates hegemony, 2 indicates dominance of the right,
3 indicates parity, 4 dominance of the left and 5 hegemony of the left. A notable drawback of the
Schmidt index is that it does not include an independent measure of Christian democrats in
government. The assumption underlying the Schmidt index seems to be that the difference between
left and right wing parties is the only relevant one. This makes the Schmidt index an unsatisfactory
indicator for this study. However, a number of other studies into health care retrenchment use the
Schmidt index. In the interest of comparability, the tests will also be run using Schmidt index to
test whether this significantly alters the estimation of partisan effects.
The other main power resource independent variables used will be unionization rate. This
is a superior and more relevant approximation of union strength than other measures such as
collective bargaining coverage rates, or wage bargaining centralization. It directly relates to union’s strength at that moment. Health insurance is an important fringe benefit in some countries.
However, this is often not the case. Using unionization rate should capture the effects of union
strength for countries where health care is a fringe benefit and where health insurance is provided
by the government. The per capita GDP growth rate is also included to account for health care
spending being driven by increases in income and improvements in the overall economy. The net
government deficit is included to account for budgetary pressures which might drive retrenchment.
Total social expenditure is included to capture whether or not potential retrenchment in health care
is compensated by increasing social expenditures in other programs. The dependency ratio is
included to control for the effects of elderly or underage population as explanatory factors of
budgetary pressure. The KOF globalisation index is also included in the analyses to assess whether
increased openness and international competition disciplines welfare states to pursue retrenchment
26 Additionally, this study has included a dummy variable for single party government (1 if
single party majority government, 0 for all other types of governments). This variable is included
to account for the fact that single party governments face fewer restraints in pursuing their ideal
policy goals than coalition or minority governments do. They do not have to rely on coalition
partners or others in parliament to legislate. I have also included an interaction term between single
party government and right wing cabinet share, this variable accounts for single party governments
formed by the right wing. Additionally, constitutional constraints are included as well. This
variable is included to assess whether states with more constraints in policymaking and veto
players present in the system exhibit some status quo bias. It hampered expansion in the old politics
era, and halted retrenchment in the new politics era (Huber, Ragin and Stephens, 2001: p. 32). The
ability of governments to unilaterally impose cost containment is lower in social and private health
insurance systems due to various factors, e.g. corporatism and the role of social and private actors
in regulating access and provision (Fervers et al, 2016: p. 202; Böhm et al, 2013). Whereas in
National Health Service systems, the capacity for governments to act is larger and they can more
directly enact cost containment measures. To account for this, this study uses state run health care
system as an additional control variable. The expectation is that countries with state run health care
systems will be successful in imposing cost containments and reducing the availability of health
care resources. Lastly, the values of the dependent variable at 1981 are included, in order to assess
whether path dependency accounts for outcomes. This test is meant to rule out whether the
arrangements in 1981 explain the outcome in 2014.
Table 2: Summary of association with non-power resource independent variables
Control variable Expected association
Social expenditure -
Deficit -
Dependency ratio +
GDP growth +
Single government -/+
Right wing single party government -
Globalization -
Centralization of health care system -
27
Table 3: Overview of variables used
Operationalization Source
Dependent variable
Health care financing Share of total health care expenditures that is publicly financed OECD (2017c)
Total health care expenditure as a percentage of GDP
Health care regulation Additive index combining share covered by the largest public
scheme and overall share covered with health insurance
OECD (2017c)
Health care resources Hospital beds per 1.000 inhabitants combined with curative care beds
per 1.000 inhabitants
OECD (2017c)
Physicians per 1.000 inhabitants combined with nurses per 1.000
inhabitants
Health and social service employment as a share of civilian
employment
Independent variable
Left cabinet Share of cabinet seats held by social democratic parties and parties
to their left
Swank (2013)
Right cabinet Share of cabinet seats held by secular and conservative right wing
parties
Swank (2013)
Christian democratic cabinet
Share of cabinet seats held by Christian democratic parties Swank (2013)
Schmidt index Cabinet composition: (1) hegemony of right-wing (and centre)
parties, (2) dominance of right-wing (and centre) parties, (3)
balance of power between left and right, (4) dominance of
democratic and other left par-ties, (5) hegemony of
social-democratic and other left parties.
Armingeon et al (2017)
Union density Net union membership as a proportion of wage and salary earners in
employment.
Visser (2016)
GDP growth Growth of real GDP, percent change from previous year OECD (2017b)
Dependency ratio Age dependency ratio is the ratio of dependents–people younger than
15 or older than 64–to the working-age population–those ages 15-64.
Jan et al (2018)
Social security expenditures Total public and mandatory private social expenditure as a percentage of GDP.
OECD (2017a)
Government deficit Annual deficit (overall balance / net lending of general government)
as a percent-age of GDP.