Percutaneous transluminal coronary revascularization procedures (PCI) traumatize the arterial wall, leading to platelet activation, increased thrombin generation and activity, and intracoronary thrombosis.1-6Activation of the platelet glycoprotein (GP) IIb/IIIa receptor is the final common pathway of platelet aggregation.7 Treat-ment of patients with inhibitors of the GPIIb/IIIa inte-grin during interventional procedures has been shown
to decrease acute ischemic complications in large prospective studies.8-12The mouse-human chimeric monoclonal antibody abciximab (c7E3 Fab, ReoPro), which blocks GPIIb/IIIa and the related αVβ3receptor,13 inhibits platelet aggregation.14,15Although abciximab has also been shown to decrease thrombin generation in vitro,16it has not been determined whether it exerts an antithrombin effect in vivo.We have recently shown that the addition of abciximab to aspirin plus heparin during coronary interventional procedures decreases both platelet thrombus formation and fibrin deposition in an ex vivo model of thrombosis on an injured vascular sur-face under dynamic flow conditions.17
In this study, we investigated the effect of abciximab treatment during coronary interventional procedures on thrombin generation and thrombin activity in vivo as assessed by the change induced in activated clotting time (ACT) and plasma levels of prothrombin fragment
with abciximab on thrombin generation and
activity during percutaneous coronary intervention
George Dangas, MD, Jonathan D. Marmur, MD, Traci E. King, BS, Joshua De Leon, MD, Samin K. Sharma, MD, Raghuraman Vidhun, MD, Dmitriy Feldman, BA, Michael Y. Stoynov, BA, Juan J. Badimon, PhD, and John A. Ambrose, MD New York, NY
Background
Antagonists of the platelet glycoprotein IIb/IIIa decrease acute ischemic complications after percutaneous coronary interventions (PCI). Abciximab (c7E3 Fab, ReoPro) has been reported to decrease thrombin generation in vitro. We investigated in vivo the effect of abciximab therapy on thrombin generation, thrombin activity, and the activated clotting time (ACT) during PCI.Methods
We studied 32 consecutive patients who underwent PCI for unstable coronary syndromes. Group I (n = 11) was treated with heparin plus aspirin, and group II (n = 21) was treated with heparin plus aspirin plus standard-dose abcix-imab, administered 5 minutes after the initial heparin bolus. Patients received a standardized heparin bolus at time 0, and arterial blood specimens for prothrombin fragment F1.2, fibrinopeptide A (FPA), and ACT were obtained from the guiding catheter at 5 minutes, 10 minutes (ACT only), 20 minutes, and at the end of the PCI. Standard-dose abciximab was adminis-tered in group II only. Each patient served as his or her own control, and the changes against the baseline were compared between the 2 groups.Results
There were no significant differences between the 2 groups regarding baseline characteristics, hematocrit, and platelet count. Group I patients had higher ACT and lower F1.2 and FPA compared with group II at baseline. Subsequent measurements demonstrated a gradual decrease in FPA and F1.2 in group II; the end of procedure versus baseline changes that occurred in F1.2 were significantly different compared with group I (decrease of 0.59 ± 0.22 nmol/L in group II vs increase of 0.22 ± 0.3 nmol/L in group I, P= .04), and a trend in the same direction was evident for FPA changes (decrease of 1.46 ± 1.16 ng/mL in group II vs increase of 2.25 ± 1.58 ng/mL in group I, P= .07). The ACT response to abciximab was variable, but a 6.3% increase (+20 sec) in ACT was documented 5 minutes after abciximab bolus in group II compared with the 3.4% decrease (–10 sec) observed in group I at the same time point (P= .1).Conclusion
Addition of abciximab to heparin plus aspirin during PCI was associated with a significant decrease in thrombin generation and a borderline decrease in thrombin activity. (Am Heart J 1999;138:49-54.)From the Cardiovascular Institute, Mount Sinai School of Medicine.
Supported in part by grants 19278 and 54469 from the National Heart Lung and Blood Institute and by grant 5 M01 RR00071 to the Mount Sinai General Clinical Research Center from the National Center for Research Resources, National Insti-tutes of Health.
Submitted June 26, 1998; accepted September 18, 1998.
Reprint requests: Jonathan D. Marmur, MD, Box 1030, Mount Sinai Medical Cen-ter, New York, NY 10029-6574.
E-mail: [email protected] Copyright © 1999 by Mosby, Inc. 0002-8703/99/$8.00 + 0 4/1/95343
F1.2 and fibrinopeptide A (FPA).18,19We report that the addition of abciximab was associated with significantly decreased thrombin generation.
Methods
All patients transferred to the Mount Sinai Hospital, New York, for PCI after diagnostic angiography performed at the City Hospital Center at Elmhurst, Queens, from March to July 1997 were eligible for enrollment in this study.A single inter-ventionalist (J.D.M.) performed all procedures. Inclusion crite-ria were the presence of an unstable coronary syndrome or an angiographically high-risk lesion. Exclusion criteria included restenosis, acute myocardial infarction (primary or rescue inter-vention), thrombocytopenia, or bleeding disorders.The values of F1.2, FPA, and ACT were periodically measured during the intervention according to the study protocol.The study was approved by the Institutional Review Board at Mount Sinai Hos-pital, and all enrolled patients gave written informed consent.
Definitions
In this study, unstable coronary syndrome was defined as unstable angina Braunwald classes II (rest pain), III (rest pain within 48 hours), B (primary) or C (postinfarction).20High-risk
lesions were defined as complex lesions by Ambrose criteria21
or lesions of type B2or C according to the American Heart
Association/American College of Cardiology classification.22
Study protocol
Patients were divided into 2 groups: group I was composed of patients treated with heparin plus aspirin during the inter-vention; group II was composed of patients treated with abciximab in addition to heparin plus aspirin.Abciximab was administered in patients with Braunwald class III or C unstable angina (group II), whereas patients in classes II and B were treated with heparin and aspirin only (group I, control).
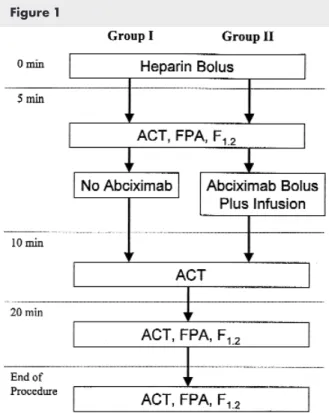
The study protocol is outlined in Figure 1.All patients had a complete blood count, platelet count, and prothrombin time/international normalized ratio preprocedure. Patients received a heparin bolus at time 0 (Table I); the first blood drawing was performed at 5 minutes, and then group II received standard-dose abciximab. Further blood drawings were performed at the 10-minute and 20-minute time points and at the end of the procedure.All arterial blood specimens were obtained from the 8F guiding catheter, positioned at the coronary ostium, after discarding the first 10 mL of blood. During blood withdrawal, the guiding catheter was either empty (beginning and end of procedure), or had a 0.014-inch diameter coronary guide wire (during the procedure). Blood samples were never drawn with devices other than the coro-nary guide wire inside the guiding catheter lumen.
The initial heparin bolus was adjusted according to the ACT value in patients already treated with heparin (Table I). Dur-ing all procedures, the ACT was targeted at 350 to 400 onds for the control group (group I) and at 300 to 350 sec-onds for the abciximab group (group II), with administration of additional heparin boluses as needed after obtaining the 10-minute specimen.
Laboratory determinations
At each time point the ACT value was calculated as the mean of 2 measurements performed simultaneously with a Hemochron 8000 (INC, Edison, NJ) in the catheterization laboratory.
Blood for F1.2 (4 mL) was collected in a citrated tube, and blood for FPA (4 mL) was collected in a PPACK-coated tube (Hematologic Technologies, Inc).All specimens were cen-trifuged at 3000gfor 15 minutes, and the plasma was sepa-rated and frozen at –70°C.The plasma F1.2 and FPA levels were measured with commercially available enzyme-linked immunosorbent assays (Enzygnost F1.2 by Behring Diagnos-tics,Westwood, Mass, and Asserachrom FPA by Diagnostica Stago,Asnieres-sur-Seine, France) by a single operator (T.E.K.) blinded to the specimen origin.
Heparin bolus (U/Kg)
ACT (sec) Group I Group II
<150 125 70
150–200 75 40
200–250 50 25
250–300 25 10
>300 None None
Table I. Nomogram calculation of initial bolus of heparin (at time 0) for patients already receiving heparin infusion before procedure
Figure 1
Outline of study protocol. All blood specimens were obtained from coronary ostium through guiding catheter after discard-ing first 10 mL of blood withdrawn.
Revascularization procedure
All interventions were performed with the transfemoral approach by an 8F arterial sheath.All stents were electively deployed with high pressure (16 to 18 atm for 30 sec, balloon-to-artery ratio 1.0) and without intravascular ultrasound guid-ance.The balloon-to-artery ratio during balloon angioplasty was 1.0 to 1.1 with an inflation pressure 6 to 8 atm for 100 seconds. Patients who received stents received the first dose of ticlopidine after completion of the intervention. Rotational atherectomy was performed when appropriate with the stepped burr approach, a final burr-to-artery ratio of 0.7, and with adjunctive balloon postdilatation at 2 to 4 atm for 100 seconds. Procedural success was defined as <30% final diame-ter stenosis and absence of dissection or major complications, such as death, infarction, or need for bypass surgery.
Statistical analysis
The study design allowed each patient to serve as his or her own control.The changes that occurred at 20 min versus base-line and at the end of the procedure versus basebase-line in plasma F1.2 and FPA were obtained in each group.The primary end points were the differences in these observed changes in F1.2 and FPA in the abciximab group (group II) compared with the control group (group I).A secondary end point was the com-parisons of the observed changes in ACT values between the 2 groups at the 10-minute specimen versus baseline. Continuous variables were expressed as mean ± SE and compared with a 2-tail Studentttest; categoric variables were compared with Fisher’s exact test.The statistical software JMP 3.2 (SAS Insti-tute, Cary, NC) was used for all analyses.With respect to the primary end points, the Bonferroni correction (multiple com-parisons) was used and the corrected statistical significance was considered a 2-tailed probability value ≤.04. Other between-group comparisons were considered significant if the 2-tail Pvalue was <.05.
Results
Of 46 patients transferred for coronary interventions during the study period, 14 were excluded because of acute myocardial infarction (n = 3), restenosis (n = 4),
Braunwald class I angina (n = 3), or stable angina with-out a high-risk lesion (n = 4).The remaining 32 patients comprised the entire population: 11 patients in group I (control) 21 patients in group II (abciximab treated).
There were no significant differences between the 2 groups of patients regarding clinical or angiographic characteristics (Table II). Groups I and II had similar val-ues in platelet count (236 ± 20 ×103/dL vs 218 ± 15 ×103/dL), hematocrit (38.6% ± 1.2% vs 38.5% ± 0.9%), and international normalized ratio (1.0 ± 0.1 vs 1.1 ± 0.1).Total procedural heparin doses were 8036 ± 561 U in group I versus 4700 ± 406 U in group II (P< .01). The procedural duration was 74 ± 13 minutes in group I compared with 96 ± 9 minutes in group II (P= not significant [NS]). Rotational atherectomy was per-formed in 4 patients in group I and 12 patients in group II (40% vs 57%,P= NS), and stents were placed in 2 patients in group I and 3 patients in group II (20% vs 14%,P= NS).All other patients were treated with bal-loon angioplasty.All procedures were successful and all patients were discharged home the day after the inter-vention without any complications.
Thrombin generation and activity
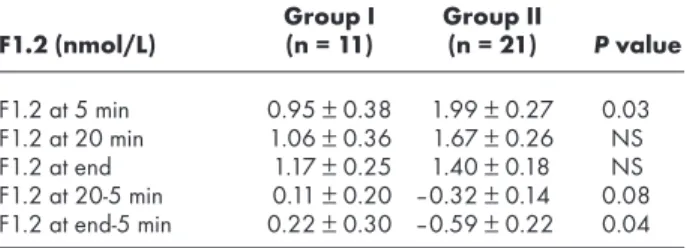
Changes in thrombin generation as assessed by the plasma F1.2 levels are shown in Table III.At the 5-minute specimen after heparin bolus (baseline F1.2), there was evidence of significantly higher F1.2 levels in group II versus group I (1.99 ± 0.27 nmol/L vs 0.95 ± 0.38 nmol/L,P= .03). During the procedure, F1.2 levels gradually increased in group I but gradually decreased in group II.The observed changes from baseline were borderline different at 20 minutes into the procedure (P= .08) and significantly different at the end of proce-dure (decrease of 0.59 ± 0.22 nmol/L in group II vs increase of 0.22 ± 0.3 nmol/L in group I,P= .04).
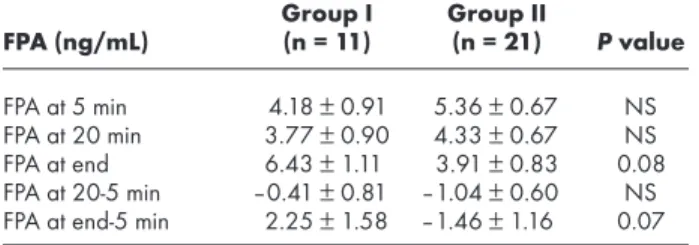
Plasma FPA levels were also somewhat higher in group II compared with group I at the 5-minute speci-men after heparin bolus (baseline FPA), but the differ-ence was statistically nonsignificant (Table IV).At subse-quent blood specimens, FPA levels decreased gradually in group II, and the observed end of procedure versus baseline change was of borderline significance when Table II. Patient characteristics
Group I Group II (n = 11) (n = 21) Pvalue Age (y) 61.3 ± 3.8 59.9 ± 2.8 NS Male 9 (81.2) 18 (85.7) NS Diabetes mellitus 2 (18) 7 (33) NS Hypertension 3 (27) 14 (67) 0.03 Hyperlipidemia 1 (9) 11 (52) 0.01 Smoking 4 (36) 4 (19) NS
Heparin before procedure 3 (27) 13 (62) NS Prior infarction 7 (63) 10 (48) NS LAD intervention 5 (45) 10 (47) NS LCX intervention 1 (9) 4 (19) NS RCA intervention 5 (45) 7 (33) NS Values as mean ± SE or n (%).
LAD,Left anterior descending coronary artery; LCX,left circumflex coronary artery; RCA,right coronary artery.
Group I Group II F1.2 (nmol/L) (n = 11) (n = 21) Pvalue F1.2 at 5 min 0.95 ± 0.38 1.99 ± 0.27 0.03 F1.2 at 20 min 1.06 ± 0.36 1.67 ± 0.26 NS F1.2 at end 1.17 ± 0.25 1.40 ± 0.18 NS F1.2 at 20-5 min 0.11 ± 0.20 –0.32 ± 0.14 0.08 F1.2 at end-5 min 0.22 ± 0.30 –0.59 ± 0.22 0.04 Time points are after administration of the heparin bolus (time 0). Abciximab was administered in group II immediately after obtaining the 5-minute specimen.
compared with the change observed in group I: a decrease of 1.46 ± 1.16 ng/mL in group II versus an increase of 2.25 ± 1.58 ng/mL in group I (P= .07).
ACT values (Table V) were within the target range in both groups in all specimens obtained.ACT was sig-nificantly lower in group II compared with group I at the 5-minute specimen (baseline ACT) and at 20 min-utes into the intervention, and there was a trend in the same direction in specimens taken at the end of the procedure.Abciximab was administered in group II patients immediately after obtaining the 5-minute specimen (Figure 1); therefore the 10-minute speci-men is the first one obtained after the initiation of abciximab administration in group II and before the administration of additional heparin in any patient. In the 10-minute specimens, we observed wide variation in ACT. Overall, an increase was noted in the ACT in group II patients compared with baseline, and this change was of borderline significance compared with the respective change in group I: a 20 ± 13 second increase in group II versus a 13 ± 18 second decrease in group I,P= .1.The observed changes at the 20-minute and the end of procedure specimens com-pared with baseline were not statistically different between the 2 groups.
Discussion
The antiplatelet effect of GPIIb/IIIa receptor blockade with abciximab has been previously documented.14,15 In a recent study, we quantified ex vivo thrombus for-mation under dynamic flow conditions and demon-strated that abciximab significantly inhibited both platelet thrombus and fibrin deposition on an injured arterial surface compared with heparin and aspirin ther-apy alone.17Cadroy et al23have also documented decreased fibrinogen deposition when nonhuman pri-mates were treated with a GPIIb/IIIa receptor antago-nist, but Weiss et al24have described increased fibrin deposition when the blood of patients with Glanz-mann’s thrombasthenia (ie, absent GPIIb/IIIa receptor) was passed through a flow chamber.Although not entirely consistent, these results suggest that inhibitors of GPIIb/IIIa may exert an antithrombin effect.
In this study, we sought to determine in human beings the in vivo effect of abciximab in thrombin gen-eration and activity by determining the plasma levels of F1.2 and FPA and the ACT values during coronary inter-ventional procedures. Our results indicate that
decreased thrombin generation and trends toward decreased thrombin activity and increased ACT values are evident with abciximab.This in vivo report is con-sistent with prior experimental findings of our group and others.17,23,24
Effect on thrombin generation and activity
The abciximab-treated group had higher levels of F1.2 and FPA at the beginning of the procedure com-pared with the control group.This finding was rather expected because the study population was not ran-domly assigned to the treatment offered.Abciximab was administered in a relatively higher risk group of
patients, including those with severe unstable angina21 and angiographically high-risk lesions.Additionally, more patients in the same group were already receiving heparin therapy before the procedure. In accordance with the clinical expectation, this group demonstrated increased thrombin generation and activity at the initial blood drawing, suggesting greater predisposition to active thrombosis, compared with the control group. Although the prespecified target ACT during the proce-dure was lower, as was the total heparin dose, there was a significant decrease in thrombin generation and a trend toward decreased thrombin activity in the abcix-imab group compared with the control group.
The mechanism through which abciximab decreases thrombin generation may be caused by the decrease in the total platelet aggregate mass because activated platelets facilitate thrombin generation by providing a surface on which coagulation reactions occur and pos-sibly through other actions.7,16 However, abciximab has been shown to reduce thrombin generation when defibrinated plasma is treated with tissue factor,16 indi-cating a possible qualitative effect of abciximab on thrombin generation.
Group I (control) patients had an increase in thrombin
Group I Group II FPA (ng/mL) (n = 11) (n = 21) Pvalue FPA at 5 min 4.18 ± 0.91 5.36 ± 0.67 NS FPA at 20 min 3.77 ± 0.90 4.33 ± 0.67 NS FPA at end 6.43 ± 1.11 3.91 ± 0.83 0.08 FPA at 20-5 min –0.41 ± 0.81 –1.04 ± 0.60 NS FPA at end-5 min 2.25 ± 1.58 –1.46 ± 1.16 0.07 Time points are after administration of the heparin bolus (time 0). Abciximab was administered in group II immediately after obtaining the 5-minute specimen.
Table IV. FPA values
Group I Group II
ACT (min) (n = 11) (n = 21) Pvalue
ACT at 5 min 384 ± 15 317 ± 11 <.01 ACT at 10 min 371 ± 19 337 ± 14 NS ACT at 20 min 374 ± 18 317 ± 13 0.02 ACT at end 364 ± 18 326 ± 13 0.1 ACT at 10-5 min –13 ± 18 20 ± 13 0.1 ACT at 20-5 min –10 ± 15 1 ± 11 NS ACT at end-5 min –20 ± 21 10 ± 15 NS Time points are after administration of the heparin bolus (time 0). Abciximab was administered in group II immediately after obtaining the 5-minute specimen.
generation and activity despite heparin and aspirin ther-apy.These changes were not statistically significant, implying that there was a mixed response within the group.This finding is consistent with our previous reports that showed increased thrombin generation and activity after procedures compared with before proce-dures in selected cases treated with various types of coronary interventions.25,26The fact that abciximab therapy reduced thrombin generation and activity in a higher risk group (group II) suggests that this agent may inhibit the procedure-related activation of blood coagu-lation.These effects of abciximab may contribute to the mechanism of action underlying its clinical benefit in decreasing ischemic complications after intervention.
Abciximab has also been previously reported to pro-long ACT both when administered to patients27and when added to heparinized blood in vitro.28In our study, we found a mixed response of ACT after abciximab adminis-tration. In group II, abciximab treatment prolonged the ACT 5 minutes after the bolus but had little effect on sub-sequent ACT values. However, the within-group response was mixed at all time points, the post–heparin bolus ACT was not a predictor of the 5-minute post–abciximab bolus ACT, and an ACT >350 seconds after heparin bolus did not necessarily predict further prolongation after abciximab bolus. Overall the average increase in ACT after abciximab bolus compared with baseline was 20 second, which was smaller than that seen in the EPIC trial, although the latter study did not use each patient as his or her own control.27
Abciximab has been shown to decrease the rate of postprocedure asymptomatic non-Q-wave myocardial infarction (creatine phosphokinase release).8-10A possi-ble mechanism of this complication may be intracoro-nary thrombosis during the interventional procedure. Decrease of thrombin generation and activity with abciximab may be specifically targeted against this spe-cific mechanism of ischemic complication and may explain this particularly accentuated efficacy of abcix-imab compared with other GPIIb/IIIa inhibitors in decreasing the incidence of these complications.8-12
Study limitations
In this study, abciximab therapy was directed by the physician to patients who were considered to be at higher risk for ischemic complications than the control group.The fact that patients were not randomly assigned likely resulted in the inclusion of higher risk cases in group II.This potentiality could mask an exist-ing effect of abciximab or decrease the magnitude of a possible antithrombin effect of abciximab.The fact that group II had higher thrombin generation and activity at baseline is consistent with previous studies demonstrat-ing increased thrombin generation with more complex lesion morphologic characteristics.25,26
Although various types of interventional procedures were performed, their distribution between the 2 groups
was similar, and patients receiving stents were given the first dose of ticlopidine after the end of the procedure. Although procedure duration was not different between the 2 groups, it was somewhat longer in the abciximab group.This may be an indicator of more technically diffi-cult interventions, which may indicate that these patients had more reasons for increased thrombotic action. In contrast, thrombin generation and activity were shown to decrease steadily along the procedure in this group, whereas they increased in the control group despite the shorter duration of the procedure. On the other hand, the “normal range” of FPA and F1.2 levels has not been well defined, and it is possible that their variability might have affected our findings. However, both groups had baseline FPA and F1.2 levels higher than those observed previously by us in stable angina.25,26
The efficacy of antithrombotic medications may differ in static compared with dynamic flow conditions.The peptides measured in this study were withdrawn from the coronary ostium, proximal to the lesion, and there-fore represent systemic levels, which may differ from those existing at the lesion site. However, because the evaluated antithrombotic regimen was administered systemically, the importance of this potential error may be small. Finally, to minimize the variability in the labo-ratory assays, we had the same investigator perform all the studies in a blinded fashion after completion of the study, and individual patient specimens were run on the same plate.
Conclusion
Our data suggest that treatment with the platelet GPIIb/IIIa inhibitor abciximab reduces thrombin gener-ation during coronary interventions and provides an additional mechanism through which GPIIb/IIIa inhibi-tion, and abciximab in particular, produce the clinically beneficial effects observed in coronary interventional trials.10The antiplatelet and antithrombin effects of abciximab may contribute to the mechanism of action underlying its clinical benefit in decreasing ischemic complications after interventions.
References
1. Fernandez-Ortiz A, Badimon JJ, Falk E, Fuster V, Meyer B, Mailhac A, et al. Characterization of the relative thrombogenicity of athero-sclerotic plaque components: implications for consequences of plaque rupture. J Am Coll Cardiol 1994;23:1562-9.
2. Marmur JD, Thiruvikraman SV, Fyfe BS, Guha A, Sharma SK, Ambrose JA, et al. Identification of active tissue factor in human coronary atheroma. Circulation 1996;94:1226-32.
3. Kirchhofer D, Tschopp B, Steiner B, Baumgartner HR. Role of colla-gen-adherent platelets in mediating fibrin formation in flowing whole blood. Blood 1995;86:3815-22.
4. Kumar R, Beguin S, Hemker HC. The influence of fibrinogen and fibrin on thrombin generation. Evidence for feedback activation of the clotting system by clot bound thrombin. Thromb Haemost 1994;72:713-21.
5. Toschi V, Gallo R, Lettino M, Fallon JT, Gertz SD, Fernandez-Ortiz A, et al. Tissue factor modulates the thrombogenicity of human ath-erosclerotic plaques. Circulation 1997;95:594-9.
6. Dangas G, Fuster V. Management of restenosis after coronary inter-vention. Am Heart J 1996;132:428-36.
7. Coller BS, Anderson K, Weisman HF. New antiplatelet agents: platelet GP IIb/IIIa antagonists. Thromb Haemost 1995;74:301-8. 8. EPIC investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in a high risk coronary angioplasty. N Engl J Med 1994;330:956-61.
9. The EPILOG investigators. Platelet glycoprotein IIb/IIIa receptor blockade and low-dose heparin during percutaneous coronary revascularization. N Engl J Med 1997;336:1689-96.
10. The CAPTURE investigators. Randomized placebo-controlled trial of abciximab before and during coronary intervention in refractory unstable angina: the CAPTURE study. Lancet 1997;349:1429-35. 11. The RESTORE Investigators. Effects of platelet glycoprotein IIb/IIIa blockade with tirofiban on adverse cardiac events in patients with unstable angina or acute myocardial infarction undergoing coro-nary angioplasty. Circulation 1997;96:1445-53.
12. The IMPACT II Investigators. Randomized placebo-controlled trial of effect of eptifibatide on complication of percutaneous coronary intervention: IMPACT II. Lancet 1997;349:1422-8.
13. Coller BS. A new murine monoclonal antibody reports and activa-tion-dependent change in the conformation and/or microenviron-ment of the platelet glycoprotein IIb/IIIa complex. J Clin Invest 1985;76:101-8.
14. Konstantopoulos K, Kamat SG, Schafer AI, Banez EI, Jordon R, Kleiman NS, et al. Shear-induced platelet aggregation is inhibited by in vivo infusion of an anti-glycoprotein IIb/IIIa antibody frag-ment, abciximab, in patients undergoing coronary angioplasty. Cir-culation 1995;91:1427-31.
15. Turner NA, Moake JL, Kamat SG, Schafer AI, Kleiman NS, Jordan R, et al. Comparative real-time effects on platelet adhesion and aggregation under flowing conditions of in vivo aspirin, heparin, and monoclonal antibody fragment against glycoprotein IIb/IIIa. Circulation 1995;91:1354-62.
16. Reverter JC, Beguin S, Kessels H, Kumar R, Coller BS. Inhibition of platelet-mediated, tissue factor-induced thrombin generation by the mouse/human chimeric 7E3 antibody. Potential implications for the effects of abciximab treatment on acute thrombosis and “clinical restenosis.” J Clin Invest 1996;98:863-74.
17. Dangas G, Badimon JJ, Coller BS, Fallon JT, Sharma SK, Hayes RM, et al. Administration of abciximab during percutaneous coro-nary intervention reduces both ex vivo platelet thrombus
forma-tion and fibrin deposiforma-tion: implicaforma-tions for a potential anticoagu-lant effect of abciximab. Arterioscl Thromb Vasc Biol 1998; 18:1342-9.
18. Teitel JM, Bauer KA, Lau HK, Rosenberg RD. Studies of the prothrombin activation pathway using radio-immunoassays for the F2/F1+2 frag-ment and thrombin-anitithrombin complex. Blood 1982;59:1086-97. 19. Nossel HL, Ti M, Kaplan KL, Spanondis K, Soland T, Butler VP Jr. The
generation of fibrinopeptide A in clinical blood samples. Evidence for thrombin activity. J Clin Invest 1976;58:1136-44.
20. Braunwald E. Unstable angina: a classification. Circulation 1989; 80:410-4.
21. Dangas G, Mehran R, Wallenstein S, Courcoutsakis NA, Kakarala V, Hollywood J, et al. Correlation between angiographic morphol-ogy and clinical presentation in unstable angina. J Am Coll Cardiol 1997;29:519-25.
22. Ryan TJ, Faxon DP, Gunnar RM. Guidelines for percutaneous trans-luminal coronary angioplasty: A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcom-mittee on Percutaneous Transluminal Coronary Angioplasty). J Am Coll Cardiol 1988;12:529-45.
23. Cadroy Y, Hanson SR, Andrew BK, Marzec UM, Evatt BL, Kunicki TJ, et al. Relative antithrombotic effects of monoclonal antibodies treating different platelet glycoprotein-adhesive molecule interac-tions in nonhuman primates. Blood 1994;83:3218-25. 24. Weiss HJ, Turitto VT, Baumgartner HR. Role of shear rate and
platelets in promoting fibrin formation on rabbit subendothelium. Studies utilizing patients with quantitative and qualitative platelet defects. J Clin Invest 1986;78:1072-82.
25. Marmur JD, Merlini PA, Sharma SK, Khaghan N, Torre SR, Israel DH, et al. Thrombin generation in human coronary arteries after percutaneous transluminal balloon angioplasty. J Am Coll Cardiol 1994;24:1484-91.
26. Marmur JD, Sharma SK, Weinrauch M, Kantrowitz N, Dangas G, Kokkinakis S, et al. Thrombin generation and activity during coro-nary angioplasty: influence of angiographic lesion morphology. J Invas Cardiol 1997;9:410-6.
27. Moliterno DJ, Califf RM, Aguirre FV, Anderson K, Sigmon KN, Weis-man HF, et al for the EPIC study investigators. Effect of platelet gly-coprotein IIb/IIIa integrin blockade on activated clotting time dur-ing percutaneous transluminal coronary angioplasty or directional atherectomy. Am J Cardiol 1995;75:559-62.
28. Ammar T, Scudder LE, Coller BS. In vitro effects of the platelet glyco-protein IIb/IIIa receptor antagonist abciximab on the activated clot-ting time. Circulation 1997;95:614-7.