Not Crying After Birth as a Predictor of
Not Breathing
Ashish KC, PhD,a,b,* Joy E. Lawn, PhD,c,* Hong Zhou, PhD,dUwe Ewald, PhD,aRejina Gurung, MSc,eAbhishek Gurung, MPH,e Avinash K. Sunny, MD,eLouise Tina Day, MRCPCH,cNalini Singhal, MDf
abstract
BACKGROUND:Worldwide, every year, 6 to 10 million infants require resuscitation at birth
according to estimates based on limited data regarding“nonbreathing”infants. In this article, we aim to describe the incidence of“noncrying”and nonbreathing infants after birth, the need for basic resuscitation with bag-and-mask ventilation, and death before discharge.
METHODS:We conducted an observational study of 19 977 infants in 4 hospitals in Nepal. We
analyzed the incidence of noncrying or nonbreathing infants after birth. The sensitivity of noncrying infants with nonbreathing after birth was analyzed, and the risk of predischarge mortality between the 2 groups was calculated.
RESULTS:The incidence of noncrying infants immediately after birth was 11.1%, and the incidence of noncrying and nonbreathing infants was 5.2%. Noncrying after birth had 100% sensitivity for nonbreathing infants after birth. Among the“noncrying but breathing”infants, 9.5% of infants did not breathe at 1 minute and 2% did not to breathe at 5 minutes. Noncrying but breathing infants after birth had almost 12-fold odds of predischarge mortality (adjusted odds ratio 12.3; 95% confidence interval, 5.8–26.1).
CONCLUSIONS:All nonbreathing infants after birth do not cry at birth. A proportion of noncrying but breathing infants at birth are not breathing by 1 and 5 minutes and have a risk for predischarge mortality. With this study, we provide evidence of an association between noncrying and nonbreathing. This study revealed that noncrying but breathing infants require additional care. We suggest noncrying as a clinical sign for initiating resuscitation and a possible denominator for measuring coverage of resuscitation.
WHAT’S KNOWN ON THIS SUBJECT:Global protocols for neonatal resuscitation are based on“noncrying” being a marker of“nonbreathing,”but the relationship between noncrying and nonbreathing, or the predictive risk for each of these for mortality, has not been examined in a large study.
WHAT THIS STUDY ADDS:In this study, we analyzed the incidence of noncrying and nonbreathing infants after birth. All nonbreathing infants were noncrying. Half of noncrying infants were nonbreathing, and 9.3% of noncrying but breathing infants received bag-and-mask ventilation. Noncrying but breathing infants after birth had 12-fold odds of predischarge mortality.
To cite:KC A, Lawn JE, Zhou H, et al. Not Crying After Birth as a Predictor of Not Breathing.Pediatrics. 2020;145(6): e20192719
a
Uppsala University, Uppsala, Sweden;bSociety of Public Health Physicians Nepal, Kathmandu, Nepal;cLondon School of Hygiene and Tropical Medicine, London, United Kingdom;dPeking University Health Science Center, Peking University, Beijing, China;eGolden Community, Lalitpur, Nepal; andfUniversity of Calgary, Calgary, Canada
*Contributed equally as co-first authors
Drs KC, Singhal, and Lawn conceptualized and designed the analyses, drafted the initial manuscript, and reviewed and revised the manuscript; Ms Gurung, Mr Gurung, and Dr Sunny designed the data collection instruments, collected data, conducted the initial analyses, and reviewed and revised the manuscript; Dr Ewald conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content; Drs Zhou and Day supported the analyses and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. This trial has been registered with the ISRCTN Register (http://isrctn.org) (identifier ISRCTN30829654).
An infant’s smooth transition from an intra- to extrauterine life depends on healthy cardiorespiratory function,1 with onset of spontaneous breathing with effective cardiac output.2 Prematurity or acute intrapartum events may disrupt this transition, leading to death or survival with impairment and disability.3According to the 2016 global burden of disease estimates, 2.1 million deaths are attributable to intrapartum-related events, of which 1.2 million deaths are intrapartum stillbirths.4Most of these deaths take place in low- and middle-income countries, where access to and quality of care is poor.5,6 Because the pathway to survival is unpredictable during the high-risk period of birth in these settings, providing optimal quality of
intrapartum and immediate postnatal care is critical.7,8
Through periodic systematic reviews, neonatal survival interventions have been updated to provide guidance to reduce mortality and morbidity.9 High-quality emergency obstetric and
neonatal care reduces the risks for mothers and infants. Basic neonatal resuscitation has been shown to reduce intrapartum-related stillbirth and first-day neonatal death by 26% and 42%, respectively.10,11
Globally, every year, an estimated 10 million infants need some degree of resuscitation.12Between 6 and 10 million infants have been estimated to require stimulation and/or suctioning, 2 to 4 million infants will require bag-and-mask ventilation (BMV), and 1 million infants will require advanced resuscitation.12 This estimate, based on 3 studies, revealed that the quality of evidence for infants requiring resuscitation was low.13–15Of these 3 studies, 2 were hospital based, and Apgar scores at 1 and 5 minutes were used as a measure to guide
resuscitation.13,14However, Apgar scoring is a subjective clinical assessment and is known to have high interobserver variability and a low predictive value to determine need for neonatal resuscitation.16,17
In the community-based study, lay workers were trained to recognize
“nonbreathing”or gasping infants at birth to require resuscitation.15
In 2015, International Liaison Committee on Resuscitation (ILCOR) guidance estimated that 15% of infants require some assistance at birth, 10% respond to stimulation and/or suctioning, 3% require BMV, and 0.1% will requiring advanced resuscitation support.18This estimation is based on Grading of Recommendations Assessment, Development, and Evaluation criteria (level of evidence: 4, low) from 3 observational studies.19–21
ILCOR 2015 guidance for neonatal resuscitation is based on 4 factors: gestation (term or preterm), breathing, crying, and tone.22The guidance stipulates that infants who are“noncrying”or nonbreathing require additional stimulation and that those who still do not initiate spontaneous breathing and have heart rate,100 beats per minute will require BMV.22In 2010, the Helping Babies Breathe (HBB) program, a pictorialflowchart neonatal resuscitation algorithm for low- and
FIGURE 1
Strengthening the Reporting of Observational Studies in Epidemiologyflow diagram from the Nepal Perinatal Quality Improvement Project study for inclusion in this analysis.
FIGURE 2
middle-income countries, was adapted from ILCOR guidance to better equipfirst responders to manage high-risk newborns at the time of birth.18The entry point for the HBB algorithm is noncrying infants at birth to initiate neonatal resuscitation steps. The HBB 1.0 and 2.0 versions have been rolled out in $80 countries with 500 000 health workers trained on the neonatal resuscitation protocol.23Evaluations have revealed that the effect of the HBB algorithm can reduce
intrapartum-related mortality by 50% as well as improve health workers’performance by more than twofold.24–26
Both the neonatal resuscitation program and the HBB advisory group have identified the need for better quality data to inform guidance on provision of resuscitation care at the time of birth. Our aim for this article
is to describe the incidence of infants who did not cry (noncrying) and/or did not breathe (nonbreathing) at 3 time points: immediately after birth and at 1 and 5 minutes after birth. In this article, we will also provide a description of the outcome at discharge on the basis of a large-scale multicenter observational study in Nepal.
METHODS
Study Design
This was an observational nested study to evaluate the scale up of the HBB quality improvement (QI) package in hospitals of Nepal (Nepal Perinatal Quality Improvement Project).27,28
Study Sites
This study was conducted in 4 publicly funded hospitals providing comprehensive emergency obstetric
and neonatal care and sick neonatal and pediatric referral services. These hospitals were Koshi Zonal Hospital, Bharatpur Hospital, Western Regional Hospital, and Lumbini Zonal Hospital.
Births in these hospitals occurred in 2 units: the labor and delivery unit for vaginal deliveries performed by nurse-midwives and obstetricians and the operation theater for cesarean deliveries performed by the obstetricians and anesthetists. As per the standard protocol, fetal heart rate isfirst assessed at the time of admission. Fetal heart rate monitoring is done by using the intermittent auscultation method during thefirst and second stages of labor. Women who had obstetric and/or neonatal complications were considered for cesarean delivery.
In both the units, nurse-midwives were the primary responders for neonatal resuscitation. The annual number of hospital births ranges from 9007 to 11 318 a year, with an intrapartum-related mortality (intrapartum stillbirth andfirst-day mortality) rate of 8.6 to 14.2 per 1000 total births.
After the introduction of the HBB QI package in the hospitals, health workers were trained to provide stimulation to“noncrying but breathing”infants.
Study Dates
The study was conducted between July 2017 and September 2018.
Participants
Eligible participants were consenting women in labor at$22 weeks’ gestation in admission to the labor and delivery room.
We excluded women whose fetus had died before admission to labor and delivery (no fetal heart sound), those referred to the operation theater for cesarean delivery, and women who were referred to other facilities before delivery.
FIGURE 3
Sample Size
This was a secondary data analysis of an estimated sample of 20 000 birth observations as part of the HBB scale-up evaluation to detect any change in the health workers’practice after QI interventions.27
Variables
We included the following variables: •noncrying infants after birth:
infants who did not cry immediately after birth; •noncrying but breathing infants
after birth: infants who did not cry but spontaneously breathed immediately after birth; •noncrying and nonbreathing
infants after birth: infants who did not cry and did not breathe spontaneously immediately after birth;
• nonbreathing at 1 minute: infants who were not breathing 1 minute after birth;
• nonbreathing at 5 minutes: infants who were not breathing at 5 minutes after birth; • extremely preterm: infants
between 22 and 28 weeks’ gestational age;
• very preterm: infants between 29 and 32 weeks’gestational age; • late preterm infants between- 33 to
36 weeks’gestational age;
• term: infants$37 weeks’gestation; • mode of delivery: infants who were delivered either by spontaneous or assisted vaginal delivery (the assisted vaginal delivery included vacuum and forceps deliveries); • induction of labor: labor that was
started by artificial rupture of
membranes, prostaglandins, and/or oxytocin;
•appropriate for gestational age: birth weight in the $10th
percentile for gestational age based on the INTERGROWTH-21st study reference point for South Asia29; •small for gestational age (SGA):
birth weight in the ,10th
percentile for gestational age based on the INTERGROWTH-21st study reference point for South Asia29; •predischarge neonatal death:
infants who died before discharge from the hospital; and
•intrapartum stillbirth: infants born at or after 22 weeks’gestation who had a fetal heart sound during the antepartum period and no fetal heart sound during labor, with no signs of life (breathing or heart rate) after neonatal resuscitation at birth.
Data Collection
The data collection team consisted of clinical nurse-midwives who have at least one year of experience in midwifery and research. The data collection team received a week of rigorous training before the start of training on the HBB program as well as the labor and delivery clinical observation tool. The data collection team was placed in admission, labor and delivery, postnatal, and sick newborn care units in each hospital. The team had 8 data collectors with a data coordinator to ensure data collection and management quality. Periodic data quality assessments were done by an independent team of clinicians. On a quarterly basis, an independent clinical team assessed the accuracy of the clinical
observation recorded by the data collectors. Discrepancies on the accuracy of the clinical observation made by data collectors were reviewed, and feedback was provided by the independent clinical team.
Data collectors observed clinical events and clinical service provided FIGURE 4
to the women and infants in the labor and delivery room but not in the operation theater . Observers recorded the induction of labor, time and mode of delivery, and the status of infant crying and infant breathing after birth at 3 distinct times: immediately after birth and at 1 and 5 minutes. Immediate newborn care practices, including any additional stimulation, suctioning or clearing of airways, BMV, additional resuscitation care, and mortality outcomes of the infant, were assessed via observation. Recording of the observation was done in real time on paper-based data collection proforma. The pretesting of the observation checklist was done in another tertiary hospital of Nepal.
Data Management
The collected information on the observed data were reviewed by the data coordinator to check for completeness. The completed data collection tools were transferred by data coordinators to the central research office in Kathmandu, where they were indexed and entered into the Census and Survey Processing
System database. Data were backed up on an external hard drive every month.
To ensure data entry accuracy, 10% of the data were reentered by the data coordinator each month, with feedback provided to the data entry officers.
Data Analysis
We categorized infants into 2 overlapping groups by their status at birth: (1) crying or noncrying and (2) breathing or nonbreathing were categorized into noncrying but breathing and noncrying and
nonbreathing after birth. We analyzed the incidence of noncrying after birth and nonbreathing after birth and at 1 and 5 minutes. We analyzed the incidence of noncrying, noncrying and nonbreathing, and noncrying but breathing after birth by different determinants: gestational age, birth weight as per gestational age, induction of labor, and mode of delivery. The sensitivity, specificity, positive predictive value, and negative predictive value of
noncrying infants after birth with nonbreathing infants were calculated.
A bivariate analysis was conducted to assess the level of association of noncrying but breathing and noncrying and nonbreathing infants after birth with predischarge neonatal mortality. A multiple regression analysis of noncrying but breathing and noncrying and nonbreathing after birth with predischarge neonatal mortality, after adjusting for gestational age, birth weight, induction of labor, mode of delivery, and sex of the infant, was performed. Missing variables and loss to follow-up were excluded during the data analysis.
Ethics Approval
Written consent from each
participant included in the study was taken during admission to the hospital. Ethical approval was received from the Ethical Review Board of Nepal Health Research Council (17/2017). Registration in the ISRCTN registry was done for the large-scale evaluation of the scale up of the HBB QI package.
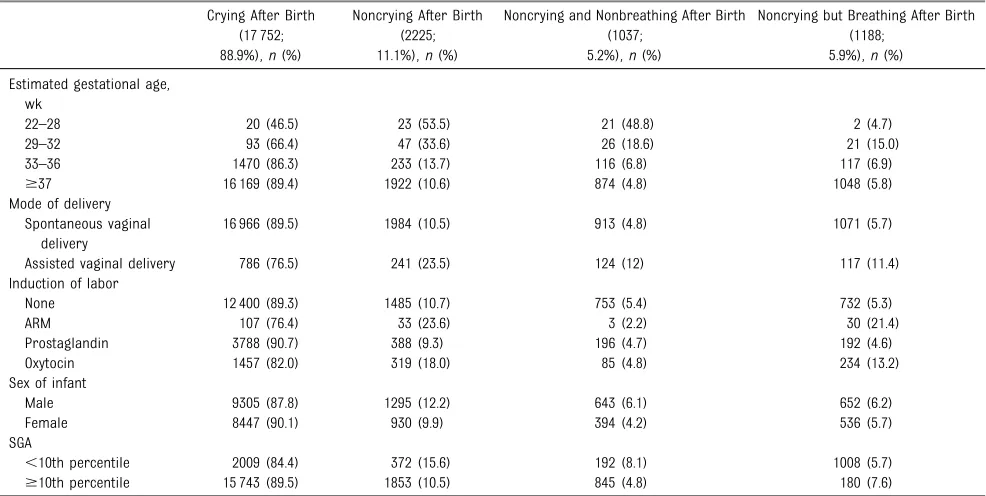
TABLE 1Incidence of Noncrying and Nonbreathing After Birth by Different Obstetric Conditions Crying After Birth
(17 752; 88.9%),n(%)
Noncrying After Birth (2225; 11.1%),n(%)
Noncrying and Nonbreathing After Birth (1037;
5.2%),n(%)
Noncrying but Breathing After Birth (1188;
5.9%),n(%) Estimated gestational age,
wk
22–28 20 (46.5) 23 (53.5) 21 (48.8) 2 (4.7)
29–32 93 (66.4) 47 (33.6) 26 (18.6) 21 (15.0)
33–36 1470 (86.3) 233 (13.7) 116 (6.8) 117 (6.9)
$37 16 169 (89.4) 1922 (10.6) 874 (4.8) 1048 (5.8)
Mode of delivery Spontaneous vaginal
delivery
16 966 (89.5) 1984 (10.5) 913 (4.8) 1071 (5.7)
Assisted vaginal delivery 786 (76.5) 241 (23.5) 124 (12) 117 (11.4) Induction of labor
None 12 400 (89.3) 1485 (10.7) 753 (5.4) 732 (5.3)
ARM 107 (76.4) 33 (23.6) 3 (2.2) 30 (21.4)
Prostaglandin 3788 (90.7) 388 (9.3) 196 (4.7) 192 (4.6)
Oxytocin 1457 (82.0) 319 (18.0) 85 (4.8) 234 (13.2)
Sex of infant
Male 9305 (87.8) 1295 (12.2) 643 (6.1) 652 (6.2)
Female 8447 (90.1) 930 (9.9) 394 (4.2) 536 (5.7)
SGA
,10th percentile 2009 (84.4) 372 (15.6) 192 (8.1) 1008 (5.7)
$10th percentile 15 743 (89.5) 1853 (10.5) 845 (4.8) 180 (7.6)
RESULTS
Of the total 33 430 pregnant women admitted into the hospitals during the 15-month study period, 26 345 were assessed for eligibility, of whom 22 340 (84.8%) women were recruited. Among the total women recruited, 183 (0.8%) had stillbirths, 169 (0.8%) had neonatal deaths, and 8% were lost to follow-up (Fig 1).
Of the 19 977 infants observed, 11.1% did not cry after birth. Of the infants observed, 5.2% were noncrying and nonbreathing and 5.9% were noncrying but breathing after birth. Of the infants observed, 1.9% (373) did not breathe
spontaneously until 1 minute, and 0.8% (168) did not breathe
spontaneously until 5 minutes (Fig 2).
Among noncrying and nonbreathing infants after birth, 71.0% received stimulation, 25.1% were
nonbreathing at 1 minute, 23.8% received BMV, and 13.9% were nonbreathing at 5 minutes. Among noncrying but breathing infants after birth, 96.3% received stimulation, 9.5% were nonbreathing at 1 minute, 9.3% received BMV, and 2.0% were nonbreathing at 5 minutes (Fig 3).
Among the term noncrying and nonbreathing infants after birth, 73.1% received stimulation, 22.3%
were nonbreathing at 1 minute, 22.9% received BMV, and 10.8% were nonbreathing at 5 minutes. Among the term noncrying but breathing infants after birth, 96.4% received stimulation, 9.2% were nonbreathing at 1 minute, 8.9% received BMV, and 1.8% were nonbreathing at 5 minutes (Fig 4). Among the term noncrying but breathing infants after birth, 9 of them died before discharge.
Among the extremely preterm infants (22–28 weeks), 53.5% were
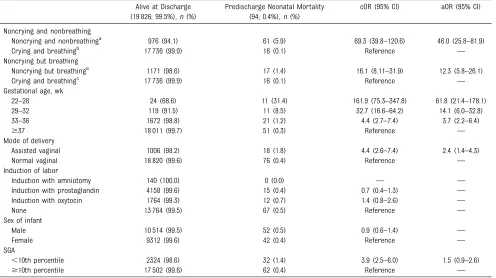
noncrying after birth, with 48.8% noncrying and nonbreathing after birth and 4.7% noncrying but breathing after birth. Among the infants born with assisted vaginal delivery, a higher proportion (23.5%) were noncrying after birth, with 11.4% noncrying but breathing and 12.0% noncrying and nonbreathing after birth. Among women with induced labor by using artificial TABLE 2Risk of Predischarge Neonatal Mortality With Noncrying and Nonbreathing Infants After Birth
Alive at Discharge (19 826; 99.5%),n(%)
Predischarge Neonatal Mortality (94; 0.4%),n(%)
cOR (95% CI) aOR (95% CI)
Noncrying and nonbreathing
Noncrying and nonbreathinga 976 (94.1) 61 (5.9) 69.3 (39.8–120.6) 46.0 (25.8–81.9)
Crying and breathingb 17 736 (99.9) 16 (0.1) Reference —
Noncrying but breathing
Noncrying but breathinga 1171 (98.6) 17 (1.4) 16.1 (8.11–31.9) 12.3 (5.8–26.1)
Crying and breathingc 17 736 (99.9) 16 (0.1) Reference —
Gestational age, wk
22–28 24 (68.6) 11 (31.4) 161.9 (75.3–347.8) 61.8 (21.4–178.1)
29–32 119 (91.5) 11 (8.5) 32.7 (16.6–64.2) 14.1 (6.0–32.8)
33–36 1672 (98.8) 21 (1.2) 4.4 (2.7–7.4) 3.7 (2.2–6.4)
$37 18 011 (99.7) 51 (0.3) Reference —
Mode of delivery
Assisted vaginal 1006 (98.2) 18 (1.8) 4.4 (2.6–7.4) 2.4 (1.4–4.3)
Normal vaginal 18 820 (99.6) 76 (0.4) Reference —
Induction of labor
Induction with amniotomy 140 (100.0) 0 (0.0) — —
Induction with prostaglandin 4158 (99.6) 15 (0.4) 0.7 (0.4–1.3) —
Induction with oxytocin 1764 (99.3) 12 (0.7) 1.4 (0.8–2.6) —
None 13 764 (99.5) 67 (0.5) Reference —
Sex of infant
Male 10 514 (99.5) 52 (0.5) 0.9 (0.6–1.4) —
Female 9312 (99.6) 42 (0.4) Reference —
SGA
,10th percentile 2324 (98.6) 32 (1.4) 3.9 (2.5–6.0) 1.5 (0.9–2.6)
$10th percentile 17 502 (99.6) 62 (0.4) Reference —
cOR, crude odds ratio;—, not applicable.
aSample size = 1037. bSample size = 17 752. cSample size = 1188.
TABLE 3Noncrying Infants After Birth and Nonbreathing Infants After Birth Nonbreathing
After Birth
Breathing After Birth Total
Noncrying after birth 1037 1188 2225
Crying after birth 0 17 752 17 752
rupture of membranes, 23.6% of infants were noncrying after birth, with 21.4% noncrying but breathing and 2.2% noncrying and nonbreathing after birth. Among SGA infants, 15.6% were noncrying after birth, with 5.7% noncrying but breathing and 8.1% noncrying and nonbreathing after birth (Table 1).
Compared with infants crying and breathing after birth, noncrying and nonbreathing infants had 46 times higher odds of predischarge neonatal
mortality (adjusted odds ratio [aOR] 46.0; 95% confidence interval [CI], 25.8–81.9) after adjustment for preterm birth, assisted vaginal delivery, and SGA. Preterm birth, assisted vaginal delivery, and SGA revealed an association with predischarge neonatal mortality. Compared with infants crying and breathing after birth, noncrying but breathing infants had 12 times higher odds (aOR 12.3; 95% CI, 5.8–26.1) of predischarge mortality after adjustment for risk of preterm birth, assisted vaginal delivery, and SGA (Table 2).
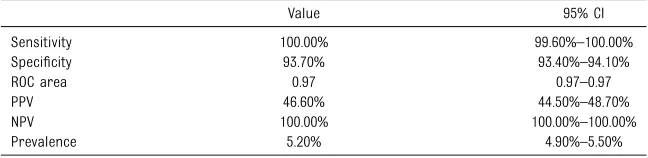
This study revealed that all nonbreathing infants after birth were noncrying (sensitivity = 100%). The positive predictive value after birth of noncrying infants with nonbreathing was 46.0% (95% CI, 44.5%–48.7%). The negative predictive value after birth of noncrying infants with nonbreathing was 100% (95% CI, 100%–100%) (Tables 3 and 4).
DISCUSSION
This is the largest study to date in which we report on observation at birth of noncrying and nonbreathing infants. Among the total 19 977 observed births, approximately one-tenth of infants did not cry after birth. Almost half of the noncrying infants after birth were breathing. The proportion of noncrying infants increases with lower gestational age, with.50% of infants at 22 to 28 weeks’gestation not crying at birth.
In the ILCOR guideline for neonatal resuscitation, the clinical algorithms use noncrying as decision points for resuscitation steps. In this cohort, all nonbreathing infants were noncrying after birth (100%). The positive predictive value of noncrying infants was 50% for nonbreathing infants.
In the cohort of noncrying and nonbreathing infants at birth, more than two-thirds received simple measures of stimulation, and almost one-fourth of them received BMV. In the cohort of noncrying but breathing infants at birth, almost all of them received simple measures of stimulation, and 1 in 10 infants received BMV. Infants who are noncrying but breathing may have primary or secondary apnea. These infants would require additional stimulation to assist in transition to spontaneous breathing, whereas some would require BMV.
Among the noncrying but breathing infants after birth, 9.5% were nonbreathing at 1 minute and 2.0% did not breathe at 5 minutes and had
12-fold odds for predischarge mortality. Crying assists in clearing lungfluid, and it may assist in establishment of functional residual capacity. Noncrying of the infant coupled with perinatal depression might increase the risk of mortality. Further mechanistic studies are required to understand the physiology.
So far, the incidence of infants who received resuscitation at birth is mostly derived from intervention-based studies in which the effects of neonatal resuscitation interventions on clinical performance and mortality are reported.19,20,30 For example, in a study conducted in Tanzania, Ersdal et al19proposed that 16% of the infants who did not breathe spontaneously received basic resuscitation. From our study, of the noncrying infants after birth, 16.8% did not breathe at 1 minute and required BMV.
Defining the population of infants who require resuscitation is crucial for measuring the coverage of neonatal resuscitation interventions. The Every Newborn Action Plan Measurement Improvement Roadmap (2016–2020) prioritized research to validate the coverage indicators for neonatal interventions (including neonatal resuscitation) to improve tracking of national and global progress to the Sustainable Development Goals for newborn survival.31,32The Every
Newborn–Birth Indicators Research Tracking in Hospitals study in Nepal, Bangladesh, and Tanzania is designed to validate these indicators for use in maternal-report surveys and in routine facility data.33Because documentation of facility data is often done by the health worker providing the care, ensuring measurement (both numerator and denominator) that is meaningful to reinforce clinical practice is crucial.33
This study has several strengths, including that observation was done TABLE 4Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value, Area Under the
Curve, and Inflation Factor of Noncrying Infants After Birth on Nonbreathing Infants After Birth
Value 95% CI
Sensitivity 100.00% 99.60%–100.00%
Specificity 93.70% 93.40%–94.10%
ROC area 0.97 0.97–0.97
PPV 46.60% 44.50%–48.70%
NPV 100.00% 100.00%–100.00%
Prevalence 5.20% 4.90%–5.50%
by trained researchers in multiple hospitals in Nepal in a consistent way and with a large sample size. Using observational methods limited recall bias.
However, there are several limitations. First, this observation was only done for vaginal deliveries and not for cesarean deliveries. Second, there might have been observer reporting bias, especially when the case load for deliveries was high; however, periodic quality assessment was done to reduce the bias. Third, we did not assess whether the infant cried or breathed after stimulation. Fourth, the physiologic response to hypoxia is gasping (deep and irregular breathing), which might have been captured by the clinical observers as breathing; however, these infants who were gasping would have required BMV. Finally, we did not have cord base values to determine if infants who did not cry had perinatal depression.
CONCLUSIONS
With this study, we provide incidence of noncrying and nonbreathing infants after birth, prediction of infants receiving resuscitation, and risk of neonatal mortality in Nepal. Eleven percent of the infants did not cry after birth. One-fifth of infants born by assisted vaginal delivery and/or with induction of labor (artificial rupture of membranes) were noncrying at birth. Almost half of these infants were nonbreathing after birth. Noncrying but breathing infants after birth had 12-fold odds of predischarge mortality compared with crying infants. All noncrying infants require further assessment and initial steps of resuscitation. With this study, we provide evidence of the association
between noncrying and nonbreathing. Ourfindings support noncrying as an indicator for initiating
resuscitation and closer monitoring and potentially as a denominator for coverage measurement to maintain integrity between clinical and measurement practice.
ACKNOWLEDGMENTS
We thank Omkar Basnet and data collectors for the contribution to the study. Most of all, we thank the women, their newborns, and their families.
ABBREVIATIONS
aOR: adjusted odds ratio BMV: bag-and-mask ventilation CI: confidence interval
HBB: Helping Babies Breathe ILCOR: International Liaison
Committee on Resuscitation QI: quality improvement
SGA: small for gestational age
Address correspondence to Ashish KC, PhD, International Maternal and Child Health, Department of Women’s and Children’s Health, Uppsala University, Dag Hammarskjölds väg 14B, Floor 1, Akademiska sjukhuset SE-751 85, Uppsala, Sweden. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:Funded by the Swedish Research Council and Laerdal Foundation for Acute Medicine as part of the evaluation of neonatal resuscitation protocols in hospitals of Nepal.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Hooper SB, Polglase GR, te Pas AB. A physiological approach to the timing of umbilical cord clamping at birth.Arch Dis Child Fetal Neonatal Ed. 2015;100(4): F355–F360
2. Gao Y, Raj JU. Regulation of the pulmonary circulation in the fetus and newborn. Physiol Rev. 2010;90(4):1291–1335
3. Crossley KJ, Allison BJ, Polglase GR, Morley CJ, Davis PG, Hooper SB. Dynamic changes in the direction of bloodflow through the ductus arteriosus at birth. J Physiol. 2009;587(pt 19):4695–4704
4. GBD 2015 Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015 [published correction appears in Lancet. 2017;389(10064):e1].Lancet. 2016;388(10053):1725–1774
5. Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution [published correction appears inLancet Glob Health. 2018;
6(11):e1162].Lancet Glob Health. 2018; 6(11):e1196–e1252
6. Kruk ME, Gage AD, Joseph NT, Danaei G, García-Saisó S, Salomon JA. Mortality due to low-quality health systems in the universal health coverage era: a systematic analysis of amenable deaths in 137 countries. Lancet. 2018;392(10160):2203–2212
accelerate scale-up in countries. Lancet. 2014;384(9941):438–454
8. Oza S, Cousens SN, Lawn JE. Estimation of daily risk of neonatal death, including the day of birth, in 186 countries in 2013: a vital-registration and modelling-based study.Lancet Glob Health. 2014;2(11):e635–e644
9. Bhutta ZA, Das JK, Bahl R, et al; Lancet Newborn Interventions Review Group; Lancet Every Newborn Study Group. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? [published correction appears in Lancet. 2014;384(9940):308].Lancet. 2014;384(9940):347–370
10. Patel A, Khatib MN, Kurhe K, Bhargava S, Bang A. Impact of neonatal
resuscitation trainings on neonatal and perinatal mortality: a systematic review and meta-analysis.BMJ Paediatr Open. 2017;1(1):e000183
11. Dol J, Campbell-Yeo M, Murphy GT, Aston M, McMillan D, Richardson B. The impact of the Helping Babies Survive program on neonatal outcomes and health provider skills: a systematic review.JBI Database System Rev Implement Rep. 2018;16(3):701–737
12. Lee AC, Cousens S, Wall SN, et al. Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect. BMC Public Health. 2011;11(suppl 3):S12
13. Zhu XY, Fang HQ, Zeng SP, Li YM, Lin HL, Shi SZ. The impact of the neonatal resuscitation program guidelines (NRPG) on the neonatal mortality in a hospital in Zhuhai, China.Singapore Med J. 1997;38(11):485–487
14. Deorari AK, Paul VK, Singh M, Vidyasagar D; Medical Colleges Network. Impact of education and training on neonatal resuscitation practices in 14 teaching hospitals in India.Ann Trop Paediatr. 2001;21(1):29–33
15. Bang AT, Bang RA, Baitule SB, Reddy HM, Deshmukh MD. Management of birth asphyxia in home deliveries in rural Gadchiroli: the effect of two types of birth attendants and of resuscitating with mouth-to-mouth, tube-mask or bag-mask. J Perinatol. 2005;25(suppl 1):S82–S91
16. Apgar V. A proposal for a new method of evaluation of the newborn infant.Curr Res Anest Anal. 1953;32(4):260–267
17. O’Donnell CP, Kamlin CO, Davis PG, Carlin JB, Morley CJ. Interobserver variability of the 5-minute Apgar score.J Pediatr. 2006;149(4):486–489
18. Wyllie J, Perlman JM, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 7: neonatal resuscitation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2015;95:e169–e201
19. Ersdal HL, Mduma E, Svensen E, Perlman JM. Early initiation of basic resuscitation interventions including face mask ventilation may reduce birth asphyxia related mortality in low-income countries: a prospective descriptive observational study. Resuscitation. 2012;83(7):869–873
20. Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery room. Associated clinical events.Arch Pediatr Adolesc Med. 1995;149(1):20–25
21. Wyckoff MH, Perlman JM, Laptook AR. Use of volume expansion during delivery room resuscitation in near-term and term infants.Pediatrics. 2005;115(4):950–955
22. Wyllie J, Perlman JM, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 11: neonatal resuscitation: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations.
Resuscitation. 2010;81(suppl 1):e260–e287
23. Kamath-Rayne BD, Berkelhamer SK, Kc A, Ersdal HL, Niermeyer S. Neonatal resuscitation in global health settings: an examination of the past to prepare for the future.Pediatr Res. 2017;82(2):194–200
24. Kc A, Wrammert J, Nelin V, et al. Evaluation of Helping Babies Breathe Quality Improvement Cycle (HBB-QIC) on retention of neonatal resuscitation skills six months after training in Nepal. BMC Pediatr. 2017;17(1):103
25. Kc A, Wrammert J, Clark RB, et al. Reducing perinatal mortality in Nepal
using Helping Babies Breathe. Pediatrics. 2016;137(6):e20150117
26. Budhathoki SS, Gurung R, Ewald U, Thapa J, Kc A. Does the Helping Babies Breathe Programme impact on neonatal resuscitation care practices? Results from systematic review and meta-analysis.Acta Paediatr. 2019;108(5):806–813
27. Kc A, Ewald U, Basnet O, et al. Effect of a scaled-up neonatal resuscitation quality improvement package on intrapartum-related mortality in Nepal: a stepped-wedge cluster randomized controlled trial.PLoS Med. 2019;16(9):e1002900
28. Kc A, Bergström A, Chaulagain D, et al. Scaling up quality improvement intervention for perinatal care in Nepal (NePeriQIP); study protocol of a cluster randomised trial [published correction appears inBMJ Glob Health. 2019;4(6): e000497corr1].BMJ Glob Health. 2017;2(3): e000497
29. Lee AC, Kozuki N, Cousens S, et al; CHERG Small-for-Gestational-Age-Preterm Birth Working Group. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21st standard: analysis of CHERG datasets [published correction appears inBMJ. 2017;358:j4229].BMJ. 2017;358:j3677
30. Wyckoff MH, Perlman JM. Use of high-dose epinephrine and sodium bicarbonate during neonatal resuscitation: is there proven benefit? Clin Perinatol. 2006;33(1):141–151, viii–ix
31. Moxon SG, Ruysen H, Kerber KJ, et al. Count every newborn; a measurement improvement roadmap for coverage data.BMC Pregnancy Childbirth. 2015; 15(suppl 2):S8
32. Lawn JE, Blencowe H, Oza S, et al; Lancet Every Newborn Study Group. Every Newborn: progress, priorities, and potential beyond survival [published correction appears in Lancet. 2014;384(9938):132].Lancet. 2014;384(9938):189–205
DOI: 10.1542/peds.2019-2719 originally published online May 12, 2020;
2020;145;
Pediatrics
Avinash K. Sunny, Louise Tina Day and Nalini Singhal
Ashish KC, Joy E. Lawn, Hong Zhou, Uwe Ewald, Rejina Gurung, Abhishek Gurung,
Not Crying After Birth as a Predictor of Not Breathing
Services
Updated Information &
http://pediatrics.aappublications.org/content/145/6/e20192719
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/145/6/e20192719#BIBL
This article cites 33 articles, 5 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/public_health_sub Public Health
http://www.aappublications.org/cgi/collection/neonatology_sub Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2019-2719 originally published online May 12, 2020;
2020;145;
Pediatrics
Avinash K. Sunny, Louise Tina Day and Nalini Singhal
Ashish KC, Joy E. Lawn, Hong Zhou, Uwe Ewald, Rejina Gurung, Abhishek Gurung,
Not Crying After Birth as a Predictor of Not Breathing
http://pediatrics.aappublications.org/content/145/6/e20192719
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.