ARTICLE
Intermittent Hydronephrosis Secondary to
Ureteropelvic Junction Obstruction: Clinical and
Imaging Features
Jeng-Daw Tsai, MDa,b, Fu-Yuan Huang, MDa,b, Chun-Chen Lin, MDa, Tsuen-Chiuan Tsai, MDa, Hung-Chang Lee, MDa,b, Jin-Cherng Sheu, MDc, Pei-Yeh Chang, MDd
Departments ofaPediatrics andcPediatric Surgery, Mackay Memorial Hospital, Taipei, Taiwan;bDepartment of Pediatrics, Taipei Medical University, Taipei, Taiwan; dDepartment of Pediatric Surgery, Chang Gung Children’s Hospital, Taoyuan, Taiwan
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.We sought to assess the clinical and imaging findings in intermittent
hydronephrosis secondary to ureteropelvic junction obstruction, with particular emphasis on the characteristic ultrasonographic findings.
METHODS.This prospective, longitudinal, observational study included all children who had intermittent ureteropelvic junction obstruction and presented with ab-dominal pain over 6 years. Renal ultrasound was used as an initial screening tool to detect intermittent hydronephrosis. Renal ultrasonography was repeated every 1 to 2 days to record serial changes from the symptomatic to the asymptomatic stage. Their clinical manifestations and imaging findings were studied.
RESULTS.Eighteen patients (14 boys, 4 girls) were studied. Most had sharp pain that
began acutely and typically lasted for⬍2 days. Most of the children (16 of 18) had
nausea and vomiting that accompanied the pain. The acute episode generally resolved spontaneously and was followed by a pain-free interval that ranged from days to months. Factors that predisposed to an attack included increased water intake, vigorous exercise, or bladder distention. All patients had clearly demon-strable obstruction of the renal pelvis during an acute attack, a finding that diminished or resolved during the symptom-free intervals. During convalescence, all patients had renal pelvic wall thickening on ultrasonography. This finding appeared on the second or third day after a painful episode subsided, persisted for 6 to 9 days, and then disappeared in the symptom-free stage. Pyeloplasty was performed in 17 patients, none of whom had recurrent pain on follow-up. Ex-trinsic obstructions were found in 9 patients.
CONCLUSIONS.The keys to diagnosis are awareness of the syndrome, a detailed
history, and immediate and serial imaging studies during painful crises. A thick-ened renal pelvic wall during convalescence is an important ultrasonic sign of intermittent hydronephrosis.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-0583
doi:10.1542/peds.2005-0583
Key Words
intermittent hydronephrosis, ureteropelvic junction obstruction, prospective studies, renal ultrasonography, renal pelvic wall thickening, convalescence, intravenous pyelogram, diuretic renal scan, computed tomography, dismembered pyeloplasty, follow-up
Abbreviations
UPJO— ureteropelvic junction obstruction
IVP—intravenous pyelogram VCUG—voiding cystourethrography, CT— computed tomography DTPA— diethylene triamine pentaacetic acid
Accepted for publication Jun 20, 2005 Address correspondence to Pei-Yeh Chang, MD, Department of Pediatric Surgery, Chang Gung Children’s Hospital, 5-7, Fu-Hsin St, Kwei-Shan, Taoyuan, Taiwan. E-mail: pyjchang@cgmh.org.tw
U
RETEROPELVIC JUNCTION OBSTRUCTION(UPJO) is at-tributed to a functional or anatomic narrowing of the junction between the renal pelvis and the ureter. It is 1 of the most enigmatic clinical problems today. The obstruction may remain stable, diminish over time, progress, or occur intermittently. Intermittent UPJO is usually acute but self-limited. It causes a distinct clinical syndrome of severe episodic abdominal pain, nausea, and vomiting associated with intermittenthydronephro-sis known as Dietl’s crihydronephro-sis.1It was first described by Dietl
in 1864. Rapid distention of the pelvis and stretching of
the renal capsule explain the acute pain.2It is not
un-usual for these patients to have a long-standing history of episodic abdominal pain that is not diagnosed correct-ly.2–5
In 1956, Nesbit6 was the first to point out that the
intravenous pyelogram (IVP) in patients with intermit-tent hydronephrosis may be normal between acute ep-isodes. Unless patients are investigated during the brief episode of pain, the obstruction is easily missed, and the pelvicaliceal system may appear normal or only mini-mally dilated during pain-free intervals. Imaging during an attack or on provocative testing, eg, diuretic IVP, diuretic ultrasonography, or diuretic renal scan, is
needed for correct diagnosis.7The purpose of this study
is to present our experience in the diagnosis of intermit-tent hydronephrosis, with particular emphasis on the characteristic clinical and imaging findings in intermit-tent UPJO. We present serial ultrasound findings from the acute episode through to recovery.
METHODS
From July 1998 to May 2004, all children who had intermittent hydronephrosis and presented with abdom-inal pain were studied prospectively. Informed consent was obtained from the parents of the children. The di-agnosis of intermittent hydronephrosis required all of the following criteria: (1) episodes of intermittent ab-dominal pain were associated with demonstrable UPJO
only during an attack or on provocative testing8; (2)
urinary tract infection was ruled out by finding a nega-tive urine culture and no evidence of pyonephrosis on ultrasonography; (3) vesicoureteral reflux was ruled out by voiding cystourethrography (VCUG); (4) a renal stone in the ureteropelvic junction was excluded by plain abdominal film, ultrasonography, or computed to-mography (CT) when necessary; and (5) the imaging studies demonstrated obstructive hydronephrosis during an acute attack but no obstruction during symptom-free intervals.
Renal ultrasound was used as an initial screening tool to detect intermittent hydronephrosis. All ultrasound examinations were performed by 1 pediatric nephrolo-gist using a Toshiba (Tokyo, Japan) SSA-260A scanner with a 3.5-MHz transducer. The urinary tract was exam-ined in both supine and prone positions. Hydronephrosis
was defined and graded as follows: mild renal pelvic dilatation (grade 1), only a slit of fluid in the renal pelvis; mild hydronephrosis (grade 2), a dilated pelvis extend-ing to the calyces and upper ureter; moderate hydrone-phrosis (grade 3), a dilated pelvis and calyces but normal parenchyma; and severe hydronephrosis (grade 4), a dilated pelvis and calyces associated with a thin or dis-torted parenchyma. Renal pelvic wall thickening was defined as a circumferential hypoechoic rim delineated on each side by thin hyperechoic lines, the rim being
thicker than 0.8 mm.9The thickness of the pelvic wall
was measured with the patient lying prone. When marked hydronephrosis was demonstrated by ultra-sound during the symptomatic stage, an IVP and Tc-99m diethylene triamine pentaacetic acid (DTPA) diuretic re-nal scan were performed as soon as possible. All patients were evaluated preoperatively with a DTPA diuretic re-nal scan to confirm obstruction and assess split rere-nal function. Renal ultrasonography was repeated every 1 or 2 days to record serial changes in the hydronephrosis as the patients progressed from the symptomatic to asymp-tomatic stages. When only mild hydronephrosis or a nondilated pelvis was demonstrated on the initial ultra-sonographic examination during the symptom-free stage, the patient was asked to return during the next attack for assessment. Immediate ultrasonography and other imaging studies were performed at that time to detect hydronephrosis. Once intermittent hydronephro-sis secondary to UPJO was diagnosed and imaging stud-ies were completed, surgery was suggested. Renal ultra-sonography and DTPA diuretic renal scan were used for follow-up. Data collected for the study included symp-toms, physical examination, laboratory data, and imag-ing studies.
RESULTS
From July 1998 to May 2004, 18 patients (14 boys, 4 girls) received a diagnosis of intermittent hydronephro-sis in our hospital. Their ages ranged from 4.1 to 15.2 years (mean: 7.5 years). All had unilateral intermittent hydronephrosis, 16 on the left and 2 on the right. Three had asymptomatic contralateral mild hydronephrosis without progressive pelvic enlargement. All presented with acute abdominal pain, 15 with a history of recur-rences (beginning 2 months to 2 years [mean: 8.1 months] before diagnosis) and 3 during their first attack. Three had a history of mild hydronephrosis noted on prenatal ultrasonography but developed episodes of acute pain only at an older age.
The clinical features and associated symptoms and signs are shown in Tables 1 and 2. In most cases, the pain was acute and sharp, with a sudden onset. It typically
lasted for⬍2 days, during which the children had
initiated or exacerbated by the ingestion of excess fluid in 6 (33%) children and by vigorous physical activity in 3 (17%). Four children had acute attacks that woke them from sleep early in the morning. One of them, intermittent hydronephrosis secondary to UPJO, re-ceived the diagnosis during his previous hospitalization, and he was scheduled for operation. He had intense, intolerable pain in the morning and was subsequently found on ultrasonography and CT to have spontaneous rupture of the kidney with no history of trauma (Fig 1). There were no identifiable precipitating factors in 7 (39%) patients; their pain occurred unpredictably. The pain was predominantly in the left, periumbilical, and epigastric areas. Older children might describe flank or unilateral back pain. Children who were younger than 5 were less likely to describe the sensation accurately and generally pointed to the periumbilical or epigastric re-gion. In addition to abdominal pain, 16 (89%) children
had nausea and vomiting. Bilious vomiting was noted in 4, and 1 had bloody vomitus. Other associated symptoms and signs included hypertension (2 patients), urinary retention (1 patient), urinary frequency (1 patient), and intestinal ileus (1 patient). Ten of the patients initially received a diagnosis of other diseases, including intesti-nal ileus (2 patients), appendicitis (1 patient), abdomiintesti-nal mass (1 patient), renal stone (2 patients), chronic con-stipation (1 patient), gastrointestinal dysfunction (2 pa-tients), and urinary tract infection (1 patient).
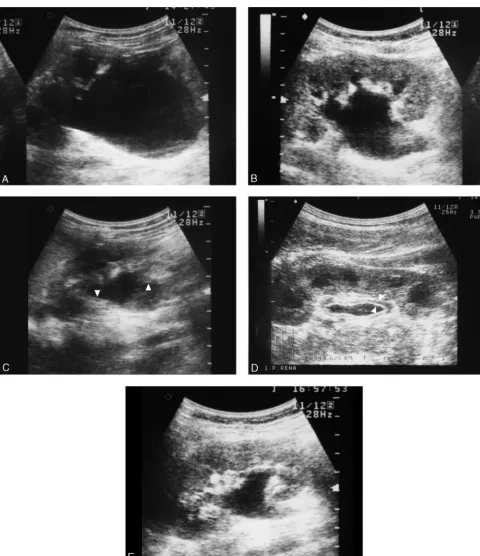
On ultrasonography, all patients had either moderate (8 patients) or severe (10 patients) hydronephrosis in the acute stage. During symptom-free intervals, 7 had only mild pelvic dilatation and 9 had mild hydronephro-sis; 2 patients had moderate hydronephrosis during re-covery from acute hydronephrosis (Table 3). During convalescence, all had renal pelvic wall thickening (Fig 2). This finding appeared on the second or third day after pain had subsided. The hydronephrosis gradually de-creased in degree. A thickened pelvic wall persisted for 6 to 9 days and then disappeared, with only a minimally dilated pelvis present in the symptom-free stage. The maximum measured thickness of the pelvic wall ranged from 2.5 to 5.6 mm (mean: 3.4 mm). A diagnosis of intermittent hydronephrosis was suspected in 8 patients because of the finding of a thickened pelvic wall in the convalescent period, although only mild hydronephrosis was found on initial ultrasound examination. We rec-ommended that they come for immediate ultrasonogra-TABLE 1 Clinical Features in 18 Patients With Intermittent
Hydronephrosis
Clinical Features n(%)
Quality of the pain
Cramping 16 (89)
Dull 2 (11)
Peritoneal signs 1 (6)
Location of pain
Flank/back 14 (78) (Right: 2, left: 12)
Periumbilical 4 (22)
Epigastric 4 (22)
Diffuse abdominal 1 (6)
Duration of acute episode, d
⬍1 6 (33)
1–2 10 (56)
2–3 2 (11)
Frequency of attacks
Once (the first attack) 3 (17)
Every 1 wk 3 (17)
Every 2 wk 6 (33)
Every 4 wk 4 (22)
Every 2–3 mo 2 (11)
Precipitating factors
Increased fluid intake 6 (33)
Vigorous exercise 3 (17)
Bladder filling during sleep 4 (22)
None identified 7 (39)
TABLE 2 Associated Symptoms and Signs During Acute Episodes
Associated Symptoms and Signs n(%)
(N⫽18)
Nausea and vomiting 16 (89)
Palpable abdominal mass 4 (22)
Gross hematuria 2 (11)
Microscopic hematuria 7 (39)
Hypertension 2 (11)
Urinary retention (dysuria) 1 (6)
Urinary frequency 1 (6)
Ileus on plain abdominal film 1 (6)
Spontaneous rupture of kidney 1 (6)
FIGURE 1
CT of ruptured kidney. The patient had intense pain that woke him from sleep in the morning. CT showed rupture of the right kidney with perinephric fluid collection. Bloody urine was drained via a percutaneous nephrostomy.
TABLE 3 Degree of Hydronephrosis on Sonogram During Acute and Symptom-Free Stages
Grade 1 Grade 2 Grade 3 Grade 4
Acute stage,n 8 10
phy during the next attack, and all were demonstrated to have intermittent UPJO. After surgical correction, none had a thickened pelvic wall on follow-up ultrasonogra-phy.
Abdominal CT was performed in 8 patients, 3 in the emergency department for evaluation of an acute abdo-men, 1 to assess a palpable flank mass, 1 who exhibited spontaneous kidney rupture, and 3 to exclude a ureteral
FIGURE 2
stone. All patients were free of vesicoureteral reflux according to VCUG. IVP was performed in 14 patients in the acute period. Ten patients had delayed filling and marked hydronephrosis without enlargement of the ureter, suggestive of UPJO. In 4 patients, the involved kidney appeared enlarged but functioned poorly second-ary to acute obstruction. Only a small amount of contrast medium was excreted into the pelvis, so the detailed anatomy of the UPJ was not demonstrated clearly. An-tegrade pyelography was done via a percutaneous ne-phrostomy in the patient with the ruptured kidney, and UPJO was demonstrated. A DTPA diuretic renal scan was performed in 17 patients within 3 days after the acute attack. The preoperative split renal function ranged from 10% to 55% (mean: 35.5%) in the involved pelvis. Fifteen patients had an obstructive pattern on washout curves with prolonged half times. Two patients had an equivocal pattern of the washout curve after furosemide. Three patients noticed some discomfort on the hydrone-phrotic side during this test.
Open surgery was performed in 17 patients, including a dismembered pyeloplasty in 16 cases and pyeloplasty with ureteropelvic anastomosis in front of the crossing vessel in 1. The other one was lost to follow-up. Intrinsic obstructions, such as ureteral narrowing or an adynamic segment, were noted in 6 (35%) patients. Extrinsic ob-structions were found in 9 (53%) patients, including 6 with a kinked ureter, 2 with a high ureteral insertion, and 1 with an aberrant vessel. Two (12%) patients had a fibroepithelial polyp of the ureter. Only 7 (50%) of 14 cases were diagnosed correctly before operation by IVP, including 3 cases of intrinsic stenosis, 2 of kinking of the ureter, 1 ureteral polyp, and 1 aberrant vessel. Fol-low-up ranged from 4 months to 7.3 years, with a mean of 3.6 years. Stable moderate hydronephrosis was found in 2 (12%) kidneys and mild hydronephrosis in 7 (41%) kidneys. Mild pelvic dilation was noted in the remaining 8 (47%) kidneys. Ultrasonography after operation showed diminished hydronephrosis in all 17 children, and the DTPA scans all showed improved drainage curves. The postoperative split renal function ranged from 25% to 54% (mean: 46%). None of the children had additional episodes of colicky pain after pyeloplasty. Two children who had hypertension became normoten-sive shortly after release of the obstruction.
DISCUSSION
Classic UPJO, once it is suspected clinically, usually pre-sents no diagnostic difficulty on radiologic study. How-ever, intermittent hydronephrosis is a difficult condition to identify, and it requires a different diagnostic ap-proach. The pelvis is minimally dilated between episodes of hydronephrosis. This condition accounted for only 3.4% of all patients who underwent pyeloplasty during
a 10-year period at the Mayo Clinic.10
Acute UPJO almost immediately produces symptoms.
The rapid development of hydronephrosis causes a direct increase in the intraluminal pressure of the collecting system, physically stretching the renal capsule and col-lecting system and stimulating nerve endings in the
lam-ina propria.11 Therefore, the acute obstruction causes
pain, which is classically colicky in nature. The severity of the pain correlates with the rate of onset of the obstruction rather than the degree of distention. Even moderate distention of the pelvis will result in severe pain when it develops acutely. Intermittent hydrone-phrosis presents as recurrent, acute abdominal pain, a pattern that is not necessarily specific for Dietl’s crisis,5so
a detailed history of the pattern of pain and a thorough physical examination are the keys to diagnosing this condition. The history should include the location, na-ture, duration, frequency, precipitating factors, and tim-ing of the episodes, along with associated symptoms.
Our patients all were older than 4 years and were predominantly boys. The left kidney was more com-monly involved than the right. The pain was typically extremely intense, of sudden onset, cramping in nature, and frequently associated with nausea and vomiting and generally localized to the flank or back. However, younger children may point to the periumbilical or
epi-gastric areas. In most cases, the pain lasted for⬍48 to 72
hours followed by pain-free interval that ranged from days to months. Gross or microscopic hematuria, which was found in 50% of our patients, is an important clue that narrows the diagnosis to the urinary system. It results from acute stretching of the renal collecting
sys-tem.2Less common associated symptoms and signs
in-cluded palpable abdominal mass, hypertension, dysuria, or urinary frequency. The association of hypertension
with Dietl’s crisis has been reported repeatedly.4,12–14It is
caused by activation of the renin-angiotensin system secondary to reduced renal perfusion during acute
ure-teral obstruction.15 The 2 patients in our series with
hypertension became normotensive shortly after the ob-struction was relieved. The colicky pain may be associ-ated with gastrointestinal symptoms because of reflex stimulation of the celiac ganglion and the proximity of
adjacent intraperitoneal organs.15 Seven (39%) of our
patients received a diagnosis of gastrointestinal inflam-mation, obstruction, or dysfunction in the absence of typical urologic symptoms and signs such as back pain, hematuria, hypertension, or dysuria. Urinary tract infec-tion and ureteral or pelvic calculi also have similar pre-sentations and should be ruled out before diagnosing intermittent hydronephrosis.
Although inciting factors such as increased water in-take or use of diuretics have been reported in 40% of
patients with intermittent hydronephrosis,3,4,10the actual
pathophysiology of intermittent obstruction is not clear.
Koff et al16 reported that extrinsic mechanical
because of the volume-dependent restriction to pelvic emptying during diuresis. Mechanical obstruction is ac-tivated and resistance that is caused by the obstruction increases suddenly when pelvic volume expands and the pressure is increased. However, nearly 40% of our pa-tients had no obvious precipitating events; their acute attacks occurred unpredictably, consistent with many
other reports in the literature.3,17–19Three of our patients
had symptoms precipitated by vigorous exercise, a factor also noted by Flotte et al.4It is interesting that 4 children,
including the 1 whose kidney ruptured, had acute pain in the early morning, presumably precipitated by filling of the bladder overnight. It is reported that the degree of bladder filling and intravesical pressure are crucial
fac-tors that affect upper tract drainage.20 Bladder filling
decreases drainage of the upper tract, thus affecting up-per tract pressure. Flank pain with obstruction may be reproduced by filling the bladder in patients with
poten-tial obstructive uropathy,20 as was the case with our
patients.
Provocative tests that cause forced diuresis, such as
hydration, a diuretic IVP,10 diuretic ultrasonography,21
diuretic DTPA renal scan,8or Whitaker’s
pressure-per-fusion study,16sometimes may induce acute obstruction.
However, pain has not been reproducible uniformly with these techniques; neither is any provocative test
guaranteed to reveal obstruction.10 Ultimate diagnosis
often requires that testing be performed during an epi-sode of pain because this is the only way actually to
prove the diagnosis.10 Obstructive hydronephrosis on
any imaging study when the patient is having pain, with nonobstructive hydronephrosis or normal findings after the pain is gone, strongly suggests the diagnosis of in-termittent hydronephrosis. Therefore, multiple repeated imaging studies may be required to demonstrate rapid changes in renal anatomy during the development and the resolution of acute hydronephrosis.
Ultrasound is the preferred screening modality in the evaluation of intermittent hydronephrosis. It is nonin-vasive, quick, and repeatable; does not involve contrast media exposure or ionizing radiation; and is also useful in evaluating other organs to exclude other causes of abdominal pain. Ultrasound has high sensitivity for
de-tecting hydronephrosis.22 Therefore, if a symptomatic
patient has no or only mild dilation of the pelvis, then intermittent hydronephrosis can be excluded. UPJO is suspected when the renal pelvis is enlarged during an acute episode in the absence of ureteral dilation. How-ever, from our point of view, demonstration of decreas-ing pelvis size after an attack is as important as is dem-onstrating marked hydronephrosis in the acute stage. If the hydronephrosis cannot be shown to decrease, then it is a chronic rather than an intermittent condition. In that case, the relationship between the pain and the hydronephrosis is unclear.
By the time a patient is evaluated by ultrasound, the
obstruction may have resolved so that the hydronephro-sis has disappeared or there remains only mild dilation of the renal pelvis. Mild hydronephrosis can occur in pa-tients with normal variants, bladder distention, vesi-coureteral reflux, and chronic nonobstructive hydrone-phrosis. In addition, hydronephrosis can be found in asymptomatic children, with a reported prevalence in schoolchildren of 0.193% by portable ultrasound
screening.23Therefore, the question is how to determine
when mild hydronephrosis indicates previous obstruc-tion that has resolved, rather than some other condiobstruc-tion. From our study, we think that renal pelvic wall thick-ening on ultrasonography during convalescence is an important clue to recent dilation of the pelvis. According
to Robben et al,24 the normal pelvic wall thickness in
normal children ranges from 0.1 to 0.8 mm. They sug-gested a threshold of 0.8 mm as a reliable discriminator for pathologic conditions. All of our patients had much thicker pelvic walls, ranging from 2.5 to 5.6 mm. A thickened pelvic wall is reported to occur in various
diseases, including acute pyelitis,9,24–26 vesicoureteral
re-flux,9,24–26rejection of a renal transplant,27acute tubular
necrosis,28congenital hydronephrosis after pyeloplasty,28
mobile nephrolithiasis,29 and structural causes of
inter-mittent dilation of the collecting system.24
Three groups have mentioned the relationship
be-tween UPJO and pelvic wall thickening. Babcock et al28
first reported it in patients with UPJO after pyeloplasty.
Sorantin et al26 reported 4 cases of UPJO with renal
pelvic wall thickening, but the clinical presentation in
those cases was not described. Robben et al24 recently
evaluated the significance of renal pelvic wall thickening and found that intermittent dilation of the collecting system was an important cause. If vesicoureteral reflux is excluded, then the differential diagnosis of a thickened renal pelvic wall includes a high-pressure bladder, pri-mary obstructing megaureter, and UPJO. However, none of these studies determined the incidence of pelvic wall thickening, the timing of its occurrence, or the duration of recovery in patients with intermittent hy-dronephrosis. In all of our patients, pelvic wall thicken-ing appeared on the second or third day after a painful episode subsided, at the time when the degree of hydro-nephrosis was gradually beginning to decrease. The thickened wall then persisted for 6 to 9 days and disap-peared during the symptom-free stage, when very slight pelvic dilation was present.
The pathophysiology of renal pelvic wall thickening in intermittent hydronephrosis relates to the acute ure-teral obstruction that produces hyperperistalsis and high
intrapelvic pressure.30The thickening of the wall may be
hydronephrosis obliterates a clear view of the wall on ultrasound so that the thickening is apparent only after the obstruction is relieved and hydronephrosis
diminish-es.27 The resolution of edema and inflammation is
fol-lowed by return of the wall to its normal thickness. In our series, the thickness of the pelvic wall completely normalized during follow-up, an additional confirma-tion of the intermittent nature of this entity. We there-fore believe that the diagnosis of intermittent hydrone-phrosis could be made in most cases by a careful history, a physical examination, and serial ultrasound studies that follow the condition from the acute stage through convalescence to recovery.
Although ultrasound is useful in diagnosing intermit-tent hydronephrosis, it does not delineate the cause of UPJO or permit functional evaluation of the kidney. Therefore, additional imaging studies may be needed before surgical intervention is undertaken. Non– con-trast-enhanced CT accurately detects and characterizes
obstructing renal and ureteral calculi.31 If no stone is
present, then CT accurately identifies other causes of
flank or abdominal pain.7Therefore, CT is an effective
initial imaging tool for evaluating suspected renal colic.11
In our patients, because most of their conditions were diagnosed by a detailed history and ultrasound, CT was performed only in patients without a typical history of recurrent pain, when ureteral stone was suspected, or when the symptoms were very atypical or very acute. A VCUG is required to exclude vesicoureteral reflux. IVP has significant limitations in the evaluation of hydrone-phrosis in patients with a poorly functioning kidney or an extremely dilated pelvis. However, an IVP identifies the site of obstruction in a substantial number of cases and depicts the anatomy of UPJ. Of the 14 patients in our series who had an IVP, the correct diagnosis was appar-ent in only half. IVP is particularly helpful in evaluating the mechanism of obstruction in intermittent hydrone-phrosis, which mostly exhibits an extrinsic
compo-nent.2–6Diuretic renal scan is the most widely used
tech-nique to assess the function and drainage of the kidneys in the presence of hydronephrosis. Although a delayed double-peak sign on diuretic renal scan is thought to be diagnostic of intermittent hydronephrosis during
symp-tom-free intervals,8 it still is necessary to demonstrate
obstructive hydronephrosis during an acute attack be-fore proceeding to surgery. As with ultrasonography, an IVP or a diuretic renal scan is best performed in the symptomatic period. We believe that the timing of diag-nostic studies is actually more important than the imag-ing modality used.
UPJO may involve intrinsic2–5,8,17,32 or extrinsic
com-ponents.5,8,10,19,32Intrinsic narrowing or an adynamic
seg-ment of the ureter is characterized by a linear pressure-flow response pattern with fixed resistance at the UPJ. Extrinsic compression of the ureter produces a complex volume-dependent response pattern with an acute
self-obstructing crisis after diuresis.16 Although extrinsic
causes of UPJO were recognized at operation in most
patients with intermittent hydronephrosis,2–5,8,17,32
intrin-sic mechanisms were also repeatedly reported.5,8,10,19,32
Lebowitz33 believed that when a child presents with
UPJO because of symptoms, approximately half are caused by extrinsic obstruction. In our patients, intrinsic obstruction was present in 35% and extrinsic compres-sion in 53%. Only 2 children had a fibroepithelial polyp accounting for the disorder. Although aberrant vessels, bands, adhesions, or kinks all have been implicated in
UPJO, Homsy et al8suggested that other factors may be
involved, although such factors have yet to be identified.
Koff et al16 suggested that extrinsic and intrinsic UPJO
may coexist to produce intermittent hydronephrosis.
Park et al34also concluded that most patients likely had
⬎1 possible cause of obstruction. They stated that most
UPJO caused by either intrinsic stenosis or aberrant ves-sels also had secondary obstruction, such as anomalous insertions and periureteral fibrosis. Therefore, coexisting intrinsic and extrinsic causes must be considered and assessed intraoperatively. In addition to relief of extrinsic compression, intrinsic stenosis requires appropriate management. For most patients, dismembered pyelo-plasty is adequate in this regard. In general, pyelopyelo-plasty relieves the pain and obstruction and ensures excellent functional recovery. Good renal function is expected in most of these children, because the obstruction is tran-sient. We believe that intermittent hydronephrosis is an absolute indication for surgery. Without correction, there is the potential for irreversible hydronephrosis
cul-minating in severe renal dysfunction5or even rupture of
the kidney, as occurred in 1 of our patients.
REFERENCES
1. Dietl J. On strangulation of floating kidneys [in German].Wien Med Wochenschr.1864;14:153–166, 579 –181, 593–595 2. Belman AB. Ureteropelvic junction obstruction as a cause for
intermittent abdominal pain in children. Pediatrics. 1991;88: 1066 –1069
3. Mergener K, Weinerth JL, Baillie J. Dietl’s crisis: a syndrome of episodic abdominal pain of urologic origin that may present to a gastroenterologist.Am J Gastroenterol.1997;92:2289 –2291 4. Flotte TR. Dietl syndrome: intermittent ureteropelvic junction
obstruction as a cause of episodic abdominal pain. Pediatrics.
1988;82:792–794
5. Byrne WJ, Arnold WC, Stannard MW, Redman JF. Uretero-pelvic junction obstruction presenting with recurrent abdomi-nal pain: diagnosis by ultrasound.Pediatrics.1985;76:934 –937 6. Nesbit RM. Diagnosis of intermittent hydronephrosis: impor-tance of pyelography during episodes of pain.J Urol.1956;75: 767–771
7. Shokeir AA. The diagnosis of upper urinary tract obstruction.
BJU Int.1999;83:893–901
8. Homsy YL, Mehta PH, Huot D, Danais S. Intermittent hydro-nephrosis: a diagnostic challenge.J Urol.1988;140:1222–1226 9. Alton DJ, LeQuesne GW, Gent R, Siegmann JW, Byard R.
10. Malek RS. Intermittent hydronephrosis: the occult ureteropel-vic obstruction.J Urol.1983;130:863– 866
11. Shokeir AA. Renal colic: pathophysiology, diagnosis and treat-ment.Eur Urol.2001;39:241–249
12. Johnston JH, Evans JP, Glassberg KI, Shapiro SR. Pelvic hy-dronephrosis in children: a review of 219 personal cases.J Urol.
1977;117:97–101
13. Nixon HH. Hydronephrosis in children: a clinical study of seventy-eight cases with special reference to the role of aber-rant renal vessels and the results of conservative operations.
Br J Surg.1953;40:601– 609
14. Perlberg S, Pfau A. Management of ureteropelvic junction obstruction associated with lower polar vessels.Urology.1984; 23:13–18
15. Nemoy NJ, Fichman, Sellers A. Unilateral ureteral obstruction: a cause of reversible high rennin content hypertension.JAMA.
1973;225:512–513
16. Koff SA, Hayden LJ, Cirulli C, Shore R. Pathophysiology of ureteropelvic junction obstruction: experimental and clinical observations.J Urol.1986;136:336 –338
17. Gabutti L, Alerci M, Marone C. Spiral CT angiography for discriminating between megacalyces and intermittent hydro-nephrosis.Nephrol Dial Transplant.1997;12:1487–1489 18. Jacobs JA, Berger BW, Goldman SM, Robbins MA. Young JD
Jr. Ureteropelvic obstruction in adults with previously normal pyelograms: a report of 5 cases.J Urol.1979;121:242–244 19. O’Reilly PH. Relationship between intermittent
hydronephro-sis and megacalicohydronephro-sis.Br J Urol.1989;64:125–129
20. Jones DA, Lupton EW, George NJR. Effect of bladder filling on upper tract urodynamics in man.Br J Urol.1990;65:492– 496 21. Rosi P, Virgili G, Di Stasi SM, et al. Diuretic ultrasound. A non-invasive technique for the assessment of upper tract ob-struction.Br J Urol.1990;65:566 –569
22. Scheible W, Talner LB. Gray scale ultrasound and the genito-urinary tract: a review of clinical applications.Radiol Clin North Am.1979;17:281–300
23. Sheih CP, Liu MB, Hung CS, Yang KH, Chen WY, Lin CY. Renal abnormalities in schoolchildren. Pediatrics. 1989;84: 1086 –1090
24. Robben SGF, Boesten M, Linmans J, Lequin MH, Nijman RM. Significance of thickening of the wall of the renal collecting system in children: an ultrasound study.Pediatr Radiol.1999; 29:736 –740
25. Tain YL. Renal pelvic wall thickening in children urinary tract infections: evidence of acute pyelitis or vesicoureteral reflux?
Scand J Urol Nephrol.2003;37:28 –30
26. Sorantin E, Fotter R, Aigner R, Ring E, Riccabona M. The sonographically thickened wall of the upper urinary tract system: correlation with other imaging methods.Pediatr Radiol.
1997;27:667– 671
27. Nicolet V, Carignan L, Dubuc G, He´bert G, Bourdon F, Paquin F. Thickening of the renal collecting system: a nonspecific finding at US.Radiology.1988;168:411– 413
28. Babcock DS. Sonography of wall thickening of the renal col-lecting system. A nonspecific finding.J Ultrasound Med.1987; 6:29 –32
29. Benya EC. Thickening of the renal collecting system wall in children.Pediatr Radiol.2000;30:717–718
30. Crowley AR, Byrne JC, Vaughan ED Jr, Marion DN. The effect of acute obstruction on ureteral function. J Urol.1990;143: 596 –599
31. Langer JE. Computed tomography and ultrasonography of acute renal abnormalities.Semin Roentgenol.2001;2:99 –107 32. Higuchi A, Nakai H, Miyazato M, Izumitani M, Shishido S,
Kawamura T. [Intermittent hydronephrosis. A clinical study in 23 pediatric patients].Nippon Hinyokika Gakkai Zasshi.1996;87: 1145–1150
33. Lebowitz RL. Paediatric urology and uroradiology: changes in the last 25 years.BJU Int.2003;92(suppl):7–9
34. Park JM, Bloom DA. The pathophysiology of UPJ obstruction. Current concepts.Urol Clin North Am.1998;25:161–169
RANDOMIZED TRIALS STOPPED EARLY FOR BENEFIT: A SYSTEMATIC REVIEW
Context:Randomized clinical trials (RCTs) that stop earlier than planned because of apparent benefit often receive great attention and affect clinical practice. Their prevalence, the magnitude and plausibility of their treatment effects, and the extent to which they report information about how investi-gators decided to stop early are, however, unknown. . . .
Data Synthesis:Of 143 RCTs stopped early for benefit, the majority (92) were published in 5 high-impact medical journals. Typically, these were industry-funded drug trials in cardiology, cancer, and human immunodefi-ciency virus/AIDS. The proportion of all RCTs published in high-impact journals that were stopped early for benefit increased from 0.5% in 1990 –
1994 to 1.2% in 2000 –2004 (P⬍.001 for trend) . . .
Conclusions:RCTs stopped early for benefit are becoming more common, often fail to adequately report relevant information about the decision to stop early, and show implausibly large treatment effects, particularly when the number of events is small. These findings suggest clinicians should view the results of such trials with skepticism.
DOI: 10.1542/peds.2005-0583
2006;117;139
Pediatrics
Lee, Jin-Cherng Sheu and Pei-Yeh Chang
Jeng-Daw Tsai, Fu-Yuan Huang, Chun-Chen Lin, Tsuen-Chiuan Tsai, Hung-Chang
Clinical and Imaging Features
Intermittent Hydronephrosis Secondary to Ureteropelvic Junction Obstruction:
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/1/139
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/1/139#BIBL
This article cites 34 articles, 5 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/urology_sub
Urology
http://www.aappublications.org/cgi/collection/radiology_sub
Radiology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-0583
2006;117;139
Pediatrics
Lee, Jin-Cherng Sheu and Pei-Yeh Chang
Jeng-Daw Tsai, Fu-Yuan Huang, Chun-Chen Lin, Tsuen-Chiuan Tsai, Hung-Chang
Clinical and Imaging Features
Intermittent Hydronephrosis Secondary to Ureteropelvic Junction Obstruction:
http://pediatrics.aappublications.org/content/117/1/139
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.