Original Article
Intercellular adhesion molecule 1
rs5498 A>G
polymorphism is associated with coronary
artery disease risk: a meta-analysis
Xingchun Zheng1*, Weifeng Tang2*, Yafeng Wang3*, Haiyong Gu4, Chao Liu2, Rong Hu1
1Department of Cardiology, Union Hospital, Fujian Medical University, Fuzhou, Fujian Province, China; 2
Depart-ment of Cardiothoracic Surgery, Affiliated People’s Hospital of Jiangsu University, Zhenjiang, Jiangsu Province, China; 3Department of Cardiology, The People’s Hospital of Xishuangbanna Dai Autonomous Prefecture, Jinghong,
Yunnan Province, China; 4Department of Thoracic Srugery, Shanghai Chest Hospital, Shanghai Jiaotong University,
Shanghai, China. *Equal contributors.
Received March 9, 2016; Accepted June 3, 2016; Epub July 15, 2016; Published July 30, 2016
Abstract: Objectives: The association of intercellular adhesion molecule 1 (ICAM-1) rs5498 A>G (K469E) polymor-phism with coronary artery disease (CAD) susceptibility has been widely explored; however, these studies have
yielded conflicting results. To address the correlation more precisely, we performed this pooled analysis. Design and
Methods: EmBase, PubMed and China Biology Medicine (CBM) databases were independently searched by two au-thors for eligible studies before January 15, 2016. Fixed-effects or random-effects model was used to calculate the
odds ratios (ORs) and their 95% confidence intervals (CIs) when appropriate. Results: Meta-analysis of total studies demonstrated that variants of ICAM-1 rs5498 A>G were significantly correlated with the decreased susceptibility of CAD. Subgroup analyses by different types of CAD and different populations also identified a significant correla -tion. In addition, sensitivity analysis further suggested a relationship of ICAM-1 rs5498 A>G polymorphism with CAD risk. Conclusions: In summary, the present meta-analysis of available data indicates that the ICAM-1 rs5498 A>G polymorphism probably decreases the susceptibility of CAD, especially in Caucasians and myocardial infarction subgroups.
Keywords: Polymorphism, ICAM-1, coronary artery disease, myocardial infarction susceptibility, meta-analysis
Introduction
Coronary artery disease (CAD) is the leading cause of death in developed countries, and the prevalence is expected to promote worldwide [1]. The incidence and mortality rate of CAD boost largely for aging of the population, as well as an increasing prevalence of established CAD-related lifestyles, such as physical inactiv-ity, heavy smoking, drinking and ‘westernized’ diets. However, the mechanism of atheroscle-rosis is very complicated and remains unclear, although it has been considered a chronic inflammation process.
The intercellular adhesion molecule 1 (ICAM-1) gene, a member of the immunoglobulin (Ig) superfamily, is located on chromosome 19q- 13.3. ICAM-1 is a cell adhesion molecule and plays an important role in leukocytes adhering
Accumulating evidences indicate single nucleo-tide polymorphisms (SNPs) of ICAM-1 gene may play crucial roles in atherosclerotic pro-cesses. ICAM-1 gene is polymorphic, and a lot of SNPs have been identified, such as rs5498 A>G (K469E), rs1799969 G>A, rs3093030 C>T, rs5030382 A>G, rs281432 C>G, rs5496 A>G, rs5490 A>C and rs281428 C>T polymor-phisms etc. Among them, the rs5498 A>G (K469E) polymorphism of ICAM-1 gene was the most extensively studied for its implication in CAD risk. Some previous studies showed that
ICAM-1 rs5498 A>G polymorphism was invol-ved in the etiology of CAD and myocardial infarction (MI). However, the findings of previ -ous studies remain inconsistent rather than conclusive. Considering the important role of
ICAM-1 rs5498 A>G polymorphism in athero-sclerotic processes, we conducted a pooled analysis on all available data to assess the CAD risk correlated with ICAM-1 rs5498 A>G poly-morphism. To the best of our knowledge, the present meta-analysis is the most comprehen-sive study with respect to the relationship of
ICAM-1 rs5498 A>G variants with CAD risk.
Materials and methods
Search strategy
We carried out an extensively online search of the PubMed, Embase and China Biology Medicine (CBM) databases from the inception up to January 15, 2016. Search terms for ICAM-1 polymorphism and CAD risk were: ‘Intercellular adhesion molecule-1’ or ‘intercellular adhesion molecule 1’ or ‘ICAM 1’ or ‘ICAM-1’, ‘SNP’ or ‘polymorphism’ or ‘variant’ or ‘mutation’ and ‘coronary artery disease’ or ‘CAD’ or ‘coronary heart disease’ or ‘CHD’ or ‘myocardial infarc-tion’ or ‘MI’. No language restriction was imposed. In addition, all references cited in the retrieved publications were manually searched to identify additional publications.
Inclusion and exclusion criteria
The major selection criteria were: (1) case-con-trol studies which evaluated the relationship of
ICAM-1 rs5498 A>G polymorphism with CAD
susceptibility, (2) genotype distribution of con-trols consistent with Hardy-Weinberg Equili- brium (HWE), (3) containing data on genotype and allele frequency for estimating odds ratios (ORs) with 95% confidence intervals (95% CIs).
Accordingly, publications without sufficient da-ta, duplicated dada-ta, not case-control study design, reviews, meta-analysis and comments were excluded.
Data extraction
Two reviewers (X. Zheng and W. Tang) extracted the corresponding information independently. Disagreements were resolved based on discus-sion among all authors. The extracted informa-tion contained: the surname of first author, year of publication, country, ethnicity, type of CAD, genotyping method and genotype frequencies.
Statistical analysis
The association of ICAM-1 rs5498 A>G variants with CAD risk was assessed by calculating ORs with 95% CIs, based on the genotype number in cases and controls. The pooled ORs and their CIs were calculated for four genetic models, such as dominant model, recessive model, homozygote comparison and allele comparison model. A Chi-square-based statistic I2 test was
used to evaluate heterogeneity [10] and an
I2<25% indicates low heterogeneity, 25%≤I2≤
50% indicates moderate heterogeneity and
I2>50% indicates large heterogeneity [11].
Mantel-Haenszel method (the fixed effects model) was harnessed when there was no sig-nificant heterogeneity [12]; otherwise, Der Simonian-Laird method (the random effects model) was used [13]. One-way sensitivity anal-ysis was performed by omitting each individual study at a time from the total and re-calculating the remainder [21]. Sub-group analyses were performed to identify the source of heterogene-ity, such as ethnicheterogene-ity, the type of CAD, sample size and source of control. Publication bias was assessed with Begg’s funnel plot and Egger’s regression method [14] (P<0.05 was defined representative of statistical publication bias). All p values were two-sided. All available data were analyzed using STATA version 12.0 soft-ware (Stata Corp, College Station, Texas USA).
Results
Characteristics
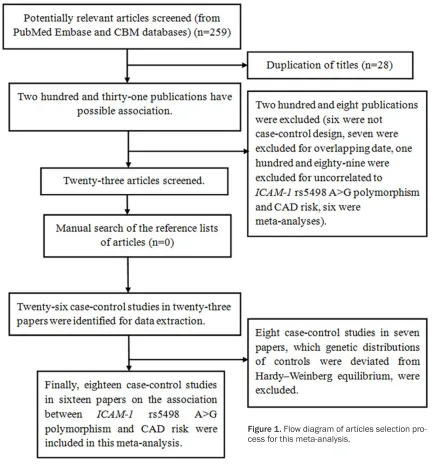
In total, 259 potentially relevant articles were retrieved from the initial search. Figure 1
eigh-teen comparisons were identified [15-30]. Of these articles, eight investigated MI [15, 18-23, 25], nine investigated non-MI [16, 17, 21, 22, 26-30] and one investigated mixed CAD [24]. Among eighteen case-control studies, ten were from Caucasians [15, 18-23, 30] and eight were from Asians [16, 17, 24-29]. The detailed characteristics of these eligible studies and the distribution of ICAM-1 rs5498 A>G variants as well as alleles are shown in Tables 1 and 2, respectively.
Quantitative synthesis
Eighteen eligible studies with 3,484 cases and 3,911 controls met the major inclusion criteria.
The results of the meta-analysis on ICAM-1
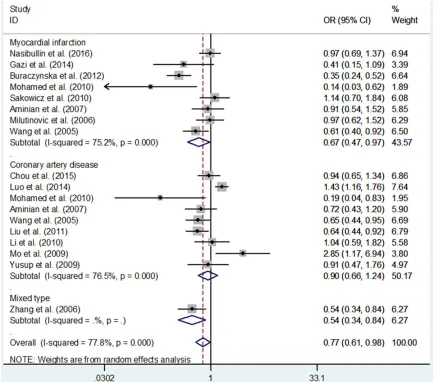
[image:3.612.91.524.71.538.2]rs5498 A>G polymorphism and CAD risk are listed in Table 3. Overall, there was a signifi -cantly decreased risk of CAD risk in four genetic models: OR, 0.76; 95% CI, 0.62-0.94; P=0.011 for G vs. A; OR, 0.63; 95% CI, 0.42-0.93; P= 0.019 for GG vs. AA; OR, 0.77; 95% CI, 0.61-0.98; P=0.030 for GG+AG vs. AA and OR, 0.70; 95% CI, 0.51-0.95; P=0.023 for AG vs. AA (Figure 2 and Table 3). In a subgroup analysis by ethnicity, a significantly decreased CAD risk was found among Caucasians (OR, 0.64; 95% CI, 0.46-0.89; P=0.008 for G vs. A; OR, 0.48; 95% CI, 0.26-0.89; P=0.020 for GG vs. AA; OR, 0.67; 95% CI, 0.48-0.95; P=0.023 for GG+AG
vs. AA and OR, 0.59; 95% CI, 0.36-0.96; P= 0.035 for GG vs. AG+AA), but not Asians (Figure 2 and Table 3). In a subgroup analysis by the type of CAD, ICAM-1 rs5498 A>G polymorphism
was correlated with a significantly decreased risk of MI (OR, 0.63; 95% CI, 0.44-0.91; P= 0.012 for G vs. A; OR, 0.43; 95% CI, 0.21-0.86;
P=0.017 for GG vs. AA; OR, 0.67; 95% CI,
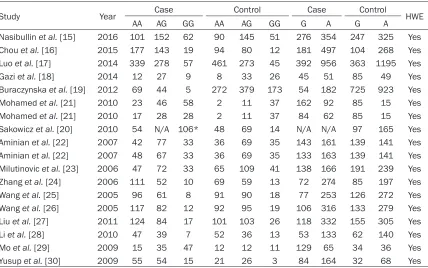
0.47-Table 1. Characteristics of the individual studies included in the meta-analysis
Study Year Country Ethnicity Type No. of cases/ controls Source of control Genotype Method
Nasibullin et al. [15] 2016 Russian Federation Caucasians Myocardial infarction 315/286 HB PCR-RFLP Chou et al. [16] 2015 China Asians Coronary artery disease 339/186 HB TaqMan
Luo et al. [17] 2014 China Asians Coronary artery disease 674/779 PB PCR-RFLP
Gazi et al. [18] 2014 Turkey Caucasians Myocardial infarction 48/67 HB Real-time PCR Buraczynska et al. [19] 2012 Poland Caucasians Myocardial infarction 118/824 HB Nested PCR Mohamed et al. [21] 2010 Egypt Caucasians Coronary artery disease 127/50 HB PCR-RFLP Mohamed et al. [21] 2010 Egypt Caucasians Myocardial infarction 73/50 HB PCR-RFLP Sakowicz et al. [20] 2010 Poland Caucasians Myocardial infarction 163/140 PB PCR-RFLP Aminian et al. [22] 2007 Iran Caucasians Myocardial infarction 152/140 HB PCR-RFLP Aminian et al. [22] 2007 Iran Caucasians Coronary artery disease 148/140 HB PCR-RFLP Milutinovic et al. [23] 2006 Slovenia Caucasians Myocardial infarction 152/215 HB PCR-RFLP Zhang et al. [24] 2006 China Asians Mixed type 173/141 HB PCR-RFLP
Wang et al. [25] 2005 China Asians Myocardial infarction 165/199 HB PCR-RFLP
Wang et al. [26] 2005 China Asians Coronary artery disease 211/206 HB PCR-RFLP
Liu et al. [27] 2011 China Asians Coronary artery disease 312/302 HB PCR-RFLP
Li et al. [28] 2010 China Asians Coronary artery disease 93/101 HB PCR-SSP
Mo et al. [29] 2009 China Asians Coronary artery disease 97/35 PB PCR-RFLP
Yusup et al. [30] 2009 China Caucasians Coronary artery disease 124/50 PB PCR-RFLP
[image:4.612.91.525.85.332.2]PCR-RFLP: polymerase chain reaction-restriction fragment length polymorphism; PCR-SSP: polymerase chain reaction-sequence specific primer.
Table 2. Distribution of ICAM-1 polymorphism genotype and allele
Study Year Case Control Case Control HWE
AA AG GG AA AG GG G A G A
Nasibullin et al. [15] 2016 101 152 62 90 145 51 276 354 247 325 Yes Chou et al. [16] 2015 177 143 19 94 80 12 181 497 104 268 Yes Luo et al. [17] 2014 339 278 57 461 273 45 392 956 363 1195 Yes
Gazi et al. [18] 2014 12 27 9 8 33 26 45 51 85 49 Yes
Buraczynska et al. [19] 2012 69 44 5 272 379 173 54 182 725 923 Yes
Mohamed et al. [21] 2010 23 46 58 2 11 37 162 92 85 15 Yes
Mohamed et al. [21] 2010 17 28 28 2 11 37 84 62 85 15 Yes
Sakowicz et al. [20] 2010 54 N/A 106* 48 69 14 N/A N/A 97 165 Yes Aminian et al. [22] 2007 42 77 33 36 69 35 143 161 139 141 Yes Aminian et al. [22] 2007 48 67 33 36 69 35 133 163 139 141 Yes Milutinovic et al. [23] 2006 47 72 33 65 109 41 138 166 191 239 Yes Zhang et al. [24] 2006 111 52 10 69 59 13 72 274 85 197 Yes Wang et al. [25] 2005 96 61 8 91 90 18 77 253 126 272 Yes Wang et al. [26] 2005 117 82 12 92 95 19 106 316 133 279 Yes Liu et al. [27] 2011 124 84 17 101 103 26 118 332 155 305 Yes Li et al. [28] 2010 47 39 7 52 36 13 53 133 62 140 Yes Mo et al. [29] 2009 15 35 47 12 12 11 129 65 34 36 Yes
Yusup et al. [30] 2009 55 54 15 21 26 3 84 164 32 68 Yes
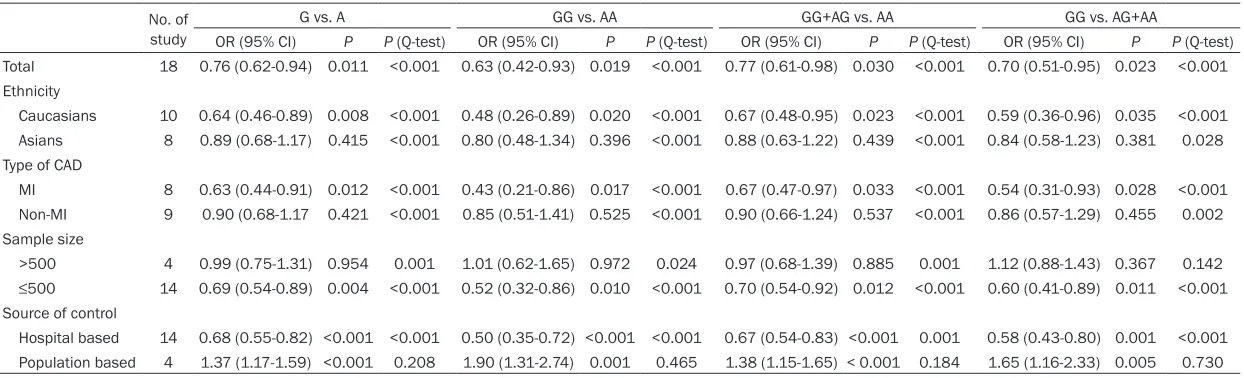
[image:4.612.94.522.376.644.2]Table 3. Meta-analysis of the ICAM-1 rs5498 A>G polymorphism and CAD risk No. of
study
G vs. A GG vs. AA GG+AG vs. AA GG vs. AG+AA
OR (95% CI) P P (Q-test) OR (95% CI) P P (Q-test) OR (95% CI) P P (Q-test) OR (95% CI) P P (Q-test) Total 18 0.76 (0.62-0.94) 0.011 <0.001 0.63 (0.42-0.93) 0.019 <0.001 0.77 (0.61-0.98) 0.030 <0.001 0.70 (0.51-0.95) 0.023 <0.001 Ethnicity
Caucasians 10 0.64 (0.46-0.89) 0.008 <0.001 0.48 (0.26-0.89) 0.020 <0.001 0.67 (0.48-0.95) 0.023 <0.001 0.59 (0.36-0.96) 0.035 <0.001 Asians 8 0.89 (0.68-1.17) 0.415 <0.001 0.80 (0.48-1.34) 0.396 <0.001 0.88 (0.63-1.22) 0.439 <0.001 0.84 (0.58-1.23) 0.381 0.028 Type of CAD
MI 8 0.63 (0.44-0.91) 0.012 <0.001 0.43 (0.21-0.86) 0.017 <0.001 0.67 (0.47-0.97) 0.033 <0.001 0.54 (0.31-0.93) 0.028 <0.001 Non-MI 9 0.90 (0.68-1.17 0.421 <0.001 0.85 (0.51-1.41) 0.525 <0.001 0.90 (0.66-1.24) 0.537 <0.001 0.86 (0.57-1.29) 0.455 0.002 Sample size
>500 4 0.99 (0.75-1.31) 0.954 0.001 1.01 (0.62-1.65) 0.972 0.024 0.97 (0.68-1.39) 0.885 0.001 1.12 (0.88-1.43) 0.367 0.142
≤500 14 0.69 (0.54-0.89) 0.004 <0.001 0.52 (0.32-0.86) 0.010 <0.001 0.70 (0.54-0.92) 0.012 <0.001 0.60 (0.41-0.89) 0.011 <0.001 Source of control
Hospital based 14 0.68 (0.55-0.82) <0.001 <0.001 0.50 (0.35-0.72) <0.001 <0.001 0.67 (0.54-0.83) <0.001 0.001 0.58 (0.43-0.80) 0.001 <0.001 Population based 4 1.37 (1.17-1.59) <0.001 0.208 1.90 (1.31-2.74) 0.001 0.465 1.38 (1.15-1.65) < 0.001 0.184 1.65 (1.16-2.33) 0.005 0.730
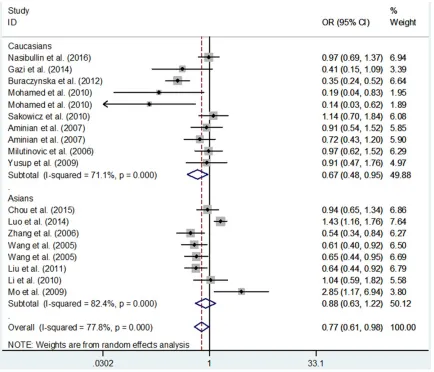
Figure 2. Meta-analysis with a random-effects model for the relationship between ICAM-1 rs5498 A>G polymor-phism and CAD risk in different ethnicity (GG+AG vs. AA genetic model).
0.97; P=0.033 for GG+AG vs. AA and OR, 0.54; 95% CI, 0.31-0.93; P=0.028 for GG vs. AG+AA), but not of non-MI (Figure 3 and Table 3).
Tests for publication bias
We carrieded out Begg’s funnel plot and Egger’s test to measure the publication bias of eligible studies. No evidence of publication bias was found in our findings (GG+AG vs. AA: Begg’s test
P=0.325, Egger’s test P=0.059) (Figure 4).
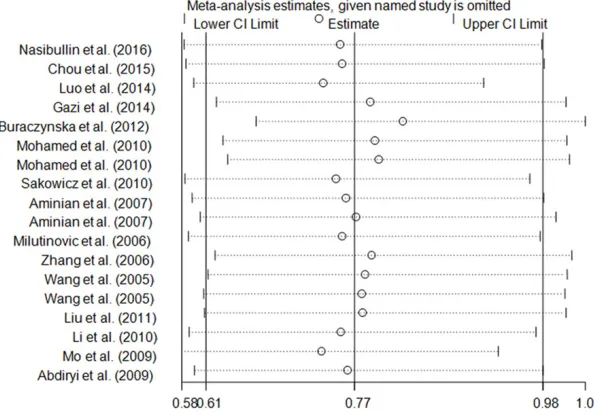
Tests for sensitivity analyses
Influence of an individual case-control study involved in the present meta-analysis on the pooled ORs and CIs was evaluated by removing each study in turn and repeating the meta-anal-ysis. As shown in Figure 5, the corresponding
pooled ORs and CIs were not materially altered (data not shown).
Tests for heterogeneity
As shown in Table 3, significant heterogeneity between included studies was found in overall comparisons. Thus, we examined the source of heterogeneity by subgroup analysis (Table 3). The results indicated that Caucasians, MI, small sample size and hospital-based sub-groups may contribute to the major source of heterogeneity (Table 3).
Discussion
patho-Figure 3. Meta-analysis with a random-effects model for the relationship between ICAM-1 rs5498 A>G polymor-phism and CAD risk in different CAD type (GG+AG vs. AA genetic model).
genic process of inflammatory diseases, ath -erosclerosis and thrombosis [31-34]. During inflammation reaction, sICAM-1 is produced by several cells, such as fibroblasts, leukocytes, endothelial cells and epithelial cells, which is activated by multiple cytokines and then pro-duce a number of membrane ICAM-1 [35]. The level of serum sICAM-1 was relatively low in healthy controls; however, it was elevated with acute coronary syndrome [6, 36].
Recently, accumulating studies focused on the relationship between ICAM-1 rs5498 A>G vari-ants and CAD risk. In the present study, we con-ducted a meta-analyses to assess the associa-tion between CAD risk and ICAM-1 rs5498 A>G polymorphism. The findings suggested that the
ICAM-1 rs5498 G allele was a protective factor
for CAD. Several meta-analyses have been per-formed on this SNP correlated with the suscep-tibility of CAD [37-40]. However, none of them have comprehensively covered all eligible stud-ies on ICAM-1 rs5498 A>G polymorphism. In the present pooled analysis, we included all the potential papers published to date on this SNP correlated with CAD risk, and thus incorporated more eligible case-control studies than the pre-viously published studies. To the best of our knowledge, our study was the most comprehen-sive meta-analysis in this field.
The rs5498 A>G polymorphism, a SNP in exon 6 of ICAM-1, encodes a glutamate→lysine sub -stitution at amino acid residue 469 (E469K). The previous study indicated that ICAM-1
[image:7.612.89.527.71.453.2]splicing patterns which resulted in AA genotype may have a lower sensitivity to apoptosis than GG genotype [41], then altered the ability of cell-cell interactions and inflammatory res-ponse. In the present study, we found that
ICAM-1 rs5498 A>G locus conferred the de- creased susceptibility to CAD, suggesting the presence of the G allele, which was correlated with apoptosis, might decrease the susceptibil-ity of CAD. In a subgroup analysis by ethnicsusceptibil-ity, a significant association between ICAM-1 rs5498
[image:8.612.90.391.73.275.2]the results of this meta-analysis were based on the crude estimates. Thirdly, large heterogene-ity was found in our study, thus the results should be interpretated with cautions. Fourth, the sample size of the eligible studies was rela-tively small. Simultaneously, in this meta-ana- lysis, no genome-wide association studies (GWAS) was recruited. Compared to the classi-cal candidate-gene approach, GWAS is a pow-erful approach to assess the common genetic variants. Finally, in this study, we only focused
Figure 4. Begg’s funnel plot of meta-analysis of the relationship between the
ICAM-1 rs5498 A>G polymorphism and the risk of CAD (GG+AG vs. AA genetic model).
Figure 5. Sensitivity analysis of the influence of GG+AG vs. AA genetic model in
CAD meta-analysis (random-effects estimates for ICAM-1 rs5498 A>G polymor-phism).
A>G polymorphism and the decreased CAD risk was found in Caucasians, but not Asians. Results of the present study indicat-ed the influence of ICAM-1 rs5498 A>G polymor-phism and diversity in different races to the risk of CAD. In a subgroup analysis by the type of CAD, ICAM-1 rs5498 A>G polymorphism was corre-lated with the decreased risk of MI, but not of non-MI. We first confirmed that ICAM-1 rs5498 A>G polymorphism conferred a decreased risk to MI. However, these findings should be interpreted with caution. For MI, only eight small sample sizes studies with 1186 cases and 1921 controls were included in this meta-analysis, which may have limited power to obtain a real influence. Large het -erogeneity also should be considered.
[image:8.612.93.390.331.538.2]on ICAM-1 rs5498 A>G polymorphism, and did not ponder other locus in ICAM-1 gene or risk genes.
In summary, the present meta-analysis sug-gests that the ICAM-1 rs5498 A>G polymor-phism probably decreases the susceptibility of CAD, especially in Caucasians and myocardial infarction subgroups. To further confirm the findings, large-scale epidemiological studies with different ethnic groups assessing gene-environment and gene-gene interactions are needed.
Acknowledgements
This study was supported in part by Jiangsu University Clinical Medicine Science and Tech- nology Development Fund (JLY20140012).
Disclosure of conflict of interest
None.
Address correspondence to: Rong Hu, Department of Cardiology, Union Hospital, Fujian Medical Uni- versity, Fuzhou 350001, China. E-mail: 1336591- [email protected]
References
[1] WRITING GROUP MEMBERS, Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB, Ford E, Furie K, Gil-lespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lack-land D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Rog-er VL, Thom T, WassRog-erthiel-SmollRog-er S, Wong ND, Wylie-Rosett J; American Heart Associa-tion Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke sta-tistics--2010 update: a report from the Ameri-can Heart Association. Circulation 2010; 121: e46-e215.
[2] Lawson C and Wolf S. ICAM-1 signaling in en-dothelial cells. Pharmacol Rep 2009; 61: 22-32.
[3] Yang L, Froio RM, Sciuto TE, Dvorak AM, Alon R and Luscinskas FW. ICAM-1 regulates neutro-phil adhesion and transcellular migration of TNF-alpha-activated vascular endothelium
un-der flow. Blood 2005; 106: 584-592.
[4] Dietrich JB. The adhesion molecule ICAM-1 and its regulation in relation with the blood-brain barrier. J Neuroimmunol 2002; 128: 58-68.
[5] Roebuck KA and Finnegan A. Regulation of in-tercellular adhesion molecule-1 (CD54) gene expression. J Leukoc Biol 1999; 66: 876-888. [6] Mashru MR, Shah VK, Soneji SL, Loya YS,
Vas-vani JB, Payannavar S, Walvalkar A, Mith-bawkar SS, Mokal R, Kudalkar K, Abraham A, Thakur PK and Shalia KK. Soluble levels of cell adhesion molecules (CAMs) in coronary artery disease. Indian Heart J 2010; 62: 57-63. [7] Mizia-Stec K, Gasior Z, Zahorska-Markiewicz B,
Holecki M and Kumor P. Inflammatory markers
in a 2-year follow-up of coronary artery dis-ease. Heart Vessels 2006; 21: 302-308. [8] Hajilooi M, Sanati A, Ahmadieh A, Ghofraniha A
and Massoud A. Circulating ICAM-1, VCAM-1, E-selectin, P-selectin, and TNFRII in patients with coronary artery disease. Immunol Invest 2004; 33: 263-275.
[9] Poston RN, Haskard DO, Coucher JR, Gall NP and Johnson-Tidey RR. Expression of intercel-lular adhesion molecule-1 in atherosclerotic plaques. Am J Pathol 1992; 140: 665-673. [10] Higgins JP and Thompson SG. Quantifying
het-erogeneity in a meta-analysis. Stat Med 2002; 21: 1539-1558.
[11] Higgins JP, Thompson SG, Deeks JJ and Altman DG. Measuring inconsistency in meta-analy-ses. BMJ 2003; 327: 557-560.
[12] Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 1959; 22: 719-748.
[13] DerSimonian R and Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7: 177-188.
[14] Egger M, Davey Smith G, Schneider M and Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629-634.
[15] Nasibullin TR, Timasheva YR, Sadikova RI, Tuk-tarova IA, Erdman VV, Nikolaeva IE, Sabo J,
Kruzliak P and Mustafina OE. Genotype/allelic
combinations as potential predictors of myo-cardial infarction. Mol Biol Rep 2016; 43: 11-16.
[16] Chou CH, Ueng KC, Liu YF, Wu CH, Yang SF and Wang PH. Impact of Intercellular Adhesion Mol-ecule-1 Genetic Polymorphisms on Coronary Artery Disease Susceptibility in Taiwanese Subjects. Int J Med Sci 2015; 12: 510-516. [17] Luo JY, Ma YT, Xie X, Yang YN, Li XM, Ma X, Yu
Z, Chen BD and Liu F. Association of intercel-lular adhesion molecule1 gene polymorphism with coronary heart disease. Mol Med Rep 2014; 10: 1343-1348.
coronary slow flow. Med Princ Pract 2014; 23:
346-350.
[19] Buraczynska M, Zaluska W, Baranowicz-Gaszc-zyk I, Buraczynska K, NiemcBaranowicz-Gaszc-zyk E and Ksiazek A. The intercellular adhesion molecule-1 (ICAM-1) gene polymorphism K469E in end-stage renal disease patients with cardiovascu-lar disease. Hum Immunol 2012; 73: 824-828. [20] Sakowicz A, Fendler W, Lelonek M and Pietru-cha T. Genetic variability and the risk of myo-cardial infarction in Poles under 45 years of age. Arch Med Sci 2010; 6: 160-167.
[21] Mohamed AA, Rashed L, Amin H, Abu-Farha M, El Fadl SA and Pakhoum S. K469E polymor-phism of the intercellular adhesion molecule-1 gene in Egyptians with coronary heart disease. Ann Saudi Med 2010; 30: 432-436.
[22] Aminian B, Abdi Ardekani AR and Arandi N. ICAM-1 polymorphisms (G241R, K469E), in coronary artery disease and myocardial infarc-tion. Iran J Immunol 2007; 4: 227-235. [23] Milutinovic A and Petrovic D. The K469E
poly-morphism of the intracellular adhesion mole-cule 1 (ICAM-1) gene is not associated with myocardial infarction in Caucasians with type 2 diabetes. Folia Biol (Praha) 2006; 52: 79-80. [24] Zhang SR, Xu LX, Gao QQ, Zhang HQ, Xu BS,
Lin J and Huang WJ. [The correlation between ICAM-1 gene K469E polymorphism and coro-nary heart disease]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 2006; 23: 205-207.
[25] Wang M, Li Y, Zhang PA, Yang C, Xiang PX, Wei YS, Li XY and Huang CX. [Study on the intercel-lular molecule-1 polymorphisms in an Chinese population with myocardial infarction]. Zhong-hua Liu Xing Bing Xue Za Zhi 2005; 26: 702-706.
[26] Wang M, Liu Y, Zhang P, Yang X, Zhou X, Li X and Huang C. Interaction of intercelular adhe-sion molecule-1 gene polym orphism s and other exposure factors on coronary heart dis-ease. Chin J Lab Med 2006; 29: 1123-1128. [27] Liu Z, Wei Y and Tan Z. Assocaition between
Intracellular Adhesion Molecule-1 K469E Poly-morphism and coronary heart disease in a Chi-nese Zhuang Population. Chin J Geriatr 2011; 30: 581-582.
[28] Li Y, Hang M, Zheng B, Liu B, Su M, Han Y and Wen J. Relationshio of Intracellular Adhesion Molecule-1 K469E Polymorphism and Coro-nary Heart Disease. Chin J Geriatr 2010; 30: 3494-3495.
[29] Mo H, Huang Y, Hong Y and Zhu H. Correlation of Intracellular Adhesion Molecule-1 K469E Polymorphism with Coronary Heart Disease. Journal of New Chinese Medicine 2009; 41: 25-28.
[30] Yusup A, Abla A, Ibrayim A. and Upur H. The Gene Polymorphism of A CE, eNOS, FVII and
ICAM-1 Genes in Uighur Patients with Coronary Heart Disease in Xinjiang. Sci Technol Revi 2009; 37: 76-81.
[31] Hayflick JS, Kilgannon P and Gallatin WM. The
intercellular adhesion molecule (ICAM) family of proteins. New members and novel func-tions. Immunol Res 1998; 17: 313-327. [32] Blankenberg S, Barbaux S and Tiret L.
Adhe-sion molecules and atherosclerosis. Athero-sclerosis 2003; 170: 191-203.
[33] Iiyama K, Hajra L, Iiyama M, Li H, DiChiara M, Medoff BD and Cybulsky MI. Patterns of vascu-lar cell adhesion molecule-1 and intercelluvascu-lar adhesion molecule-1 expression in rabbit and mouse atherosclerotic lesions and at sites pre-disposed to lesion formation. Circ Res 1999; 85: 199-207.
[34] Isogai N, Tanaka H and Asamura S. Thrombo-sis and altered expression of intercellular ad-hesion molecule-1 (ICAM-1) after avulsion in-jury in rat vessels. J Hand Surg Br 2004; 29: 230-234.
[35] Gho YS, Kim PN, Li HC, Elkin M and Kleinman HK. Stimulation of tumor growth by human soluble intercellular adhesion molecule-1. Cancer Res 2001; 61: 4253-4257.
[36] Hulok A, Sciborski K, Marczak J, Bankowski T, Poreba R and Negrusz-Kawecka M. Soluble Cell Adhesion Molecules - Does Estimating sV-CAM-1 and sIsV-CAM-1 Concentration Provide Ad-ditional Information About Cardiovascular Risk in Patients with Coronary Artery Disease? Adv Clin Exp Med 2014; 23: 735-741.
[37] Zou S, Pan X, Chen Z, Wei C, He B and Zhang H. Intercellular adhesion molecule-1 K469E poly-morphism and risk of coronary artery disease: a meta-analysis. Med Sci Monit 2014; 20: 2677-2682.
[38] Li D, Qu C and Dong P. The ICAM-1 K469E poly-morphism is associated with the risk of coro-nary artery disease: a meta-analysis. Coron Artery Dis 2014; 25: 665-670.
[39] Ji YN, Wang Q and Zhan P. Intercellular adhe-sion molecule 1 gene K469E polymorphism is associated with coronary heart disease risk: a meta-analysis involving 12 studies. Mol Biol Rep 2012; 39: 6043-6048.
[40] Yanyan L. Intercellular adhesion molecule-1 E469K gene polymorphism and coronary ar-tery disease in the Chinese population: a me-ta-analysis involving 3065 subjects. Clin Car-diol 2012; 35: 55-60.