Official Journal of
the Italian Society of Andrology
Journal of
ANDROLOGICAL
SCIENCES
ALIANE SP
A - Spedizione in Abbonamento Postale - D.L. 353/2003 conv
. in L. 27/02/2004 n° 46 art. 1, comma 1 DCB PISA
OBSTRUCTIVE AZOOSPERMIA GYNECOMASTIA CHLAMIDYA TRACHOMATIS INFECTION SURGERY OF PEYRONIE’S DISEASE NUTRACEUTICAL FOR ERECTILE DYSFUNCTION BILATERAL LEYDIG CELL TUMOR
IN THIS ISSUE
www.andrologiaitaliana.it
Vol. 17 t/P t December 2010 ORIGINAL ARTICLESCurrent techniques in management of obstructive azoospermia... 149 Gynecomastia: pathophysiology, clinical evaluation and management... 156 Chlamydia trachomatis infection: the urologist’s point of view ... 164 Peyronie’s disease: endocavernous plaque excision without substitutive graft:
critical 5-year experience ... 169 Corporoplasty with soft axial tutors and safenous grafting. Following three years... 171 Efficacy of a nutraceutical preparation as add-on treatment in patients with erectile dysfunction
treated with 5-PDE inhibitors: a pilot study... 178 CASE REPORT
Bilateral Leydig cell tumor with adrenal hyperplasia ... 183 TABLE OF CONTENTS... 186
CONTENTS
Vol. 17t/PtDecember2010 Journal of ANDROLOGIC AL SCIENCE SOfficial Journal of the Italian Society of
Androlog
y
Official Journal of the Italian Society of Andrology
Journal of
ANDROLOGICAL
SCIENCES
Past Editors Fabrizio Menchini Fabris (Pisa) 1994-2004 Edoardo Pescatori (Modena) Paolo Turchi (Pisa) 2005-2008 Vincenzo Ficarra (Padova) Andrea Salonia (Milano) Editor-in-Chief Ferdinando Fusco (Napoli) Managing Editor Furio Pirozzi Farina (Sassari)
Editorial Board Antonio Aversa (Roma) Ciro Basile Fasolo (Pisa)
Carlo Bettocchi (Bari) Guglielmo Bonanni (Padova) Massimo Capone (Gorizia) Tommaso Cai (Trento) Luca Carmignani (Milano) Antonio Casarico (Genova) Carlo Ceruti (Torino) Fulvio Colombo (Milano) Luigi Cormio (Foggia) Federico Dehò (Milano)
Giorgio Franco (Roma) Andrea Galosi (Ancona) Giulio Garaffa (London) Andrea Garolla (Padova) Paolo Gontero (Torino) Vincenzo Gulino (Roma) Massimo Iafrate (Padova) Sandro La Vignera (Catania) Francesco Lanzafame (Catania) Giovanni Liguori (Trieste) Mario Mancini (Milano) Alessandro Mofferdin (Modena) Nicola Mondaini (Firenze) Giacomo Novara (Padova) Enzo Palminteri (Arezzo) Furio Pirozzi Farina (Sassari) Giorgio Pomara (Pisa) Marco Rossato (Padova) Paolo Rossi (Pisa) Antonino Saccà (Milano) Gianfranco Savoca (Palermo) Omidreza Sedigh (Torino) Marcello Soli (Bologna) Paolo Verze (Napoli) Alessandro Zucchi (Perugia) Copyright 4*"44SMtWJB-VJHJ#FMMPUUJ#PO 3PNB Editorial Office -VDJB$BTUFMMJ &EJUPSJBM"TTJTUBOU 5FMt'BY MDBTUFMMJ!QBDJOJFEJUPSFJU 1BDJOJ&EJUPSF4Q"t7JB"(IFSBSEFTDB 1JTB*UBMZ Publisher 1BDJOJ&EJUPSF4Q" 7JB"(IFSBSEFTDB 1JTB*UBMZ 5FMt'BY *OGP!QBDJOJFEJUPSFJU XXXQBDJOJNFEJDJOBJU 17 t 2010
www.andrologiaitaliana.it
Cited in
INDEX
Original articles
Current techniques in management of obstructive azoospermia
G. Liguori, A. Zordani, R. Napoli, S. Bucci, M. Rizzo, S. Benvenuto, E. Belgrano, C. Trombetta ... 149 Gynecomastia: pathophysiology, clinical evaluation and management
M. Rossato, M. Sogaro, R. Vettor ... 156 Chlamydia trachomatis infection: the urologist’s point of view
T. Cai, S. Mazzoli, N. Mondaini, G. Malossini, R. Bartoletti ... 164 Peyronie’s disease: endocavernous plaque excision without substitutive graft: critical 5-year experience
F. Mantovani, E. Tondelli, G. Cozzi, I. Oliva, E. Finkelberg, M. Talso, D. Varisco, C. Palumbo, F. Rocco ... 169 Corporoplasty with soft axial tutors and safenous grafting. Following three years
M. Silvani, S. Pecoraro, A. Zucchi ... 171 Efficacy of a nutraceutical preparation as add-on treatment in patients with erectile dysfunction treated with 5-PDE inhibitors: a pilot study G. Piubello ... 178 case rePOrt
Bilateral Leydig cell tumor with adrenal hyperplasia
T. Zenico, M. Saccomani, U. Salomone, E. Bercovich ... 183 table Of cOntents ... 186
current techniques in management of obstructive
azoospermia
G. Liguori, A. Zordani, R. Napoli, S. Bucci, M. Rizzo, S. Benvenuto, E. Belgrano, C. Trombetta
Department of Urology, University of Trieste, Italy
Key words
Azoospermia • Techniques
Summary
Azoospermia is the total absence of spermatozoa in the ejaculate. Azoo-spermia is found in 10% to 15% of male infertility cases and is caused by a testicular insufficiency in the majority of patients. Obstructive azoospermia is less frequent and arises in 15-20% of men with azoospermia.
Most causes of male infertility are treatable, and many treatments restore the ability to father a children naturally.
In case of vasal or epididymal obstruction, microsurgical reconstruction of the seminal pathways, if possible, remains the safest and most cost-effective treatment option for these patients, allowing natural conception in many cases.
Not all men with obstructive azoospermia are tractable by microsurgical reconstruction. In such situations, various sperm-retrieval techniques can be employed to take sperm for use with in vitro fertilization via intracytoplasmic sperm injection.
introduction
Azoospermia is defined as the total absence of spermatozoa in the ejaculate. Azoospermia is found in 10% to 15% of male infertility cases and is caused by a testicular insufficiency in the majority of pa-tients. Obstructive azoospermia is less frequent and arises in 15-20% of men with azoospermia.
Common causes of obstructive azoospermia results most commonly from previous vasectomy, but also may be caused by epididymal, vassal, or ejaculatory duct pathology relating to genitourinary infec-tion, iatrogenic injury during scrotal or inguinal surgery, and congenital
anomalies 1.
Most causes of male infertility are treatable, and many treatments restore the ability to father a children naturally.
Men with obstructive azoospermia present with normal size testes and normal FSH. On examination, enlargement of the epididymis can be found and sometimes the vas deferens appears absent, due to congenital factors or previous inguinal or scrotal surgery. Although obstructions in primary infertile men are commonly present at the epididymal level, other sites of obstruction are the ejaculatory ducts and the vas deferens.
Corresponding author
In 25% of men with a suspected obstruction, no spermatozoa are found in the epididymis during scrotal exploration, indicating that there is an
intrat-esticular obstruction 2.
Moreover, clinical management of obstructive azoospermia must also take into account any con-comitant infertility factors in the female partner. As a result, both partners should be examined before making a specific treatment proposal.
treatment options for obstructive azoospermia
Men with obstructive azoospermia may father chil-dren in one of two ways:• surgical correction of the obstruction;
• retrieval of sperm directly from the epididymis or the testis followed by in vitro fertilization (IVF) or intracytoplasmatic sperm injection.
In case of vasal or epididymal obstruction, micro-surgical reconstruction of the seminal pathways, if possible, remains the safest and most cost-effective treatment option for these patients, allowing natural
conception in many cases 3-5. The surgical
manage-ment of OA depends on the site of obstruction: if obstruction is present at the level of the vas def-erens or epididymis microsurgery is indicated; on the contrary, ejaculatory duct obstruction is treated by transurethral resection of the ejaculatory ducts
(TURED) 2.
transurethral resection of the ejaculatory
ducts
Ejaculatory duct obstruction is suspected when the ejaculate volume is < 2.0 mL and no sperm or fruc-tose is present. Clinical suspicion can be confirmed by TRUS demonstration of dilated seminal vesicles or dilated ejaculatory ducts.
Transurethral resection of the ejaculatory ducts is performed cystoscopically. A small resectoscope and electrocautery loop are inserted, and the veru-montanum is resected in the midline. Since the area of resection is at the prostatic apex, near the external urethral sphincter and the rectum, careful positioning of the resectoscope is essential. There is convinc-ing evidence from several large studies of patients treated for infertility that 65-70% of men show sig-nificant improvement in semen quality after TURED and that a 20-30% pregnancy rate can be expected. The complication rate from TURED is approximately 20%. Most complications are self-limited and include hematospermia, hematuria, urinary tract infection,
epididymitis, and a watery ejaculate. Rarely reported
complications include retrograde ejaculation, rectal perforation, and urinary incontinence.
Microsurgical reconstruction of the vas
derfe-rens and epididymis
Microsurgical reconstruction to correct male in-fertility, although usually performed for vasectomy reversal, also is performed to correct other types of iatrogenic, congenital, and post inflammatory obstruction.
Microsurgical reconstruction of the seminal path-ways may be accomplished via anastomosis of the vasal ends (vasovasostomy) or anastomosis of the abdominal end of the vas deferens to the epididymis (vasoepididymostomy).
Before surgery, it is necessary for the surgeon to alert the cryobank laboratory personnel: as a matter of fact intraoperative retrieval of sperms from the vas, epididymis or testis is performed in order to cryopreserve sperm for possible later use for IVF/ ICSI in case of microsurgery failure.
Vasovasostomy or vasoepididymostomy?
Vasovasostomy almost always is performed for the reversal of an elective vasectomy (6% of men who undergo vasectomy ultimately request reversal), but, vasovasostomy is not always a feasible option to
re-store vasal patency; as a matter of fact if epididymal
obstruction is present, whether primary or secondary to chronic vasal obstruction, a vasoepididymostomy is required proximal to the obstruction to restore
continuity for sperm transport 6.
Every procedure begins with the careful dissection of the vas deferens with an intact sheath and me-ticulous preservation of the blood supply. Once the site of the previous vasectomy has been identified, the vas is transected perpendicularly on the abdomi-nal and testicular limbs as close as possible to the obstructed segment to preserve vasal length and the fluid is examined under a separate bench light microscope to determine whether vasovasostomy or vasoepididymostomy is indicated. If copious, clear, watery fluid is identified or if intact sperm or sperm parts are identified, then vasovasostomy is indicated.
Vasovasostomy
Vasovasostomy represents the simplest form of microsurgical reconstruction of the reproductive tract. The microsurgical anastomosis may be
per-formed with either a modified one-layer or a two-layer technique. The modified one-two-layer
anastomo-sis 7 is performed using six to eight interrupted full
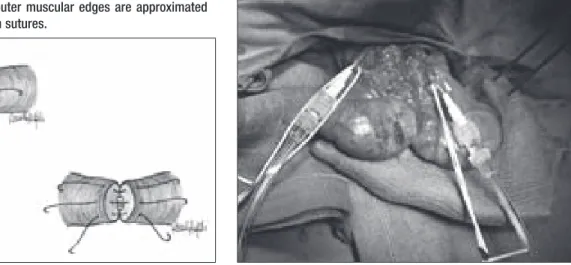
thickness sutures of 9-0 nylon placed equidistantly around the circumference of each end of the vas, followed by the placement of more superficial outer muscular layer sutures of 9-0 nylon between adja-cent full thickness sutures.
The two-layer end-to-side microsurgical
anastomo-sis 8 is performed by placing six to eight interrupted
sutures of 10-0 nylon through the mucosa of each end of the vas, followed by the placement of ap-proximately eight interrupted sutures of 9-0 nylon through the outer muscular layer of the vas (Fig. 1). A folding vas approximating clamp is useful to perform
this anastomosis 9.
The one-layer technique is performed in patients in whom there is little difference in the diameters of vas deferens between the distal and the proximal sides. Nevertheless, to simplify the surgical proce-dure and to shorten the duration of the operation, the one-layer technique might be sufficient for va-sectomy reversal. In vasovasostomy after hernior-rhaphy, when there used to be a large difference in the diameters of the vas deferens between the distal and the proximal sides because of the long duration of obstruction, the two-layer technique is required to ensure the precise attachment of the mucosa of the vas deferens. When compared with the fertility rate (42% to 50%) for the patients who underwent vasec-tomy reversal with duration < 10 years, the results for the patients who underwent vasectomy reversal with duration > 10 years after vasectomy showed
mark-edly poor results (37%) 10. Known inhibiting factors
of pregnancy after vasovasostomy include stricture and obstruction of the seminal tract at the
anasto-motic site; ruptured ductus epididymis caused by
occlusion or back pressure and secondary obstruc-tion of ruptured ductus epididymidis, and antisperm
antibodies have also been reported to play a role 11.
Vasoepididymostomy
This procedure is performed by creating vertical scrotal incisions that are adequately long to extrude the scrotal contents. Otherwise the testicles are ex-posed by means of an infrapubic incision according to Kelami.
The presence of active spermatogenesis is an obvi-ous prerequisite to this surgical procedure and, if a testis biopsy has not already been carried out before this surgery, it can be done in a standard fashion and the tissue examined under the microscope (400×) for the presence of sperm, some of which may be motile.
It is necessary to prove that the vasa are patent. For this reason a 27-gauge needle is inserted into the lumen of the vas, pointing away from the testicle (Fig. 2) and a vasography is carried out: a vasogram involves the injection of contrast media into the vas toward the bladder from the scrotum. Vasography can delineate the proximal vas deferens, seminal vesicle and ejaculatory duct anatomy and determine whether obstruction is present (Fig. 3).
The procedure begins by first freeing up the abdomi-nal limb of the vas deferens that will be used for the anastomosis. Mobilization of the vas with meticulous preservation of blood supply is necessary to create a tension-free anastomosis. For this purpouse the vas must be prepared to the level of the ring and drawed through an opening in the tunica vaginalis: Then the vas is brought to the epididymis in a straight-line
Figure 1. Inner mucosal edges are approximated with interrupted 10-0 nylon sutures and outer muscular edges are approximated with interrupted 9-0 nylon sutures.
Figure 2. A 27-gauge needle is inserted into the lumen of the vas, pointing away from the testicle and the contrast media is injected into the vas toward the bladder from the scrotum.
fashion and the posterior edge of the epididymal tunic is sewed to the posterior edge of the vasal muscularis with interrupted 9-0 nylon sutures in or-der to position the lumen of the vas adjacent to the
selected epididymal tubule 12.
The results of vasoepididymostomy are increasingly successful the lower the anastomosis is performed
in the epididymis 13. While it is important to perform
the anastomosis at the lowest possible epididymal level, the level must be at a point in the epididymis at which spermatozoa are present in the epididymal tubular fluid, which assures that the anastomosis will be performed above the obstruction in the
epididymis. Although vasovasostomy may have a successful result despite the intraoperative absence of spermatozoa from the vas fluid, vasoepididymos-tomy never will be successful when performed at an epididymal level at which spermatozoa are absent
from the epididymal tubular fluid 14.
Multiple anastomotic techniques have been de-scribed, although three variations are currently used: direct end, direct side, and
end-to-side intussusceptions 15.
Of all the modifications reported in literature, in-tussusception vasoepididymostomy anastomotic techniques have had the greatest impact on clini-cal practice and are now used widely by urologic microsurgeons.
Berger 16 first described the use of an invagination
va-soepididymostomy in clinical practice. He described a triangulation intussusception technique using three double-armed 10-0 nylon sutures, which would be equivalent to six luminal sutures. In a series of 12 men who underwent bilateral vasoepididymostomy with this technique, the patency rate was 92%.
Marmar 17 then described a two-suture
intussuscep-tions vasoepididymostomy technique that many regarded as another significant advance: the sutures were placed transversely in the epididymal tubule with a single, simultaneous needle placement. The Cornell group also has reported on a two-suture method. In their study, the sutures were placed
lon-gitudinally rather than transversely 18.
This maneuver then was followed by a tubulotomy cut between the sutures. After the epididymal fluid is tested for sperm and aspirated into micropipettes for cryopreservation, the two needles within the epididymal tubule are pulled through, and all four needles are placed through the vas lumen at the marked locations. Tying down the sutures allows the epididymal tubule to be intussuscepted into the vasal lumen, completing the anastomosis (Fig. 2). The patency rate with the longitudinal intussuscep-tion vasoepididymostomy approach was over 90% in a recent clinical series, and intussusception is the
preferred method for all vasoepididymostomies 19.
Sperm retrieval techniques
Not all men with obstructive azoospermia are trac-table by microsurgical reconstruction. In such situa-tions, various sperm-retrieval techniques can be em-ployed to take sperm for use with in vitro fertilization (IVF) via intracytoplasmic sperm injection (ICSI). For obstructive azoospermia, fertilization and pregnancy rates are comparable with those achieved with
Figure 3. Vasography delineates the proximal vas deferens, seminal vesicle and ejaculatory duct anatomy. In this case distal obstruction is not present.
Figure 4. Transversal two-suture intussusceptions vasoepididy-mostomy. The sutures were placed transversely in the epididymal tubule with a single, simultaneous needle placement 17.
ejaculated sperm. The results with frozen testicular sperm are comparable to those obtained with fresh testicular sperm.
Sperm retrieval with IVF/ICSI offers the possibility of early achievement of a relatively high live delivery rate, but any couple considering IVF/ICSI should be apprised of the risks involved in this type of treat-ment. These include the possibility of ovarian hy-perstimulation, the potential complications of oocyte retrieval and the risks and consequences of multiple
gestations 20.
In men with obstructive azoospermia, sperm may be retrieved from either the epididymis or the testis via a variety of percutaneous, open, or microsurgical techniques.
The microsurgical techniques may also be used con-comitantly with reconstructive procedures as a means to obtain sperm for cryopreservation in the event the attempt at reconstruction is not successful.
The obvious advantages of percutaneous acquisi-tion are the minimally invasive nature of this method and the ability to sample multiple sites within the testes with minimal potential of harm to the testis. The obvious disadvantage is that the area of tissue sampled is decreased markedly compared with the open biopsy.
Sperm retrieval techniques
According to the Practice Committee of Ameri-can Society for Reproductive Medicine Guidelines, since only 20% to 40% of couples conceive after attempted vasoepididymostomy despite patency rates of 60% to 80%, it is reasonable to consider sperm retrieval at the time of surgical
reconstruc-tion 21. If motile sperm are found at the site of
reconstruction, they may be aspirated and cryop-reserved. Alternatively, sperm may be retrieved via testicular biopsy.
The first successful attempt at ICSI using epididymal sperm (MESA or microsurgical epididymal sperm
aspiration) was reported by Silber 22 and Tournaye 23.
Many reports have shown that the cause of obstruc-tion is not important when considering the success rate with MESA. The MESA procedure is performed under general anaesthesia. After exposure a dilated tubule of the epididymis is microsurgically opened and its fluid examined for the presence of motile spermatozoa. The best quality sperm are typically found in the proximal epididymis close to the testis. Puncture sites may be closed or cauterized. Per-forming aspiration under direct vision with the aid of the operating microscope allows for procurement of
a large number of good quality, motile sperm from
the epididymal tubules 24.
An alternative method for epididymal aspiration of sperm is PESA (percutaneous epididymal sperm aspiration), being less invasive and less costly than MESA.
Epididymal aspiration also can be performed without surgical scrotal exploration, repeatedly, easily, and at low cost, without an operating microscope or exper-tise in microsurgery. PESA can be performed under local anesthesia. This technique is indicated in pa-tients with obstructive azoospermia who were unable to undergo or who decided against surgical recon-struction. A needle is introduced through the skin into the epididymis and is then aspirated (Fig. 6). Multiple punctures may be required to obtain sufficient fluid. However, the numbers of sperm retrieved are often not sufficient to allow for cryopreservation, so repeat procedures may be warranted for multiple IVF cycles. In addition, there is a risk for development of scrotal hematoma or injury to the epididymal or testicular vessels given the blind nature of this procedure. Despite the good results with MESA and PESA, many studies have shown that ICSI with testicular sperma-tozoa retrieved by TESE (testicular sperm extraction) could also be successfully applied in almost all cases of azoospermia. The most popular methods of sperm re-trieval are conventional “open biospy” rere-trieval (TESE), FNA (fine needle aspiration) or TESA (testicular sperm aspiration). In patients with normal spermatogenesis it
seems that FNA and TESE give comparable results 25.
Figure 5. Longitudinal 2-suture longitudinal end-to-side vasoepidi-dymostomy technique 18.
The choice of sperm retrieval method in men with obstructive azoospermia depends primarily on the experience and preference of both the physician who will perform the retrieval and the IVF laboratory embryologist. There are not enough data to conclude that either the technique of sperm retrieval (open or percutaneous) or the source of sperm (testicular, epididymal, vasal or seminal vesicular) significantly affects pregnancy rates.
Moreover, epididymal and testicular sperm could be frozen, stored and subsequently used in future ICSI cycles. For obstructive azoospermia, fertilization and pregnancy rates are comparable with those us-ing ejaculated spermatozoa, and results with frozen sperm are comparable to those obtained with fresh testicular sperm.
Cryopreservation of sperm is an essential technique in the treatment of infertile couples wherein the man has obstructive azoospermia. and, whenever avail-able, excess retrieved spermatozoa should be cryo-preserved to avoid unnecessary subsequent sperm
retrieval procedures 21.
The results achieved with retrieved sperm and ICSI are excellent. Contemporary pregnancy rates of 24% to 64% have been achieved using sperm
retrieved from azoospermic 26 27. Maternal factors
(maternal age, oocyte number, and oocyte quality) alone now are considered the principal determinants of outcomes achieved with ART and ICSI for couples
with infertility related to obstructive azoospermia 28.
conclusion
Microsurgical reconstruction should be offered to men having a reparable reproductive tract obstruc-tion and is preferable to sperm retrieval with IVF/
ICSI in men with prior vasectomy if the obstructive interval is less than 15 years and no female fertility risk factors are present. If an epididymal obstruction is present, the decision to use either microsurgi-cal reconstruction or sperm retrieval with IVF/ICSI should be individualized.
Vasoepididymostomy should be performed by an expert in reproductive microsurgery.
Sperm retrieval with ART is an alternative to micro-surgical repair for men with correctable reproductive tract obstruction and represents the only treatment that can offer men with irreparable obstruction the opportunity to have their own genetic children. Al-most all men with obstructive azoospermia have abundant sperm in the testes that can be retrieved successfully using a variety of different techniques. Sperm retrieval/ICSI is preferred to surgical treatment when (1) advanced female age is present (2) female factors requiring IVF are present (3) the chance for suc-cess with sperm retrieval/ICSI exceeds the chance for success with surgical treatment or (4) sperm retrieval/ ICSI is preferred by the couple for financial reasons.
references
1 Sheynkin YR, Hendin BN, Schlegel PN, et al.
Microsur-gical repair of iatrogenic injury to the vas deferens. J
Urol 1998;159:139-41.
2 Practice Committee of the American Society for
Re-productive Medicine. The management of infertility
due to obstructive azoospermia. Fertil Steril 2008;90
(Suppl 3):121-4.
3 Donovan JF Jr, Di Baise M, Sparks AE, et al.
Com-parison of microscopic epididymal sperm aspiration and intracytoplasmic sperm injection/in-vitro fertiliza-tion with repeat microscopic reconstrucfertiliza-tion following vasectomy: is second attempt vas reversal worth the
effort? Hum Reprod 1998;13:387-93.
4 Pavlovich CP, Schlegel PN. Fertility options after
vasectomy: a cost-effectiveness analysis. Fertil Steril
1997;67:133-41.
5 Kolettis PN, Thomas AJ. Vasoepididymostomy for
va-sectomy reversal: a critical assessment in the era of
intra-cytoplasmic sperm injection. J Urol 1997;158:467-70.
6 Goldstein M, Li PS, Matthews GJ. Microsurgical
vas-ovasostomy: the microdot technique of precision
su-ture placement. J Urol 1998;159:188-90.
7 Schmidt SS. Vasovasostomy. Urol Clin North Am
1978;5:585-92.
8 Belker AM. Microsurgical two-layer vasovasostomy.
Simplified technique using hinged,
folding-approximat-ing clamp. Urology 1980;16:376-81.
9 Belker AM, Thomas AJ Jr, Fuchs EF, et al. Results of
1,469 microsurgical vasectomy reversals by the
vas-ovasostomy Study Group. J Urol 1991;145:505-11.
10 Nagler HM, Jung H. Factors predicting successful
microsurgical vasectomy reversal. Urol Clin North Am
2009;36:383-90.
Figure 6. PESA: a needle is introduced through the skin into the epididymis and is then aspirated.
11 Royle MG, Parslow ]M, Kingscott MMB, et al. Reversal
of vasectomy: the effect of sperm antibodies on
subse-quent fertility. Br J Urol 1981;53:654-9.
12 Kolettis PN. Restructuring reconstructive
techniques--advances in reconstructive techniques. Urol Clin North
Am 2008;35:229-34.
13 Jarow JP, Oates RD, Buch JP. Epididymovasostomy
outcomes based upon level of anastomosis and
in-traepididymal sperm quality. Assisted Reprod Reviews
1997;7:179-83.
14 Niederberger C, Ross LS. Microsurgical
epidi-dymovasostomy: predictors of success. J Urol
1993;149:1364-7.
15 Lipshultz L, Homas A Jr, Khera M. Surgical
manage-ment of male infertility. In: Wein A, Kavoussi L, Novick
A, et al., editors. Campbell-Walsh Urology, vol. 1. 9th
edn. Philadelphia: Saunders Elsevier 2007.
16 Berger R. Triangulation end-to-side
vasoepididymos-tomy. J Urol 1998;159:1951-3.
17 Marmar JL. Modified vasoepididymostomy with
simul-taneous double needle placement, tubulotomy, and
tubular invagination. J Urol 2000;163:483-6.
18 Chan P, Li P, Goldstein M. Microsurgical
vasoe-pididymostomy: a prospective, randomized study
of three intussusceptions techniques in rats. J Urol
2003;169:1924-9.
19 Chan PT, Brandell RA, Goldstein M. Prospective
analy-sis of outcomes after microsurgical intussusception
vasoepididymostomy. BJU Int 2005;964:598-601.
20 Schlegel PN, Girardi SK. Clinical review 87: in vitro
fertilization for male factor infertility. J Clin Endocrinol
Metab 1997;82:709-16.
21 Practice Committee of American Society for
Re-productive Medicine. Sperm retrieval for obstructive
azoospermia. Fertil Steril 2008;90 (5 Suppl):S213-8.
22 Silber SJ, Nagy ZP, Liu J, et al. Conventional in-vitro
fertilization versus intracytoplasmic sperm injection for
patients requiring microsurgical sperm aspiration. Hum
Reprod 1994;9:1705-9.
23 Tournaye H, Devroey P, Liu J, et al.
Microsurgi-cal epididymal sperm aspiration and intracytoplasmic sperm injection: a new effective approach to infertility as a result of congenital bilateral absence of the vas
deferens. Fertil Steril 1994;61:1045-51.
24 Nudell DM, Conaghan J, Pedersen RA, et al. The
mini-micro-epididymal sperm aspiration for sperm
retrieval: a study of urological outcomes. Hum Reprod
1998;13:1260-5.
25 Tournaye H. Use of testicular spermfor the treatment
of male infertility. Baillieres Clin Obstet Gynaecol
1997;11:753-62.
26 Craft IL, Khalifa Y, Boulos A, et al. Factors influencing
the outcome of in vitro fertilization with percutaneous aspirated epididymal spermatozoa and
intracytoplas-mic sperm injection in azoosperintracytoplas-mic men. Hum Reprod
1995;10:1791-4.
27 Palermo GD, Schlegel PN, Hariprashad J, et al.
Fertil-ization and pregnancy outcome with intracytoplasmic
sperm injection for azoospermic men. Hum Reprod
1999;14:741-8.
28 Silber SJ, Nagy Z, Devroey P, et al. The effect of female
age and ovarian reserve on pregnancy rate in male in-fertility: treatment of azoospermia with sperm retrieval
and intracytoplasmic sperm injection. Hum Reprod
Corresponding author
Marco Rossato, University of Padova, Department of Medical and Surgical Sciences, Endocrine-Metabolic Unit, via Ospedale 105, 35128 Padova, Italy – Tel. +39 049 8218747 – Fax +39 049 8213332 – E-mail: [email protected]
gynecomastia: pathophysiology, clinical evaluation
and management
M. Rossato, M. Sogaro, R. Vettor
University of Padova, Department of Medical and Surgical Sciences, Clinica Medica 3-Endocrine-Metabolic Unit
Key words
Gynecomastia • Pathophysiology • Management • Estrogen • Androgen
Summary
Introduction. Gynecomastia is a common clinical condition characterized by an enlargement of the glandular tissue of the male breast, with a high preva-lence in young and old subjects. It is due generally to an absolute or relative increase of estrogens over androgens.
Methods. This article reviews the clinical management of gynecomastia, with particular attention to the causes and pathophysiological mechanisms leading to an absolute or relative excess of estrogens over androgens deter-mining gynecomastia. We face also a brief review of all medical and surgical therapies available to treat this condition that often troubles many patients above all in the pubertal age.
Results. Gynecomastia may be the result of an increased absolute estrogen production from estrogen secreting glands and/or to increased androgens conversion in the peripheral tissues or to a relative prevalence of estrogens over androgens. The efficacy of the management of gynecomastia depends on its causes and the time from its appearance due to possible time-depen-dent fibrotic modifications of breast tissue. For its treatment, depending on each specific cause, we can consider first the use of anti-estrogens. When pharmacological therapy shows no efficacy, surgery might be necessary.
Conclusions. Gynecomastia is a relatively common clinical condition. Usually a careful clinical history and physical examination are sufficient to identify the possible different causes ranging from pubertal gynecomastia, drug-induced causes, or an underlying pathological condition. Since gynecomastia often resolves spontaneously (as well as pubertal gynecomastia in a large part of pubertal boys), periodic clinical follow-up is usually sufficient to manage these patients. Nonetheless there are conditions where further clinical evaluation is necessary as well as medical or surgical treatment.
introduction
Gynecomastia is an enlargement of the glandular component of the
male breast due to ductular elements proliferation; it can be unilat -eral or bilat-eral. This condition has to be differentiated from excessive breast adipose tissue accumulation, a condition known as pseudogy-necomastia. Histologically, gynecomastia is characterized by the pro-liferation and dilatation of mammary ductules with periductal fibrocon-nective tissue. True terminal acini are rarely seen since acini require the
epidemiology
Gynecomastia is a common condition, being present on physical examination in 36% of healthy young men, 57% of healthy older men and in more than 70% of elderly hospitalized men (and as high as 85% in older men with a body mass index greater than 25
kg/m2) 4, while in autopsy studies, its prevalence
ranges from 40 to 55% 4-7. Typically, gynecomastia
has a trimodal age distribution during life:
1. neonatal: 60-90% of infants have transient gyne-comastia due to transplacentar transfer of
mater-nal estrogens;
2. puberty: 50-60% of adolescents have gyneco-mastia with a peak age of onset between 13 and
14 years, followed by a progressive decline;
3. adult: up to 70%, with the highest prevalence
between age 50-80 3 8.
Pathogenesis
The pathophysiological process of gynecomastia primarily involves an absolute or relative imbalance between estrogen and androgen action at breast
tissue level 9-11.
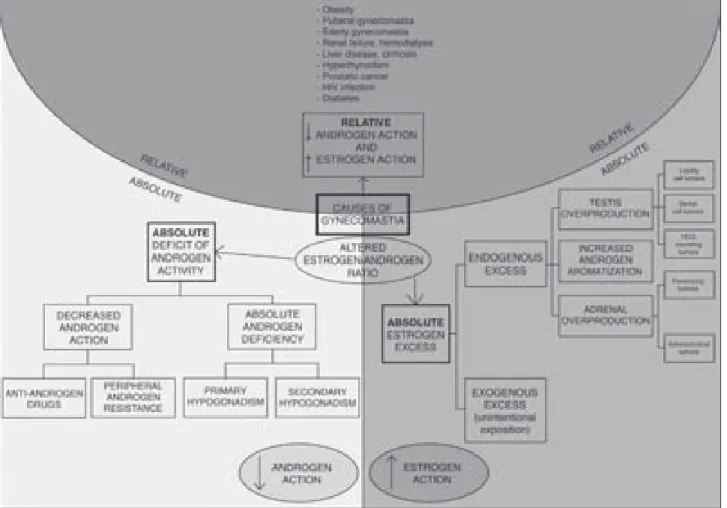
causes
The causes of gynecomastia can be distinguished in absolute estrogen excess, absolute androgen deficiency, relative estrogen excess/androgen defi-ciency, decreased androgen action.
An absolute estrogen excess directly stimulates the growth of male breast tissue, and may be due to endogenous estrogen overproduction as well as exogenous estrogen administration.
Endogenous estrogen overproduction can origin from the testis and from the adrenal gland, or from an increased androgen aromatization.
Testis
Leydig cell tumors. Leydig cell tumors are rare, representing the 3% of all testicular neoplasms. The natural history is usually benign, and malignant cases have been described in 10% of cases. They are generally seen in young adults, although they
can occur at any age 12. Leydig cell tumors directly
produce high estrogen levels, which cause a luteiniz-ing hormone (LH) suppression from the pituitary thus leading to a reduction in the testicular testosterone production. In this condition, there is an absolute estradiol overproduction by the tumor, a reduction of testicular testosterone production due to LH suppression, and a sex hormone-binding globulin
(SHBG) elevation due to estrogen stimulation, thus leading to a decrease in free testosterone concentra-tion. All these situations contribute to the increase of free estrogens/free androgens ratio.
Sertoli cell tumors. These tumors are very rare, and usually benign, occurring in boys and young men. These tumors do not directly secrete estrogens, but overexpress aromatase, the enzyme catalyzing the conversion of androgens to estrogens, thus leading to
increased androgen transformation to estrogens 13-15.
hCG secreting tumors. Human chorionic gonado-tropin (hCG) is very close to LH in its structure and action within the testis. Many germ cell tumors of the testis secrete hCG together with different tu-mors origining from other organs. hCG preferentially stimulates estradiol secretion from the testis, thus contributing to a relative or absolute systemic estro-gen excess.
Adrenal gland and increased androgen
aromatiza-tion
Feminizing tumors. This type of tumors are generally malignant, with a peak incidence in young and mid-dle-aged men. This cancer may secrete estrogens directly together with weak androgens (dehydroepi-androsterone – DHEA, androstenedione) that may be
aromatized into estrogens in peripheral tissues 16.
Increased aromatization to estrogens. Aromatase is present in adipose tissue, in the testis, bone, brain, muscle, hair follicles. Aromatase catalyzes the pe-ripheral aromatization of androgens in estrogens. All clinical conditions characterized by aromatase overexpression lead to increased aromatization of
androgens to estrogens (i.e. Thyreotossicosis) 17 18.
Exogenous estrogen exposure. Unintentional ex-posure to estrogens may occur by means of food (milk or meat from estrogen-treated cows), beer and
wine 19 20. However, these dietary estrogens are not
likely to be significant in men gynecomastia patho-genesis, unless we consider huge administration. Absolute androgen deficiency. Primary hypogonad-ism of any cause can result in gynecomastia. An absolute deficiency of testosterone contributes to a
relative estrogen excess 21 22.
Secondary hypogonadism: the lack of testicular stim-ulation by a deficient LH secretion by the pituitary leads to a reduction of testosterone secretion by the
testis, with relative estrogen excess; this relative es -trogen prevalence is further increased by the periph-eral aromatization of adrenal androgen precursors. Peripheral deficient androgen action. In partial and complete androgen insensitivity syndromes, de-fective androgen receptor function results in a
decreased androgen effect, thus leading to gyneco-mastia. The elevation of LH and follicle-stimulating hormone (FSH) due to the lack of inhibitory feedback at the pituitary leads to a further increase of estradiol synthesis, thus worsening gynecomastia.
Relative estrogen excess/androgen deficiency.There are many different causes of relative estrogen ex-cess, leading to an altered androgen/estrogen ratio as detailed in Figure 1.
Male breast cancer.Male breast cancer is rare, and usually gynecomastia does not increase the risk of future breast carcinoma development, excluding
patients affected by Klinefelter syndrome 23 24. The
clinical features suggestive of breast cancer in male are a hard asymmetric mass fixed to the skin and/ or underlying tissues, skin ulceration, axillary lymph-adenopathy or bloody nipple discharge. In the pres-ence of these features, breast biopsy is mandatory.
clinical evaluation
Gynecomastia requires a careful clinical history and an accurate physical examination.
A family history of gynecomastia has been reported in 58% of patients affected by pubertal
gynecomas-tia; history can also be helpful to reveal a causative
drug (Table I), or symptoms of hepatic, renal dys-function, testicular insufficiency, adrenal and thyroid hyperfunction.
Physical examination has to differentiate between true gynecomastia from fatty enlargement of the breast
without glandular proliferation (pseudogynecomastia);
if gynecomastia is present, the examination reveals a firm, tender and mobile mound of tissues, usually bilat-eral – unilatbilat-eral gynecomastia may actually represent
a step in the development of bilateral disease 5 11, but
it’s important to keep in mind that male breast cancer usually presents as unilateral –. The subareolar breast
tissue has to be at least 2 cm in diameter; this limit
was chosen to ensure the presence of gynecomastia, in fact if the tissue is smaller than that, gynecomastia can be considered not to be present. It is suggested to measure it as follows: with a finger at the superior in-ner quadrant and thumb at the inferior outer one, pick up a firm disc of breast tissue from the chest wall and
measure its diameter with a flexible rule 25-28.
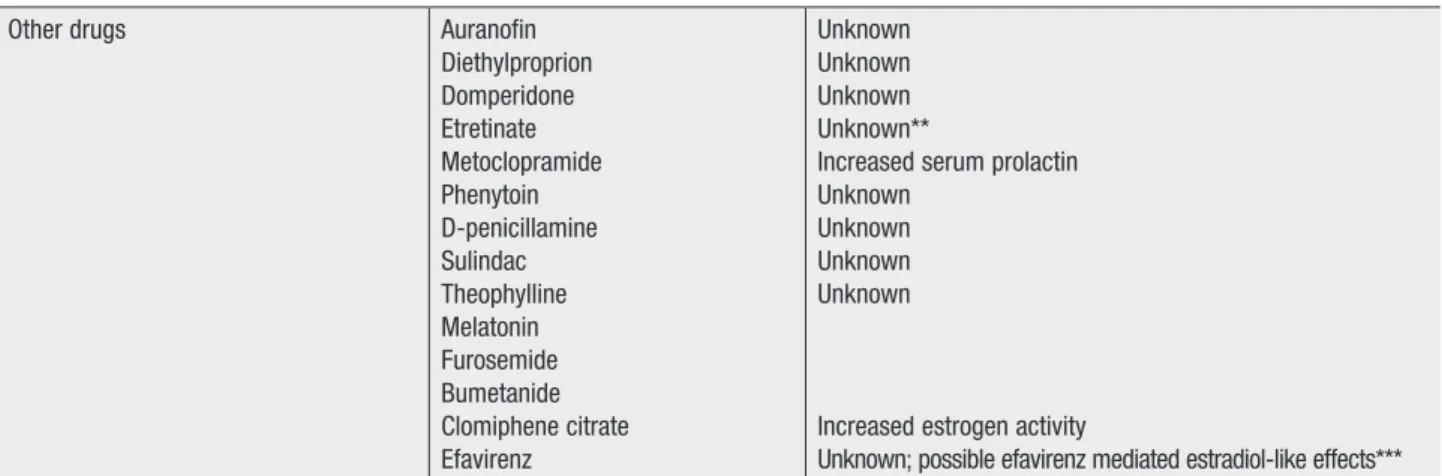
Table I. Drugs inducing gynecomastia and their pathophysiological mechanism of action.
Drug class Drug MechanisM
Antiandrogens/inhibitors of androgen synthesis
Cyproterone acetate Flutamide
Finasteride
AR blockade or inhibition of androgen synthesis Reduction of DHT biosynthesis Antibiotics Ethionamide Isoniazid Ketoconazole Metronidazole Unknown
Unknown; possible refeeding gynecomastia Decreased testosterone or DHT biosynthesis Antiulcer drugs Cimetidine
Ranitidine Omeprazole
AR blockade Unknown
Adverse reaction; possible estrogen activity; possible de-creased testosterone (induction of cytocrome metabolism*) Cancer chemotherapeutic drugs Alkylating agents
Methotrexate Vinca alkaloids Combination chemother Nitrosureas Imatinib Busulfan
Destruction or inhibition of Leydig cells
Cardiovascular drugs Amiodarone Enalapril Captopril Digitoxin Digitalis Amlodipine Diltiazem Verapamil Nifedipine Reserpine Spironolactone Methyldopa Unknown Unknown Estrogen-like activity Estrogen-like activity Unknown
Decreased testosterone or DHT biosynthesis AR blockade Unknown
Drugs of abuse Alcohol Amphetamines Heroin Marijuana Methadone
Increased aromatization of androgens to estrogens Unknown
Decreased testosterone biosynthesis AR blockade
Decreased testosterone biosynthesis
Hormones Androgens
Anabolic steroids Diethylstilbestrol
Human chorionic gonadotropin Estrogens and estrogen agonists Growth hormone
Medroxyprogesterone acetate Oral contraceptives
Increased aromatization of androgens to estrogens Exogenous estrogen
Stimulation of testicular estrogen secretion Increased estrogen activity
Unknown
Exogenous estrogens Exogenous estrogens Psychoactive drugs Diazepam
Haloperidol Paroxetine Phenothiazines Risperidone Tricyclic antidepressants Unknown
Increased serum prolactin Unknown
Gynecomastia can be classified in four grades with increasing severity, on the basis of physical
exami-nation 29:
• grade I: increase in diameter and protrusion lim
-ited to the areolar region; grade I can be mono -lateral or bi-lateral. There is no inframammary fold,
adipose tissue accumulation;
• grade II: hypertrophy of all breast components;
the areola-nipple complex is above the inframam-mary fold, independently from the maminframam-mary
vol-ume increase;
• grade III: hypertrophy of all breast components;
the areola-nipple complex is at the same height
as, or about 1 cm below the inframammary fold; • grade IV: hypertrophy of all breast components;
the areola-nipple complex is more than 1 cm below the inframammary fold. This grade is char-acterized by marked cutaneous ptosis.
The presence of testis cancer has to be excluded. An-thropometric measurements (body mass index – BMI) may also be helpful, because of the association of obesity and gynecomastia, due to an increased
pe-ripheral conversion of androgens 4. It is also important
to reveal signs and symptoms of hypogonadism, adre-nal and thyroid hyperfunction, liver or readre-nal disease.
Management
Gynecomastia is a benign, usually self-limiting con-dition. Most cases of pubertal gynecomastia usually
resolve in less than one year 30; if clinical work-up
does not reveal significant underlying pathologies, periodic follow-up is suggested. Obviously, each medical condition causing gynecomastia has to be investigated and, if present, treated. In particular, medications, recreational drugs or nutritional expo-sure causing gynecomastia should be withdrawn
if possible. For asymptomatic long-standing stable gynecomastia, no specific treatment is necessary. For symptomatic gynecomastia or if associated with psychological distress, pharmacological and/or sur-gical options have to be addressed (Fig. 2).
treatment
Medical treatment options are generally most effec-tive during the early, proliferaeffec-tive, aceffec-tive phase of gynecomastia. As gynecomastia is the result of a relative or absolute estrogen excess, medical therapy is aimed to block estrogen effects in the breast tissue or to decrease estrogen production, or to give andro-gens to counteract the effects of estroandro-gens. To this aim selective estrogen receptor modulators (SERMs)
appear to be very effective and fairly safe drugs 8.
Tamoxifen
Tamoxifen has been used for its anti-estrogenic activity, and is commonly used as an effective treat-ment of female breast cancer. In men with gyneco-mastia, tamoxifen is being used in doses of 10-20 mg/day for 3-9 months. Although few randomized double-blind placebo-controlled trials have limited a strong scientific evidence, resolution of gynecomas-tia has been reported in up to 90% of the treated men 31-34. If gynecomastia recurs on the medication withdrawing, a second attempt is suggested. Ta-moxifen is usually well-tolerated.
Raloxifene
Another member of the SERM family is raloxifene, a molecule closely related with tamoxifen and found to be effective in reducing mammary gland in boys presenting pubertal gynecomastia at the dose of 60
mg/once daily for 3 to 9 months 35.
Other drugs Auranofin
Diethylproprion Domperidone Etretinate Metoclopramide Phenytoin D-penicillamine Sulindac Theophylline Melatonin Furosemide Bumetanide Clomiphene citrate Efavirenz Unknown Unknown Unknown Unknown**
Increased serum prolactin Unknown
Unknown Unknown Unknown
Increased estrogen activity
Unknown; possible efavirenz mediated estradiol-like effects*** AR: androgen receptor; * Rosenshein et al., 2004; ** Carmichael et al., 2004; *** Jover et al., 2004.
Clomiphene
Clomiphene is another molecule used for its anti-es-trogenic activity that has been used in the treatment of gynecomastia but the results obtained (at the dose of 50 mg/once daily for 1 to 3 months) have not been so satisfying as those obtained with tamoxifen
and raloxifene 36.
Another class of drugs that has been used in the treat-ment of gynecomastia is that of aromatase inhibitors.
Testolactone
Testolactone, an old aromatase inhibitor, has been reported to be effective in the treatment of gyneco-mastia (450 mg/daily for 2 to 6 months), although
with lower efficacy than tamoxifen 37.
Anastrazole
Anastrazole, a relatively novel aromatase inhibitor, has been used to treat gynecomastia (1 mg/daily for 6 to 11 months) but with low efficacy compared with
tamoxifen 38 39.
Androgens
Androgens have been used to reduce the
gonado-tropins secretion and to increase the androgen-estrogen ratio. Testosterone is an obvious treat-ment possibly leading to the resolution of gyne-comastia in male hypogonadism, but since it can be aromatized to estradiol, testosterone treatment may also lead to worsening of gynecomastia in
some men. To this regard, dihydrotestosterone,
a non-aromatizable androgen, has been used to treat gynecomastia as local topical application, and it has been shown to be effective in some
forms of gynecomastia 40.
In previous years, danazole, an androgen with weak activity, has also been used (400 mg/daily) to reduce gonadotropin secretion and thus testicular estradiol production with some effect in the reduction of
gy-necomastia 41.
Radiotherapy
Radiotherapy directed at the mammary gland has been previously utilized to prevent gynecomastia in men with prostate cancer, and in pubertal boys with gynecomastia, but in this case the long-term risk of breast cancer due to radiation exposure is a
signifi-cant concern limiting its use 42.
Surgery
If gynecomastia has been present for more than one year, fibrotic tissue replaces the glandular tissue component, and thus it is unlikely its regression ei-ther spontaneously or with pharmacological ei-therapy. In such circumstances, surgical mastectomy or US-assisted liposuction and suction-US-assisted lipectomy
are the best cosmetic options 43-45.
conclusions
Gynecomastia is a relatively common clinical condi-tion. Usually a careful clinical history and physical examination are sufficient to identify the possible dif-ferent causes ranging from pubertal gynecomastia, drug-induced causes, or an underlying pathological condition. The likelihood of discovering a patho-logical condition is low in patients with long stand-ing asymptomatic gynecomastia. Since often these situations resolve spontaneously (as well as pubertal gynecomastia in a large part of pubertal boys), peri-odic clinical follow-up is usually sufficient to manage these patients. Other conditions resolve promptly after suspension of a drug causing gynecomastia. In adults showing acute onset of gynecomastia without an reliable cause, hormonal evaluation (hCG, testosterone, LH and estradiol plasma levels) should be performed to rule out pathological potentially harmful conditions that have to be treated.
Pharmacological treatment with anti-estrogens (ta-moxifen as detailed previously) may be suggested. If the gynecomastia has not regressed by 12 months, or in patients suffering with long-standing gynecomastia who are psychologically embarassed by their physical appearance, pharmacological treatment is not advis-able given its possible inefficacy due to fibrotic tissue proliferation within the breast. Thus surgical removal of the mammary gland and subareolar fat is an option that has quite good cosmetic and psychological result in the large part of patients. Mammography and breast biopsy are necessary if gynecomastia is of recent rapid appearance, unilateral, firm, irregular and associ-ated to mastodynia and skin retraction.
For patients who are completely asymptomatic, that are not troubled by their gynecomastia, and do not have a significant history or physical examination, no further clinical evaluation nor pharmacological treat-ment is advisable other than weight reduction.
Acknowledgments
The Authors wish to thank Francesco Tresca for his help in the preparation of figures.
references
1 Braunstein GD. Gynecomastia. N Engl J Med
2007;357:1229-37.
2 Narula HS, Carlson HE. Gynecomastia. Endocrinol
Me-tab Clin N Am 2007;36:497-519.
3 Gikas P, Mokbel K. Management of gynaecomastia: an
update. Int J Clin Pract 2007;61:1209-15.
4 Niewoehner CB, Nuttall FQ. Gynecomastia in an
hospi-talized male population. Am J Med 1984; 77:633-8.
5 Andersen JA, Gram JB. Male breast at autopsy.
Acta Pathol Microbiol Immunol Scand (Sect A)
1982;90:191-7.
6 Williams MJ. Gynecomastia: its incidence, recognition
and host characterization in 447 autopsy cases. Am J
Med 1963;34:103-12.
7 Nuttall FQ. Gynecomastia as a physical finding in
nor-mal men. J Clin Endocrinol Metab 1979;48:338-40.
8 Johnson RE, Murad MH. Gynecomastia:
pathophysi-ology, evaluation, and management. Mayo Clin Proc
2009;84:1010-5.
9 Marthur R, Braunstein GD. Gynecomastia:
path-omechanisms and treatment strategies. Horm Res
1997;48:95-102.
10 Rochefort H, Garcia M. The estrogenic and
antiestro-genic activities of androgens in female target tissues.
Pharmacol Ther 1983;23:193-216.
11 Wilson JD, Aiman J, MacDonald PC. The pathogenesis
of gynaecomastia. Adv Intern Med 1980;25:1-32.
12 Rossato M, Tavolini IM, Calcagno A, et al. The novel
hormone INSL3 is expressed in human testicular Ley-dig cell tumors: a clinical and immunohistochemical
study. Urol Oncol 2008;29:33-7.
13 Gabrilove JL, Nicolis GL, Mitty HA, Sohval AR.
Femi-nizing interstitial cell tumor of the testis; personal
observations and a review of the literature. Cancer
1975;35:1184-202.
14 Bercovici JP, Nahoul K, Tater D, et al. Hormonal prolife
of Leydig cell tumors with gynecomastia. J Clin
Endo-crinol Metab 1984;59:625-30.
15 Young S, Gooneratne S, Straus FH, et al. Feminizing
Sertoli cell tumors in boys with Peutz-Jeghers
syn-drome. Am J Surg Pathol 1995;19:50-8.
16 Gabrilove JL, Sharma DC, Wotiz HH, et al.
Feminiz-ing adrenal cortical tumors in the male: a review of 52
cases including a case report. Medicine
1965;44:37-79.
17 Bulun SE, Fang JZ, Gurates B, et al. Aromatase in
health and disease. Endocrinologist 2003;13:269-76.
18 Braunstein GD. Aromatase and gynecomastia.
Endocr-Relat Cancer 1999;6:315-24.
19 Daxenberger A, Ibarreta D, Meyer HH. Possible health
impact of animal oestrogens in food. Hum Reprod
Up-date 2001; 7:340-55.
20 Gavaler JS, Rosenblum ER, Deal SR, et al. The
phy-toestrogen congeners of alcoholic beverages: current
status. Proc Soc Exp Biol Med 1995;208:98-102.
21 Smyth CM, Bremner WJ. Klinefelter syndrome. Arch
Intern Med 1998;158:1309-14.
22 Lanfranco F, Kamischke A, Zitzmann M, et al.
23 Fentiman IS, Fourquet A, Hortobagyi GN. Male breast
cancer. Lancet 2006;367:595-604.
24 Swerdlow AJ, Schoemaker MJ, Higgins CD, et al.; UK
Clinical Cytogenetics Group. Cancer incidence and mortality in men with Klinefelter syndrome: a cohort
study. J Natl Cancer Inst 2005;97:1204-10.
25 Georgiadis E, Papandreou L, Evangelopoulou C, et al.
Incidence of gynecomastia in 954 young males and
its relationship to somatometric parameters. Ann Hum
Biol 1994; 21:579-87.
26 Cavanaugh J, Niewoehner CB, Nuttall FQ.
Gyne-comastia and cirrhosis of the liver. Arch Intern Med
1990;150:563-65.
27 Hudson B, Burger HG, De Krester DM. Virility and
fertility. In: Shearman RP, editor. Clinical Reproductive
Endocrinology. Edinburgh, United kingdom: Churchill
Livingston 1985; pp. 58-60.
28 Ersoz H, Onde ME, Terekeci H, et al. Causes of
gynecomastia in young adult males and factors
as-sociated with idiopathic gynecomastia. Int J Androl
2002;25:312-6.
29 Cordova A, Moschella F. Algorithm for clinical
evalu-ation and surgical treatment of gynecomastia. J Plast
Reconstruct Aesthet Surg 2008;61:41-9.
30 Biro FM, Lucky AW, Huster GA, et al. Hormonal studies
and physical maturation in adolescent gynecomastia. J
Pediatr 1990;116:450-5.
31 Treves N. Gynecomastia: the origins of mammary
swelling in the male: an analysis of 406 patients with breast ipertrophy, 525 with testicular tumors, and 13
with adrenal neoplasms. Cancer 1958;11:1083-102.
32 Gruntmanis U, Braunstein GD. Treatment of
gyneco-mastia. Curr Opin Investig Drugs 2001;2:643-9.
33 Ting ACW, Chow LWC, Leung YF. Comparison of
ta-moxifen with danazol in the management of idiopathic
gynecomastia. Am Surg 2000;66:38-40.
34 Khan HN, Rampaul R, Blamey RW. Management of
physiological gynecomastia with tamoxifen. Breast
2004;13:615.
35 Lawrence SE, Faught KA, Vethamuthu J, et al.
Benefi-cial effects of raloxifene and tamoxifen in the treatment
of pubertal gynecomastia. J Pediatr 2004;145:71-6.
36 Plourde PV, Kulin HE, Santner SJ. Clomiphene in the
treatment of adolescent gynecomastia. Clinical and
endocrine studies. Am J Dis Child 1983;137:1080-2.
37 Braunstein GD. Aromatase and gynecomastia. Endocr
Relat Cancer 1999; 6:315-24.
38 Boccardo F, Rubagotti A, Battaglia M, et al.
Evalu-ation of tamoxifen and anastrazole in the prevention of ginecomastia and breast pain induced by
bicalut-amide monotherapy of prostate cancer. J Clin Oncol
2005;23:808-15.
39 Plourde PV, Reiter EO, Jou HC, et al. Safety and
effica-cy of anastrazole for the treatment of pubertal gyneco-mastia: a randomized, double-blind, placebo-controlled
trial. J Clin Endocrinol Metab 2004;89:4428-33.
40 Benveniste O, Simon A, Herson S. Successful
percuta-neous dyhidrotestosterone treatment of ginecomastia occurring during highly active antiretroviral therapy:
four cases and a review of the literature. Clin Infect Dis
2001;33:891-3.
41 Ting AC, Chow LW, Leung YF. Comparison of
tamox-ifen with danazol in the management of idiopathic
gynecomastia. Am Surg 2000;66:38-40.
42 Dicker AP. The safety and tolerability of low-dose
irradiation for the management of gynecomastia
caused by antiandrogen monotherapy. Lancet Oncol
2003;4:30-6.
43 Rohrich RJ, Ha RY, Kenkel JM, et al. Classification
and management of gynecomastia: defining the role of
ultrasound-assisted liposuction. Plast Reconstr Surg
2003;111:909-23.
44 Tashkandi M, Al-Qattan MM, Hassanain JM, et al. The
surgical management of high-grade gynecomastia. Ann
Plast Surg 2004;53:17-20.
45 Hines SL, Tan WW, Yasrebi M, et al. The role of
mam-mography in male patients with breast symptoms.
Corresponding author
Tommaso Cai, Department of Urology, Santa Chiara Hospital, Largo Medaglie d’Oro 9, Trento, Italy – Tel. +39 0461 903306 – Fax +39 0461 903101 – E-mail: ktommy@ libero.it
Chlamydia trachomatis infection:
the urologist’s point of view
T. Cai1, S. Mazzoli2, N. Mondaini3, G. Malossini1, R. Bartoletti3
1 Department of Urology, Santa Chiara Hospital, Trento; 2 Sexually Transmitted Disease Centre, Santa Maria Annun-ziata Hospital, Florence; 3 Department of Urology, University of Florence
Key words
Chlamydia trachomatis • Prostatitis • Sexu-ally transmitted diseases • Infection • Qui-nolones • Sexually active young men
Summary
The role of Chlamydia trachomatis in everyday clinical practice is now on the increase because Chlamydia trachomatis infections are the most prevalent sexually transmitted bacterial infections worldwide. Chlamydia trachomatis
can cause urethritis, cervicitis, pharyngitis, or epididymitis, although as-ymptomatic infections are quite common. Chlamydia trachomatis infection remains asymptomatic in approximately 50% of infected men and 70% of infected women, with risk for reproductive tract sequelae both in women and men. A proper early diagnosis and treatment is essential in order to prevent persistent consequences. An accurate comprehension of the pathology, diagnosis and treatment of this entity is essential for the urologist. We review the literature about the new findings in diagnosis and treatment of Chlamydia trachomatis infection in sexually active young men.
introduction
Sexually transmitted diseases (STDs) are among the first ten causes of unpleasant diseases in young adult males in developing countries and the second major cause of unpleasant diseases in young adult
wom-en, with an enormous health and economic consequences 1. Among
these, Chlamydia trachomatis (Ct) is the most common sexually
trans-mitted bacterium worldwide 2 with over three million new infections per
year3. In particular, Chlamydia is the most frequently reported sexually
transmitted infection in Europe and the number of cases is steadily increasing, with more than 255,000 cases in people below 25 years
of age 4. Ct infection could remain asymptomatic in about 70% of
cases 5-6. Ct infection long-term effects include ectopic pregnancy and
tubal inflammation with subsequent infertility 6-7. Absence of
symp-toms increases the risk of infecting sexual partners and may cause long-term complications in men too, such as poor quality of semen
and infertility 5 7. Several factors contribute to make difficult
detect-ing Ct by a conventional analysis 8. To date, the DNA recombination
techniques are universally accepted as the “gold standard” to
evalu-ate the presence of Ct in biologic samples 9. However, immunologic
cytokines have been detected in total ejaculate and seminal plasma samples to demonstrate their role in
monitoring men with CP 10-11. Moreover, the proper
treatment of urological Ct infection is not totally indi-cated. For these reasons, Ct represents a challenge for the urologist both for diagnostic and treatment. We summarize the most current developments in the diagnostics and therapeutic approaches in Ct infec-tions in sexually active young men.
Materials and methods
We conducted a search of the English-language literature from 1960 through December 2010 with use of the Medline computerized database of the US National Library of Medicine (http://www.ncbi.nlm. nih.gov/pubmed). The Medline search have been divided into two sections: diagnosis and therapy. The first review section about diagnosis has been carried-out by using the following Medical Subject Headings and free text terms: “Chlamydia tracho-matis”, and “Chlamydia infections” (exploded) were combined with the terms “diagnosis”, “urine”, “ure-thral swab”, “total ejaculate”, “serum”, “antibodies, “prostate massage” and then limited to humans, male and young adult: 19-24 years. The second review section about therapy has been carried-out by using the following Medical Subject Headings and free text terms: “Chlamydia trachomatis”, and “Chlamydia infections” (exploded) were combined with the terms “treatment”, “therapy”, “antibiotic”, “drug”, “quinolones”, “tetracycline” and then lim-ited to humans, male and young adult: 19-24 years. Moreover, we searched reference lists of articles to identify potential additional references. All original paper and review studies of Ct diagnosis and treat-ment in young adult have been considered for this review. We considered also guidelines from the National Institute for Health and Clinical Excellence and the European Centre for Disease Prevention and Control, the US Centers for Disease Control and Prevention, and World Health Organization.
results
Ct diagnosis
From an initial literature search with 188 unique citations, a total of 27 articles were selected for the present review. A matched research between “Chlamydia trachomatis” and “Chlamydia infections” (exploded) and the following terms “total ejaculated” and “prostate massage” has not found any items.
Diagnosis of Ct infection can be made by using:
• direct detection; • indirect detection.
Direct detection
Ct is an obligate intracellular bacterium and cell culture remains a reference method (about 100%
specificity) 13. However, all Authors are agree that
it is not recommended for routine use, due to its lack of sensitivity, its technical complexity and the
long turn-around time 14. Other Authors suggest that
Ct can be found by using antigen-based detection
methods 13. In particular, direct fluorescent
stain-ing with monoclonal antibodies (DFA) and enzyme immunoassay (EIA). EIA tests are more reproduc-ible than DFA, and the sensitivity of the best EIA is comparable to that of culture but lower than that of nucleic acid amplification tests (NAATs), due to the cross-reactions with the lipopolysaccharide (LPS) of
other microorganisms 13. Recently, Mahilum-Tapay
and co-workers, evaluated the performance of the Chlamydia Rapid Test, a new assay developed at the Diagnostics Development Unit, University of
Cambridge 15. They compared sensitivity, specificity,
positive predictive value, and negative predictive
value of the Chlamydia Rapid Test with the gold
standard test for Ct infections (NAATs) 15. In this
study, they found a good diagnostic performance: sensitivity 83.5%, specificity 98.9%, positive pre-dictive value 86.7%, and negative prepre-dictive value
98.6% 15. However, NAATs are the tests of choice
for the diagnosis of Ct genital infections 13. In
every-day clinical practice, several commercial NAATs are available, and make use of different technologies: PCR and real-time PCR (Roche Diagnostics, Abbott,
IL, USA); strand displacement amplification (Becton Dickinson, NJ, USA); transcription-mediated ampli
-fication (Gen Probe); and nucleic acid
sequence-based amplification (bioMerieux, Nancy L’Etoile,
France) 13 16. These assays are automated and can
be used for screening programmes and for the de-tection of Ct and Neisseria gonorrhoeae in the same
specimen 13. We currently used Roche COBAS
AM-PLICOR CT/NG reagents kits and instruments (Ro-che Molecular Systems,Branchburg, NJ) with good
level of accuracy 8. NAATs tests generally show two
important drawbacks: the cost and the presence of inhibitors in specimens. However, they show a
high specificity 13. Finally, in 2006, a new C.
tracho-matis variant belonging to serovar E, with a 377-bp deletion in the cryptic plasmid, was described in
Sweden 17. This new variant can obviously not be
area, but can be detected by amplification targeting
a chromosomal gene, e.g. ompA or a rRNA gene 17.
However, new versions of the COBAS Taqman v2.0 test and of the Abbott test allow simultaneous detection of the cryptic plasmid and of ompA, and simultaneous detection of two different regions of
the cryptic plasmid, respectively 17.
Indirect detection
A recent review by Persson suggested that serol-ogy is useful only in some cases of Ct infection
and in seroepidemiological studies 18. On the other
hand, recent evidences showed that anti-Ct immu-noglobulin A (IgA) in association with interleukin 8 (IL-8) evaluation appear to be the best immunologic
markers of chronic chlamydial prostatitis status 8.
Mazzoli and co-workers, highlighted, in 78 consecu-tive patients with a diagnosis of chronic prostatitis due to Ct infection by IPAzyme Chlamydia IgG/IgA by Savyon Diagnostics (Ashdod, Israel), an immune-peroxidase test, the role of immune system activa-tion in the pathophysiology of chronic prostatitis due to Ct infection and that seminal IL-8 and mucosal IgA levels specific to Ct antigens appear to be the best immunologic markers of chronic chlamydial
prostatitis status 8. They, however, did not showed
any role of serum anti-Ct immunoglobulin in Ct
infec-tion diagnosis 8.
Chlamydia trachomatis therapy
From an initial literature search with 164 unique citations, a total of 18 articles were selected for the present review. A matched research between “Chlamydia trachomatis” and “Chlamydia infections” (exploded) and the following terms “quinolones” has not found any items.
A recent review by suggested that antimicrobial groups effective agains