Report Title Here
Report Subtitle Here
Date
Michigan Birth
Defect Registry
Implementation Guide for Ambulatory
Healthcare Provider Reporting to Central
Birth Defect Registries, HL7 Clinical
Version 1.2
G. Copeland, R. Humphrys, R. Kommareddi, R. May-Gentile, L. Rappleye, L. Simmons
Michigan Birth
Defect Registry
Implementation Guide for Ambulatory
Healthcare Provider Reporting to Central Birth
Defect Registries, HL7 Clinical Document
Architecture (CDA)
August, 2015
Table of Contents
Table of Contents ... i
List of Figures ... iv
List of Tables ... v
Preface ...x
1.0
Introduction ... 1
1.1
Background ... 1
1.2
Legal Mandate for Michigan Birth Defects Reporting ... 2
1.2.1
Public Health Code as Amended ... 2
1.2.2
Data ... 2
1.2.3
Rules ... 2
1.3
Purpose... 3
1.4
Audience ... 3
1.5
Scope ... 3
1.6
Use Case, Scenarios, Diagrams ... 3
1.6.1
Scenario ... 3
1.6.2
Use Case Overview ... 4
1.7
Use of Vocabulary Standards... 7
1.8
HIPAA ... 7
1.9
Clinical Document Architecture Release 2 (CDA R2) ... 7
2.0
Ambulatory Healthcare Provider Birth Defects Report ... 9
2.1
Document Constraints ... 9
2.2
Parent Template ... 10
2.3
Specification ... 10
2.4
Birth Defects Header ... 10
2.5
Conventions Used in this Guide ... 11
2.5.1
Conformance (Optionality Constraints) ... 11
2.7
Null Flavor ... 12
2.8
Birth Defects Specification Table ... 13
2.9
Organization of Implementation Guide ... 21
2.9.1
Conventions ... 21
2.9.2
Document Content Module ... 21
2.9.3
Sections ... 21
2.9.4
Entry Content ... 21
2.9.5
Vocabulary and Value Sets ... 21
2.10
Vocabulary Conformance ... 21
2.11
CDA Header Section Value Sets ... 22
2.11.1
Marital Status ... 22
2.11.2
Religious Affiliation ... 22
2.11.3
Race ... 24
2.11.4
Ethinicity ... 44
2.11.5
Personal Relation Role Type ... 44
2.11.6
Guardian ... 47
3.0
Document Level Templates ... 48
3.1
U.S. Realm Header ... 48
3.2
CDA Header Content Modules ... 49
3.3
Participants in Birth Defects Header ... 50
3.3.1
Record Target ... 50
3.3.2
Patient ... 51
3.3.3
Patient Contacts ... 52
3.3.4
Information Recipient ... 52
3.3.5
Address Constraints ... 53
3.3.6
Multiple Races ... 54
3.3.7
Provider Referred From ... 54
3.3.8
Birthplace ... 55
4.0
Section Level Templates ... 56
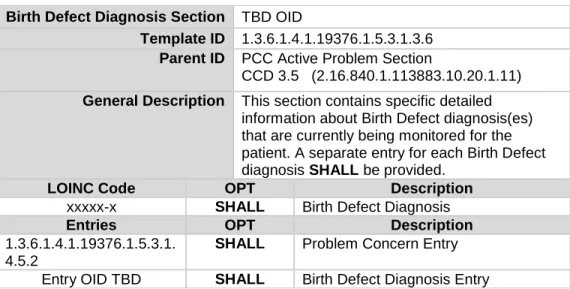
4.1
Birth Defect Diagnosis Section ... 56
4.1.1
Birth Defect Diagnosis Entry ... 57
4.2
Coded Results Section ... 61
4.2.1
Simple Observation Constraints Overview ... 62
4.3
Payers Section ... 64
4.3.1
Payer Type Vocabularies ... 65
4.3.3
Payor Role Code Names ... 66
4.4
Cytogenetics Section ... 66
4.4.1
Genetic Testing Report ... 66
4.4.2
Clinical Genomic Statement Cytogenetics ... 67
4.4.3
Associated Observation Cells Analyzed Count ... 70
4.4.4
Associated Observation Cells Count ... 70
4.4.5
Associated Observation Cells Karyotyped Count ... 70
4.4.6
Associated Observation Colonies Count ... 71
4.4.7
Associated Observation International System for Human Cytogenetic
Nomenclature (ISCN) Band Level... 71
4.4.8
Chromosome Analysis Overall Interpretation ... 73
4.5
Labor and Delivery History and Physical ... 73
4.5.1
Pregnancy History Section ... 74
4.5.2
Social History Section ... 101
4.6
Labor and Delivery Events Section ... 103
4.6.1
Coded Detailed Physical Examination... 105
4.6.2
Procedures and Interventions ... 106
4.6.3
Coded Event Outcomes ... 134
4.6.4
Medications Administered ... 153
4.7
Newborn Delivery ... 167
4.7.1
Newborn Delivery Information Section... 167
4.7.2
Coded Detailed Physical Examination Section ... 169
4.7.3
Active Problems ... 175
4.7.4
Procedures and Interventions ... 179
4.7.5
Medications Administered ... 186
4.7.6
Coded Event Outcomes ... 192
4.8
Care Plan Section ... 200
4.9
Disposition Section ... 204
Appendix A – Reportable Birth Defect Conditions ... 1
Appendix B – Value Sets ... 4
Appendix C – Data Element and CDA Element Relationship Table ... 119
List of Figures
Figure 1-1: Birth Defect Sequence Diagram ... 6
Figure 2-1: Birth Defects Header - Subject Type Code ... 10
Figure 2-2: Birth Defect Header – Participant Code Type ... 11
Figure 2-3: nullFlavor Examples ... 12
Figure 2-4: nullFlavor attribute required Example ... 13
Figure 2-5: Allowed nullFlavors when element is required example ... 13
Figure 2-6: nullFlavor explicitly disallowed example ... 13
Figure 2-7: Ambulatory Healthcare Provider Birth Defect Event Report Document Example ... 19
Figure 3-1: Example of a US Realm Header ... 49
Figure 3-2: Patient Contacts Example ... 52
Figure 3-3: Information Recipient Example ... 53
Figure 3-4: Address Example ... 54
Figure 3-5: sdtc:raceCode Example ... 54
Figure 3-6: Provider Referred From Example ... 55
Figure 3-7: Birthplace Example ... 55
Figure 4-1: Birth Defects Diagnosis Section Example ... 57
Figure 4-2: Birth Defects Diagnosis Template Example ... 60
Figure 4-3: Coded Results Section Example ... 61
Figure 4-4: Figure Simple Observation Example ... 64
Figure 4-5: Payers Section Example ... 65
Figure 4-6: Genetic Testing Report Example ... 67
Figure 4-7: Clinical Genomic Example ... 68
Figure 4-8: History of Pregnancies Example ... 75
Figure 4-9: Coded Social History Section Example ... 101
Figure 4-10: Labor and Delivery Events Section Example ... 104
Figure 4-11: Newborn Delivery Section Example ... 168
Figure 4-12: Active Problems Section Example ... 176
Figure 4-13: Procedures and Interventions Section Example... 179
Figure 4-14: Procedure Entry Example ... 179
Figure 4-15: Medications Administered Section Example ... 186
Figure 4-16: Care Plan Section Example ... 202
Figure 4-17: Encounter Entry Example ... 204
List of Tables
Table 1-1:
Prepare and Transport Ambulatory Healthcare Provider Birth Defect Report for Michigan
Birth Defects Registry ... 5
Table 1-2: Use Case Flow ... 6
Table 2-1: Document Specification Table ... 13
Table 2-2: Marital Status Value Set ... 22
Table 2-3: Religious Affiliation Value Set ... 22
Table 2-4: Race Value Set ... 24
Table 2-5: Ethnicity Value Set ... 44
Table 2-6: Personal Relationship Role Type Value Set ... 44
Table 2-7: Guardian Value Set ... 47
Table 3-1: CDA Header Constraints ... 50
Table 3-2: Participants in Birth Defects Header ... 50
Table 4-1: Birth Defects Diagnosis Section ... 56
Table 4-2: Birth Defects Diagnosis Entry Template ... 58
Table 4-3: Coded Results Section ... 61
Table 4-4: Simple Observation Constraints Overview ... 62
Table 4-5: Payers Section ... 64
Table 4-6: Payer Type Vocabularies ... 65
Table 4-7: Payor Role Codes ... 66
Table 4-8: Role Code Names ... 66
Table 4-9: Cytogenetics Procedure Type Codes ... 72
Table 4-10: Chromosome Analysis Codes ... 73
Table 4-11: Labor and Delivery History and Physical Section ... 73
Table 4-12: Pregnancy History Section ... 74
Table 4-13: Pregnancy Observation Value Set... 75
Table 4-14: Pregnancy Observation Value Sets ... 75
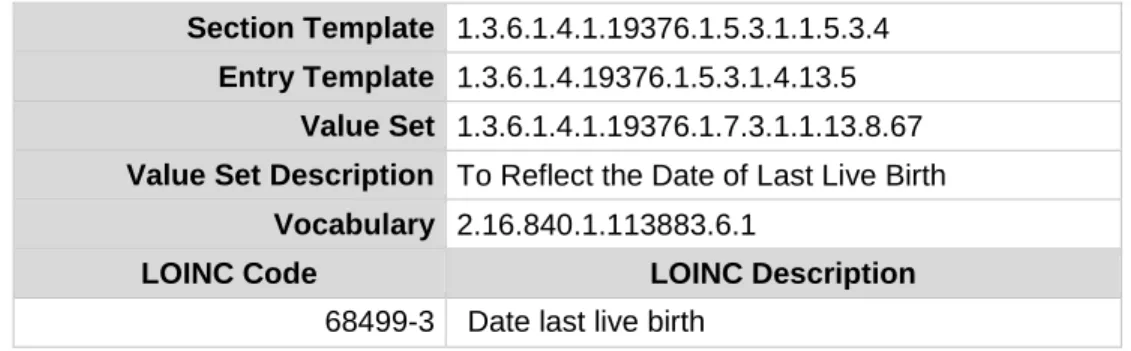
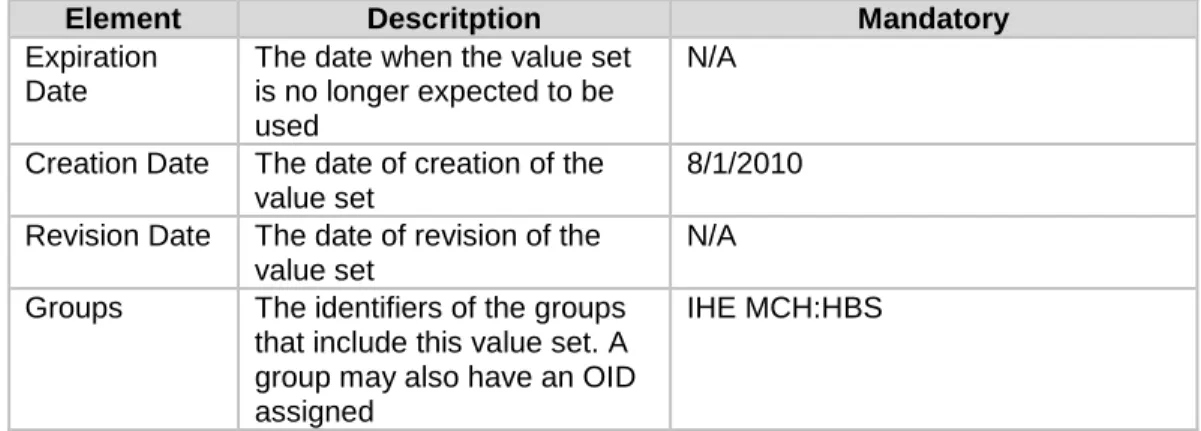
Table 4-15: MCH HBS Date of Last Live Birth Metadata ... 77
Table 4-16: MCH HBS Date of Last Live Birth Value Set ... 78
Table 4-17: MCH HBS Date of Last Other Pregnancy Outcome Metadata ... 78
Table 4-18: MCH HBS Date of Last Other Pregnancy Outcome ... 79
Table 4-19: MCH HBS Number of Prior Pregnancies Metadata ... 79
Table 4-20: MCH HBS Number of Prior Pregnancies Value Set ... 80
Table 4-21: MCH HBS Number of Previous Live Births Now Living Metadata ... 80
Table 4-22: MCH HBS Number of Previous Live Births Now Living Value Set ... 81
Table 4-23: MCH HBS Number of Previous Live Births Now Dead Metadata ... 81
Table 4-24: MCH HBS Number of Previous Live Births Now Dead Value Set ... 82
Table 4-26: BFDR Number of Preterm Births Value Set ... 83
Table 4-27: MCH HBS Poor Pregnancy Outcome History Metadata ... 84
Table 4-28: MCH HBS Poor Pregnancy Outcome History Value Set ... 84
Table 4-29: Maternal Risk Factors Value Set ... 85
Table 4-30: MCH HBS First Prenatal Care Visit Metadata ... 87
Table 4-31: MCH HBS First Prenatal Care Visit Value Set ... 87
Table 4-32: MCH HBS Last Prenatal Care Visit Metadata ... 88
Table 4-33: MCH HBS Last Prenatal Care Visit Value Set ... 88
Table 4-34: MCH HBS Number of Prenatal Care Visits Metadata... 89
Table 4-35: MCH HBS Number Prenatal Care Visits Value Set ... 90
Table 4-36: MCH HBS Pre-Pregnancy Weight Metadata ... 90
Table 4-37: MCH HBS Pre-Pregnancy Weight Value Set ... 91
Table 4-38: BFDR Date of Last Menses Metadata ... 91
Table 4-39: BFDR Date of Last Menses Value Set... 92
Table 4-40: BFDR Infertility Treatment Metadata ... 93
Table 4-41: BFDR Infertility Treatment Value Set ... 93
Table 4-42: BFDR Assistive Reproductive Technology Metadata ... 94
Table 4-43: BFDR Assistive Reproductive Technology Value Set ... 95
Table 4-44: BFDR Fertility Enhancing Drugs Metadata ... 96
Table 4-45: BFDR Fertility Enhancing Drugs Value Set ... 97
Table 4-46: BFDR Obstetric Estimate of Gestation Metadata ... 100
Table 4-47: BFDR Obstetric Estimate of Gestation
Value Set ... 101
Table 4-48: Coded Social History Section ... 101
Table 4-49: Coded Social History Observation Value Set ... 102
Table 4-50: Labor and Delivery Events Section ... 103
Table 4-51: Labor and Delivery Coded Detailed Physical Examination Value Set ... 105
Table 4-52: BFDR Mother’s Delivery Weight Metadata ... 105
Table 4-53: BFDR Mother’s Delivery Weight Value Set ... 106
Table 4-54: Labor and Delivery Procedures and Interventions Value Sets ... 106
Table 4-55: BFDR Unplanned Hysterectomy Metadata ... 107
Table 4-56: BFDR Unplanned Hysterectomy Value Set ... 108
Table 4-57: BFDR Facility Location OR Metadata ... 109
Table 4-58: BFDR Facility Location OR Value Set ... 109
Table 4-59: BFDR Delivery Metadata ... 110
Table 4-60: BFDR Delivery Value Set ... 111
Table 4-61: BFDR Unplanned Operation Metadata ... 113
Table 4-62: BFDR Unplanned Operation Value Set ... 114
Table 4-63: BFDR Transfusion Whole Blood or Packed Red Blood Metadata ... 115
Table 4-65: BFDR Epidural Anesthesia – Procedure Metadata ... 116
Table 4-66: BFDR Epidural Anesthesia – Procedure Value Set ... 117
Table 4-67: BFDR Spinal Anesthesia – Procedure Metadata ... 118
Table 4-68: BFDR Spinal Anesthesia – Procedure Value Set ... 119
Table 4-69: BFDR Route and Method of Delivery – Spontaneous Delivery Metadata ... 120
Table 4-70:
BFDR Route and Method of Delivery – Spontaneous Delivery Value Set ... 120
Table 4-71: BFDR Route and Method of Delivery – Forceps Metadata ... 121
Table 4-72: BFDR Route and Method of Delivery – Forceps Value Set ... 122
Table 4-73: BFDR Route and Method of Delivery – Vacuum Metadata ... 123
Table 4-74: BFDR Route and Method of Delivery – Vacuum Value Set ... 124
Table 4-75: BFDR Route and Method of Delivery – Cesarean Metadata ... 125
Table 4-76: BFDR Route and Method of Delivery – Cesarean Value Set ... 126
Table 4-77: BFDR Route and Method of Delivery – Trial of Labor Metadata ... 127
Table 4-78: BFDR Route and Method of Delivery – Trial of Labor Value Set ... 127
Table 4-79: BFDR Route and Method of Delivery – Scheduled Cesarean Metadata ... 128
Table 4-80: BFDR Route and Method of Delivery – Scheduled Cesarean Value Set ... 128
Table 4-81: BFDR Augmentation of Labor – Procedure Metadata ... 129
Table 4-82: BFDR Augmentation of Labor – Procedure Value Set ... 130
Table 4-83: BFDR Induction of Labor Metadata ... 130
Table 4-84: BFDR Induction of Labor Value Set ... 131
Table 4-85: BFDR Cervical Cerclage Metadata ... 132
Table 4-86: BFDR Cervical Cerclage Value Set ... 132
Table 4-87: BFDR Tocolysis Metadata ... 133
Table 4-88: BFDR Tocolysis Value Set ... 134
Table 4-89: Labor and Delivery Coded Event Outcome Value Sets ... 134
Table 4-90: MCH HBS Number of Live Births Metadata ... 135
Table 4-91: MCH HBS Number of Live Births Value Set ... 136
Table 4-92: Pregnancy Outcome Value Set ... 136
Table 4-93: BFDR Birth Plurality of Delivery Metadata ... 137
Table 4-94: BFDR Birth Plurality of Delivery Value Set ... 137
Table 4-95: BFDR Fetal Presentation at Birth- Breech Metadata ... 138
Table 4-96: BFDR Fetal Presentation at Birth- Breech Value Set ... 138
Table 4-97: BFDR Fetal Presentation at Birth- Cephalic Metadata ... 139
Table 4-98: BFDR Fetal Presentation at Birth- Cephalic Value Set ... 140
Table 4-99: BFDR Fetal Presentation at Birth- Other Metadata ... 141
Table 4-100: BFDR Fetal Presentation at Birth- Other Value Set ... 142
Table 4-101: BFDR ICU Care Metadata ... 143
Table 4-102: BFDR ICU Care Value Set ... 144
Table 4-104: BFDR Third Degree Perineal Laceration Value Set ... 145
Table 4-105: BFDR Fourth Degree Perineal Laceration Metadata ... 145
Table 4-106: BFDR Fourth Degree Perineal Laceration Value Set ... 146
Table 4-107: BFDR Ruptured Uterus Metadata ... 147
Table 4-108: BFDR Ruptured Uterus Value Set ... 147
Table 4-109: Meconium Staining Metadata ... 148
Table 4-110: Meconium Staining Value Set ... 149
Table 4-111: BFDR Premature Rupture Metadata ... 149
Table 4-112: BFDR Premature Rupture Value Set ... 150
Table 4-113: Precipitous Labor Metadata ... 151
Table 4-114: Precipitous Labor Value Set ... 151
Table 4-115: Prolonged Labor Metadata ... 152
Table 4-116: Prolonged Labor Value Set ... 153
Table 4-117: Labor and Delivery Medications Administered Value Set ... 153
Table 4-118: BFDR Antibiotics Metadata... 154
Table 4-119: BFDR Antibiotics Value Set ... 155
Table 4-120: BFDR Glucocortico Steroids Metadata ... 159
Table 4-121: BFDR Glucocortico Steroids Value Set ... 160
Table 4-122: BFDR Augmentation of Labor - Medication Metadata ... 161
Table 4-123: BFDR Augmentation of Labor - Medication Value Set ... 162
Table 4-124: BFDR Epidural Anesthesia – Medication Metadata ... 162
Table 4-125: BFDR Epidural Anesthesia – Medication Value Set ... 163
Table 4-126: BFDR Spinal Anesthesia – Medication Metadata ... 164
Table 4-127: BFDR Spinal Anesthesia – Medication Value Set ... 165
Table 4-128: Newborn Delivery Information Section ... 167
Table 4-129: Coded Detailed Physical Examination Section ... 169
Table 4-130: Newborn Coded Vital Signs Value Set ... 170
Table 4-131: MCH HBS Birth Weight Metadata ... 170
Table 4-132: MCH HBS Birth Weight Value Set ... 171
Table 4-133: MCH HBS Birth Height Metadata ... 171
Table 4-134: MCH HBS Birth Height Value Set ... 172
Table 4-135: Newborn General Appearance Value Set ... 172
Table 4-136: MCH HBS 5 Min Apgar Score Metadata ... 173
Table 4-137: MCH HBS 5 Min Apgar Score Value Set ... 173
Table 4-138: MCH HBS 10 Min Apgar Score Codes ... 174
Table 4-139: MCH HBS 10 Min Apgar Score Value Set ... 174
Table 4-140: Active Problems Section ... 175
Table 4-141: Newborn Delivery Information Active Problems Value Sets ... 176
Table 4-143: MCH HBS Seizure or Serious Neurologic Dysfunction Value Set ... 177
Table 4-144: Procedures and Interventions ... 179
Table 4-145: Newborn Delivery Information Procedures and Interventions Value Sets ... 180
Table 4-146: MCH HBS Antibiotic Administration Procedure Metadata ... 181
Table 4-147: MCH HBS Antibiotic Administration Procedure Value Set ... 181
Table 4-148: MCH HBS Karyotype Determination Metadata ... 182
Table 4-149: MCH HBS Karyotype Determination Value Set ... 183
Table 4-150: MCH HBS Assisted Ventilation Immediately Following Delivery Metadata ... 183
Table 4-151: MCH HBS Assisted Ventilation Immediately Following Delivery Value Set ... 184
Table 4-152: BFDR Total Time on Ventilator Metadata ... 184
Table 4-153: BFDR Total Time on Ventilator Value Set ... 185
Table 4-154: Medications Administered Section ... 186
Table 4-155: Newborn Delivery Medications Administered Product Value Sets ... 187
Table 4-156: BFDR Newborn Receiving Surfactant Replacement Therapy Metadata ... 187
Table 4-157: BFDR Newborn Receiving Surfactant Replacement Therapy Value Set ... 188
Table
4-158: MCH HBS Intramuscular Medication Administration Route Metadata ... 189
Table 4-159: MCH HBS Intramuscular Administration Route Value Set ... 189
Table 4-160: BFDR IV Medication Administration Metadata ... 190
Table 4-161: BFDR IV Medication Administration Route Value Set ... 191
Table 4-162: BFDR Neonatal Sepsis Metadata ... 191
Table 4-163: BFDR Neonatal Sepsis Value Set ... 192
Table 4-164: Newborn Delivery Information Coded Event Outcome Value Sets ... 192
Table 4-165: BFDR NICU Care Codes ... 193
Table 4-166: BFDR NICU Care Value Set ... 194
Table 4-167: MCH HBS Significant Birth Injury Value Set Metadata ... 194
Table 4-168: MCH HBS Significant Birth Injury Value Set ... 195
Table 4-169: BFDR Birthplace Value Set Metadata ... 197
Table 4-170: BFDR Birthplace Value Set ... 198
Table 4-171: Cause of Death Codes Metadata ... 199
Table 4-172: Cause of Death Value Set Excerpt ... 200
Preface
The Michigan Department of Health and Human Services (MDHHS) is supporting eligible
professionals meet the
Stage 2 Meaningful Use Specialized Registry Objective: Capability to Identify
and Report Specific Cases to a Specialized Registry
. Michigan’s birth defect registry will be
accepting birth defect case information in accordance to this implementation guide. For more
information on Michigan’s process to submit birth defect case reports to meet the specialized registry
objective, please contact Laura Rappleye at [email protected].
1.0
Introduction
Birth defects are a serious public health problem across the nation. Every 4 ½
minutes, a baby is born with a major birth defect in the United States. Major birth
defects are conditions present at birth that cause structural changes in one or more
parts of the body. They can have a serious effect on health, development, or
functional ability.
About one in every 33 babies is born with a birth defect. Birth defects are a leading
cause of infant death, accounting for more than 1 of every 5 infant deaths. In
addition, babies born with birth defects have a greater chance of illness and long
term disability than babies without birth defects. Birth defects contribute
significantly to childhood mortality, morbidity, and long-term disability. Despite
the prevalence of birth defects, the reporting of them is lacking.
As ambulatory healthcare providers adopt modern electronic health record (EHR)
systems, the opportunity to automate and improve birth defect registry reporting is
increasing and becoming more feasible. This document provides clear and concise
specifications for electronic reporting from ambulatory healthcare provider EHR
systems to central birth defect registries) using Health Level Seven (HL7) Clinical
Document Architecture (CDA) based standards. This document is designed to
guide EHR vendors and public health central birth defect registries in the
implementation of standardized electronic reporting. It includes both business rules
and standardized specifications.
1.1
Background
In 1992, the Michigan Department of Health and Human Services (MDHHS),
Division of Vital Records and Health Statistics established the Michigan Birth
Defects Registry (MBDR). The MBDR is a confidential and secure registry that
relies on reports submitted by all Michigan hospitals and cytogenetic laboratories.
In addition to hospitals and cytogenetic laboratories, outpatient pediatric genetic
clinics, and other facilities, may report birth defects.
The MBDR maintains a file of case reports on children from birth to two years of
age born in Michigan or to Michigan residents and diagnosed with a reportable
condition in the state of Michigan. About 10,000 Michigan children are born
annually with birth defects or other reportable conditions. As of 2013, the MBDR
contains over 638,000 reports on more than 307,000 individual children born from
1992 to 2012 with statistical data on the prevalence of birth defects available
through the state website
1. Epidemiology and vital records staff analyze registry
data and conduct special studies to better understand the impact of birth defects on
public health.
1 Michigan Department of Health and Human Services, Birth Defects. January 15, 2014. Website:
The registry enables the collection and development of statistical data on birth
defects; surveillance of birth defects; studies of birth defect causes and prevention;
and ensures the families of children with birth defects receive appropriate support
services. Specifically, the MBDR provides the information needed to compute
baseline birth defects incidence and mortality rates and analyze trends; identify and
respond to potential clusters; formulate and test hypotheses of causation; plan and
develop relevant programs; coordinate assistance for long-term care and follow up;
evaluate programs and services; and further educate professionals and the
community at large.
These activities improve the knowledge concerning the prevention of birth defects
and to assure that Michigan children with birth defects have access to available
resources and assistance. The ability to meet these goals is largely dependent on the
successful functioning of a statewide registry and the quality of the data collected.
1.2
Legal Mandate for Michigan Birth Defects Reporting
1.2.1
Public Health Code as Amended
The MBDR was established as part of the Public Health Code (Act 368 of 1978) by
amending sections 5721 and 5805. Section 5721 of Part 57 stipulates that "(1) Each
diagnosed incidence of a birth defect, including a congenital or structural
malformation, or a biochemical or genetic disease, and any information relevant to
incidents of birth defects, shall be reported to the department. (2) The department
shall maintain comprehensive statewide records of all information reported to the
birth defects registry." The Rules governing reporting, the quality, manner,
collection and analysis of the data, and confidentiality regulations are proscribed by
the Code and the legislation. Confidentiality of all data is required by law and
strictly maintained by the Health Department staff. Section 2631 of the Public
Health Code regulates procedures protecting confidentiality and regulating
disclosure of data and records.
1.2.2
Data
The MBDR maintains a file of case reports on children diagnosed with a reportable
condition at birth through two years of age who were born in Michigan or to a
Michigan resident mother. This information is reported to the Registry by hospitals,
cytology laboratories, genetics counselors, physicians and others as is authorized
by Public Act 236 of 1988 which amended the Public Health Code, Act 368 of
1978. The Act directs the Michigan Department of Health and Human Services to
establish a comprehensive birth defects registry. The amendment is aimed at
improving statewide identification of children with birth defects and facilitating the
assessment of service and referral needs for these children.
1.2.3
Rules
The Michigan Birth Defects reporting rules, R 325.9071-9076, define a reportable
defect as "an abnormality of the body's structure or inherent function present at
birth, whether the abnormality is detected at the time of delivery or becomes
apparent at a later date." A registrant is defined as "a child age birth to 2 years who
is diagnosed with a reportable birth defect in the state of Michigan." In addition,
the rules authorize the Director of the MDHHS to designate case reporting for
specific conditions up to the age of 12 years to assure complete case ascertainment.
The reports are required for children in an inpatient or outpatient setting or
diagnosed by clinical laboratories conducting cytogenetic tests or postmortem
examinations. R 325.9072 identifies reportable defects. Reports are to be submitted
within 30 days of diagnosis on the confidential Birth Defects Registry report forms
provided by the Department of Community Health or by electronic media.
1.3
Purpose
This Implementation Guide (IG) contains the necessary specifications for the
implementation of standardized data transmissions from an ambulatory healthcare
provider EHR to the MBDR. A single standardized method will allow efficient and
accurate transmission of birth defects information while reducing the burden on
EHR system-specific or registry-specific implementations.
1.4
Audience
This IG is designed to provide EHR vendors with the specifications for developing
the functionality of the EHR systems used by ambulatory healthcare providers to
report information on birth defects patients to the MBDR. The IG may also be
informative to ambulatory healthcare providers, MBDR staff, developers, analysts
and managers of public health information systems and/or data exchanges. This IG
is not intended for use for implementation of birth defects reporting from entities
other than ambulatory care settings.
1.5
Scope
This IG is intended to provide EHR developers and birth defect registry technical
staff with the operational context for use of the ambulatory care electronic birth
defect reporting.
1.6
Use Case, Scenarios, Diagrams
1.6.1
Scenario
There are a variety of scenarios in which a patient encounter includes activities
related to birth defects, including diagnosis, referral, treatment, and follow-up. For
purposes of this document, an encounter is defined as an interaction between a
patient and an ambulatory setting for the purpose of providing healthcare-related
service(s). The Use Case is triggered every time the encounter’s diagnosis is a birth
defect.
Scenario: Ambulatory Care Electronic Birth Defect Reporting to a Birth Defect
Registry
User Story Summary: Of the more than 4 million infants born each year in the
United States, approximately 120,000 have birth defects. Major birth defects are
conditions that: 1) result from a malformation, deformation, or disruption in one or
more parts of the body; 2) are present at birth; and 3) have serious, adverse effects
on the affected person’s health, development, or functioning. Birth defects are a
leading cause of morbidity and infant death accounting for more than 20% of infant
deaths.
2Surveillance of birth defects in a population is vital for quantifying the public
health impact of birth defects, monitoring trends, forming the basis for etiologic
and clinical studies, evaluating prevention strategies and interventions, planning for
services, and making informed policy decisions. Many birth defect surveillance
programs have instituted mandatory reporting requirements in an effort to receive
accurate and complete information about the suspected or diagnosed condition.
However, in the existing paper world of medical records, it has made reporting
complete and accurate information to public health registries difficult. Reporting
only occurs on a targeted basis. Hospitals and health care providers equipped with
an electronic means have the capability to submit the information needed.
Physicians in settings with limited electronic capabilities are presented with a
significant burden when required to report as they must screen for reportable cases
then gather and collate the paper documentation from the various testing and
diagnostic resources to complete the public health report. This leads to missed
cases and undercounting of many conditions. Underreporting of birth defect
conditions can slow down progress in measuring the prevalence and impact of
these conditions, complicate finding the underlying etiology and delay the
development of primary and secondary prevention and intervention strategies.
The purpose of the Ambulatory Care Electronic Birth Defect Reporting to a Birth
Defect Registry use case is to streamline birth defect reporting to improve the
timeliness and completeness of birth defect case information sent to a birth defect
or specialized registry while enabling healthcare providers achieve the Meaningful
Use Stage 2 Specialized Registry Objective.
1.6.2
Use Case Overview
Use Case Description: This use case describes the automated generation and
transmission of birth defects case information from an ambulatory healthcare
provider’s EHR to public health agencies birth defect or specialized registry. This
is intended to provide EHR developers and birth defect registry technical staff with
the operational context for use of the ambulatory care electronic birth defect
reporting implementation guide.
Pre-Conditions:
Business, legal and Health Insurance Portability and Accountability
Act (HIPAA) policy, procedures and agreements are in place
2 Division of Birth Defects and Developmental Disabilities, NCBDDD, Centers for Disease Control
and Prevention (July 19, 2013). Facts About Birth Defects. Retrieved from
Reportable birth defect case information has been captured and stored
in the EHR using the data elements and vocabulary standards
referenced in this implementation guide
The EHR has the capability to trigger and transmit the generation of
electronic report in conformance with the structure and content
standards specified in this implementation guide
Connectivity to the transport network has been established
Table 1-1: Prepare and Transport Ambulatory Healthcare Provider Birth
Defect Report for Michigan Birth Defects Registry
Actors Description
Ambulatory Healthcare Provider EHR System
An electronic health record with the capability to capture and transform birth defect case information in accordance with the Michigan IG for Ambulatory Healthcare Provider Reporting to the Birth Defect Registry
Intermediary Systems A system performing vocabulary translations, structure and content validations
Public Health Agency Birth
Defect/Specialized Registry
A system collecting electronic birth defect case information
Transport Networks Systems providing secure document transport, i.e. Health Information Exchanges (HIE), DIRECT Health Information Service Providers (HISP)
Diagnosis and Problem List Triggers:
Clinical records of children under the age of 24 months, containing an
encounter diagnosis or a problem list
reportable birth defect
conditions documented in Appendix A
Clinical records of children greater than 24 months of age with a
previous encounter diagnosis or a problem list reportable birth defect
condition with an encounter for treatment for the existing birth defect
condition
Clinical records of children up to and including 12 years of age for
certain medical conditions which are commonly diagnosed after the
age of two years containing an
encounter diagnosis or a problem list
reportable birth defect conditions documented in Appendix A
Clinical records of deceased children under the age of 24 months,
containing an
encounter diagnosis or a problem list
reportable birth
defect conditions documented in Appendix A
Clinical records of deceased children up to and including 12 years of
age for certain medical conditions which are commonly diagnosed
after the age of two years containing an
encounter diagnosis or a
problem list
reportable birth defect conditions documented in
Appendix A
Table 1-2: Use Case Flow
Step Number Step Description
1 EHR captures and stores patient-level birth defect case information 2 EHR generates and transforms an electronic birth defect report in
accordance with the Implementation Guide for Ambulatory Healthcare Provider Reporting to the Birth Defect Registry
3 EHR prepares CDA for secure transport
4 CDA sent through a secure transport network
5 EHR logs the transmission information
6 Intermediary system performs translation and validation operations and transforms document into birth defect registry format
Figure 1-1: Birth Defect Sequence Diagram
Figure 1-3 illustrates the movement of the birth defects CDA from the EHR, to the
central birth defect registry. In the first band, the EHR generates and logs the
CDA, then securely passes the CDA through the transport network. An
intermediary system translates and transforms the CDA into a format readable by
the central birth defect registry.
Birth Defect CDA Basic Flow
T ra n s p o rt N e tw o rk E H R In te rm e d ia ry S y s te m B ir th D e fe c t R e g is tr y
1. Birth Defect Case Information Entered
2. Birth Defect CDA Generated 3. CDA Configured for Secure Transmission 4. CDA Transported 6. CDA validated, translated and transformed 5. Transmission Logged
7. Birth Defect Case Information Processed 8. Confirmation of receipt generated and logged 9. Confirmation Transported 10. Confirmation Logged
Flow Exceptions:
Transport network is unavailable
EHR, Intermediary system or registry is unavailable
Post Conditions:
Birth Defect/Specialized Registry surveillance team review case
information
1.7
Use of Vocabulary Standards
This guide calls for specific vocabulary standards for the exchange of birth defect
information. Standard vocabularies, particularly coded data items, enable
automated decision support for patient healthcare, as well as for public health
surveillance of populations.
1.8
HIPAA
Providing information on diagnosed birth defects is permitted under HIPAA and is
requested to enhance the ability of the MDHHS to effectively conduct public health
surveillance of birth defects. More specifically, 45 Code of Federal Regulations
164.512 stipulates that personal health information may be disclosed to public
health authorities authorized by law to collect or receive the information for the
purpose of preventing or controlling disease, injury, or disability, including but not
limited to public health surveillance, investigation, and intervention. MDHHS has
been authorized by Michigan Compiled Law (MCL) 333.5717 to establish a birth
defects registry to develop information on birth defects incidence, the causes of
birth defects and the prevention of birth defects.
1.9
Clinical Document Architecture Release 2 (CDA R2)
Clinical documents have two key functions: they need to communicate information
between health care providers, and they need to comply with local policies, laws
and regulations. There are six characteristics of clinical documents defined in the
CDA standard.
Persistence
Stewardship
Potential for authentication
Context
Wholeness
Human readability
The CDA standard also defines two major sections of a CDA document. The first
section of the document is the header, which is use for classification and
management. The second section is the document body which contains the
information from the clinical record.
2.0 Ambulatory Healthcare Provider Birth
Defects Report
The Ambulatory Healthcare Provider Birth Defects Event Report contains a
cumulative record of a patient’s encounters for diagnosis and/or treatment of Birth
Defects. This content module inherits from the Medical Documents content
module, and so must conform to the requirements of that template as well.
2.1
Document Constraints
The Ambulatory Healthcare Provider Birth Defects Event Report specification
collects information from several Integrating the Healthcare Enterprise (IHE)
Technical Frameworks and Profiles and the HL7 Continuity of Care Document
(CCD) IG
3into one document. These include:
IHE Quality, Research, and Public Health (QRPH) Technical
Framework Supplements
o
Birth and Fetal Death Reporting
4o
Health Birth Summary (HBS)
5o
Maternal Child Health (MCH) – Birth and Fetal Death
Reporting (BFDrpt)
6o
Mother and Child Health (MCH)
7
IHE Patient Care Coordination (PCC) Technical Framework
8
IHE PCC Technical Framework Supplement – CDA Content Modules
9
IHE Cardiology Technical Framework Supplement – Cardiac Imaging
Report Content (CIRC)
10
IG for CDA Release 2 – Genetic Testing Report (GTR)
11
IG for Ambulatory Healthcare Provider Reporting to Central Cancer
Registries
12Additional constraints have been placed on certain sections and entries and one
new section has been created. All sections and further constraints are fully
described and specified in the Section Content Module section of the IG.
3HL7/ASTM Implementation Guide for CDA® R2 – Continuity of Care Document (CCD®) Release
1. Copyright 2011: Health Level Seven.
4IHE QRPH – BFDR Trial Implementation. Copyright 2013: IHE International, Inc.
5 IHE QRPH – HBS Draft for Public Comment. Copyright: 2012: IHE International, Inc.
6IHE QRPH – MCH BFDrpt Trial Implementation. Copyright 2011: IHE International, Inc. 7IHE QRPH – MCH Trial Implementation. Copyright 2010: IHE International, Inc.
8IHE Patient Care Coordination Technical Framework, Volume 2 (PCC TF-2): Transaction and
Content Modules. Copyright 2013: IHE International, Inc.
9IHE PCC Technical Framework Supplement, CDA Content Module: Trial Implementation.
Copyright 2013: IHE International, Inc.
10IHE Cariology Technical Framework Supplement, CIRC Content: Trial Implementation.
Copyright 2011: IHE International, Inc.
11Implementation Guide for CDA Release 2 – GTR – Draft Standard for Trial Use – Second Ballot.
Copyright 2011: Health Level Seven.
12Implementation Guide for Ambulatory Healthcare Provider Report to Central Cancer Registries
2.2
Parent Template
The Ambulatory Healthcare Provider Birth Defects Event Report uses the Medical
Document template (1.3.6.1.4.1.19376.1.5.3.1.1.1) as its parent template and
inherits all of the constraints from that template.
2.3
Specification
This section references content modules using Template ID as the key identifier.
Definitions of the modules are found in either the:
IHE PCC Volume 2: Final Text
IHE PCC Content Modules 2010 Supplement
Note: It is important to notice that the BxDefects Report contains information
pertaining to a single newborn. In case of multiple births each newborn will be
assigned a new CDA if a birth defect is present. The subject participation identifies
the subject of a section or entry within a CDA document. This participation is used
to identify family members (e.g., in a family history observation), or mother (e.g.,
in a labor and delivery record) for the purpose of identifying who the particular
content in the document applies to when it is other than the patient.
2.4
Birth Defects Header
Birth Defects Header shall include the child as the unique patient Role element,
while the newborn’s mother, and the newborn's father shall be identified, for any
sections/entries concerned by means of a subject participation element.
Figure 2-1: Birth Defects Header - Subject Type Code
<subject typeCode='SBJ'>
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.4.15.2'/> <relatedSubject>
<code code='MTH' codeSystem=2.16.840.1.113883.5.111 codeSystemName='IHERoleCode'/>
<!-- Mother's Id -->
<sdtc:id extension"1234567891123" root="1.2.250.1.213.1.4.1"/> <name/>
<administrativeGenderCode code="M" codeSystem="2.16.840.1.113883.5.1" codeSystemName='administrativeGender'/>
<birthTime/> </relatedSubject> </subject>
Note: In order to avoid redundant data such as address and telecom to be defined
within a <subject> tag each time a section/entry will use it, the mother could be, as
well as the father, as a <participant> entity. In this case the related <subject>
elements shall refer to it, using the <participant> id for that purpose. In this case,
the ID element subject/relatedSubject[/code@code='MTH']/subject/[sdtc:id] shall
be the same as the one declared in the header for the related participant:
Figure 2-2: Birth Defect Header – Participant Code Type
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.2.4'/> The <templateId> element
identifies this person as a patient contact and must be recorded exactly as shown
below.
<participant typeCode='IND'>
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.2.4'/> <associatedEntity classCode="PRS">
<code code="MTH" codeSystem='1.3.5.1.4.1.19376.1.5.3.3' displayName='Mother'/> <!-- Mother's Id -->
<id extension="1234567890121" root="1.2.250.1.213.1.4.1"/> <addr/> <telecom/> <associatedPerson> <name/> </associatedPerson> </associatedEntity> </participant>
2.5
Conventions Used in this Guide
2.5.1
Conformance (Optionality Constraints)
The optionality constraints in this implementation guide use the HL7 Consolidated
CDA conformance verbs (copyright 2011 Health Level Seven International).
The keywords SHALL, SHOULD, MAY, NEED NOT, SHOULD NOT, and
SHALL NOT in this document are to be interpreted as described in the HL7
Version 3 Publishing Facilitator's Guide.
13
SHALL: an absolute requirement
SHALL NOT: an absolute prohibition against inclusion
SHOULD/SHOULD NOT: best practice or recommendation. There
may be valid reasons to ignore an item, but the full implications must
be understood and carefully weighed before choosing a different
course
MAY/NEED NOT: truly optional; can be included or omitted as the
author decides with no implications
The keyword SHALL allow the use of nullFlavor unless the requirement is on an
attribute or the use of nullFlavor is explicitly precluded.
The subject of a conformance verb (keyword) in a top-level constraint is the
template itself. In nested constraints, the subject is the element in the containing
constraint.
14
13 Health Level Seven International. Retrieved from http://www.hl7.org. January 2014. 14 HL7 Implementation Guide for CDA® Release 2: IHE Health Story Consolidation, Release 1;
2.6
Cardinality
Cardinality expresses the number of times an attribute or association may appear in
a CDA document instance that conforms to the specifications described within
section 4.0. Cardinality is expressed as a minimum and a maximum value separated
by ‘..’, and enclosed in ‘[ ]’, e.g., ‘[0..1]’.
Minimum cardinality is expressed as an integer that is equal to or greater than zero.
If the minimum cardinality is zero, the element need only appear in message
instances when the sending application has data with which to value the element.
Mandatory elements must have a minimum cardinality greater than zero.
The maximum cardinality is expressed either as a positive integer (greater than zero
and greater than or equal to the minimum cardinality) or as unlimited using an
asterisk (“*”).
The cardinality indicators may be interpreted as follows:
0..1 as zero to one present
1..1 as one and only one present
1..* as one or more present
0..* as zero to many present
2.7
Null Flavor
The nullFlavor definitions in this implementation guide use the HL7 Consolidated
CDA nullFlavor information technology solutions store and manage data, but
sometimes data are not available: an item may be unknown, not relevant, or not
computable or measureable.
15In HL7, a flavor of null, or nullFlavor, describes the
reason for missing data. The following are nullFlavor examples.
Figure 2-3: nullFlavor Examples
Use null flavors for unknown, required, or optional attributes:
NI
No information. This is the most general and default null flavor.
NA
Not applicable. Known to have no proper value (e.g., last menstrual period
for a male.
NAV
Temporarily unavailable. Information is not available at this time, but it is
expected that it will be available later.
UNK Unknown. A proper value is applicable, but is not known.
15 HL7 Implementation Guide for CDA® Release 2: IHE Health Story Consolidation, Release 1;
(US Realm) Draft Standard for Trial Use. December 2011.
Figure 2-4: nullFlavor attribute required Example
Figure 2-5: Allowed nullFlavors when element is required example
1.
SHALL
contain at least one [1..*]
id
2.
SHALL
contain exactly one [1..1]
code
3.
SHALL
contain exactly one [1..1]
effectiveTime
<entry>
<observation classCode="OBS" moodCode="EVN"> <id nullFlavor="NI"/>
<code nullFlavor="OTH">
<originalText>New Grading system</originalText> </code>
<statusCode code="completed"/> <effectiveTime nullFlavor="UNK"/> <value xsi:type="CD" nullFlavor="NAV">
<originalText>Spiculated mass grade 5</originalText> </value>
</observation> </entry>
Figure 2-6: nullFlavor explicitly disallowed example
2.8
Birth Defects Specification Table
Table 2-1: Document Specification Table
Template ID TBD
Parent Template Medical Document 1.3.6.1.4.1.19376.1.5.3.1.1.1
General Description The Ambulatory Healthcare Provider BxDefects Event Report contains a record of a patient’s encounter for diagnosis and/or treatment of BxDefects. This content module inherits from the Medical Documents content module, and so must conform to the requirements of that template as well.
Document Code LOINC = TBD BxDefect Event Report
1.
SHALL contain exactly one [1..1] code/@code="11450-4" Problem List
(CodeSystem: LOINC 2.16.840.1.113883.6.1) or
2.
SHALL contain exactly one [1..1] effectiveTime/@value
1. SHALL contain exactly one [1..1] effectiveTime
Conf orm a nc e (O pti on a li lty ) Template Name Section Template Id Value Set Template Id Further Constraints applied by Ambulatory Healthcare Provider
Birth Defects Event Report Specification SHALL [1..1] Header Section 2.16.840.1.113883 .10.20.3 General Header Constraints for CDA R2
First Name recordTarget/patient Role/Patient/name/gi ven
Birth Name recordTarget/patient Role/patient/name/fa mily
Date and Time of Birth recordTarget/patient Role/patient/birthTim e Gender recordTarget/patient Role/patient/administ rativeGenderCode
[1..*] Address Useable Period element SHALL be present to indicate the beginning and ending dates the patient indicated that the address was used: ClinicalDocument/rec ordTarget/patientRole/ addr/useablePeriod Use attribute SHOULD be present to indicate the purpose of the address (e.g., mailing, home): ClinicalDocument/re cordTarget/patientR ole/addr/@use MAY [0..*] sdtc:raceCode 2.16.840.1.113883 .10.20.22.1.1 HL7 Implementatio n Guide for CDA® Release 2: IHE Health Story Consolidation, Release 1 ClinicalDocument/rec ordTarget/patientRole/ patient/sdtc:raceCode /@* Newborn Medical Record Number recordTarget/patientR ole/id
Conf orm a nc e (O pti on a li lty ) Template Name Section Template Id Value Set Template Id Further Constraints applied by Ambulatory Healthcare Provider
Birth Defects Event Report Specification SHALL [1..1] Provider Referred From 1.3.6.1.4.1.19376. 1.4.1.3.1 Cardiac Imaging Report Content (CIRC) Supplement Provider Referred From element SHALL
be present. An appropriate distinction of “None” is permitted: ClinicalDocument/com ponentOf/encompassi ngEncounter/encount erParticipant//* SHALL [1..1] Birthplace Name, State, City, Town, County, or Location of Birth Birthplace element SHALL be present. An appropriate distinction of “None” is permitted: ClinicalDocument/rec ordTarget/patientRole/ patient/birthplace//* Birth Facility
Birth facility Id, name, address recordTarget/patientR ole/providerOrganizati on Child's Facility Address recordTarget/patientR ole/providerOrganizati on/addr
Child's Facility ID recordTarget/patientR ole/providerOrganizati on/id[1] Child Facility's National Provider Identification Number (NPI) recordTarget/patientR ole/providerOrganizati on/id[2] Where: id[2]@extension is the child facility's NPI id[2]@root is the NPI's OID Child's Facility Name recordTarget/patientR ole/providerOrganizati on/name Guardian 1.3.6.1.4.1.19376. 1.5.3.1.2.4 The guardians of a patient shall be recorded in the <guardian> element beneath the <patient> element.
Guardian element
SHALL be present when the patient is a minor child :
ClinicalDocument/rec ordTarget/patientRole/ patient/guardian//*
Conf orm a nc e (O pti on a li lty ) Template Name Section Template Id Value Set Template Id Further Constraints applied by Ambulatory Healthcare Provider
Birth Defects Event Report Specification Participant Other contacts are
recorded as <participant>
elements appearing in the document header. The classCode attribute shall be set to 'IND'.
The contacts can be agents of the patient, care givers,
emergency contacts, next of kin, or other relations like mother, father respectively. Participant element SHALL be present. An appropriate distinction of “None” is permitted: ClinicalDocument/Part icipant SHALL [1..1] Active Problems Section 1.3.6.1.4.1.19376. 1.5.3.1.3.6 PCC TF-2 No Further Constraints SHALL [1..1] BxDefects Diagnosis Section This section documents the ambulatory healthcare provider’s diagnosis of the BxDefect(s) after review of all relevant diagnostic examinations and studies. Includes information about the date of diagnosis, the location of the defect. TBD OID PCC Content Module Supplement
This is the key section for the Ambulatory Healthcare Provider BxDefects Event Report and therefore
Conf orm a nc e (O pti on a li lty ) Template Name Section Template Id Value Set Template Id Further Constraints applied by Ambulatory Healthcare Provider
Birth Defects Event Report Specification NEWBORN DETAILS SHALL [1..1] Newborn Delivery Information This section should contain information about: gestational age, size, birth order, Apgar scores, height, weight and cephalic circumference, and resuscitation measures. 1.3.6.1.4.1.19376. 1.5.3.1.1.21.2.4 PCC TF Supplement CDA Content Modules (TI) Vol 2: 6.3.3.2.40 SHALL [1..1] Labor and Delivery Events This section SHALL contain information pertinent to the labor and delivery process and outcome (e.g. type of labor, method of delivery, membrane detail, placenta detail, admission reason, gestational age at delivery, fetal surveillance, labor complications, and delivery complications). This section shall include the following sections: Problems, Procedures and Interventions, and Event Outcomes subsections. 1.3.6.1.4.1.19376. 1.5.3.1.1.21.2.3 PCC TF Supplement CDA Content Modules (TI) Vol 2: 6.3.3.2.39 SHALL [1..1] Labor and Delivery History and Physical 1.3.6.1.4.1.19376. 1.5.3.1.1.21.1.1
Conf orm a nc e (O pti on a li lty ) Template Name Section Template Id Value Set Template Id Further Constraints applied by Ambulatory Healthcare Provider
Birth Defects Event Report Specification SHALL [1..1] Coded Results Section 1.3.6.1.4.1.19376. 1.5.3.1.3.28 PCC TF-2
The Coded Results Section SHALL
contain at least one entry for a simple observation for the test result. An appropriate distinction of “None” is permitted. ClinicalDocument/com ponent/structuredBod y/component/section[t emplateId[@root=’1.3. 6.1.4.1.19376.1.5.3.1. 3.28’]]/entry/observati on[templateId[@root=’ 1.3.6.1.4.1.19376.1.5. 3.1.4.13’]] SHALL [1..1] Procedures Section 2.16.840.1.113883 .10.20.1.12 CCD 3.1.4 Procedures SHALL [1..1] Payers Section 1.3.6.1.4.1.19376. 1.5.3.1.1.5.3.7 PCC TF-2 No Further Constraints SHALL [1..1] Medications Administered The medications administered section shall contain a description of the relevant medications administered to a patient during the course of an encounter. It shall include entries for medication administration. 1.3.6.1.4.1.19376. 1.5.3.1.3.21 IHE PCC 2:6.3.3.2.10 An appropriate distinction of “None” is permitted. SHALL [1..1] Medications Section 1.3.6.1.4.1.19376. 1.5.3.1.3.19 PCC TF-2 An appropriate distinction of “None” is permitted. SHALL [1..1] Cytogenetics The Cytogenetic Section resides at the highest level of the Genetic Testing Report and consists of data related to cytogenetic testing such as FISH. 2.16.840.1.1138 83.10.20.20.1.4
Conf orm a nc e (O pti on a li lty ) Template Name Section Template Id Value Set Template Id Further Constraints applied by Ambulatory Healthcare Provider
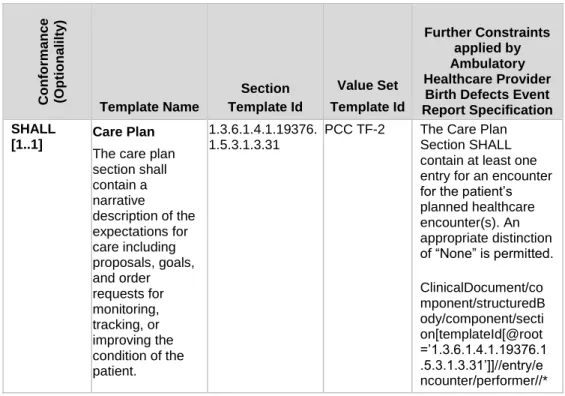
Birth Defects Event Report Specification SHALL
[1..1] Care Plan
The care plan section shall contain a narrative description of the expectations for care including proposals, goals, and order requests for monitoring, tracking, or improving the condition of the patient. 1.3.6.1.4.1.19376. 1.5.3.1.3.31
PCC TF-2 The Care Plan
Section SHALL contain at least one entry for an encounter for the patient’s planned healthcare encounter(s). An appropriate distinction of “None” is permitted. ClinicalDocument/co mponent/structuredB ody/component/secti on[templateId[@root =’1.3.6.1.4.1.19376.1 .5.3.1.3.31’]]//entry/e ncounter/performer//*
Figure 2-7: Ambulatory Healthcare Provider Birth Defect Event Report
Document Example
<ClinicalDocument xmlns='urn:hl7-org:v3'>
<typeId extension="POCD_HD000040" root="2.16.840.1.113883.1.3"/> <!-- OIDS for Medical Document, H&P and BxDefect -->
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.1.1'/> <!-- Medical Document -->
<templateId root=’2.16.840.1.113883.10.20.3’/>
<!-- CDA Header -- ><templateId root='1.3.6.1.4.1.19376.1.5.3.1.1.21.1.4'/> <!-- BxDefect OID -->
<id root=' ' extension=' '/>
<code code='XX-BxDefect' displayName='BxDefect Event Report' codeSystem='2.16.840.1.113883.6.1' codeSystemName='LOINC'/> <title> Ambulatory Healthcare Provider Report to BxDefect Registry </title> <effectiveTime value='20080601012005'/>
<confidentialityCode code='N' displayName='Normal'
codeSystem='2.16.840.1.113883.5.25' codeSystemName='Confidentiality' /> <languageCode code='en-US'/>
<!-- one or more patient --> <recordTarget>
<patientRole> .. </patientRole> </recordTarget>
<!-- one or more author --> <author> .. </author>
<!-- one or more participants --> <participant> .. </ participant >
<!-- the organization issuing this report and in charge with its lifecycle --> <custodian> .. </custodian>
<!—one or more health care providers who referred the patient to this provider for care -->
<componentOf>
<encompassingEncounter>
</encompas singEncounter> </componentOf> <informationRecipient></informationRecipient> <recordTarget> <patientRole> <patient> <birthplace> <place>..</place> </birthplace> </patient> </patientRole> </recordTarget>
<!—one or more birthplace observations --> <component>
<structuredBody> <component> <section>
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.1.21.2.4'/>
<!-- Required Newborn Delivery Information Section content --> </section>
</component> <component> <section>
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.1.21.2.3'/>
<!-- Required if known Labor and Delivery Events Section content --> </section>
</component> <component> <section>
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.3.21'/> <!-- Required Medications Section content --> </section>
</component> <component> <section>
<templateId root='1.3.6.1.4.1.19376.1.5.3.1.3.28'/> <!-- Required Coded Results Section content --> </section>
</component> <component> <section>
<templateId root='2.16.840.1.113883.10.20.20.1.4'/> <!-- Required Cytogenetics Section content --> </section>
</component> <component> <section>
<templateId root=’1.3.6.1.4.1.19376.1.5.3.1.1.21.1.1’/>
<!-- Required Labor and Delivery History and Physical Section content --> </section>
</component> <component> <section>
<templateId root=’1.3.6.1.4.1.19376.1.5.3.1.3.31’/> <!-- Required Care Plan Section content -->
</section> </component> </strucuredBody> </component> </ClinicalDocument>
2.9
Organization of Implementation Guide
2.9.1
Conventions
Conventions describe the rules adhered to in this specification.
2.9.2
Document Content Module
The Document Content Module describes the constraints for the CDA header, body
and entry sections.
2.9.3
Sections
The Section Content Module specifies section-level constraints. For example, the
Cytogenetics Genetic Testing Report Section contains a templateId element, a code
element, and the results and genetic testing observations.
2.9.4
Entry Content
The Entry Content Module defines the core semantic units of the ambulatory
healthcare provider birth defects event report—the conformance requirements for
CDA clinical statements including associated vocabularies and value sets.
2.9.5
Vocabulary and Value Sets
Vocabularies are groups of terms that are used to create the document. Some of the
vocabularies are in general use in the healthcare community; others have been
created by the birth defects registry community specifically for birth defects
reporting. A value set is a subset of the vocabulary chosen as appropriate for birth
defects reporting. Conformance statements indicate whether a specific vocabulary
or value is required.
2.10
Vocabulary Conformance
This guide calls for specific vocabulary standards for the exchange of BxDefect
information. Standard vocabularies, particularly coded data items, enable
automated decision support for patient healthcare, as well as for public health
surveillance of populations. Public Health Information Network (PHIN)
Vocabulary Services seeks to promote the use of standards-based vocabulary
within PHIN systems and foster the use and exchange of consistent information
among public health partners. These standards are supported by the PHIN
Vocabulary Access and Distribution System (VADS) for accessing, searching, and
distributing standards-based vocabularies used within PHIN to local, state and
national PHIN partner.
Furthermore, the templates in this document use terms from several code systems.
These vocabularies are defined in various supporting specifications and may be
maintained by other bodies, as is the case for the Logical Observation Identifiers
Names and Codes (LOINC®) and Systematized Nomenclature of Medicine
Clinical Terms (SNOMED CT®) vocabularies.
2.11
CDA Header Section Value Sets
The following are value sets used in the CDA Header Section, including marital
status, religious affiliation, race, ethnicity, personal relation role type, and guardian.
However, for a complete list of those value sets used in a CDA, see Appendix B.
2.11.1
Marital Status
Table 2-2: Marital Status Value Set
Value Set HL7 Marital Status
ID 2.16.840.1.113883.1.11.12212
Marital Status 2.16.840.1.113883.5.2
Code Print Name
A Annulled D Divorced T Domestic partner I Interlocutory L Legally Separated M Married S Never Married P Polygamous W Widowed
2.11.2
Religious Affiliation
Table 2-3: Religious Affiliation Value Set
Value Set HL7 2.16.840.1.113883.1.11.19185 DYNAMIC
Code System Religious Affiliation
ID 2.16.840.1.113883.5.1076
Description A value set of codes that reflect spiritual faith affiliation
Concept Code Concept Name
1001 Adventist 1002 African Religions 1003 Afro-Caribbean Religions 1004 Agnosticism 1005 Anglican 1006 Animism 1061 Assembly of God 1007 Atheism
1008 Babi & Baha'I faiths 1009 Baptist
Concept Code Concept Name
1062 Brethren 1011 Cao Dai 1012 Celticism
1013 Christian (non-Catholic, non-specific) 1063 Christian Scientist 1064 Church of Christ 1065 Church of God 1014 Confucianism 1066 Congregational 1015 Cyberculture Religions 1067 Disciples of Christ 1016 Divination 1068 Eastern Orthodox 1069 Episcopalian 1070 Evangelical Covenant 1017 Fourth Way 1018 Free Daism 1071 Friends 1072 Full Gospel 1019 Gnosis 1020 Hinduism 1021 Humanism 1022 Independent 1023 Islam 1024 Jainism 1025 Jehovah's Witnesses 1026 Judaism
1027 Latter Day Saints 1028 Lutheran 1029 Mahayana 1030 Meditation 1031 Messianic Judaism 1073 Methodist 1032 Mitraism 1074 Native American 1075 Nazarene 1033 New Age 1034 non-Roman Catholic 1035 Occult 1036 Orthodox 1037 Paganism 1038 Pentecostal 1076 Presbyterian 1039 Process, The 1077 Protestant 1078 Protestant, No Denomination 1079 Reformed 1040 Reformed/Presbyterian 1041 Roman Catholic Church 1080 Salvation Army
Concept Code Concept Name 1043 Scientology 1044 Shamanism 1045 Shiite (Islam) 1046 Shinto 1047 Sikism 1048 Spiritualism 1049 Sunni (Islam) 1050 Taoism 1051 Theravada 1081 Unitarian Universalist 1052 Unitarian-Universalism 1082 United Church of Christ 1053 Universal Life Church 1054 Vajrayana (Tibetan) 1055 Veda 1056 Voodoo 1057 Wicca 1058 Yaohushua 1059 Zen Buddhism 1060 Zoroastrianism
2.11.3
Race
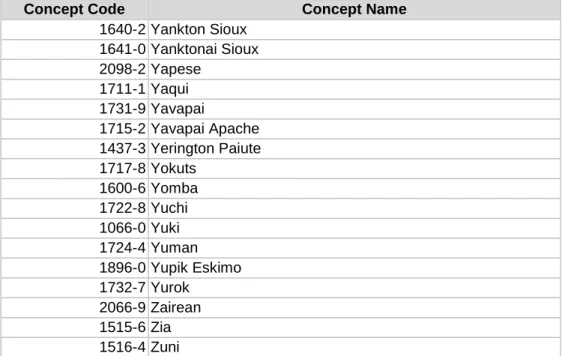
Table 2-4: Race Value Set
Value Set Race 2.16.840.1.113883.1.11.14914 DYNAMIC
Code System(s) Race and Ethnicity - CDC 2.16.840.1.113883.6.238
Description A Value Set of codes for Classifying data based upon race. Race is always reported at the discretion of the person for whom this attribute is reported, and reporting must be completed according to Federal guidelines for race reporting. Any code descending from the Race concept (1000-9) in that terminology may be used in the exchange
http://phinvads.cdc.gov/vads/ViewCodeSystemConcept.acti on?oid=2.16.840.1.113883.6.238&code=1000-9
Concept Code Concept Name
1006-6 Abenaki 1579-2 Absentee Shawnee 1490-2 Acoma 2126-1 Afghanistani 2060-2 African 2058-6 African American 1994-3 Agdaagux 1212-0 Agua Caliente
1045-4 Agua Caliente Cahuilla 1740-0 Ahtna
Concept Code Concept Name 1993-5 Akhiok 1897-8 Akiachak 1898-6 Akiak 2007-3 Akutan 1187-4 Alabama Coushatta 1194-0 Alabama Creek 1195-7 Alabama Quassarte 1899-4 Alakanuk 1383-9 Alamo Navajo 1744-2 Alanvik 1737-6 Alaska Indian 1735-0 Alaska Native 1739-2 Alaskan Athabascan 1741-8 Alatna 1900-0 Aleknagik 1966-1 Aleut 2008-1 Aleut Corporation 2009-9 Aleutian 2010-7 Aleutian Islander 1742-6 Alexander 1008-2 Algonquian 1743-4 Allakaket 1671-7 Allen Canyon 1688-1 Alpine 1392-0 Alsea 1968-7 Alutiiq Aleut 1845-7 Ambler 1004-1 American Indian
1002-5 American Indian or Alaska Native 1846-5 Anaktuvuk 1847-3 Anaktuvuk Pass 1901-8 Andreafsky 1814-3 Angoon 1902-6 Aniak 1745-9 Anvik 1010-8 Apache 2129-5 Arab 1021-5 Arapaho 1746-7 Arctic
1849-9 Arctic Slope Corporation 1848-1 Arctic Slope Inupiat 1026-4 Arikara 1491-0 Ariz