Air and surface contamination patterns of meticillin-resistant Staphylococcus aureus on eight acute hospital wards
Authors: Eilish Creamer, MSc;1 Anna C. Shore, PhD; 2,3 Emily C. Deasy BA (Mod.); 2 Sandra Galvin, PhD; 1 Anthony Dolan, PhD;1 Niamh Walley, MB;1 Seamus McHugh, MD; 4 Deirdre Fitzgerald-Hughes, PhD; 1 Derek J. Sullivan, PhD; 2 Robert Cunney, MD; 5,6 David C. Coleman, ScD; 3 Hilary Humphreys, MD.1,7*
1Department of Clinical Microbiology, Education and Research Centre, Royal College of Surgeons in Ireland, Dublin, 2Microbiology Research Unit, Division of Oral Biosciences, School of Dental Science and Dublin Dental University Hospital, University of Dublin, Trinity College Dublin 2, 3Department of Clinical Microbiology, School of Medicine, University of Dublin, Trinity College, St. James’s Hospital, Dublin 8, 4 Department of Surgery, the Royal College of Surgeons in Ireland and Beaumont Hospital, 5Health Protection Surveillance Centre, Dublin, 6Department of Microbiology, Children’s University Hospital, Temple Street, Dublin, 7Department of Microbiology, Beaumont Hospital, Dublin, Ireland.
* Corresponding author:
Hilary Humphreys, Department of Clinical Microbiology, RCSI Education and Research Centre, Beaumont Hospital, PO Box 9063, Beaumont Road, Dublin 9, Ireland.
Tel.: +353 1 8093710/3708 Fax +353 1 8092871. E-mail address: [email protected]
Key words: aerial transmission of MRSA, environmental sampling, air sampling, cross-transmission, MRSA, spa typing, DNA microarray profiling
Running title: Aerial dispersal of MRSA 1
2
3
4
5 6 7
8 9 10 11 12 13 14
15
16 17 18 19 20 21
Abstract
BACKGROUND. Methicillin-resistant Staphylococcus aureus (MRSA) can be recovered from
hospital air and from environmental surfaces. This poses a potential risk of transmission to patients.
OBJECTIVE. To investigate associations between MRSA isolates recovered from air and environmental surfaces with those from patients when undertaking extensive patient and environmental screening.
DESIGN. A prospective observational study of patients and their environment in eight wards of a 700-bed tertiary care hospital during 2010 and 2011.
METHODS. Sampling of patients, air and surfaces was carried out on all ward bays, with more extended environmental sampling in ward high-dependency bays (HDBs) and at particular times of the day. The genetic relatedness of isolates was determined by DNA microarray profiling and
spa typing.
RESULTS. MRSA was recovered from 30/706 (4.3%) patients and from 19/132 (14.4%) air
samples. On 9/132 (6.8%) occasions both patient and air samples yielded MRSA. In 32 HDBs, MRSA was recovered from 12/161 (7.4%) patients, 8/32 (25%) air samples, and 21/644 (3.3%) environmental surface samples. On 10/132 (7.6%) occasions, MRSA was isolated from air in the
absence of MRSA-positive patients. Patient demographic data combined with spa typing and DNA microarray profiling revealed four transmission clusters, where patient and environmental
isolates were indistinguishable or deemed to be very closely related. 23
24
25 26
27 28 29
30 31
32 33 34
35
36
37 38 39
40 41
CONCLUSIONS. Air sampling yielded MRSA on frequent occasions, especially in HDBs.
Environmental and air sampling combined with patient demographic data, spa typing and DNA
microarray profiling indicated the presence of clusters that were not otherwise apparent
.
4344
Introduction
Numerous studies have shown that the hospital environment is frequently contaminated with
potential pathogens that pose a risk of cross-transmission to patients.1,2 Methicillin-resistant Staphylococcus aureus (MRSA) can survive for long periods on environmental surfaces, and may be transmitted to patients via healthcare workers hands or the environment.3,4 Studies on MRSA in the environment have mostly related to outbreaks,5 intensive care units (ICUs), 6,7 or isolation rooms with MRSA patients, rather than in routine ward areas over a period of time.8,9
There is relatively little information on the dispersal of airborne MRSA and this may be an often underestimated method of transmission that results in clusters or outbreaks. It is not clear what
impact MRSA in the environment and in air have on patient acquisition and cross-transmission and many studies involving the sampling of air in the vicinity of patients have been once-off investigations Previous studies have strongly suggested or confirmed the transmission of bacteria
by air, especially when carriers of S. aureus have viral infection.10,11 However, the extent to which MRSA may be recovered from the air and how commonly this occurs in an acute hospital
outside of an outbreak is unclear.
The current study describes the pattern of MRSA recovered from air and the patient’s
environment on a number of wards where MRSA is endemic over a period of time and
investigates patient and environmental links using spa typing and DNA microarray profiling of
isolates. 46
47
48 49
50 51 52
53 54
55 56 57
58 59
60
61 62
63 64
Methods
Patients. The study was conducted on patients and their environment on eight wards, four general surgical and four general medical in a 700-bed tertiary referral acute care hospital during 2010-2011. The study was undertaken as part of a larger study of MRSA that was approved by
the Hospital Ethics (Medical Research) Committee. Patient and environmental sampling were conducted on a scheduled basis, and were not in response to an outbreak investigation. Bed occupancy was approximately 100%. Sampling was carried out accordingly in three separate
but complementary ways. Firstly, sampling was conducted on 132 occasions on eight wards between March 2010 and February 2011. From March to June 2010, eight wards were sampled
successively; three wards were sampled once and five twice. From September 2010 to February 2011, the patients and the environment of four wards were each sampled for four weeks
consecutively. Patient screening involved the taking of swabs from the nose, groin and
non-intact skin/wound if, available (n = 706), with one air sample taken in each ward bay. Secondly, on 32 occasions, extended environmental sampling was conducted in the immediate area of
patients in two high-dependency bays (HDBs) on eight wards, where more vulnerable and sicker patients are cared for. Patients were screened for MRSA on study wards as previously
described.12,13 At- risk patients were those as defined in national guidelines, i.e. patients known
to be previously MRSA-positive, patients transferred from another hospital or a long-term care facility, patients with chronic ulcers or urinary catheters and patients who had been hospitalized
within the last 18 months1. Environmental sampling involved surface sampling of each patient’s mattress, pillow, bedrail or bedframe and locker. In addition, a settle-plate was placed on each patient’s locker and one air sampling was conducted at the window-ledge of each ward bay. 67
68
69 70
71 72 73
74 75
76 77 78
79 80
81 82 83
84 85
Thirdly, air sampling was conducted on HDBs at different times over a 24 h period; between;
07.30 -09.00 h, 09.30-11.30 h, 14.00-16.00 h, 17.00-19.00 h, and 20.00-22.00 h, but without simultaneous patient sampling. However during this study phase, routine ward screening did not reveal any MRSA-positive patients to be present in the HDBs during these periods of sampling.
No area sampled had any form of artificial ventilation. Cleaning was performed daily by the cleaning services, using water and detergent. A hypochlorite, 1000 ppm av. chlorine was used
for MRSA and other infected/contaminated patients. Terminal decontamination of the bed and bed area after a patient’s discharge of the bed and bed area was performed by a designated cleaning team.
Air and environmental surface sampling.Samples of air (1,000 L) were taken using an impact air sampler (AES Chemunex Air Sampler, Dėpartment SAV, Rue Maryse Bastiė-Ker Lann, 35172 BRUZ cedex, France) with MRSASelect chromogenic agar (CA) plates (Bio-Rad Life Science Group, France) which was placed on the ledges of outer wall windows in ward bays. CA settle
plates were also placed on patients’ lockers for one hour. Neutralising buffer swabs (Technical Services Consultants, Lancashire,UK) were used to sample mattresses, pillows, bedrail or bed
frames and patient lockers. An area, 10 cm x 10 cm, of each surface was sampled. In addition, mattresses were assessed by sweeping a CA plate over the surface of the mattress. Most wards consisted of 35 beds, each with one 4-bedded and one 6-bedded HDB, three other 6-bedded bays,
one 2-bedded bay and five single rooms (Figure 1a). HDBs mainly comprised of four (wards A) or six-bedded (wards B) ward bays but one ward had a five-bedded bay. The environmental
sampling sites were those immediately associated with the patient’s bed area and are shown in Figure 1b. All environmental swabs were enriched in tryptone soy broth with 6% (w/v) NaCl 89
90 91 92
93 94
95 96 97
98 99
100 101 102
103 104
105 106 107
108 109
(TB05S-100, Cruinn Diagnostics, Ireland) and incubated at 37°C for 18 h. These were
subsequently subcultured onto CA and incubated along with settle plates and sweep plates for 24 h at 37°C. Presumptive MRSA was confirmed by coagulase and clumping factor production using Staphaurex Plus (Remel, U.K.) and methicillin resistance determination using oxacillin
minimum inhibitory concentration (MIC) evaluator strips (Oxoid, U.K.) and detection of resistance with cefoxitin, 30µg disks (Oxoid, U.K.).
Molecular typing. spa typing was carried out on one isolate per MRSA-positive patient and/or the patients’ environment in the HDBs using the method described at the SeqNet website and amplimer sequencing was performed by Source BioScience (Guinness Enterprise Centre, Dublin,
Ireland). Where two sampling methods (e.g. swab and sweep-plate) were MRSA-positive from mattress sampling, only one MRSA isolate was included in the analysis. DNA microarray
profiling was performed using the StaphyType Kit (Alere, Germany) on all except two of the isolates that underwent spa typing; these two isolates were not available for DNA microarray profiling. The StaphyType Kit detects 334 S. aureus gene sequences and alleles including typing
and species-specific markers as well as virulence-associated and antimicrobial resistance genes. DNA microarray procedures were performed according to the manufacturer’s instructions.14
Statistical analysis. Statistical analysis was performed using Epi Info 6 (version 6.04c; Centers for Disease Control and Prevention, Atlanta, GA) and odds ratios (ODs) were calculated. The Mantel-Haenszel chi square method was used to assess the significance of the difference
between proportions. 112
113 114 115
116 117
118 119 120
121 122
123 124 125
126 127
128 129 130
Results
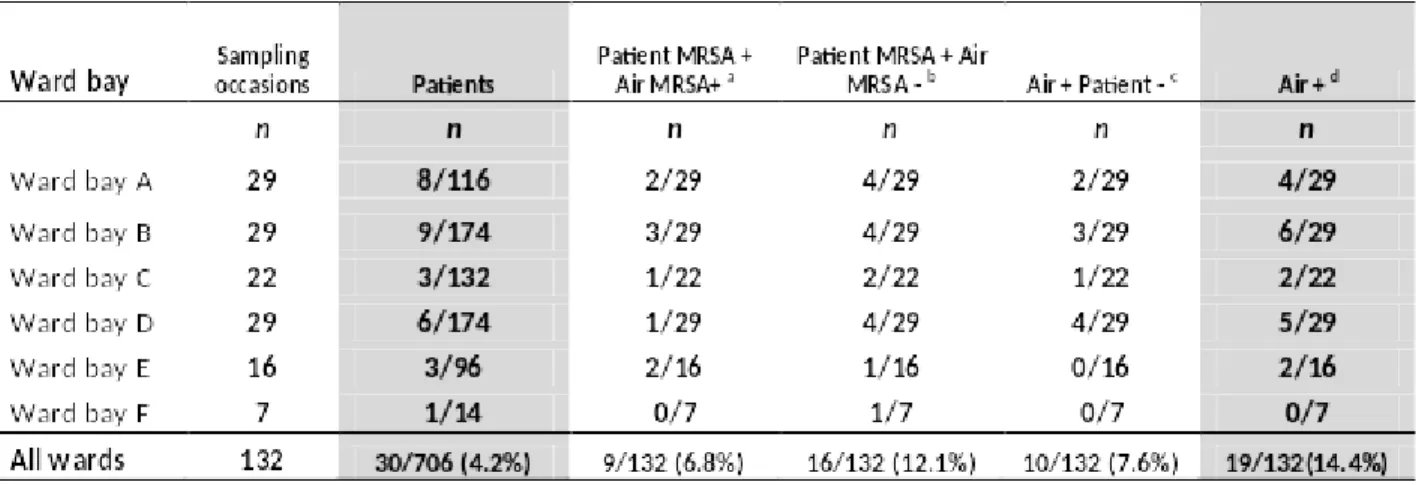
Patient and air sampling. Overall, 30/706 (4.3%) patients and 19/132 (14.4%) air samples yielded MRSA (Table 1). Only two of the MRSA positive patients had infections, the remainder were colonized only. . On 9/132 (6.8%) sampling occasions both patient and air samples were
positive, but on 10/132 (7.6%) occasions air samples yielded MRSA but no MRSA-positive patients were identified. When four wards were sampled consecutively for a four-week period, MRSA was isolated on week 1, (5 patients, 2 air samples); week 2 (4 patients, 2 air
samples); week 3, (1 patient, no air samples) and week 4 (2 patients, 1 air sample). Three of the five air samples were linked to a MRSA-positive patient in a specific ward bay.
Environmental sampling on 32 occasions in HDBs. MRSA was recovered from 9/85 (10.6%) male and 3/76 (4%) female patients on nine environmental sampling occasions resulting in
(12/161 (7.4%) positive samples. MRSA was recovered from 8/32 (25%) air samples, from 12/161 (7.5%) settle plates and from 21/644 (3.3%) surface environmental sites. On five
occasions, MRSA was isolated from two patients in a ward bay. Ten of 161 (6.2%) mattresses, 2/161 (1.2%) pillows, 3/161 (1.9%) bedrail/frames and 6/161 (3.7%) bedside lockers yielded MRSA. MRSA was isolated from at least one sample (patient or environment) on 16/32 (50%)
occasions. On 2/32 (6.3%) occasions, MRSA was recovered from one or more patients as well as from air samples, settle plates and one or more environmental surface sites. For three of twelve
MRSA-positive patients, MRSA was recovered from the patient’s mattress, plus the locker for one patient, from the mattress and locker for another patient, and from the mattress, bed frame and pillow of another patient. Two of these MRSA-positive patients were associated with 132
133 134
135 136
137 138 139
140 141
142 143 144
145 146
147 148 149
150 151
extensive contamination, (ward 2 in June 2010 and ward 7 in January 2011). Patient risk factors
for the 12 MRSA patients included previous MRSA (1/12), transfer from another hospital (1/12), the presence of a urinary catheter (3/12) and admission within the previous 18 months (7/12). MRSA was isolated from nasal swabs in ten patients, a groin swab in one and both nasal and
groin in one patient. One of 12 patients with nasal/groin swab MRSA-positive was associated with extensive MRSA environmental contamination in January 2011.
Air sampling over a 24 h period. Thirteen of 128 (10%) air samples in HDBs yielded MRSA; 7/32 (22%) between 07.30-09.00h, 3/32 (9%), between 09.30-11.30h, 1/32 (3%), between 14.00-16.00h, 0/16 (0%), between 17.00-19.00h and 2/16 (13%), between 20.00-22.00h, with
significantly more MRSA-positive samples recovered between 07.30h and 09.00h compared to other times, i.e. 7/32 (22%) versus 6/96 (6%), odds ratio (OR), 4.20 (95% confidence interval
(CI), 1.13-15.81), p=0.01.
Molecular epidemiological typing. spa typing was conducted on 42/53 (79%) MRSA isolates arising from extended patient and environmental screening in HBDs; 10 patient isolates, five air
samples, nine settle-plate isolates and 18 environmental surface isolates. Four different spa types were identified among patient and environmental isolates including t515, (19 isolates) t557, (19
isolates), t032, (four isolates) and t022 (one isolate). DNA microarray profiling was performed on 42 of the isolates that were spa-typed. The array assigned all isolates to ST22-MRSA-IV and revealed that all harbored the beta-lactamase resistance gene blaZ, the enterotoxin gene cluster
egc and the immune evasion complex (IEC) genes sak, chp and scn. Limited variability was seen among the isolates in relation to the carriage of the macrolide resistance gene erm(C) (37/40,
92.5%) and the co-located enterotoxin genes sec & sel (36/40, 90%). The DNA microarray 155
156 157 158
159 160
161 162 163
164 165
166
167 168
169 170
171 172 173
174 175
profiles of all spa type t557 isolates were indistinguishable (blaZ, erm(C), sec & sel, egc and IEC
type B, n = 20). Two array profiles were identified among t515 isolates (blaZ, erm(C), sec & sel, egc and IEC B, n = 12; blaZ, erm(C), egc and IEC B, n = 3), whereas three were identified among t032 isolates (blaZ, egc, IEC B, n = 1; blaZ, sec & sel, egc, IEC B, n = 1; blaZ, ermC,
sec & sel, egc, IEC B, n = 2).
On epidemiological grounds there were four potential MRSA clusters, i.e. MRSA isolated from one or more patients and their environment or from two or more patients without any
environmental sites positive for MRSA. Patient demographic data combined with spa typing and
DNA microarray profiling suggested four clusters (Table 2). The first of these was on the 06/11/10 and involved 19 spa type t557 isolates from threepatients with 16 environmental sites
in two bays of ward 2; these isolates all yielded indistinguishable DNA microarray profiles. The second spa typing cluster was recovered on the 14/06/10 and involved two spa type t032 isolates from two patients in two ward bays of ward 3; these isolates differed by one gene combination
only using the DNA microarray and are considered to be closely related. The next spa typing cluster was recovered on 26/10/10 and again involved two spa type t032 isolates, one recovered
from a patient and the other from an environmental site of ward bay A on ward 5; these isolates exhibited indistinguishable DNA microarray profiles. The final spa typing cluster involved 12 spa type t515 isolates recovered on 01/04/11 and involved one patient and 11 environmental isolates on ward A; again these isolates exhibited indistinguishable DNA microarray profiles. Three of four other environmental isolates yielded indistinguishable spa (t515) and microarray 177
178 179 180
181
182
183 184 185
186 187
188 189 190
191 192
193 194 195
pattern profiles, on the 23/06/2011, in two bays of ward 5. However, no positive MRSA patients
were identified as being epidemiologically associated with these isolates.
Discussion
MRSA is endemic in most Irish hospitals and this study was part of a program of research to
determine if current methods of screening underestimate the extent of MRSA colonization and environmental contamination. Through a combination of admission screening of all patients (not just those in at-risk categories such as patients being transferred from another hospital),
follow-up screening while in-patients, air and environmental sampling and the prospective collection of detailed demographic data and molecular typing, we have endeavored to gain a deeper
understanding of the extent of MRSA colonization and transmission. Results showed that some patients are MRSA-positive even though not in an at-risk category and who would not normally be routinely screened, that transmission can occur but remain undetected if solely relying on
routine screening and that the method of environmental sampling influences the density of MRSA recovered from the healthcare environment.12, 13, 15
In this study MRSA was mainly isolated from the air in ward bays, (air sampling sites outlined in Figure 1b), where MRSA-positive patients were identified. However, on 7.6% of 132 sampling
occasions, MRSA was detected from air samples when no known MRSA-positive patients were identified, possibly because of unidentified MRSA-positive individuals in the vicinity, recently
discharged MRSA-positive patients, or environmental contamination. When patient screening and air sampling were conducted on four wards over a 4-week period, more MRSA-positive patients and environmental samples were identified during the first two weeks, than during 198
199
200
201
202 203 204
205 206
207 208 209
210 211
212
213 214
215 216
weeks 3-4. This may suggest that the early identification of MRSA patients arising from this
study and their subsequent isolation may have contributed to fewer MRSA-positive samples during the last two weeks of screening.
In HDBs, MRSA was recovered on 50% of occasions from either patients or their environment, probably due to the greater risk of these more vulnerable patients having MRSA. Apart from the
presence of a urinary catheter in 3/12 patients, no other MRSA risk factors were associated with environmental contamination. Skin scales can travel significant distances especially when associated with extensive activity.9,16,17,18 While we assessed particle counts and particle size
variation on one occasion (data not shown), we found no correlation with bacteriological sampling results.
Active air sampling by its very nature draws air from a wide area, which makes it difficult to associate environmental isolates with specific patients. In order to more accurately measure the
dispersal of MRSA from individual patients we conducted environmental sampling of beds. For three of twelve MRSA-positive patients, MRSA was recovered from the patients mattress as well
as other environmental sites surrounding the patient’s bed. Two of these patients were associated with extensive environmental contamination on ward 2 on the 11/06/2010 and on ward 7 on the 04/01/2011. While not conclusive, these patients may have been index patients for the outbreaks.
The greater likelihood of recovering MRSA from air samples compared with settle plates and environmental surfaces is possibly related to the increased sensitivity of this method of sampling 220
221 222
223
224 225
226 227 228
229 230
231
232 233
234 235
236 237 238
due to the increased volume of air sampled (i.e. 1,000 L).19 Seven of 12 (75%) MRSA-positive
settle plates were related to two clusters involving four patients, suggesting that MRSA can be dispersed in the air from the immediate vicinity of MRSA-positive patients to other ward areas.
Rates of recovery of MRSA are higher during ward activities, and at different times during the day, before, during and after cleaning.18,6 We recovered significantly higher rates of MRSA in air
samples early in the morning, i.e. between 07.30-09.00 h compared with at other times. Sampling at this time, before routine ward cleaning would generally be regarded as a low activity time, i.e. less movement of patients and staff.20-22 Air samples positive for MRSA declined during the day
when cleaning, ward rounds and other activities were taking place, with less MRSA being isolated during the afternoon/evening, similar to a study on two respiratory wards that showed
higher levels of particulate matter in the morning during ward activity , i.e. bed making,
nebulisation, peaking again around lunch time and reducing during times of low activity.12 The more frequent recovery of MRSA from surfaces in ICUs has been reported between 08.00-09.00
h than during the rest of the day.6 Aerial dispersal of Clostridium difficile was found to be higher during the distribution of meals.23 However, patients may shed more skin scales6,23 during the
night when sleeping, and this may explain our finding of more MRSA between 07.30-09.00 h, but some ward activity may have been taking place before 7.30 AM.
Effective cleaning and the decontamination of environmental surfaces have been associated with reduced MRSA in the patient’s environment,24 but cleaning may not always be effective. In the 241
242 243
244
245 246
247 248 249
250 251
252 253 254
255 256
257 258
259
present study, mattresses were the items of equipment from which MRSA was most frequently
isolated and these may be a significant reservoir in the environment. Patients may acquire MRSA from a previous MRSA-positive patient if decontamination between patient admission to that clinical area is inadequate.25 The surface of patients’ lockers was also contaminated, possibly
from aerial transmission, but also due to indirect contact with MRSA-positive patients via healthcare staff combined with inadequate cleaning.
The use of spa typing as a standalone typing method for differentiating between highly clonal ST22-MRSA-IV isolates has been shown to be inadequate.26 In the present study spa typing was
combined with DNA microarray profiling to attempt to enhance discrimination of the ST22-MRSA-IV isolates based on the presence or absence of virulence-associated and antimicrobial
resistance genes. This combined molecular typing approach together with epidemiological data identified four clusters, three of which were on different wards involving patients and the environment. In addition, three of four isolates that were linked epidemiologically and isolated
from the environment were indistinguishable but these were not associated with MRSA-positive patients. While it is important not to rely on spa typing alone for typing of MRSA particularly in
an endemic setting, in the present study DNA microarray profiling did not result in isolates clustered based on spa typing being further differentiated. However, the DNA microarray permits identification of characteristic resistance and virulence genes among isolates as we have
demonstrated for a collection of isolates causing MRSA bloodstream infection.27 262
263 264 265
266 267
268 269 270
271 272
273 274 275
276 277
278 279 280
281
Patterns of air dispersal of S. aureus are not generally well understood in the healthcare
environment or elsewhere. A recent study of livestock-associated MRSA traced the spread of MRSA in the vicinity of pig barns and spa typing indicated that MRSA spread was influenced by the season and the wind direction.28 The clinical areas sampled in our study were naturally
ventilated and therefore air flow would have been influenced by open doors and windows and the movement of patients and staff.
The limitations of this study include taking samples mainly in HDBs and not as frequently throughout the rest of the ward, as this would have more accurately determined the full extent of
MRSA dispersal. We sampled mainly nasal and groin sites but not other sites such as throat, sputum, urine, etc. which may be associated with significant additional air dispersal. Because of
logistical and resource reasons, air sampling was conducted at one position only, i.e. the outer window of each ward bay and not beside each patient in all ward bays, thus our sampling possibly missed MRSA dispersion from patients further away from the window. Sampling was
conducted during the day and early night periods, but not between 22.00h-07.30h, when patients were asleep and there was less activity on the ward. Broth enrichment was not used for patient
samples and healthcare staff were not screened; both may have underestimated the true number of MRSA- positive carriers on the ward and may explain the presence of MRSA in the air without known MRSA positive patients in the immediate vicinity. One study found that the
average limit of detection for direct culture and broth enrichment in an in vitro study was
approximately 750 CFU/ml and 40 CFU/ml, respectively.29Hence broth enrichment significantly 283
284 285 286
287 288
289 290 291
292 293
294 295 296
297 298
299 300 301
enhances the sensitivity of MRSA detection but with a longer time to confirmation of MRSA
status.
In conclusion, MRSA was recovered from either patients or their environment on 50% of
sampling occasions with patterns suggesting dispersal from patients to the surrounding air. This suggests that aerial transmission from patient-to-patient may be common. While not conclusive,
patients appear to shed MRSA more frequently early in the morning or during the night. The use of computational fluid dynamics might assist in the accurate prediction of the spatial distribution of MRSA as shown in a recent study which investigated the use of a physical partition between
patients and the location of patients vis a vis the air supply.30 However, further prospective studies of patients in different settings including in single rooms and in multiple bed settings,
during different periods of activity such as the changing of bed linen, and under natural and artificially ventilated facilities are required.
Acknowledgements
This study was funded by the Health Research Board, Ireland (TRA/2006/4). We are grateful to
all members of the Infection Prevention and Control Team and the Department of Microbiology in Beaumont Hospital for their assistance. We also acknowledge the co-operation,
encouragement and support from all nursing, medical and other staff. 304
305
306 307
308 309
310 311 312
313 314
315 316
317
318
319
Conflict of interest: HH has received research support from Steris Corporation, Inov8 Science, Pfizer & Cepheid in recent years. He has also recently received lecture & other fees from Novartis, Astellas and AstraZeneca.
No conflict of interest is reported by the other co-authors. 323
324 325
References
1 Health Protection Surveillance Centre. The control and prevention of
MRSA in hospital and in the community. Dublin: Health Protection Surveillance Centre; 2005.
2 Smith TC, Moritz ED, Leedom Larson KR, Ferguson DD. The
environment as a factor in methicillin-resistant Staphylococcus aureus transmission. Rev Environ Health 2010;25: 121-134.
3 Boyce JM, Potter-Bynoe G, Chenevert C, King T. Environmental contamination due to methicillin-resistant Staphylococcus aureus: possible infection control implications.
Infect Control Hosp Epidemiol 1997;18:622-627.
4 Hota B. Contamination, disinfection, and cross-colonization: are hospital surfaces reservoirs for nosocomial infection? Clin Infect Dis 2004;39:1182-1189.
5 Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the
transmission of nosocomial pathogens. Infect Control Hosp Epidemiol 2011;32:687-699.
6 Wilson AP, Smyth D, Moore G, et al. The impact of enhanced cleaning within the intensive care unit on contamination of the near-patient environment with hospital pathogens: A randomized crossover study in critical care units in two hospitals. Crit Care
Med 2011;39:651-658.
7 Wilson RD, Huang SJ, McLean AS. The correlation between airborne
methicillin-resistant Staphylococcus aureus with the presence of MRSA colonized patients in a general intensive care unit. Anaesth Intensive Care 2004;32: 202-209.
327
328
329 330
331 332 333
334 335
336 337 338
339 340
341 342 343
344 345
8 Sexton T, Clarke P, O'Neill E, Dillane T, Humphreys H. Environmental reservoirs of
methicillin-resistant Staphylococcus aureus in isolation rooms: correlation with patient isolates and implications for hospital hygiene. J Hosp Infect 2006;62:187-194.9.
9 Gehanno JF, Louvel A, Nouvellon, M, Caillard J-F, Pestel-Caron M. Aerial dispersal of
meticillin-resistant Staphylococcus aureus in hospital rooms by infected or colonised patients. J Hosp Infect 2009;71:256 -262.
10 Sherertz RJ, Reagan DR, Hampton KD, et al. A cloud adult: The Staphylococcus aureus -virus interaction revisited. Ann Intern Med1996;124:539-547.
11 Yap FHY, Gomersall CD, Fung KS, et al. Increase in methicillin-resistant
Staphylococcus aureus acquisition rate and change in pathogen pattern associated with an outbreak of severe acute respiratory syndrome. Clin Infect Dis 2004;39: 511-6.
12 Creamer E, Galvin S, Dolan A et al. Evaluation of screening risk and non risk patients for methicillin-resistant Staphylococcus aureus on admission in an acute care hospital. Am J Infect Control 2012;40: 411-5.
13 Creamer E, Shore AC, Rossney AS, et al. Transmission of endemic ST22-MRSA-IV on four acute hospital wards investigated using a combination of spa, dru and pulsed field
gel electrophoresis typing. Eur J Clin Microbiol Infect Dis 2012;31:3151–3161.
14 Monecke S, Jatzwauk L, Weber S, Slickers P, Ehricht R. DNA microarray-based genotyping of methicillin-resistant Staphylococcus aureus strains from Eastern Saxony.
Clin Microbiol Infect 2008; 14: 534-45.
15 Dolan A, Bartlett M, McEntee, B, Creamer E, Humphreys H. Evaluation of different
methods to recover meticillin-resistant Staphylococcus aureus from hospital environmental surfaces. J Hosp Infect 2011;79: 227-30.
348
349 350 351
352 353
354 355 356
357 358
359 360 361
362 363
364 365 366
367 368
16 Eames I, Tang JW, Li Y, Wilson P. Airborne transmission of disease in hospitals. J. R.
Soc. Interface 2009; 6:S697–S702.
17 Roberts K, Hathway A, Fletcher LA, Beggs CB, Elliott MW, Sleigh PA. Bioaerosol production on a respiratory ward. Indoor Built Environment 2006: 15: 35-40.
18 Shiomori T, Miyamoto H, Makishima K, et al. Evaluation of bed making-related airborne and surface methicillin-resistant Staphylococcus aureus contamination. J Hosp Infect
2002;50:30-35.
19 Pasquarella C, Pitzurra O, Savino A. The index of microbial air contamination. J Hosp Infect 2000;46:241-256.
20 Wong V, Staniforth K, Boswell TC. Environmental contamination and airborne microbial counts: a role for hydroxyl radical disinfection units? J Hosp Infect 2011;78:194-199.
21 Greene VW, Bond RG, Michaelsen MS. Air handling systems must be planned to reduce the spread of infection. Mod Hospit 1960; 95: 136-144.
22 Solberg CO. Spread of Staphylococcus aureus in hospitals: causes and prevention. Scand
J Infect Dis 2000;32:587-595.
23 Best EL, Fawley WN, Parnell P,Wilcox MH. The potential for airborne dispersal of
Clostridium difficile from symptomatic patients Clin Infect Dis 2010; 50:1450–1457.
24 Dancer SJ, White LF, Lamb J, Girvan EK, Robertson C. Measuring the effect of
enhanced cleaning in a UK hospital: a prospective cross-over study. BMC Medicine 2009,
7:28 http://www.biomedcentral.com/1741-7015/7/28 accessed 27-08-2011.
25 Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior
room occupants. Arch Intern Med 2006;166:1945-1951. 371
372 373 374
375 376
377 378 379
380 381
382 383 384
385 386
387 388 389
390 391
26 Shore AC, Rossney AS, Kinnevey PM, et al. Enhanced discrimination of highly clonal
ST22-methicillin-resistatn Staphylococcus aureus IV isolates achieved by combining spa, dru, and pulsed field gel electrophoresis typing data. J Clin Microbiol 2010; 48: 1839-52.
27 McNicholas S, Shore AC, Coleman DC, Humphreys H, Fitzgerald Hughes D. DNA
microarray genotyping and virulence and antimicrobial resistance gene profiling of methicillin-resistant Staphylococcus aureus bloodstream isolates from renal patients. J
Clin Microbiol 2011; 49: 4349-4351.
28 Schulz J, Friese A, Klees S, et al. Longitudinal study of the contamination of air and soil surfaces in the vicinity of pig barns by livestock-associated methicillin-resistant
Staphylococcus aureus. Appl Environ Microbiol 2012; 78:5666-71.
29 Rossney AS, Herra C, Brennan GI, Morgan PM, O’Connell B. Evaluation of the Xpert
methicillin-resistant Staphylococcus aureus (MRSA) assay using the GeneExpert real- time PCR platform for rapid detection of MRSA from screening specimens. J Clin Microbiol 2008; 46: 3285-3290.
30 King MF, Noakes CJ, Sleigh MA, Camargo-Valero MA. Bioaerosol deposition in single and two-bed hospital rooms: a numerical and experimental study. Build Environ 2012;
doi: 10.1016/j.buildenv.2012.09.011. 393
394 395 396
397 398
399 400 401
402 403
404 405 406
407 408
409
410
411
Figure 1a. Schematic layout of ward bays in a typical 35-bed ward
SR, single room 417
418 419
420 421 422
423 424
425 426 427
428 429
430 431 432
Figure 1b, Schematic layout of environmental sampling sites in typical high-dependency bays (ward bay A, 4-bed, ward bay B, 6-bed)
1 1
2/6 2/6
3 3 3 3
4 5 5 4 4 5 5 4
2/6 2/6
2/6 2/6
3 3 3 3
4 5 5 4 4 5 5 4
2/6 2/6
2/6
3 3
4 5 5 4
2/6 Nurses
Station
1, Air sampling 2, Air settle-plate 3, Mattress 4, Pillow
5, Bedrail/bedframe 6, Locker
6-bedded bay (B) 4-bedded bay (A)
434
435 436
437
438
Table 1. Isolation of MRSA from patients and air on 132 sampling occasions
aPatient MRSA + Air MRSA +, among patients who were MRSA+, the number of air sampling MRSA+
bPatient MRSA + Air MRSA -, among patients who were MRSA+, the number of air sampling MRSA-,
cAir MRSA+ and Patient -, among air sampling that was MRSA+, the number of patients MRSA-
d Air +, number of air MRSA-positive in each ward bay 444
445 446 447 448 449 450 451 452 453
454
455
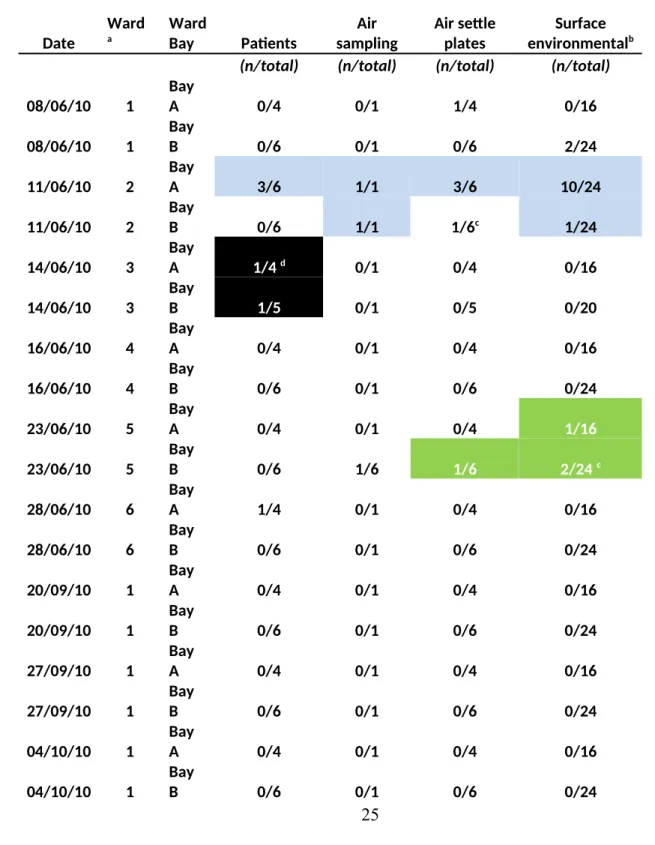
Table 2. The distribution of MRSA recovered from patients, air, settle plates and environmental surfaces on 32 occasions of high-dependency bays with spa typing of 42/52 isolates and DNA microarray profiling of 40/52 isolates
Date Ward a Ward Bay Patients Air sampling Air settle plates Surface environmentalb
(n/total) (n/total) (n/total) (n/total)
08/06/10 1
Bay
A 0/4 0/1 1/4 0/16
08/06/10 1
Bay
B 0/6 0/1 0/6 2/24
11/06/10 2
Bay
A 3/6 1/1 3/6 10/24
11/06/10 2
Bay
B 0/6 1/1 1/6c 1/24
14/06/10 3
Bay
A 1/4 d 0/1 0/4 0/16
14/06/10 3
Bay
B 1/5 0/1 0/5 0/20
16/06/10 4
Bay
A 0/4 0/1 0/4 0/16
16/06/10 4
Bay
B 0/6 0/1 0/6 0/24
23/06/10 5
Bay
A 0/4 0/1 0/4 1/16
23/06/10 5
Bay
B 0/6 1/6 1/6 2/24 c
28/06/10 6
Bay
A 1/4 0/1 0/4 0/16
28/06/10 6
Bay
B 0/6 0/1 0/6 0/24
20/09/10 1
Bay
A 0/4 0/1 0/4 0/16
20/09/10 1
Bay
B 0/6 0/1 0/6 0/24
27/09/10 1
Bay
A 0/4 0/1 0/4 0/16
27/09/10 1
Bay
B 0/6 0/1 0/6 0/24
04/10/10 1
Bay
A 0/4 0/1 0/4 0/16
04/10/10 1
Bay
B 0/6 0/1 0/6 0/24
466
18/10/10 5
Bay
A 0/4 0/1 0/4 0/16
18/10/10 5
Bay
B 0/6 0/1 0/6 0/24
26/10/10 5
Bay
A 1/4 1/1 0/4 0/16
26/10/10 5
Bay
B 2/6 e 1/1 0/6 0/24
08/11/10 5
Bay
A 0/4 0/1 0/4 0/16
08/11/10 5
Bay
B 0/6 0/1 0/6 0/24
04/01/11 7
Bay
A 0/4 1/1 1/4 0/16
04/01/11 7
Bay
B 1/6 1/1 5/6 5/24
10/01/11 7
Bay
A 0/4 0/1 0/4 0/16
10/01/11 7
Bay
B 0/6 1/1 0/6 0/24
31/01/11 8
Bay
A 0/4 0/1 0/4 0/16
31/01/11 8
Bay
B 1/6 0/1 0/6 0/24
21/02/11 8
Bay
A 0/4 0/1 0/4 0/16
21/02/11 8
Bay
B 1/6 0/1 0/6 0/24
Total
8 wards
32
Bays 12/161(7.5%) 8/32(25%) 12/161(7.5%) 21/644(3.3%)
a Wards 1-8
b Mattress, pillow, bedrail/frame or locker. c One isolate not spa typed.
d Using DNA microarray, one t032 spa type isolate lacked the sec & sel gene cluster e Total 2/6 isolates MRSA-positive, one t515 spa type, one t022
Cell shading indicates the combined spa types and DNA microarray profiles of isolates within the four clusters;
spa type t557; DNA microarray profile blaZ , erm (C), sec & sel , egc and IEC B spa
spa type t032, DNA microarray profile blaZ, erm (C) , sec & sel, egc and IEC B 477
478
479