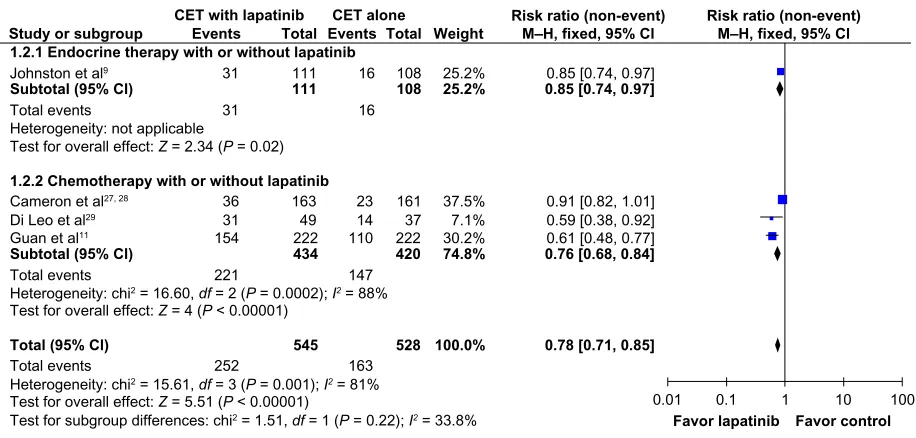
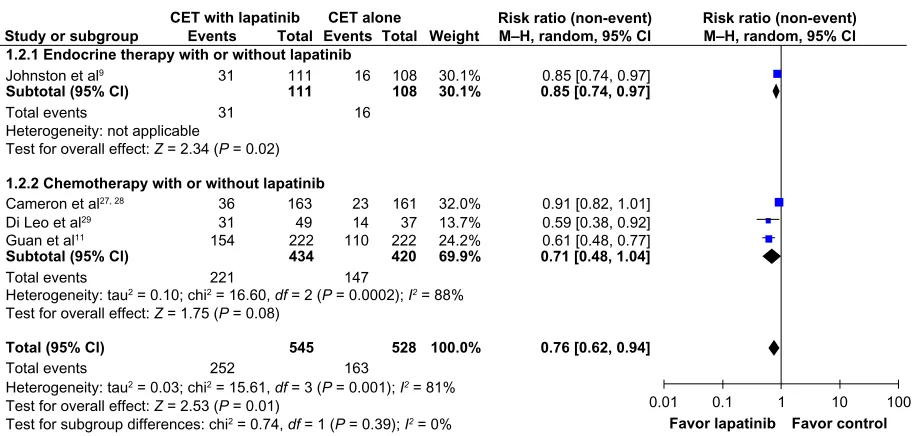
Lapatinib plus chemotherapy or endocrine therapy (CET) versus CET alone in the treatment of HER-2-overexpressing locally advanced or metastatic breast cancer: systematic review and meta-analysis
Full text
Figure


Related documents
The court stated, "We are unable to accept the premise that recovery for inter- ference with the use of land should depend on anything as irrelevant as whether the wing
Running an optimization algorithm for both the internal geometry as well as the thickness of each member to lower the failure indices to those specified in the original
Patients were classified into four groups, according to the intensity of fibrosis and inflammatory findings: group I (mild lobular inflammatory infiltrate with mild or no involvement
disassembling the filter. Unfortunately, most of our design alternatives focused on only one or two aspects of the filter disassembly. In order to better fulfill our design
Although the adjoint field method is meant to be used for retrieving the phase from measured amplitudes in front of a source, a suitable way to test the implementation of the
The firm also employs a full-time pro bono administrator and three full-time pro bono coordinators who work in the firm’s three neighborhood pro bono offices Richmond, Virginia,
The objective of this study was to de- scribe the incidence, patterns, and trends of pediatric mobility aid– related injuries (attributable to the use and misuse of crutches,
