Meta-Analysis of Mitral Valve Repair
Versus Replacement for Mitral Valve
Infective Endocarditis
Michael Tzu Min Wang
1,2, Matthew Haydock
2,3, James Pemberton
2,4, Tom Kai Ming Wang
1,21. Department of Medicine, University of Auckland, Auckland, New Zealand
2. Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, New Zealand 3. Department of Surgery, University of Auckland, Auckland, New Zealand
4. Department of Cardiology, Dunedin Hospital, Dunedin, Auckland Corresponding author:
Dr Tom Kai Ming Wang
Green Lane Cardiovascular Service, Auckland City Hospital Private Bag 92024, Victoria St West, Auckland 1142, New Zealand Email: [email protected]
Introduction
The indications and benefits of mitral valve repair are ingrained in current clinical practice[1, 2]. It is clear that mitral valve repair offers desirable long term profile with freedom from the durability and anticoagulation issues of mitral valve prostheses[3]. Therefore techniques of repair have become an important part of a surgeon’s skill set and as a result the types of repairs and the types of valves deemed suitable for repair are becoming increasingly complex and broad respectively[2].
One example of this is in the setting of infective endocarditis where there are a number of pertinent issues to contend with. Infective endocarditis is a heterogeneous disease with high mortality, and
surgery is frequently indicated for patients with valvular heart failure, uncontrolled infection or embolic prevention[4]. Firstly, there is the primary issue of microbial contamination of the native valve and therefore a desire to minimise the amount of prosthetic material implanted. Secondly, is the degree to which infective processes can disrupt the anatomy of the valve. Finally, the demographics of patients affected by infective endocarditis tend to be different than those affected with other aetiologies of valve dysfunction (i.e. they tend to be include younger patients) [5] and therefore may have more to gain from a successful mitral valve repair. With this in mind the rationale for attempting mitral valve repair in infective endocarditis is clear. However this must
Abstract
Background
Mitral valve repair has superior results to replacement for severe degenerative mitral valve disease, however in the infective endocarditis setting, mixed results have been reported. We compared the outcomes of mitral valve repair and replacement for infective endocarditis in this meta-analysis.
Methods
MEDLINE, Embase and Cochrane databases from 1 January 1980 to 30 June 2018 were searched for original studies. Two authors evaluated these studies for inclusion independently, then data were extracted and pooled.
Results
A total of 4,527 papers was obtained from the search, 121 full-texts were reviewed, and 18 studies which included both mitral valve repair and replacement patients involving 12,339 patients were included for analyses. Pooled rates and odds ratio (95% confidence interval) for operative mortality of repair versus replacement were 4.0% versus 10.5%, 0.37 (0.29-0.48) in 17 studies. Other in-hospital complications of stroke and renal failure were lower for repair than replacement odds ratios 0.65 (0.50-0.84) and 0.42 (0.34-0.52) respectively. Odds ratio for mortality at 1-year (n=4) was 0.31 (0.14-0.72), and at long term follow-up (n=12) was 0.50 (0.41-0.61). There were no differences in long term stroke, recurrent endocarditis and redo-operations (odds ratios 0.55-0.81, P=0.21-0.66). Conclusions
Mitral valve repair is associated with significant reduction in mortality short and long term, as well was in-hospital stroke and renal failure, with similar rates of long-term stroke, recurrent endocarditis and redo-operation rates at long term follow-up compared to replacement for endocarditis. It should be therefore be the preferred strategy for mitral valve endocarditis surgery.
Keywords: Endocarditis, mitral valve surgery, heart valve surgery
Citation: Wang MTM, Haydock M, Pemberton J, Wang TKM. Meta-Analysis of Mitral Valve Repair Versus Replacement for Mitral Valve Infective Endocarditis. International Cardiovascular Forum Journal 2018;13:23-27, DOI: 10.17987/icfj.v13i0.504
ISSN: 2410-2636 © Barcaray Publishing
© 2018 Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution CC-BY-4.0 license CC-BY-4.0 (http://creativecommons.org/ licenses/by/4.0/), which permits use, distribution and reproduction, provided the original work is properly cited. Published by Barcaray (International) Publishing.
be balanced against the likelihood of a successful repair in the long term.
A number of retrospective non-controlled studies have reported on outcomes of mitral valve replacement versus mitral valve repair in the setting of infective endocarditis with mixed results. Therefore a review of literature and meta-analysis was performed with the aim of providing short and medium term outcome data of mitral valve repair and mitral valve replacement in the setting of infective endocarditis.
Materials And Methods
Literature Search
This meta-analysis was conducted following the PRISMA guidelines. Five electronic databases, including MEDLINE, EMBASE, PubMed, Cochrane Central Register for Controlled Trials (CENTRAL), and Web of Science, were searched for original studies from January 1 1980 to June 30 2018. The search terms used were “mitral”, or “mitral valve”; and “repair”, “replacement”, “surgery”, or “operation”; and “endocarditis”, or “infective endocarditis”. The search terms were supplemented with corresponding MeSH terms, where possible. The reference lists of retrieved articles were also screened for potentially relevant studies. Two reviewers (MTMW and TKMW) independently conducted the search and evaluated studies for inclusion. Discrepancies were then resolved by discussion and consensus.
Inclusion and exclusion criteria
Original studies reporting both mitral valve repair and replacement outcomes, with more than twenty adult human subjects total (over 18 years of age), more than ten patients per surgical arm (repair or replacement) and reporting mortality outcomes were eligible for inclusion. Editorials, reviews and expert opinions were excluded.
Data Extraction
Data extraction was conducted independently by two reviewers (MTMW and TKMW), using standardised forms. Discrepancies were resolved by discussion and consensus. Data were extracted on study design, baseline characteristics, and outcome measures. Outcomes of interests include mortality, stroke, recurrent endocarditis and redo-operations at operative (in-hospital or 30 days), 1-year and 5-years where available.
Statistical analysis
Statistical analysis was conducted using Review Manager Version 5.3 (Cochrane Collaboration, Oxford, England). Effect measures for dichotomous data were estimated using odds ratios (OR) with the Mantel-Haenszel statistical method, and weighted mean differences (WMD) used for the analysis of continuous data, with 95% confidence intervals reported for both types of measures, unless otherwise stated. Odds ratios were calculated to represent the odds of an event occurring in the mitral valve repair group compared to the replacement group, with a point estimate of <1.0 indicating a lower event rate in the mitral valve repair group. In order to account for potential clinical diversity and methodology variation between studies, random effects statistical modelling was utilised. The I^2 statistic was used as an indication of the degree in which the total variation across the aggregated studies was a result of heterogeneity instead of chance, and values of >50% were considered to represent considerable heterogeneity. All tests were two tailed and P<0.05 was considered significant.
Results
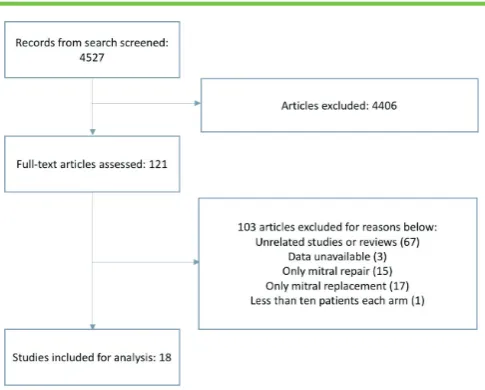
Figure 1 summarizes the study selection process. 4,527 articles were obtained from the literature search. Following
abstract evaluation and exclusion, 121 full-text articles were reviewed. Eighteen studies reporting both mitral valve repair and replacement outcomes, involving 12,339 patients (3,390 repairs, 8,948 replacements), were included for the analyses[6-23]. Table 1 lists the characteristics of included studies. Due to clinical characteristics being inconsistently reported across studies they are not separately reported here.
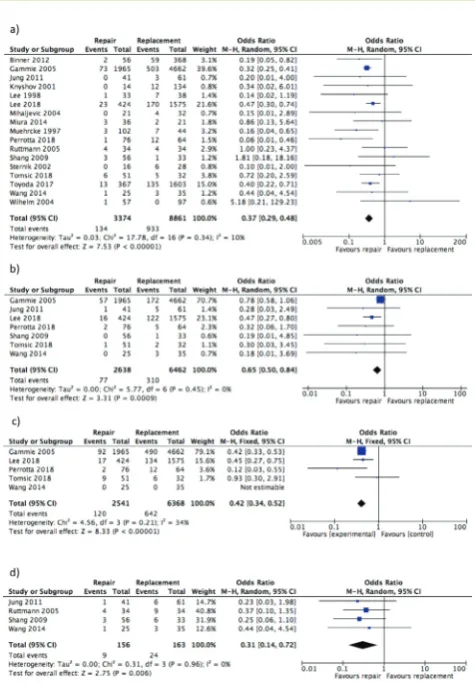
Operative mortality was significantly lower among the mitral valve repair group compared to the replacement group in 17 studies 4.0% versus 10.5%, OR 0.37 (0.29-0.48), P<0.001; figure 2(a). OR (95% confidence intervals) for in-hospital stroke and renal failure were 0.65 (0.50-0.84) in seven studies and 0.42 (0.34-0.52) in five studies respectively in favour of mitral valve repair (figure 2(b)-(c)).
At 1-year follow-up, the mitral valve repair group continued to have significantly lower mortality rates than the replacement group in four studies 5.8% vs. 14.6%, OR 0.31 (0.14- 0.72), p=0.006; figure 2 (d).
Long-term mortality rates were significantly lower in the repair group in twelve studies OR 0.50 (0.41-0.61), P<0.001; figure 3(a). There were no significant differences in the two surgical arms for long-term stroke in five studies, recurrent endocarditis in nine studies and redo operations in ten studies (OR 0.55-0.81 but P=0.21-0.66).
One large study made up just over half of the pooled cohort[7], but excluding this study did not change any of the endpoints, such as the pooled operative mortality odds ratios of the other sixteen studies being 0.41 (0.29-0.57), P<0.001. Funnel plots were symmetrical pyramid in shape for all pooled outcomes, that for operative mortality for example is shown in figure 4. This together with Egger’s statistic of all pooled outcomes having P>0.05 suggest no significant publication bias.
Discussion
A number of studies have demonstrated mixed results for mitral valve repair in endocarditis compared to mitral valve replacement but this is the first meta-analysis of studies which have compared mitral valve repair and replacement cohorts in the setting of infective endocarditis. This study showed that mitral valve repair was superior to replacement for all in-hospital outcomes for mortality and morbidities as well as long term mortality, with
otherwise similar long term outcomes, although it should be noted that the interpretation requires appropriate context. The appeal of surgical repair in the setting of infective endocarditis with respect to long term quality of life is clear[24]. Most of these benefits revolve around avoiding a prosthetic valve and its negatives such as thromboembolism and bleeding with anticoagulation and risk of recurrent endocarditis. However to acquire this benefit mitral valve repair must overcome some hurdles. Specifically, there is the added technical demand and therefore potential to increase the duration of surgery as well as the risk of repair failure or valvular degeneration requiring re-operation.
In this meta-analysis mitral valve repair had significantly lower operative mortality compared to replacement, even with removing the largest study from the analysis [7]. None of the individual studies found a significant operative survival benefit to mitral valve replacement and five studies found a significant survival benefit for mitral valve repair[6, 7, 11, 14, 15, 21]. Similar findings favouring mitral repair for in-hospital complications of stroke and renal failure, both potentially devastating outcomes, were seen. As for all cardiac operations patients must get through the peri-operative period unscathed before considering long term outcomes, so these findings are very promising for mitral repair. The support for mitral repair grows further when exploring long term mortality. Mitral valve repair encouragingly had lower mortality at one year when only four small studies with limited power reported this[8, 16, 17, 22], as well as at five years. One issue of mitral valve repair that must be considered is the risk of repair failure that requires re-operation. In the setting of infective endocarditis this has not been routinely reported. Another reason for adverse outcomes is the failure of excision of all the infected valve tissue leading to infective endocarditis. We did not find higher recurrent endocarditis or redo operation for mitral repair combined, in fact one study found significantly lower rates of both outcomes for repair[14], and nearly all the other studies showed similar rates. These outcomes are encouraging for mitral valve repair in the setting of infective
endocarditis however it should be noted that these important outcomes were only reported in a minority of the studies in this analysis, unlike mortality.
Mitral valve surgery has undergone significant progress with the evolution of techniques of repair[25]. As a result, experience with repairing increasingly complex mitral valve disease has grown with some proponents of mitral valve repair believing that all valves are repairable[26]. Clearly, data and clinical practice regarding mitral valve repair in the setting of endocarditis as opposed to degenerative disease is not unconditionally transferrable and this leads to an important point regarding studies comparing mitral valve repair versus replacement in infective endocarditis. For example the severity and or distribution of tissue destruction that is unique to endocarditis pathology is likely to impact both decision making regarding reparability of a valve and certain outcome measures, although unfortunately this was inconsistently reported across studies. Another important concern is that repair rates continue to be low, making up only about 27% of the entire analysis cohort, and in fact only four studies had repair rates over 50%[13, 15, 17, 20]. Further developments of repair techniques and gaining competence are required to increase repair rates, and it is somewhat promising that three of these high repair rates studies were amongst the five most recent studies in this meta-analysis[13, 15, 20].
This meta-analysis has some limitations. All studies were retrospective and observational which have the potential of biases, especially for patient selection for surgical strategy. Differences in baseline characteristics between surgical arms are expected but were inconsistently reported across studies to report and analyse, including meta-regression cannot be performed. This lack of patient-level data also meant we could not pool longitudinal outcomes as hazards ratio or time to endpoint measures. There were heterogeneity across the studies in terms of study design and outcomes recorded, and they were somewhat chronologically diverse. Although this was a meta-analysis, analysis of infrequent outcomes remain underpowered. However as with many challenging clinical presentations the Table 1. Characteristics of included studies (repair, replacement)
Article Repair Replacement N Study dates Country Centre Age Male
Binner 2012[6] 56 368 424 1994-2011 Germany Single
Gammie 2005[7] 1965 4662 6627 1994-2003 United States Multiple 56 59.7% Jung 2011[8] 41 61 102 1994-2009 Korea Single 34.4 vs 43.1 46.3%, 54.1%
Knyshov 2001[9] 14 134 148 1982-2000 Ukraine Single 41.7 78.8%
Lee 1998[10] 33 38 71 1987-1994 United
Kingdom Single 61.4 69%
Lee 2018[11] 424 1575 1999 2000-2013 Taiwan Multiple 49.3, 52.4 69.1%, 56.3% Mihaljevic 2004[12] 21 32 53 1992-2002 United States Single 66, 50
Miura 2014[13] 36 21 57 1999-2012 Japan Single 57, 55 75%, 38%
Muehrcke 1997[14] 102 44 146 1985-1995 United States Single 51.9 68% Perrotta 2018[15] 76 64 140 2000-2015 Sweden Single 60, 62 72%, 70% Ruttmann 2005[16] 34 34 68 1992-2004 Austria Single 51.5, 53.2 64.7%, 50.0%
Shang 2009[17] 56 33 89 2002-2007 United States Single 48 67.4%
Sheikh 2009[18] 16 87 104 1978-2004 Canada Single 50 48%
Sternik 2002[19] 16 28 44 1986-1999 United States Single
data and logistical requirement to give robust conclusions are a formidable barrier and therefore meta-analysis of smaller retrospective studies are of substantial value to clarify what would otherwise be anecdotal practice.
In conclusion, this meta-analysis found encouraging and superior outcomes for mitral valve repair compared to replacement for infective endocarditis. The implication is that mitral valve repair, when feasible, should be the preferred strategy for mitral valve endocarditis surgery. We have to be mindful of the limitations of the analysis and manage patient on an individualised basis however, and the next step in this question is perhaps to elucidate the type of patient that is more likely to benefit with mitral valve repair or replacement.
Declarations of interest
The authors declare no conflicts of interest.
Acknowledgements
The authors state that they abide by the “Requirements for Ethical Publishing in Biomedical Journals” [27].
References
1. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Fleisher LA, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2017;70(2):252-89. DOI: 10.1016/j.jacc.2017.03.011.
2. Savage EB, Ferguson TB, Jr., DiSesa VJ. Use of mitral valve repair: analysis of contemporary United States experience reported to the Society of Thoracic Surgeons National Cardiac Database. The Annals of thoracic surgery. 2003;75(3):820-5. DOI: 10.1016/S0003-4975(02)04645-3
3. Braunberger E, Deloche A, Berrebi A, Abdallah F, Celestin JA, Meimoun P, et al. Very long-term results (more than 20 years) of valve repair with carpentier’s techniques in nonrheumatic mitral valve insufficiency. Circulation. 2001;104(12 Suppl 1):I8-11. DOI: 10.1016/S0003-4975(02)04645-3. doi: 10.1161/01.CIR.104.suppl_1.I-8
4. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). European heart journal. 2015;36(44):3075-128. DOI: 10.1093/eurheartj/ehv319.
Figure 4. Funnel plot of included studies pooling and comparing operative mortality
Figure 2. Forest plot of odds ratio of operative (a) mortality, (b) stroke, (c) renal failure and (d) 1-year mortality after mitral valve repair or replacement in patients with infective endocarditis.
5. Hogevik H, Olaison L, Andersson R, Lindberg J, Alestig K. Epidemiologic aspects of infective endocarditis in an urban population. A 5-year prospective study. Medicine. 1995;74(6):324-39.
6. Binner C, Dohmen P, Bittner H, Borger M, Misfeld M, Mohr FW. Late outcome in surgical treatment of infective native mitral valve endocarditis: Repair or Replacement? Thorac cardiovasc surg 2012;60:V108. DOI: 10.1055/s-0031-1297498
7. Gammie JS, O’Brien SM, Griffith BP, Peterson ED. Surgical treatment of mitral valve endocarditis in North America. The Annals of thoracic surgery. 2005;80(6):2199-204. DOI: 10.1016/j.athoracsur.2005.05.036
8. Jung SH, Je HG, Choo SJ, Song H, Chung CH, Lee JW. Surgical results of active infective native mitral valve endocarditis: repair versus replacement. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2011;40(4):834-9. DOI: 10.1016/j. ejcts.2011.01.016.
9. Knyshov GV, Rudenko AV, Vorobyova AM, Atamanyuk MY, Krykunov OA. Surgical treatment of acute infective valvular endocarditis (18 years experience). Journal of cardiac surgery. 2001;16(5):388-91. DOI: 10.1111/ j.1540-8191.2001.tb00539.x.
10. Lee EM, Shapiro LM, Wells FC. Superiority of mitral valve repair in surgery for degenerative mitral regurgitation. European heart journal. 1997;18(4):655-63. 11. Lee HA, Cheng YT, Wu VC, Chou AH, Chu PH, Tsai FC, et al. Nationwide
cohort study of mitral valve repair versus replacement for infective endocarditis. The Journal of thoracic and cardiovascular surgery. 2018. doi: 10.1016/j.jtcvs.2018.04.064.
12. Mihaljevic T, Paul S, Leacche M, Rawn JD, Aranki S, O’Gara PT, et al. Tailored surgical therapy for acute native mitral valve endocarditis. The Journal of heart valve disease. 2004;13(2):210-6.
13. Miura T, Hamawaki M, Hazama S, Hashizume K, Ariyoshi T, Sumi M, et al. Outcome of surgical management for active mitral native valve infective endocarditis: a collective review of 57 patients. General thoracic and cardiovascular surgery. 2014;62(8):488-98. DOI: 10.1007/s11748-014-0377-y. 14. Muehrcke DD, Cosgrove DM, 3rd, Lytle BW, Taylor PC, Burgar AM, Durnwald
CP, et al. Is there an advantage to repairing infected mitral valves? The Annals of thoracic surgery. 1997;63(6):1718-24.
15. Perrotta S, Frojd V, Lepore V, Schersten H, Jeppsson A, Svensson G. Surgical treatment for isolated mitral valve endocarditis: a 16-year single-centre experience. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2018;53(3):576-81. doi:10.1093/ejcts/ezx416
16. Ruttmann E, Legit C, Poelzl G, Mueller S, Chevtchik O, Cottogni M, et al. Mitral valve repair provides improved outcome over replacement in active infective endocarditis. The Journal of thoracic and cardiovascular surgery. 2005;130(3):765-71. DOI: 10.1016/j.jtcvs.2005.03.016.
17. Shang E, Forrest GN, Chizmar T, Chim J, Brown JM, Zhan M, et al. Mitral valve infective endocarditis: benefit of early operation and aggressive use of repair. The Annals of thoracic surgery. 2009;87(6):1728-33; discussion 34. DOI: 10.1016/j.athoracsur.2009.02.098.
18. Sheikh AM, Elhenawy AM, Maganti M, Armstrong S, David TE, Feindel CM. Outcomes of surgical intervention for isolated active mitral valve endocarditis. The Journal of thoracic and cardiovascular surgery. 2009;137(1):110-6. DOI: 10.1016/j.jtcvs.2008.07.033.
19. Sternik L, Zehr KJ, Orszulak TA, Mullany CJ, Daly RC, Schaff HV. The advantage of repair of mitral valve in acute endocarditis. The Journal of heart valve disease. 2002;11(1):91-7; discussion 7-8.
20. Tomsic A, Versteegh MIM, Ajmone Marsan N, van Brakel TJ, Klautz RJM, Palmen M. Early and late results of surgical treatment for isolated active native mitral valve infective endocarditis. Interactive cardiovascular and thoracic surgery. 2018;26(4):610-6. doi:10.1093/icvts/ivx395
21. Toyoda N, Itagaki S, Egorova NN, Tannous H, Anyanwu AC, El-Eshmawi A, et al. Real-world outcomes of surgery for native mitral valve endocarditis. The Journal of thoracic and cardiovascular surgery. 2017;154(6):1906-12. e9. doi: 10.1016/j.jtcvs.2017.07.077.
22. Wang TK, Oh T, Voss J, Gamble G, Kang N, Pemberton J. Valvular repair or replacement for mitral endocarditis: 7-year cohort study. Asian cardiovascular & thoracic annals. 2014;22(8):919-26. DOI: 10.1177/0218492314521613. 23. Wilhelm MJ, Tavakoli R, Schneeberger K, Horstrupp S, Reuthebuch O,
Seifert B, et al. Surgical treatment of infective mitral valve endocarditis. The Journal of heart valve disease. 2004;13(5):754-9.
24. Thourani VH, Weintraub WS, Guyton RA, Jones EL, Williams WH, Elkabbani S, et al. Outcomes and long-term survival for patients undergoing mitral valve repair versus replacement: effect of age and concomitant coronary artery bypass grafting. Circulation. 2003;108(3):298-304. DOI: 10.1161/01. CIR.0000079169.15862.13
25. DiBardino DJ, ElBardissi AW, McClure RS, Razo-Vasquez OA, Kelly NE, Cohn LH. Four decades of experience with mitral valve repair: analysis of differential indications, technical evolution, and long-term outcome. The Journal of thoracic and cardiovascular surgery. 2010;139(1):76-83; discussion -4. DOI: 10.1016/j.jtcvs.2009.08.058.
26. Castillo JG, Anyanwu AC, El-Eshmawi A, Adams DH. All anterior and bileaflet mitral valve prolapses are repairable in the modern era of reconstructive surgery. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2014;45(1):139-45; discussion 45. DOI: 10.1093/ejcts/ezt196.