Differences in Bacterial Vaginosis-associated organisms
among pregnant Foreign-born and US-Born black women
By
Bih Tabah
A Master's Paper submitted to the faculty of the University of North Carolina at Chapel Hill
In partial fulfillment of the requirements for the degree of Master of Public Health in
the Public Health Leadership Program.
Chapel Hill
r
Differences in Bacterial Vaginosis-associated micro-organisms among pregnant US-Born and Foreign-born black women
ABSTRACT
Objectives: The purpose of this study was to determine whether there are
differences in vaginal colonization with bacterial vaginosis (BV) associated
organisms between pregnant US-born and Foreign-born African American
women.
Study Design: We conducted a cross-sectional study on 2890 U.S born and 349
Foreign-born Black women at gestational age of 14.8 ±0.2 weeks. BV and
associated microorganisms were diagnosed by Nugent's criteria.
Results: US-born Black women were more likely to be BV positive
compared to Foreign-born Black women (52% vs. 42.1 %; Pearson's
Chi-Square test: p <0.05). Among women with BV, US born status was
associated with specific vaginal microflora including Gardnerella Vagina/is
(OR 1.6, 95%CI 1.2-2.2); Mobiluncus spp (OR 1.5, 95%CI 1.2-2.2);
Prevotella/Bacteriodes (OR 1.5, 95%CI 1.2-2.2) after adjusting for age,
age of sexual debut, marital status, education, income, number of lifetime
partners, recent douching, recent smoking, receipt of oral within a year of
pregnancy. Among women with BV intermediate status, US born women
were 6 times more likely to have Gardnerel/a vagina/is 95%CI (2.0-17.8);
and 2.5 times more likely to have Mobil uncus. Among women with no BV;
US-born women were 4.0 times more likely to have Mobiluncus 95% Cl
Conclusions: Higher rates of BV and BV associated organisms, especially G
vagina/is and Mobiluncus among US-born black women as compared to
Foreign-born black women, may be a potential contributor to the higher rates of preterm
l
1
l Irr
'
I
I
Introduction
Preterm birth(PTB), defined as delivery before 37 weeks of gestation,
is the second leading cause of death among infants in the United States and
the leading cause of neonatal deaths among African Americans 1. African
American women are twice as likely as Caucasian women to experience
preterm delivery; this disparity has persisted over the past four decades 1-3.
Several studies have demonstrated that foreign-born black women
have better birth outcomes than US born black wornen and similar
outcomes to US-born non-Hispanic Whites4-12. The apparent protective
effect of foreign nativity has been postulated to be due to selective migration
of healthy women or high socioeconomic status and more favorable health
behaviors4· 6· 8• 10• 12. Another plausible explanation is the unique
sociocultural and political background of US-born African Americans
compared to Foreign-born blacks4• 5• 7• 10 . US-born Blacks have experienced long-term exposure to socioeconomic and structural discrimination,
foreign-born women, on the other hand, may not have had similar experiences4• 5· 7· 10
. Psychosocial stress from discrimination, mediated through the weathering hypothesis13 has been associated with adverse pregnancy outcomes among black women14.18.
One possible mechanism which has not been explored in the
literature is the role of maternal infections in pregnancy outcomes of
US-born vs. Foreign-US-born black women.
Tabah 5
Maternal infections have increasingly been associated with adverse
pregnancy outcomes including preterm birth 19-26. There is good evidence in
the medical literature linking preterm birth and systemic and ascending
genital tract infections22· 27• 28 The relationship between genital tract infections and preterm birth is evidenced by the presence of
microorganisms within the chorioamniotic membranes22• 29-33 or between the
decidua and membranes which can penetrate the membranes and infect the
amniotic fluid24· 34-37. It is estimated that intra-amniotic infection may be
responsible for up to 50% of preterm birth occurring before 30 weeks'
gestational age38
The maternal and or fetal inflammatory response to intrauterine
infection is hypothesized to be one of the mechanisms through which
preterm labor is triggered22• 39• 40. Elevated levels of pro inflammatory
mediators such as cytokines, matrix metalloproteinases and white blood
cells have been found in the sera, cervical secretions, and amniotic fluid of
women in preterm labo~2• 3943. Another possible mechanism is the
production of phospholipase A2 and endotoxins by certain bacteria which
stimulate uterine contractions and preterm labor37. These mechanisms are further supported by animal models that have placed live bacterial
organisms or bacterial endotoxins inside animal uterus resulting in a
:i
~
;
i
!
i
"j
~
I
I
I
I
ll
'~ I
Bacterial Vaginosis and Preterm Birth
More than 50 organisms have been associated with intrauterine
infections and preterm labo~2• 35• 3? Some of the micro-organisms
commonly found in the uterus before membrane rupture include
Ureaplasma, Mycoplasma, Gardnerella vagina/is, Mobiluncus,
Peptostreptococcus and Bacteroides 22. It is noteworthy that Mycoplasma, G. vagina/is, Mobiluncus, and Bacteroides are associated with the clinical
syndrome Bacterial Vaginosis (BV)45· 46. Several researchers have found
associations between BV and preterm birth2• 27· 36· 46· 47. In addition, there is
evidence in the literature of an association between preterm delivery and
some of the specific organisms associated with BV, namely the presence of
Mobiluncus species, high concentrations of G. vagina/is or Bacteroides, and
low concentrations of Lactobacillus species, especially the hydrogen
peroxide-producing species.26· 46· 48 While the evidence is unclear on the efficacy of screening for BV in high risk women, there is at least one
meta-analysis which illustrates that screening for BV in a subset of high risk
women may decrease the incidence of preterm birth49.
It is unclear whether there is a difference in vaginal colonization by
BV associated microorganisms between US born and foreign born Black
women. A Medline search using the MESH terms (Bacterial
Vaginosis/Microbiology) or (vaginal flora) AND (pregnancy or pregnancy
complications) AND (African American) OR (Nativity) did not identify any
1
-~
I
'
I
I
i
l
· Tabah 7
vaginosis/organisms during pregnancy and nativity status of African
American Women. The search was limited to articles in English published
after 1990.
This paper will investigate whether there is a difference in rates of BY
and vaginal colonization with BY-associated organisms among pregnant
Foreign-born vs. US-born Black women. Our hypothesis is that US-born
women will have higher rates of BY and BY-associated organisms
compared to Foreign-born women.
Materials and Methods
Study Question/Hypothesis. The purpose of this study is to determine
whether there are differences in vaginal colonization with BY -associated
micro-organisms among pregnant US-born and Foreign-born African
American women. We hypothesized that US-born women will have higher
rates of BY and BY-associated organisms compared to Foreign-born
women.
Study Design and Study Population This is a secondary data analysis of
a longitudinal study of clinical prevalence of maternal stress, BV and
preterm birth, based on women who received prenatal care from public
health centers in Philadelphia and met inclusion criteria for the Stress
Pregnancy Evaluation and Community Project (SPEAC). Included in the
study were women with singleton intrauterine pregnancies, who were
receiving prenatal care at one of eight public health centers in Philadelphia.
The women were recruited, screened and enrolled for participation in the
SPEAC study between February 1, 1999 and April 20 2003, during their first
prenatal care visit at the mean gestational age of 14.8 ± 0.2 weeks. We
conducted our analysis on data from a sample of 3239 African American
women; 89% of whom are US-born and 11% foreign-born. This study was
approved by the Institutional Review Board of the University of North
Carolina Chapel Hill (IRS# 05-PUB/HLTH-1 087).
Specimen collection and processing. Clinical practitioners collected 2
vaginal specimens from each study participant during routine pelvic exam at
initial prenatal visit; one of which was used for gram stain and the other for
wet mount. Practitioners also assessed for the clinical signs of BV including
vaginal discharge, positive whiff-amine test, clue cells on wet mount and
high pH. All the data collected was recorded by study personnel.
BV was diagnosed by Gram-stained vaginal fluid specimens using
Nugent's criteria
5°
Scoring of Gram-stained slides was performed by amicrobiologist who was blinded to clinical findings and demographics of
study participants.
Vaginal morphotypes including large uniform gram-positive rods
(Lactobacillus spp), small pleomorphic gram-variable rods (Gardnerel/a
vagina/is or G Vaginal/is), small gram-negative rods (Prevotel/a/Bacteriodes
1 !
I
!
I
j
l
'
!
I
Tabah 9
quantified over 5 nonadjacent fields under oil immersion (1 OOX
magnification). Each of the morphotypes was quantified on a scale of 0 to 4
based on the number of organisms seen on 5 nonadjacent fields. A
gram-stain score of 1 + was assigned for less than 1 organism per field; 2+ for 1 to
4 per field; 3+ for 5 to 30 per field; and 4+ for more than 30 per field. Using
the Nugent criteria, points were awarded by Gram-stain score based on the
relative proportions of the different bacterial morphotypes; Lactobacillus spp
and G. Vagina/is or Prevotella/Bacteroides spp were awarded points
ranging from 0 to 4 while Mobiluncus spp was scored from 0 to 2.
Lactobacillus was inversely scored with the highest number of morphotypes
awarded the least score e.g. 4+ Lactobacillus assigned 0 points, 3+
Lactobacillus spp assigned 1 point and so on. G. Vagina/is or
Prevotella/Bacteroides spp and Mobiluncus spp were scored by giving those
with the highest number of organism the highest score e.g. 4+ G Vagina/is
or Prevotella/Bacteroides spp. was assigned 4 points and 3 to 4+
Mobiluncus spp was awarded 2 points. Points were totaled to give a score
of 0 to 1 0 using the following formula: Lactobacillus + G vagina/is or
Prevotella/Bacteroides + Mobiluncus = total score. A score of 7-10 was
defined as BV positive, a score of 4 to 6 was defined as BV intermediate
and a score of 0 to 3 was considered normal.
Dependent variables. In this analysis the 2 dependent variables are BV
Gardnerella vagina/is; Mobiluncus species; Prevotella/ Bacteroides species.
BV was categorized using the Nugent criteria: A score of 7-10 was defined
as BV positive, a score of 4 to 6 was defined as BV intermediate and a
score of 0 to 3 was defined as BV negative. Lactobacillus, G Vagina/is,
Mobi/uncus and Prevotella!Bacteriodes Species were coded as positive (1)
if their Gram-stain scores were 1 + and higher and negative (0) if their
Gram-stain scores were equal to 0.
Independent variable. Nativity Status among Black women was coded as a
binary variable, defined as US born or Foreign born. Nativity and race were
determined by asking women in a questionnaire respectively about whether
there were born in the US (yes/no) and their race (Black/African American;
White/Caucasian; Latino; Asian or Pacific Islander).
Covariates. Sociodemographic and behavioral variables that have been identified
in several studies as important risk factors for BV23· 46• 51-60 were assessed in an
interview conducted by trained research staff by a questionnaire. Women were
asked about sociodemographic factors such as maternal age, education, maternal
income, marital status, insurance status and parity; and behavioral risk factors
such as age of sexual debut, number of lifetime partners, douching, oral sex,
recent smoking, and history of sexually transmitted diseases (STD).
Maternal age, a continuous variable, was created from the date of birth of the
f
J
l
I
l
j
Tabah 11
Education, a categorical variable, was defined as the highest grade in school that
was completed. For purposes of analyses, we receded education as a binary
variable, High school graduate/higher (1) or less than high school (0).
Maternal income, a continuous variable, was defined as each study participant's
yearly income which included reported income from all of the following sources:
pay checks, under-the-table/off-the books, Social Security income, Department of
Public Assistance/Aid to Families with Dependent Children checks, food stamps,
unemployment compensation, and money from baby's father, relatives, and
friends. We receded as, a binary variable, Jess that $9800 (2006 Federal Poverty
guideline for a one person household or one person in a family) (1) or greater than
$9800 (0).
Marital status, a categorical variable, was defined as single, married, living as
married. We receded as a binary variable defined as single (1) or married/living as
married (0).
Parity was a continuous variable defined as number of other pregnancies besides
the index pregnancy. We receded as a binary variable, defined as nulliparous(1) or
multiparous(O).
Age of sexual debut was a continuous variable, defined as age at first intercourse.
Number of lifetime partners was a continuous variable, defined as number of
people with whom participants had had vaginal intercourse in their lifetime. We
receded as a binary variable, lifetime partners greater than four (1) or less than or
Douching, a binary variable, was defined as douching the year before getting
pregnant(; yes (1 ), no (0)).
Recent smoking, a binary variable, was defined as smoking the year before
pregnancy (yes(1), no(O)).
Oral sex, a continuous variable, was defined as frequency of receipt of oral sex
the year before current pregnancy. We receded as a binary variable ( receipt of
oral sex of greater than 0 times before current pregnancy (1) or equal to 0 (0)).
History of STD, a binary variable created from receding several binary variables
and defined as presence of at least one of the following STDs: Gonorrhea,
Chlamydia, Trichomonas, Herpes, HIV/AIDS, syphilis or genital warts.
Statistical Analysis. We compared US-born vs. Foreign-born women on
several demographic and behavioral characteristics in order to describe
important similarities and differences between the populations and to
identify possible confounders. The differences between the two groups were
analyzed with Pearson Chi-square tests for categorical variables and
Student
t
tests for continuous variables.We determined if covariates were actual confounders of the relationship
between the independent variable, nativity status and the dependent
variables-- BV and BV-associated microflora (Lactobacillus, Gardnerella
vagina/is; Mobiluncus spp; Prevotel/al Bacteroides spp). We tested each
covariate in separate logistic regressions models. Covariates that had been
I
I
I
I
I
I
~
Tabah 13
and preliminary univariate analysis were included in the models. Parity and
private insurance were not included in the models because there was no
statistically significant variation in parity among US-born and Foreign born
women. For the sake of consistency, we considered covariates potential
confounders if the adjusted OR differed from the crude OR by at least 10%
in at least one of the dependent variables. We eliminated variables which
were not statistically significant in the models (history of BV and history of
STD). Our final model was adjusted for the following: age (continuous); age
at sexual debut (continuous); education (high school graduate or higher
versus less than high school graduate; yearly income (<$9800 vs. >$9800);
number of lifetime sexual partners (>4 vs. <4), douching within a year of
pregnancy (yes/no), smoking within a year of pregnancy (yes/no), and
receipt of oral sex within a year of pregnancy (yes/no).
Multivariate logistic regression analyses were used to determine if there
was an increased odds of colonization with BV and BV associated
microorganisms among US-born women compared to Foreign-born women.
Logistic regression models were adjusted for identified confounders.
Two-sided statistical significance was set at p s; 0.05. All analyses were
conducted using STATA 9.161.
Results
Of the 3243 women included in this analysis, 2890 ( 89%) were US-born
differed between US-born women and Foreign-born women including that
US-born women were more likely to be single, have greater than 4 lifetime
partners, to have smoked within a year of pregnancy, to have douched
recently and to have a history of an STD. US-born women were less likely to
have any education past high school compared to Foreign-born women.
The mean age of US-born women in the sample was 24 years compared to
27 years among Foreign-born women; the mean age of sexual debut for
US-born women was 15 years compared to 17.6 years among Foreign-born
women.
Table II shows the frequency of BV and BV-associated microflora
among US-born and Foreign-born women. Overall, there was a high
prevalence of BV within this study population. Rates of BV varied across
I
the two groups, with US-born women having statistically higher rates compared to Foreign-born women (52% vs. 42.1%; Pearson's Chi-Square test: p <0.05). In addition, US-born women tended to have statisticallysignificant higher rates of colonization with BV-associated organisms
I
I
compared to foreign born women. US-born women had slightly lower rates
'
of Lactobacillus (54.8% vs. 60.7%, Pearson's Chi-Square test: p <0.05) and
l
higher rates of Gardnerella vagina/is (72.8% vs. 59%, Pearson's Chi-Square
· test: p <0.05); Mobi/uncus spp (35.6% vs. 26.4%, Pearson's Chi-Square
test: p <0.05) and Prevotella!Bacteroides spp (69.3% vs. 54.9%, Pearson's
Tabah 15
vaginal colonization with Gardnerella vagina/is was 72.8% among US-born
women compared to 59.0% among Foreign-born women.
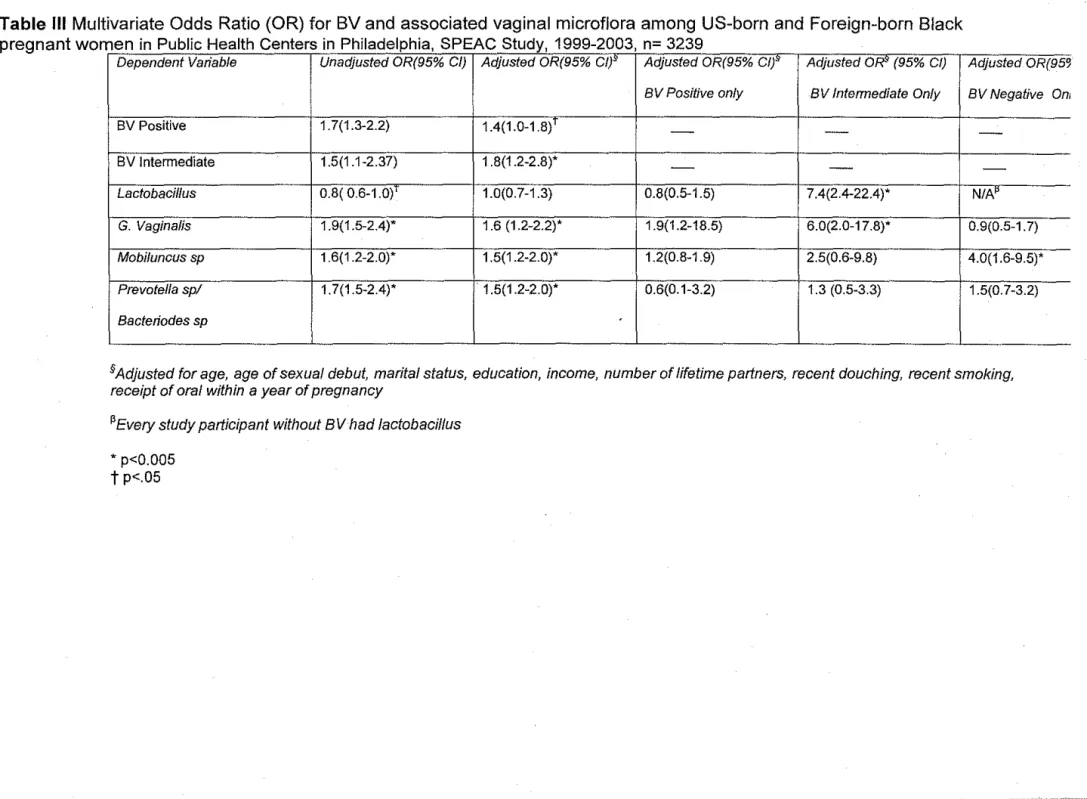
Table Ill shows the unadjusted odds ratio and the 95% confidence
interval for US-born women compared with Foreign-born women who have
colonization with BV and each microorganism. US-born women were 1. 7
times more likely to have BV positive flora (95%CI: 1.3-2.2) compared to
Foreign-born women; and 1.8 times of having BV intermediate flora (95%CI:
1.2-2.8). This association was maintained after adjusting for age, age of
sexual debut, marital status, education, income, number of lifetime partners,
recent douching, recent smoking and receipt of oral within a year of
pregnancy. US born status was associated with specific vaginal microflora
including Gardnerella Vagina/is (OR 1.6, 95%CI: 1.2-2.2); Mobiluncus spp
(OR 1.5, 95%CI: 1.2-2.2); Prevotella!Bacteriodes (OR 1.5, 95%CI 1.2-2.2)
after adjusting for confounders. US born women had lower rates of
Lactobacillus (OR 0.8, 95%CI: 0.6-1.0), however this difference disappeared
after adjusting for confounders (OR 1.0, 95%CI: 0.7-1.3).
To ascertain whether there were nativity differences in the presence
of each morphotype within the group of women classified as having
bacterial vaginosis or not, we stratified by bacterial vaginosis status and
compared the distributions of morphotypes. We conducted subgroup
analyses by stratifying our logistic models by BV status and testing for the
association of BV-associated organisms within nativity status. Among
I
Tabah 16
Gardnerella vagina/is OR 1.9; 95% C (1.2-18.5); and 1.2 times as likely to
have Mobiluncus but this relationship was not statistically significant. Among
women with BV intermediate status, US born women were 6 times more
likely to have Gardnerella vagina/is 95%CI (2.0-17.8); and 2.5 times as likely
to have Mobiluncus compared to foreign-born women. US-born women of
BV intermediate status were 7.4 times as likely to have Lactobacillus (95%
Cl: 2.4-22.4) as BV-negative women. Among women with no BV; US-born
women were 4.0 times more likely to have Mobiluncus 95% Cl (1.6-9.5).
Discussion
Foreign-born women face unique challenges in accessing adequate health
care largely due to economic, legal, linguistic and cultural barriers9. Despite these barriers, foreign born black women have better pregnancy outcomes compared to
their US born counterparts after adjusting for sociodemographic factors and health
status4· 6· 7· 9• 10. The role of maternal infections in this paradox has not been
explored in the literature.
Demba et al (2005) reported BV prevalence of 47.2% among nonpregnant
women in the Gambia52. In that study, the prevalence of BV-associated bacteria
were: G vagina/is 44.4%; Prevotella!Bacteroides 31.9%; 15.2%; Peptostretococcus
1.5%; Mobiluncus 0%; other anaerobes 3.1%52. While Dovender et al (1995)
found BV in 52% of black underprivileged pregnant women in South Africa23 higher than the BV positive rate of 42.1% in our foreign-born cohort.
Our study is the first to investigate whether there are differences in rates of
Tabah 17
American women. Our findings supported our hypothesis that US-born women
have higher rates of BV and BV-associated organisms compared to Foreign-born
women. US-born status was associated with the occurrence of higher rates of BV
positive and BV intermediate flora. US-born women were more likely to have
higher rates of BV-associated microflora. Adjusting for potential confounders did
not erase the association of nativity status and BV and G vagina/is, Mobiluncus
and Prevotella/Bacteroides. Most remarkable, among women with BV intermediate
status, US-born women were 6 times as likely to be colonized with G vagina/is
compared to foreign-born women. Among women with BV negative status,
US-born women were 4 times as likely to be colonized with Mobiluncus compared to
foreign-born women. These findings suggest that US-born women have higher
rates of BV associated organisms irrespective of whether they are BV positive or
not. Royce et al (1999) reported similar findings with a nine fold difference in
colonization with Mobiluncus among black women compared to whites.
Differential exposure to social stressors may be a possible explanation for
the higher prevalence of BV among US-born women. Culhane et al (2001)
reported that chronic social stressors were positively associated with BV among
low-income pregnant women56. US-born blacks have been exposed to unique
psychosocial stressors compared to other ethinic groups in the US62•
Another possible explanation for the difference in rates of BV associated
microflora especially G vagina/is and Mobi/uncus could be differences in the
inflammatory cytokines and toll-like receptor genes. Goepfert et al (2005) reported
compared to white women 53. It will be interesting to investigate if there are
differences in IL-6 among black women by nativity status.
An important limitation to our study is that BV-associated organisms were
identified only on the basis of Gram stain without the use of cultures. This
approach could be problematic because differentiating Gram-variable, pleomorphic
bacillus (G. Vagina/is) from uniform Gram-negative bacillus (Prevotella/Bacteroides
spp) can be difficult and is quite subjective
5°
Our analysis is further limited by theprocess of confounder determination. For the sake of consistency, we included in
our final models covariates which did not significantly alter the crude OR of all our
dependent variables; this approach widened our confidence intervals and
decreased the robustness of our results. In our preliminary analyses, some
variables acted as confounders in the analysis with some of the microorganisms as
dependent variables, while they were not confounders in others. We included any
variable that was identified as a confounder in all sub analyses.
Our study population is not representative of the US population as a whole
as most of the women were low-income inner city residents and at high risk for
sexually transmitted disease. Therefore, our study findings may only be
generalizable to other similar urban settings in the US with populations comparable
to the group of women used in our analysis.
Strengths of our study include the large number of women studied, the use
of consistent data collection protocols and the blinding of our microbiologist to the
clinical findings, demographic and behavioral characteristics of study participants.
1:
tl
II
f
Tabah 19Our review of the medical literature shows that the health outcomes, especially
obstetric outcomes, of Foreign-born black women have received very little
attention. Our study hoped to fill the gaps in the literature. Further research needs
to be done on the role of intermediate BV status on preterm birth and the role if any
of Mobi/uncus and preterm birth among BV negative black women.
The public health importance of our findings is that the presence of BV
increases the risk for adverse obstetric and gynecological diseases including
preterm birth. The increased rates of BV and associated organisms among US
born women may be a significant contributor to the high rates of PTB seen in this
population compared to foreign-born women. It is not known why non BV positive
US born black women have higher rates of BV associated organisms and whether
these higher rates result in higher risk of PTB in this non-BV group. It is possible
that some unidentified physiological factors render this group more susceptible to
colonization with Gardnerella vagina/is and Mobiluncus spp which subsequently
puts them at risk for PTB.
Conclusion
Our findings of higher rates of BV and BV associated organisms especially G
vagina/is and Mobi/uncus among US-born black women as compared to
Foreign-born black women may be potential contributor to the higher rates of preterm birth
seen in the US-born black women. Further research should investigate the
pathogenesis of preterm birth (irrespective of BV status) amongst pregnant
women.
Acknowledgement
I will like to thank Dr Jennifer Culhane for providing me with the data for this
analysis. I will like to thank Dr Vijaya Hogan and Dr Margaret Gourlay for their
expertise and comments during the writing process. I will also like to thank Dr
Julius Atashili for his assistance with the statistical analysis. Finally, thanks to Dr.
Tabah 21
REFERENCES
1. CDC. Centers for Disease Control and Prevention National Center for Health Statistics Percentage of live births with a Gestational Age of <32 weeks and <37 Weeks in Selected Years, by Race (United States). Available at: www.cdc.gov. Accessed 04/06, 2006.
2. Hillier SL, Nugent RP, Eschenbach DA, et al. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. The Vaginal Infections and Prematurity Study Group. N Eng! J Med. Dec 28
1995;333(26):1737-1742.
3. Ananth CV, Joseph KS, Oyelese Y, Demissie K, Vintzileos AM. Trends in preterm birth and perinatal mortality among singletons: United States, 1989 through 2000. Obstet Gynecol. May 2005;105(5 Pt 1):1084-1091.
4. Acevedo-Garcia D, Soobader MJ, Berkman LF. The differential effect offoreign-bom status on low birth weight by race/ethnicity and education. Pediatrics. Jan 2005;115(l):e20-30.
5. Baker AN, Hellerstedt WL. Residential racial concentration and birth outcomes by nativity: do neighbors matter? J Nat! Med Assoc. Feb 2006;98(2): 172-180. 6. Cabral H, Fried LE, Levenson S, Amaro H, Zuckerman B. Foreign-born and
US-born black women: differences in health behaviors and birth outcomes. Am J
Public Health. Jan 1990;80(1 ):70-72.
7. David RJ, Collins JW, Jr. Differing birth weight among infants ofU.S.-born blacks, African-born blacks, and U.S.-born whites. N Eng! J Med. Oct 23 1997;337(17): 1209-1214.
8. Doucet H, Baumgarten M, Infante-Rivard C. Risk of low birthweight and prematurity among foreign-born mothers. Can J Public Health. May-Jun
1992;83(3): 192-195.
9. Forna F, Jamieson DJ, Sanders D, Lindsay MK. Pregnancy outcomes in foreign-born and US-foreign-born women. Int J Gynaecol Obstet. Dec 2003;83(3):257-265.
10. Singh GK, Yu SM. Adverse pregnancy outcomes: differences between US- and foreign-born women in major US racial and ethnic groups. Am J Public Health.
Jun 1996;86(6):837-843.
11. Wasse H, Holt VL, Daling JR. Pregnancy risk factors and birth outcomes in
Washington State: a comparison of Ethiopian-born and US-born women. Am J Public Health. Sep 1994;84(9):1505-1507.
12. Guendelman S, Buekens P, Blonde! B, Kaminski M, Notzon FC, Masuy-Stroobant G. Birth outcomes of immigrant women in the United States, France, and Belgium. Matern Child Health J. Dec 1999;3(4):177-187.
13. Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis. Summer 1992;2(3):207-221.
15. DoleN, Savitz DA, Hertz-Picciotto I, Siega-Riz AM, McMahon MJ, Buekens P. Maternal stress and pretenn birth. Am J Epidemiol. Jan 1 2003;157(1):14-24.
16. DoleN, Savitz DA, Siega-Riz AM, Hertz-Picciotto I, McMahon MJ, Buekens P. Psychosocial factors and pretenn birth among African American and White women in central North Carolina. Am J Public Health. Aug
2004;94(8):1358-1365.
17. Hobel C, Culhane J. Role of psychosocial and nutritional stress on poor pregnancy outcome. J Nutr. May 2003;133(5 Suppl2):1709S-1717S.
18. Rich-Edwards JW, Grizzard TA. Psychosocial stress and neuroendocrine mechanisms in pretenn delivery. Am J Obstet Gynecal. May 2005;192(5
Suppl):S30-35.
19. Carey JC, KlebanoffMA. Is a change in the vaginal flora associated with an increased risk ofpretenn birth? Am J Obstet Gynecal. Apr
2005;192(4):1341-1346; discussion 1346-1347.
20. Goldenberg RL, Andrews WW. Intrauterine infection and why pretenn
prevention programs have failed. Am J Public Health. Jun 1996;86(6):781-783.
21. Goldenberg RL, Culhane JF. Infection as a cause of pretenn birth. Clin Perinatal. Dec 2003;30(4):677-700.
22. Goldenberg RL, Culhane JF, Johnson DC. Maternal infection and adverse fetal and neonatal outcomes. Clin Perinatal. Sep 2005;32(3):523-559.
23. Govender L, Hoosen AA, Moodley J, Moodley P, Sturm A W. Bacterial vaginosis and associated infections in pregnancy.Int J Gynaecal Obstet. Oct
1996;55(1):23-28.
24. Hillier SL, Krohn MA, Kiviat NB, Watts DH, Eschenbach DA. Microbiologic causes and neonatal outcomes associated with chorioarunion infection. Am J Obstet Gynecal. Oct 1991;165(4 Pt 1):955-961.
25. Krohn MA, Hillier SL, Nugent RP, et al. The genital flora of women with intraamniotic infection. Vaginal Infection and Prematurity Study Group. J Infect Dis. Jun 1995;171(6):1475-1480.
26. McDonald HM, O'Loughlin JA, Jolley PT, Vigneswaran R, McDonald PJ. Changes in vaginal flora during pregnancy and association with pretenn birth. J Infect Dis. Sep 1994; 170(3):724-728.
27. Goldenberg RL, Hauth JC, Andrews WW. Intrauterine infection and pretenn delivery. N Eng! J Med May 18 2000;342(20):1500-1507.
28. Lockwood CJ, Kuczynski E. Markers of risk for pretenn delivery. J Perinat Me d.
1999;27(1):5-20.
29. Romero R, Chaiworapongsa T, Espinoza J. Micronutrients and intrauterine infection, pretenn birth and the fetal inflammatory response syndrome. J Nutr.
May 2003; 133(5 Suppl 2): 1668S-1673S.
30. Guzick DS, Winn K. The association of chorioarunionitis with pretenn delivery.
Obstet Gynecol. Jan 1985;65(1):11-16.
31. Cassell G HJ, Andrews W, Cutter G, Goldenberg R. Chorioarunion colonization: correlation with gestational age in women delivered following spontaneous labor versus indicated delivery. Am J Obstet Gynecol. 1993;168(425).
Tabah 23
protein in patients with microbial invasion of the amniotic cavity, intra-amniotic inflammation, preterm labor and premature rupture of membranes. J Matern Fetal
Neonatal Med Jan 2003; 13(1 ):2-21.
33. Mueller-Heubach E, Rubinstein DN, Schwarz SS. Histologic chorioamnionitis and preterm delivery in different patient populations. Obstet Gynecol. Apr 1990;75( 4):622-626.
34. Shim SS, Romero R, Hong JS, et al. Clinical significance of intra-amniotic inflammation in patients with preterm premature rupture of membranes. Am J
Obstet Gynecol. Oct 2004;191(4):1339-1345.
35. Romero R, Sirtori M, Oyarzun E, et al. Infection and labor. V. Prevalence, microbiology, and clinical significance of intraamniotic infection in women with preterm labor and intact membranes. Am J Obstet Gynecol. Sep 1989;161(3):817-824.
36. Gravett MG, Hummel D, Eschenbach DA, Holmes KK. Preterm labor associated with subclinical amniotic fluid infection and with bacterial vaginosis. Obstet
Gynecol. Feb 1986;67(2):229-237.
37. Gibbs RS, Romero R, Hillier SL, Eschenbach DA, Sweet RL. A review of premature birth and subclinical infection. Am J Obstet Gynecol. May
1992; 166(5): 1515-1528.
38. Gravett MG, Navy MJ, Rosenfeld RG, et al. Diagnosis of intra-amniotic infection by proteomic profiling and identification of novel biomarkers. Jama. Jul 28 2004;292( 4):462-469.
39. Andrews WW, Hauth JC, Goldenberg RL, Gomez R, Romero R, Cassell GH. Amniotic fluid interleukin-6: correlation with upper genital tract microbial colonization and gestational age in women delivered after spontaneous labor versus indicated delivery. Am J Obstet Gynecol. Aug 1995;173(2):606-612. 40. Lockwood CJ, Ghidini A, Wein R, Lapinski R, Casal D, Berkowitz RL. Increased
interleukin-6 concentrations in cervical secretions are associated with preterm delivery. Am J Obstet Gynecol. Oct 1994;171(4):1097-1102.
41. Kanayama N, Terao T. The relationship between granulocyte elastase-like activity of cervical mucus and cervical maturation. Acta Obstet Gynecol Scand
1991 ;70(1 ):29-34.
42. Potter NT KL, Bigazzi PE et al. Relationships among cytokines (IL-l, TNF, and IL-8) and histologic markers of acute ascending intrauterine infection. J Matern
Fetal Med. 1992;1(142).
43. Romero R, Ceska M, Avila C, Mazor M, Behnke E, Lindley I. Neutrophil
attractant/activating peptide-1/interleukin-8 in term and preterm parturition. Am J Obstet Gynecol. Oct 1991;165(4 Pt 1):813-820.
44. Gravett MG, Witkin SS, Haluska OJ, Edwards JL, Cook MJ, Navy MJ. An experimental model for intraamniotic infection and preterm labor in rhesus monkeys. Am J Obstet Gynecol. Dec 1994;171(6):1660-1667.
46. HolstE, Goffeng AR, Andersch B. Bacterial vaginosis and vaginal
microorganisms in idiopathic premature labor and association with pregnancy outcome. J Clin Microbial. Jan 1994;32(1 ): 176-186.
47. McGregor JA, French JI, Seo K. Premature rupture of membranes and bacterial vaginosis. Am J Obstet Gynecol. Aug 1993;169(2 Pt 2):463-466.
48. McGregor JA, French JI, Richter R, eta!. Antenatal microbiologic and maternal risk factors associated with prematurity. Am J Obstet Gynecol. Nov 1990;163(5 Pt
I): 1465-14 73.
49. Kiss H, Petricevic L, Husslein P. Prospective randomised controlled trial of an infection screening programme to reduce the rate ofpreterm delivery. Bmj. Aug
14 2004;329(7462):371.
50. Nugent RP KM, Hillier SL. Reliablility of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbial.
1991 ;29:297-30 I.
51. Culhane JF, Nyirjesy P, McCollum K, Goldenberg RL, Gelber SE, Cauci S. Variation in vaginal immune parameters and microbial hydrolytic enzymes in bacterial vaginosis positive pregnant women with and without Mobiluncus species. Am J Obstet Gynecol. Apr 25 2006.
52. Demba E, Morison L, van der Loeff MS, et a!. Bacterial vaginosis, vaginal flora patterns and vaginal hygiene practices in patients presenting with vaginal
discharge syndrome in The Gambia, West Africa. BMC Infect Dis. 2005;5(1):12.
53. Fiscella K, KlebanoffMA. Are racial differences in vaginal pH explained by vaginal flora? Am J Obstet Gynecol. Sep 2004;191(3):747-750.
54. Goldenberg RL, KlebanoffMA, Nugent R, Krohn MA, Hillier S, Andrews WW. Bacterial colonization of the vagina during pregnancy in four ethnic groups. Vaginal Infections and Prematurity Study Group. Am J Obstet Gynecol. May
1996; 174(5): 1618-1621.
55. Hillier SL, Krohn MA, Nugent RP, Gibbs RS. Characteristics ofthree vaginal flora patterns assessed by gram stain among pregnant women. Vaginal Infections and Prematurity Study Group. Am J Obstet Gynecol. Mar 1992;166(3):938-944.
56. Culhane JF, Rauh V, McCollum KF, Hogan VK, Agnew K, WadhwaPD.
Maternal stress is associated with bacterial vaginosis in human pregnancy. Matern Child Health J Jun 2001;5(2):127-134.
57. Culhane JF, Rauh V, McCollum KF, Elo IT, Hogan V. Exposure to chronic stress and ethnic differences in rates of bacterial vaginosis among pregnant women. Am
J Obstet Gynecol. Nov 2002;187(5):1272-1276.
58. Pereira L, Culhane J, McCollum K, Agnew K, Nyirjesy P. Variation in microbiologic profiles among pregnant women with bacterial vaginosis. Am J Obstet Gynecol. Sep 2005;193(3 Pt 1):746-751.
59. Royce RA, Jackson TP, Thorp JM, Jr., eta!. Race/ethnicity, vaginal flora patterns, and pH during pregnancy. Sex Transm Dis. Feb 1999;26(2):96-102.
60. Taha TE, Hoover DR, Dallabetta GA, eta!. Bacterial vaginosis and disturbances of vaginal flora: association with increased acquisition ofHIV. Aids. Sep 10
1998; 12(13): 1699-1706.
61. Stata Statistical Software: Release 9. [computer program]. Version 9. College
Tabah 25
62. James SA. Racial and ethnic differences in infant mortality and low birth weight.
A psychosocial critique. Ann Epidemiol. Mar 1993 ;3(2): 130-136.
63. Goepfert AR, V amer M, Ward K, et a!. Differences in inflammatory cytokine and
Toll-like receptor genes and bacterial vaginosis in pregnancy. Am J Obstet
Table I Number(%) of US-Born and Foreign-Born Black Pregnant women with selected BV risk factors§, in Public Health Centers in Philadelphia, SPEAC Study, 1999-2003, n= 3239
US Born Foreign Born N=2890 N=349 Demographic factors N % N %
Mean age (yrs± SDoo) 2890 23.9±6.4 n/a 27.2±5.7t Marital Status
Single
I
2,428 84.0 19355.3t Married/living as married 461 16.0 156 44.7 Parity
Nulliparous
I
1,629 58.8 197 57.9 Multiparous 1 '123 41.2 143 42.1 Education
<:High School Graduate
I
1,885 65.3 273 78.7t < High School Graduate 1,004 34.8 74 22.3 Yearly income
<$9800 1,576 54.5 219 62.8t >$9800 1,314 45.5 130 37.3 Private Insurance
Yes
I
949 54.8 51 60.0No 784 45.2 34 40.0
Behavioral Factors
Mean age at sexual debut (yrs±SDoo ) \ 2890 15.2±2.2 n/a 17.6±3.8t Number of lifetime partners
I
>4 1,557 54.2 106 3o.8t
<4
Douched within year of Pregnancy Yes
No
Smoking within year of Pregnancy Yes
No
Oral Sex within year of Pregnancy Yes
No(%) History of BV
Yes No(%)
1,314 1,496 1,392 327 1,959 1,825 1,035 584 2,279
Tabah 27
45.8 138 69.2
51.8 115 33.ot
48.2 234 67.0
32.1 34 9.8t
67.9 314 90.2
63.8 129 37.9t
36.2 211 62.1
20.4 28 8.1t
79.6 319 91.9
History of STD
Yes
I
1,306 45.6 74 21.8tNo 1,556 54.4 265 78.2
Significance test for comparisons based on 2-sample t-test for continuous variables and Pearson's chi-square test for categorical variables. t Significantly different compared with US born women p<0.05
Table II. Frequency of BV and associated vaginal microflora among US-born and Foreign-born Black pregnant women in Public Health Centers in Philadelphia, SPEAC Study, 1999-2003, n= 3239
Dependent Variable
I
US-BornI
Foreign-Born
N % N %
BV Status
Positive 1439 52.0 139 42.1*
Intermediate 402 14.5 42 12.7*
Negative 925 33.4 149 45.2*
Lactobacillus
Yes 1448 54.8 198 60.7*
No 1194 45.2 128 39.3
Gardnerellla Vagina/is
Yes 1919 72.8 191 59.0*
No 718 27.2 133 41.0
Mobiluncus sp
Yes 1031 35.6 92 26.4*
No 1859 64.3 256 73.6
Prevotella sp!Bacteriodes sp
Yes 1828 69.3 178 54.9*
No 808 30.7 146 45.1
* Significantly different compared with US born women p<.05
I
I
I
Tabah 29
Table Ill Multivariate Odds Ratio (OR) for BV and associated vaginal microflora among US-born and Foreign-born Black pregnant women in Public Health Centers in Philadelphia, SPEACStudy. 1999-2003. n= 3239
Dependent Variable Unadjusted OR(95% Cl) Adjusted OR(95% Cl)' Adjusted OR(95% Cl}" Adjusted OR' (95% Cf) Adjusted OR(95~
BV Positive only BV Intermediate Only BV Negative On,
BV Positive 1. 7(1.3-2.2) 1.4(1.0-1.8)1
-
-
-BV Intermediate 1.5(1.1-2.37) 1.8(1.2-2.8)*
-
-
-Lactobacillus 0.8( 0.6-1.0)' 1.0(0.7-1.3) 0.8(0.5-1.5) 7.4(2.4-22.4)* N/A
G. Vagina/is 1.9(1.5-2.4)* 1.6 (1.2-2.2)* 1.9(1.2-18.5) 6.0(2.0-17.8)* 0.9(0.5-1.7)
Mobiluncus sp 1.6(1.2-2.0)* 1.5(1.2-2.0)* 1.2(0.8-1.9) 2.5(0.6-9.8) 4.0(1.6-9.5)*
Prevotel/a sp/ 1.7(1.5-2.4)* . 1.5(1.2-2.0)* 0.6(0.1-3.2) 1.3 (0.5-3.3) 1.5(0.7-3.2)
Bacteriodes sp
§Adjusted for age, age of sexual debut, marital status, education, income, number of lifetime partners, recent douching, recent smoking, receipt of oral within a year of pregnancy
~Every study participant without BV had lactobacillus
* p<0.005
t
p<.05Addendum to Masters Paper
Background
Epidemiology and Diagnosis of BV
BV is the most common form of vaginitis among women of
reproductive age, with a global prevalence of 5% to 60% 1• 2. The
occurrence of BV varies by population studied, with a prevalence of
17 to 19 percent in family-planning or student health clinics3; 24 to 37 percent in sexually transmitted disease clinics4 ; and 10 to 35 percent among pregnant women in the United States5.
BV is characterized by a disturbance in vaginal microflora,
with a reduction in the prevalence and concentration of the normally
occurring lactobacilli (large gram-positive rods) and an overgrowth
of mainly anaerobic bacteria such as Gardnerella vaginal/is (small
pleomorphic Gram-variable rods), Prevotel/a, Bacteriodes (small
gram-negative rods), Mobiluncus species, and Mycoplasma
Hominis, Porphyromonas, Peptostreptococcus species6 .
Clinical diagnostic criteria for BV include 3 of 4 of the 1983 Amsel
et al criteria: vaginal discharge pH>4.5, homogenous discharge
vaginal discharge, amide odor upon mixture with KOH and clue .
cells on wet mounf. The reliability of these signs in clinical practice
has not been evaluated, especially clue cells which are used most
Tabah2
criteria have been developed for diagnosis of BV; namely the
Spiegel et al criteria and the Nugent's criteria8. Comparison of gram stain to the clinical Amsel et al criteria has demonstrated
sensitivities ranging from 62%-97% and specificities from 66% to
95% for Spiegel et al criteria. Meanwhile, using the Nugent et al
criteria has shown a sensitivity of 89% and specificity of 83%8 Thus
the Nugent et al criteria is the preferred method for gram stain
evaluation.
Adverse outcomes associated with BV
BV carries potentially serious complications and is
associated with obstetrics and gynecologic disease. Causal
relations have been established between BV and plasma-cell
endometritis, postpartum fever, post-hysterectomy vaginal-cuff
cellulitis, and postabortal infection4. There may be a relationship between BV and cervical intraepithelial neoplasia9. BV may be a risk factor for HIV acquisition and transmission 10.
BV is a significant contributor to PTB. There is good
evidence that bacterial vaginosis (BV) is associated with adverse
birth outcomes 3-6• 11 ; including up to a two to three fold risk for
contribute to the persistent disparity in preterm birth among African
Americans.
The proposed mechanism of action is through the effects of
prostaglandins and cytokines released during the immunological
response to substances such as endotoxins or peptidoglycans
produced by BV-associated organisms or in response to BV
induced deciduitis and amnionitis 13. However, efforts at prevention of PTB by treatment of BV have yielded mixed results. There is
good evidence that screening for BV in average-risk asymptomatic
pregnant women does not reduce the incidence of preterm birth8• 14•
The evidence is unclear on the efficacy of screening for BV in high
risk women, but there is at least one meta-analysis which illustrates
that screening for BV in a subset of high risk women may decrease
the incidence of preterm birth 15. The 3'd US Preventive Services
Task Force reported insufficient evidence to recommend for or
against screening high-risk pregnantwomen for BV, but
recommends against screening of average-risk asymptomatic
pregnant women 14• The American College of Obstetricians and
Gynecologist reported that "current data do not support the use of
BV screening as a strategy to identify or prevent preterm birth 16. On the other hand, The 2002 Center for Disease Control and
Prevention of STD treatment guidelines recommends that
Tabah4
asymptomatic high risk pregnant women i.e. those who have a
history of a previous preterm delivery 17
BV is not the same syndrome in every woman. Microflora
vary among women who have BV positive status, BV intermediate
status or BV negative status. Investigators have found an
association between preterm delivery and some of the specific
organisms associated with BV, namely the presence of Mobiluncus
species, high concentrations of G. vagina/is or Bacteroides, and low
concentrations of Lactobacillus species, especially the hydrogen
peroxide-producing species18'21. Four studies have reported
differences in the presences of specific morphotypes by race and
ethnicity 12· 20
• 22· 23. Royce et al reported that black women are 9.26 times as likely to have Mobiluncus compared with their white
counterparts20.
Variation in bacterial morphology among African American
women may contribute to the persistent race/ethnic disparity in
preterm delivery and racial/ethnic differences in prevalence of BV.
This microbiologic variation may also explain some of the
inconsistent associations of BV with obstetric and gynecologic
outcomes in the literature and the poor effect of BV treatment on
Systematic Review of the Literature
We conducted a systematic review of the literature to identify
articles which explore variation in BV-associated organisms in
vaginal flora among African American women by nativity status.
The literature search using the MESH terms ( Bacterial
Vaginosis/Microbiology) or (vaginal flora) AND (pregnancy or
pregnancy complications) AND (African American) AND (Nativity)
did not identified any studies which examined the prevalence of BV
among Foreign-born black women of African and Caribbean
descent. Neither did our search produce any studies which
assessed variation vaginal colonization with BV-associated
organism among African American women by nativity status. The
search was limited to articles in English published after 1990.
One article was found which examined vaginal flora patterns
among women in Gambia. This article was included to provide
some background information on BV-associated microorganisms
among women in Africa. We subsequently, refined our search to
review articles which explore the variation in BV-associated
microorganisms among White and Black women.
Selection of Articles
A MEDLINE search was performed using the MESH terms (
Tabah6
Vaginal flora) AND (pregnancy or pregnancy complications) AND
(race/ethnicity). The search was limited to articles with abstracts,
articles in English and studies on Humans only published since
1990.
All abstracts were reviewed by one author (BT), and articles
that focused on variation in BV-associated microorganisms among
White versus Black pregnant and nonpregnant were included.
Articles that focused on variation of prevalence of BV only or that
explored vaginal flora among Asians or Hispanic populations only
were excluded. Articles were also excluded if they focused on
variation in microbial profile among HIV positive women.
Bibliographies were hand-searched, and articles that appeared to
be relevant to our search criteria were reviewed. Case reports,
review articles and editorials were excluded.
Our search resulted in four articles examining BV-associated
microbes among white and black women. One article examined
vaginal flora among black women in the Gambia. The five articles
are presented in Table 1. All the articles used a cross-sectional
design. Three studies examined vaginal flora among pregnant
women. Two studies were performed on nonpregant women.
Appraisal of Literature Exploring BV-associated organism among
Internal Validity Ratings
Table 2 presents quality ratings for each of the five articles
included in the systematic review. The five articles identified in the
search were assigned quality ratings by the primary reviewer
(BNT). Overall judgment of internal validity of the studies was
based on the amount of selection bias, measurement bias and
confounding bias and the strength of the results. Potential for
selection bias, potential for measurement bias, potential for
confounding were assigned ratings of+ to +++ in increasing level of
severity. The strength of the results and overall internal validity of
the studies were assigned quality ratings of poor, fair, good,
excellent.
Selection Bias
Selection bias was evaluated based on whether the source
population was adequately described and whether the study
population was representative of the source population. In addition,
selection criteria of the study population were taken in to
consideration.
Measurement Bias
Measurement bias was evaluated based on means of data
collection and identification of data collectors. Studies received low
scores for bias if the authors adequately described the methods of
Tabah8
used. Reliability and validity of instruments and blinding of
investigators during measurement of outcome was an important
factor in ascribing potential for measurement bias.
Confounding Bias
Confounding bias was evaluated based on whether the
articles named potential confounders and described how each was
controlled for.
Strength of Results
The strength of the results was evaluated based on the
magnitude and direction (point estimate; 95% confidence interval};
statistical significance of the results reported in the articles.
Summary of Internal Validity
The article by Pereira et al23 was assigned an internal validity rating of good because measurement of outcomes and
independent variables was well described and investigators were
blinded during measurement of the outcome; there was however a
high potential for confounding bias because only unadjusted
associations of Mobiluncus to race were reported.
Ness et af2 received a rating of fair for internal validity because of the potential for high measurement bias because the
vaginal specimens were self collected by the study participants and
the gram stains were blinded to demographic and behavioral
characteristics of the study participants.
The article by Goldenberg et al12 received an internal validity rating of excellent because of the low potential for selection bias
and measurement bias and the excellent strength of the results.
The study however; had a moderate potential for confounding bias
because the authors did not adjust for douching; a risk factor for BV
identified in the literature1• 2• 24• 25.
External Validity: Generalizability to other populations
Generalizability of any of the articles to other populations is
very limited to populations outside the respective study population,
because of the highly selective group of women used in the studies
e.g. pregnant women, women of low-SES or women at high risk for
sexually transmitted disease. Demba et al recruited women in the
Gambia; these results in this study can not be generalized to
Foreign-born black women in the US who are of different cultural
Tabah 10
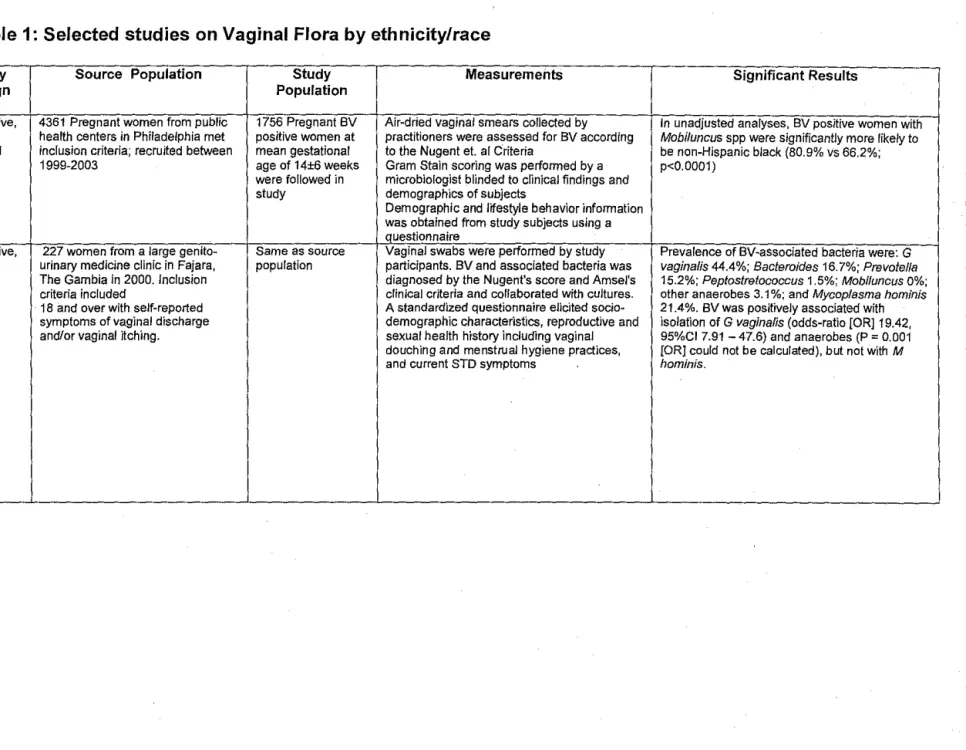
Table 1: Selected studies on Vaginal Flora by ethnicity/race
Study Study Source Population Study Measurements
Authors, Design Population
Year
Pereira, Descriptive, 4361 Pregnant women from public 1756 Pregnant BV Air-dried vaginal smears collected by Culhane, Cross- health centers in Philadelphia met positive women at practitioners were assessed for BV according McCollum, sectional inclusion criteria; recruited between mean gestational to the Nugent et. al Criteria
Agnew, 1999-2003 age of 14±6 weeks Gram Stain scoring was performed by a Nyirjesy were followed in microbiologist blinded to clinical findings and
200523 study demographics of subjects
Demographic and lifestyle behavior information was obtained from study subjects using a questionnaire
Demba, Descriptive, 227 women from a large genito" Same as source Vaginal swabs were performed by study Morison, c urinary medicine clinic in Fajara, population participants. BV and associated bacteria was Van der Loeff, The Gambia in 2000. Inclusion diagnosed by the Nugent's score and Amsel's Awasana, criteria included clinical criteria and collaborated with cultures. Gooding, 1 8 and over with self"reported A standardized questionnaire elicited socio" Bailey, symptoms of vaginal discharge demographic characteristics, reproductive and Mayaud, and/or vaginal itching. sexual health history including vaginal West 200526 douching and menstrual hygiene practices,
and current STD symptoms
Significant Results
In unadjusted analyses, BV positive women with
Mobiluncus spp were significantly more likely to
be non-Hispanic black (80.9% vs 66.2%; p<0.0001)
Prevalence of BV"associated bacteria were: G
vagina/is 44.4%; Bacteroides 16. 7%; Prevofel/a
15.2%; Peptostretococcus 1.5%; Mobiluncus 0%; other anaerobes 3.1 %; and Mycoplasma hominis
21.4%. BV was positively associated with isolation of G vagina/is (odds-ratio [OR] 19.42,
Ness, Hillier, Qualitative Women 13 to 36 years of age 1135 women Study participants self collected vaginal Black race was independently related to lack of
Richter, recruited from five sites located in included in the study specimens using Q~tip cotton swabs. Swabs H202+ lactobacillus (OR 2.0, 95%CI1.4-2.8);'
1
soper, Stam, eastern, southern, and wester analyses were smeared on slides at bedside by study Gardnerella vagina/is (OR 1.9, 95% Cl1.4-2.6); '
I Bass, Sweet, regions of the US in to the GYN staff and Gram stain assessed for BV and Mycoplasma hominis (OR 2.1, 95%CI 1.5-3.1) I
Rice 200322 Infections follow-through (GIFT) associated organisms using Nugent et af Anaerobic Gram negative rods pigmented (OR I
Study criteria. 2.0 95% Cl1.4-2.8) and nonpigmented (OR 1.7, I
Participants were asked about demographic 95%CI1.1-2.5); Mobiluncus (OR 4.5, 95% Cl
2.4-Inclusion: women with a score of information and relevant lifestyle .behaviors in a 8.4)
three points based on an algorithm 20 minute interview
developed by the study investigators Analyses adjusted for clinical site, age,
education, history of trichomoniasis, gravidity, current smoking, sex with menses, hormonal contraceptive use, and douchiQ_g _
Royce, Descriptive, Women enrolled for a study of 842 women at 24 to Vaginal smear specimens were collected Black women were more likely than white women
Jackson, Cross- preterm deflvery-the Pregnancy, 29 weeks' gestation during the routine pelvic exam conducted at to have lactobacilli morphotypes be absent from Thorp, Hillier, sectional Infection and Nutrition (PIN) study. were included in the approximately 28 weeks' gestation Gram their slide specimens (RP 1.39, 95% Cl1.05,
Rabe, PIN participants are recruited study staining was used to evaluate vaginal flora 1.84). Black women were 1.20 times as likely to Pastore, among women attending prenatal using Nugent et al criteria. have G. vagina/is or other small gram~negative
Savitz 199920 care at several public and one Investigators assessing the slides were blinded rods (95% Cl 1.02, 1.41 );
private prenata1 care clinics that to the identity and characteristics of the study
deliver in two large tertiary health participants Black women were 9.0 times as like to have care centers (Wake Medical Center Mobiluncus (OR 9.0 95% Cl3.1-26.3)
in Raleigh and University of North Study participants demographic and behavioral
Carolina Hospitals in Chapel Hill). characteristics were obtained via OR adjusted for age, income, education, marital Only women with single gestations, questionnaire. status, parity, number of sex partners in the 6 ages 16 or older, able to understand months prior to pregnancy, and during the English, and able to give informed pregnancy whether the woman smoked, engaged consent are invited to participate in in sexual intercourse in the past month, had a
the study. sexually transmitted disease {STO) (syphilis,
gonorrhea, chlamydia, or trichomonas) i
diagnosed, douched, and used condoms, foam, i suppositories or the contraceptive sponge.
Goldenberg, Cross- Women recruited for the Vaginal 13,747 Vaginal specimens were collected by Black women were more likely to be colonized Klebanoff, sectional Infections and Prematurity Study predominantly low~ investigators and assessed for BV and with BV associated organism compared to white Nubent, from 1984 to 1989 SES women at 23 microorganisms using the Nugent et al criteria women after adjusting for maternal parity, age, Krohn, Hillier, to 26 1.-V€eks' education, insurance status, marital status, Andrews gestation recruited Data was collected regarding demographic smoking, age, age at first intercourse, and 199612 from seven urban and behavioral characteristics of study number of male partners in last year.
medical center in participants were collected by interview
the·US from 1984 to Bacteroides sp (OR 2.0 95%CI1.8-2.2)
1989 M. hominis (OR 2.2 95%CI 2.0-2.4)
U. urealyticum (OR 1.9 95%CI1.7-2.2)
-Tabah 12
Table II: Quality ratings for studies in systematic review. Each study was rated on a scale of+ to+++ for potential of
bias(+= low,++= moderate,+++= high); Strength of results and overall internal validity were ascribed ratings of poor,
References
I. Morris M, Nicoll A, Simms I, Wilson J, Catchpole M. Bacterial vaginosis: a public health review. Bjog. May 2001;108(5):439-450.
2. JoesoefM SG, London 2001,4:887. Bacterial Vaginosis, In: Clinical evidence.
BMJ Publishing Group. 2001;4(887).
3. Berg AO, Heidrich FE, Fihn SD, eta!. Establishing the cause of genitourinary symptoms in women in a family practice. Comparison of clinical examination and comprehensive microbiology. Jama. Feb 3 1984;251(5):620-625.
4. Hillier S HKK. Bacterial Vaginosis. 2nd ed. New York: McGraw-Hill; 1990. 5. KlebanoffMA, Hillier SL, Nugent RP, eta!. Is bacterial vaginosis a stronger risk
factor for preterm birth when it is diagnosed earlier in gestation? Am J Obstet
Gynecol. Feb 2005;192(2):470-477.
6. Hill G. The microbiology of bacterial vaginosis. Am J Obstet Gynecol. 1993;169(2 Pt 2):450-454.
7. Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med Jan 1983;74(1):14-22.
8. Guise JM, Mahon SM, Aickin M, Helfand M, Peipert JF, Westhoff C. Screening for bacterial vaginosis in pregnancy. Am J Prev Med Apr 2001;20(3
Suppl):62-72.
9. Boyle DC, Smith JR. Infection and cervical intraepithelial neoplasia. Jnt J Gynecol Cancer. May 1999;9(3):177-186.
10. Martin HL, Richardson BA, Nyange PM, eta!. Vaginal lactobacilli, microbial flora, and risk of human immunodeficiency virus type 1 and sexually transmitted disease acquisition. J Irifect Dis. Dec 1999;180(6):1863-1868.
11. Hillier SL, Nugent RP, Eschenbach DA, eta!. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. The Vaginal Infections and Prematurity Study Group. N Eng! J Med Dec 28
1995;333(26):1737-1742.
12. Goldenberg RL, KlebanoffMA, Nugent R, Krohn MA, Hillier S, Andrews WW. Bacterial colonization of the vagina during pregnancy in four ethnic groups. Vaginal Infections and Prematurity Study Group. Am J Obstet Gynecol. May 1996;174(5):1618-1621.
13. Goldenberg RL, Culhane JF, Johnson DC. Maternal infection and adverse fetal and neonatal outcomes. ClinPerinatol. Sep 2005;32(3):523-559.
14. USPSTF. US. Preventive Services Task Force. USPSTF Guidelines: Screening for bacterial vaginosis in pregnancy: Evidence review. 3rd ed. Portland, Oregon:
Oregon Health Sciences University; 2001.
15. Kiss H, Petricevic L, Husslein P. Prospective randomised controlled trial of an infection screening programme to reduce the rate ofpreterm delivery. Bmj. Aug 14 2004;329(7462):371.
Tabah 14
17. CDC. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines. MMWR. 2002;51(No. RR-6).
18. Holst E, Goffeng AR, Andersch B. Bacterial vaginosis and vaginal
microorganisms in idiopathic premature labor and association with pregnancy outcome. J Clin Microbial. Jan 1994;32(1):176-186.
19. McDonald HM, O'Loughlin JA, Jolley PT, Vigneswaran R, McDonald PJ. Changes in vaginal flora during pregnancy and association with preterm birth. J Infect Dis. Sep 1994;170(3):724-728.
20. Royce RA, Jackson TP, Thorp JM, Jr., eta!. Race/ethnicity, vaginal flora patterns, and pH during pregnancy. Sex Transm Dis. Feb 1999;26(2):96-102.
21. McGregor JA, French JI, Richter R, et al. Antenatal microbiologic and maternal risk factors associated with prematurity. Am J Obstet Gynecol. Nov 1990; 163(5 Pt 1):1465-1473.
22. Ness RB, Hillier S, Richter HE, eta!. Can known risk factors explain racial differences in the occurrence of bacterial vaginosis? J Nat! Med Assoc. Mar 2003;95(3):201-212.
23. PereiraL, Culhane J, McCollum K, Agnew K, Nyirjesy P. Variation in microbiologic profiles among pregnant women with bacterial vaginosis. Am J Obstet Gynecol. Sep 2005;193(3 Pt 1):746-751.
24. Taha TE, Gray RH, Kumwenda NI, et a!. HIV infection and disturbances of vaginal flora during pregnancy. J Acquir Immune Defic Syndr Hum Retrovirol.
Jan 1 1999;20(1):52-59.
25. Nugent RP KM, Hillier SL. Reliablility of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbial.
1991 ;29:297-301.
26. Demba E, Morison L, van der LoeffMS, eta!. Bacterial vaginosis, vaginal flora patterns and vaginal hygiene practices in patients presenting with vaginal