www.wjpr.net Vol 4, Issue 05, 2015.
2010
PROSPECTIVE AND RETROSPECTIVE STUDY OF DIABETES AND
ITS COMPLICATIONS
Laxmi Narasimha Gupalli*
Venkateshwara Colony Saroornagar, Rangareddy District, Telangana, Hyderabad, India.
ABSTRACT
Diabetes is the most common cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) in most parts of the world. 20 to
30% of diabetic patient have diabetic nephropathy in type 1 and type 2. Hyperglycemia is the key of nephropathy creation. Hyperglycemia also by production of toxic materials, advanced glycosylated end product (AGE), increased activity of aldose reductase has some role. Some
metabolites of arachidonic acid, hemodynamic derangements and genetic factors have also some role. Although diabetic nephropathy is most common cause of nephropathy in these patients, but diabetic patients are also prone to other urinary tract and renal parenchymal disease and should not be confused with renal failure due to diabetic nephropathy. The principle of treatment of diabetic nephropathy is based on tight control of hyperglycemia, tight control of blood pressure and glomerular pressure, control of dyslipidemia, restriction of protein intake and smoking withdrawal.
KEYWORDS: Hyper glycemia, diabetes mellitus, diabetic nephropathy, Dyslipidemia, aldose reductase, prevalence, complications.
INTRODUCTION
Diabetes mellitus is a metabolic disorder that is characterized by elevated glucose levels.[1] The Continuously elevated glucose levels may result in microvascular (involving the eyes, kidneys and nerves) and macrovascular (involving the heart, blood vessels) complications accelerating the risk of strokes and claudication (pain in extremities due to lack of blood supply)[2] due to which there is a major increase in morbidity and mortality of diabetes and it is estimated to rise from 171 million to 366 million in 2030 worldwide.[3]
Volume 4, Issue 5, 2010-2028. Research Article ISSN 2277– 7105
Article Received on 06 March 2015,
Revised on 29 March 2015, Accepted on 19 April 2015
*Correspondence for Author
Laxmi Narasimha Gupalli
Venkateshwara Colony
Saroornagar, Rangareddy
District, Telangana,
www.wjpr.net Vol 4, Issue 05, 2015.
2011 Kidneys are one of the important organs that are involved in diabetes. Diabetes is the most common cause of endstage renal disease (ESRD) in most parts of the world. Involvement of Kidneys directly and indirectly, increase the involvement of other organs and increase morbidity and mortality in diabetic patients.[1]
Since with untreated diabetic nephropathy, a significant decrease in life expectancy of patients happens; therefore, prevention of this debilitating condition and if there is, early diagnosis and treatment is important.[2]
Due to the increasing industrialization of societies, increased immobility and changes in diet and lifestyle and increasing prevalence of obesity, insulin resistance and type 2 diabetes prevalence is increasing.[1]
Because many of the classic symptoms of diabetes in type 2 diabetes, unlike type 1 Diabetes, do not occur, the importance of screening methods for identifying these patients and screening them for kidney involvement is very important.[3]
One of the most frequently caused complication in diabetes case is chronic kidney failure in both developed and developing countries. Diabetic nephropathy, also known as
Kimmelstiel-Wilson syndrome or nodular diabetic glomerulosclerosis or intercapillary glomerulonephritis, is a clinical syndrome characterized by albuminuria (>300 mg/day or >200 mcg/min) confirmed on at least two occasions 3-6 months apart, permanent and irreversible decrease in glomerular filtration rate (GFR), and arterial hypertension. The syndrome was first described by a British physician Clifford Wilson (1906-1997) and American physician Paul Kimmelstiel (1900-1970) in 1936.[34]
DIABETES
The word "diabetes" is derived from the Greek word meaning "a siphon". A Greek physician, Aretus the Cappadocian, of 2nd-century A.D. named the condition "diabetes." He explained that patients with it had polyuria and "passed water like a siphon." Diabetes mellitus and diabetes insipidus share the name "diabetes" because they are both conditions characterized by excessive urination (polyuria).[18]
DIABETES MELLITUS
www.wjpr.net Vol 4, Issue 05, 2015.
2012 glucose level. In patients with diabetes, the absence or insufficient production of insulin causes hyperglycemia which lead to spillage of glucose into the urine, hence the term sweet urine.[19]
TYPES
There are of different types like Type 1, Type 2, Secondary diabetes and Gestational diabetes.
TYPE 1 DIABETES
Type 1 Diabetes was also called Insulin Dependent Diabetes Mellitus (IDDM) or juvenile onset diabetes mellitus is an autoimmune disease where antibodies are produced against the beta cells of the pancreas by the misdirected immune system or certain viral infections (mumps and Coxsackie viruses) or other environmental toxins. Therefore it can be said that the tendency to develop abnormal antibodies in type 1 diabetes in part is genetically inherited.
Type 1 diabetes occurs in young, lean individuals, usually before 30 years of age. This subgroup is referred to as Latent Autoimmune Diabetes. In Adults (LADA), this is a slow progressive form of type 1 diabetes.[19]
TYPE 2 DIABETES
It is also referred to as Non-Insulin Dependent Diabetes Mellitus (NIDDM), or Adult Onset Diabetes Mellitus (AODM). These patients can produce insulin, which is inadequate for their body's needs since they lack the sensitivity for insulin by the cells of the body (particularly fat and muscle cells).[19]
This form of diabetes usually begins with insulin resistance, a condition where the body
needs more insulin to help glucose enter the cells to generate energy. At first, the pancreas keeps up with the added demand by producing more insulin, but in time the pancreas loses its ability to secrete enough insulin in response to different stimuli. People can develop type 2 diabetes at any age, even during childhood. Now a days type 2 diabetes is more common in childhood than type 1 diabetes majorly due to sedenteric life style.
SECONDARY DIABETES
www.wjpr.net Vol 4, Issue 05, 2015.
2013 GESTATIONAL DIABETES
Elevation of blood sugar levels during pregnancy is called gestational diabetes. Gestational diabetes usually resolves once the baby is born. However, 25 to 50% of women with gestational diabetes will eventually develop Type 2 diabetes later in life, especially in those who require insulin during pregnancy and those who remain overweight after their delivery.[19]
DIABETES INSIPIDUS
Diabetes Insipidus (DI) is a rare disorder that can occur as a consequence of histiocytosis involving the pituitary gland. It should not be confused with the more common diabetes mellitus, also known as sugar diabetes, which results from too much sugar in the blood. Although both disorders have similar symptoms, in every other way including the cause and treatment, they are completely unrelated diseases
PRE-DIABETES
The blood glucose levels are higher than normal but not high enough to diagnose diabetes. These people are prone to develop Type 2 diabetes within 10 years of Pre-diabetic condition. Pre-diabetic patients have an increased risk of heart disease and stroke. With weight loss and physical activity, people with pre-diabetes can prevent type 2 diabetes.[21]
ETIOLOGY
Insufficient production of insulin (either absolutely or relative to the body's needs) or
Production of defective insulin (which is uncommon) or the inability of the cells to use insulin diabetes.[19]
Studies have shown that the appearance of islet cell antibodies often precedes the onset of
clinical diabetes by as much as 3 years, especially Type 1.[22] Other causes include
Genetic predisposition
Poor Diet (Malnutrition Related Diabetes)
Stress
Sedentary Lifestyle
Obesity and Fat Distribution
Drug Induced
www.wjpr.net Vol 4, Issue 05, 2015.
2014
Cushing's syndrome
Acromegaly
MOST PREVALENT COMPLICATION IN DIABETES
The most frequent cause of chronic kidney failure in both developed and developing countries. Diabetic nephropathy, also known as Kimmelstiel-Wilson syndrome or nodular diabetic glomerulosclerosis or intercapillary glomerulonephritis, is a clinical syndrome characterized by albuminuria (>300 mg/day or >200 mcg/min) confirmed on at least two occasions 3-6 months apart, permanent and irreversible decrease in glomerular filtration rate (GFR), and arterial hypertension. The syndrome was first described by a British physician Clifford Wilson (1906-1997) and American physician Paul Kimmelstiel (1900-1970) in 1936.[34]
Diabetic nephropathy is a chronic complication of both type 1 DM (beta cell destruction absolute lack of insulin) and type 2 DM (insulin resistance and/or decreased secretion of insulin).
STAGES OF DIABETIC NEPHROPATHY
There are five stages in the development of diabetic nephropathy.
Stage I
Hypertrophic hyper filtration. In this stage, GFR is either normal or increased. Stage I lasts approximately five years from the onset of the disease. The size of the kidneys is increased by approximately 20% and renal plasma flow is increased by 10%-15%, while albuminuria and blood pressure remain within the normal range.
Stage II
The quiet stage. This stage starts approximately two years after the onset of the disease and is characterized by kidney damage with basement membrane thickening and mesangial proliferation. There are still no clinical signs of the disease. GFR returns to normal values. Many patients remain in this stage until the end of their life.
Stage III
www.wjpr.net Vol 4, Issue 05, 2015.
2015 onset of the disease. Blood pressure may be increased or normal. Approximately 40% of patients reach this stage.
Stage IV
Chronic kidney failure (CKF) is the irreversible stage. Proteinuria develops (albumin > 300 mg/dU), GFR decreases below 60 mL/min/1.73 m2, and blood pressure increases above normal values.
Stage V
Terminal kidney failure (TKF) (GFR < 15 mL/min/1.73 m2). Approximately 50% of the patients with TKF require kidney replacement therapy (peritoneal dialysis, hemodialysis, kidney transplantation)
In the initial stages of diabetic nephropathy, increased kidney size and changed Doppler indicators may be the early morphological signs of renal damage, while proteinuria and GFR are the best indicators of the degree of the damage
In addition to diabetic nephropathy, glomerular sclerosis can also develop in other pathological conditions in patients with DM. These are.
a. dysproteinemia (amyloidosis and other deposit diseases)
b. conditions with chronic ischemia (cyanotic congenital heart disease) c. chronic membranoproliferative glomerulonephritis
d. Idiopathic diseases mostly associated with smoking and increased blood pressure.
PATHOGENESIS
Pathogenesis of diabetic nephropathy is very complicated and results from the interaction of
hemodynamic and metabolic factors.
Glomerular Hyper Filtration
Increased intraglomerular pressure and hyper filtration as early changes in the development of diabetic nephropathy were described by Stadler and Schmidt in 1959.[26] In the 1970's, Mogensen emphasized that as many as 40% newly found DM cases had increased glomerular filtration.
www.wjpr.net Vol 4, Issue 05, 2015.
2016 5. MATERIALS AND METHODOLOGY
5.1 Study Site
Department of Endocrinology, BBR hospitals, balanagar, Hyderabad, Telangana styate
Study Design
Prospective and Retrospective observational, Non-interventional study
Study Period: 6 Months.
5.2. PLAN OF WORK
• Literature Review was carried out • Ethical committee approval
• Collection of data
• Compilation of various patient population with different types of complications in
diabetes undergoing treatment, the dosage regimen used, and complications their management were studied.
• Analysis of data • Report the data.
5.3. PATIENT CASE DETAILS
Total number of cases collected: 150 • INCLUSIVE
Patients in the endocrinology department with diabetes and complications
Patients who are willing to give Verbal informed consent for the study.
EXCLUSIVE
Patients in intensive care units, critical care units and other non selected departments
Patients with previous history of any disorder or toxicity taking any other drug besides
diabetes or its complications are not taken into consideration
5.4. PARAMETERS CONSIDERED FOR ANALYSIS OF DATA COLLECTION
Age wise distribution of patients
Sex wise distribution of patients
Socio economic status wise distribution of patients
Patients by body mass index
www.wjpr.net Vol 4, Issue 05, 2015.
2017
Patients by blood glucose levels
Diabetic patients by presence of micro & macro vascular complications
Different category of drugs priscribed
Patients by type of antibiotics prescribed
Patient by serum creatinine levels
Patients by changes in health related quality of life.
ANALYSIS OF DATA
The data collected from the patients is analysed statistically based upon the parameters presented.
RESULTS
Demographic analysis of data was revealed as follows. I. AGE WISE DISTRIBUTION OF PATIENTS
Table 1: Age Wise Distribution of Cases
3
18
34
51
44
2
12
22.66
34
29.33
0 10 20 30 40 50 60
<20 21-30 31-40 41-49 >50
[image:8.595.150.451.379.718.2]number of patients percentage
Fig 1: Graph On Age Wise Distribution Of Cases
S.No Age
No of patients
n=150
% of distribution
1 <20 3 2
2 21-30 18 12
3 31-40 34 22.66
4 41-49 51 34
www.wjpr.net Vol 4, Issue 05, 2015.
[image:9.595.114.454.88.403.2]2018 II. GENDER WISE DISTRIBUTION OF PATIENTS
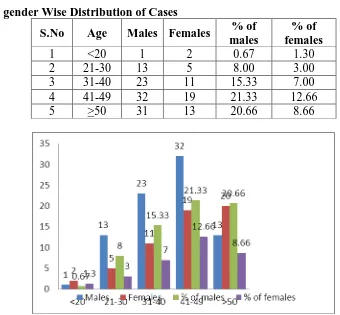
Table 2: gender Wise Distribution of Cases
S.No Age Males Females % of males
% of females
1 <20 1 2 0.67 1.30
2 21-30 13 5 8.00 3.00
3 31-40 23 11 15.33 7.00
4 41-49 32 19 21.33 12.66
5 >50 31 13 20.66 8.66
Fig 2: Graph on gender Wise Distribution of Cases
[image:9.595.129.461.468.755.2]III. SOCIO ECONOMIC STATUS WISE DISTRIBUTION OF PATIENTS Table 3: Socio Economic Status Wise Distribution of Cases
Fig 3:Graph on Socio Economic Status Wise Distribution of Cases
Sl. No Status No of patients n=150
% of distribution
1 Govt. employee 28 18.66
2 Private employee 32 21.33
3 Business man 46 30.66
4 House Wife 26 17.33
www.wjpr.net Vol 4, Issue 05, 2015.
[image:10.595.115.452.96.432.2]2019 IV. DISTRIBUTION OF PATIENTS BY BODY MASS INDEX
Table 4: Distribution of Cases Based On BMI
S.No
Body mass
index Condition
No of patients
n=150
% of distribution
1 <18.5 Under weight 6 4.00
2 18.5-24.9 Normal weight 12 8.00 3 25.0-29.9 Over weight 42 28.00 4 30.0-34.9 Class I obesity 54 36.00 5 35.0-39.9 Class II obesity 12 8.00 6 >40.0 Class III obesity 24 16.00
Fig 4: Distribution of Cases Based on BMI
[image:10.595.147.447.507.746.2]V. DISTRIBUTION OF PATIENTS BY TYPE OF DIABETES
Table 5: Cases Based On Type of Diabetes Diabetes type No. of patients
n=150
% of distribution
Type 1 (IDDM) 3 2.00
Type 2 (NIDDM) 147 98.00
3
147
2
98
0 50 100 150 200
Type 1 (IDDM) Type 2 (NIDDM)
No. of patients n=150 % of distribution
www.wjpr.net Vol 4, Issue 05, 2015.
[image:11.595.135.454.98.426.2]2020 VI. DISTRIBUTION OF PATIENTS BY BODY GLUCOSE LEVELS
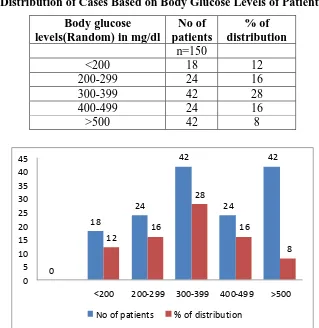
Table No 6: Distribution of Cases Based on Body Glucose Levels of Patients Body glucose
levels(Random) in mg/dl
No of patients
% of distribution n=150
<200 18 12
200-299 24 16
300-399 42 28
400-499 24 16
>500 42 8
0
18
24
42
24
42
12
16
28
16
8
0 5 10 15 20 25 30 35 40 45
<200 200-299 300-399 400-499 >500
No of patients % of distribution
Fig 6: graph ondistribution of cases based on body glucose levels of patients
[image:11.595.74.524.536.653.2]VII. DISTRIBUTION OF DIABETIC PATIENTS BY PRESENCE OF OTHER COMPLICATIONS
Table 7: Distribution Of Diabetic Patients By Presence Of Other Complications
S.No Complications No. of patients n=150 % of distribution
1 Hypertension(HT) 25 16.66
2 Obesity 31 20.66
3 Cancer 8 5
4 Angina 14 9.33
5 Asthma 11 7.33
6 Arthritis 6 4
www.wjpr.net Vol 4, Issue 05, 2015.
[image:12.595.143.454.68.257.2]2021
Fig 7 graph on Distribution of Diabetic Patients By Presence Of Other Complications
[image:12.595.85.517.328.746.2]VIII. DISTRIBUTION OF DIFFERENT CATEGORY OF DRUGS IN PRESCRIPTION
Table 8: Distribution of Different Category of Drugs In Prescription
S.No Drugs category No. of drugs
prescribed n=150
% of distribution
1 Anti diabetic (Insulin) 25 12.5
2 Oral anti diabetic drugs (ODDM) 30 17.5
3 Antibiotics (AB) 45 30
4 Analgesics (AG) 10 10
5 Antipyretic (APY) 5 2.5
6 Anti inflammatory (AI) 7 3.5
7 Anti platelets (AP) 5 7.5
8 Anti allergic (AA) 3 1.5
9 Anticoagulants (AC) 8 4
10 Steroids 2 1
11 Antihypertensive (AH) 2 1
12 B-complex and vitamins (B-C, Vit) 5 7.5
13 Others 3 1.5
www.wjpr.net Vol 4, Issue 05, 2015.
[image:13.595.92.489.75.402.2]2022 IX. DISTRIBUTION OF PATIENT BY SERUM CREATININE LEVELS
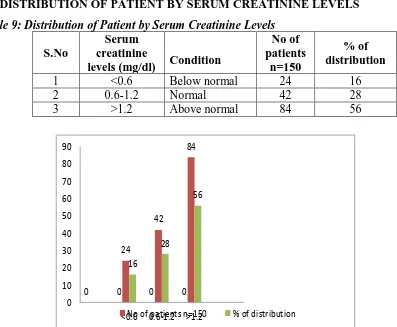
Table 9: Distribution of Patient by Serum Creatinine Levels
S.No
Serum creatinine
levels (mg/dl) Condition
No of patients
n=150
% of distribution
1 <0.6 Below normal 24 16
2 0.6-1.2 Normal 42 28
3 >1.2 Above normal 84 56
0 0 0 0 24 42 84 16 28 56 0 10 20 30 40 50 60 70 80 90
<0.6No of patients n=1500.6-1.2 >1.2 % of distribution
Fig 9 Distribution of Patient by Serum Creatinine Levels
[image:13.595.116.481.487.745.2]X. DISTRIBUTION OF PATIENTS BY CHANGES IN HEALTH RELATED QUALITY OF LIFE
Table 10: Distribution of Patients by Changes In Health Related Quality of Life S.No Physical
functionality Poor Good Excellent
1 Role limitation 12 9 4
2 Mental health 2 16 8
3 General health 12 8 5
4 Social functioning 13 8 4
5 Body pain 9 12 4
Fig 10 distribution of patients by changes in health related quality of life
0 5 10 15 20 No of pa tie nt s
Role lim
itation
Me nta
l healthGeneral hea
lth So
cial func
tioning
Body p
ain
Physical functionality
Distribution by health related quality of life
poor good
www.wjpr.net Vol 4, Issue 05, 2015.
2023 DISCUSSION
Our study was completely an observational study regarding diabetes and its complications prevailing in the present society, because of lack of knowledge among the people, about how it occur and type of diet to be taken.
Most of the diseases like kidney diseases, visual impairment, neurological disorders, heart diseases, occur due to increase in glucose levels in the body (i.e) diabetes. Present survey in American research institute says that cancer also occur due to diabetes which has the capability to change the DNA pattern.
Still in India 40% people are un-aware of diabetes and do not take proper medication or the treatment which inturn leading to major complications like nephropathy.
Therefore, by considering all the factors which contributed to diabetic nephropathy, it was proposed to study the management in diabetic patients like patient counselling, treatment with drugs, duration of treatment and little focus on other complications in diabetes, drug utilization studies.
The prevalence of diabetic complications is reported from the observational study of rural
diabetic subjects in BBR hospital. Logical observational analysis has been used to discovering potential risk factors associated with each complication.
A distinction has been made between time-related variables (age at diagnosis, duration of diabetes, diet related problems, stress related, gender etc..,) and other risk variables. We have attempted to identify the major diet-related and complication related risk variables for each complication and then examined the effect of other risk variables after accounting for the
major complication-related variables.
The important diet-related variables was found to be duration of diabetes for nephropathy,
www.wjpr.net Vol 4, Issue 05, 2015.
2024 After allowing for complication-related variables, the analysis also demonstrates positive independent associations between diabetic control (glycosylated hemoglobin) and nephropathy and between diabetic control and macrovascular disease. Plasma cholesterol (positively) and high-density lipoprotein cholesterol (negatively) were related independently to both macrovascular disease and renal impairment.
CONCLUSION
In the last several years, we have witnessed an enormous progress made not only in our understanding of the risk factors and mechanism of the development of diabetic nephropathy, but also in the treatment possibilities aimed at preventing the progression of diabetic nephropathy.
Early detection of this chronic DM complication along with the treatment of main risk factors (hyperglycemia, hypertension, and dyslipidemia) and use of renoprotective drugs (ACEI and ARB) may decrease the progression of this kidney disease. The treatment of increased blood pressure is a priority. All listed measures lead to a decrease in the overall and cardiovascular mortality in patients with DM.
The principle treatment of diabetic nephropathy is based on tight control of hyperglycemia, tight control of blood pressure and glomerular pressure, control of dyslipidemia, restriction of protein intake and smoking withdrawal and the main important is to follow the good diet and proper exercise daily.
AKNOWLEDGEMENT
We thank all doctors, patients and staff in BBR hospital, balanagar, Hyderabad, telangana state, india for their Fellowship grant support to Dr.Kiran for our work carried for 6 month It is a great pleasure to express our deep sense of gratitude and sincere thanks to our Research Co-coordinator, Dr.Sambasivarao Professor in Pharmaceutical chemistry, Principal of Sri Indu Institute of Pharmacy, Sheriguda, for his valuable suggestions and providing all facilities to carry out our research work successfully.
REFERENCES
www.wjpr.net Vol 4, Issue 05, 2015.
2025 2. Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabetic limb amputation. Basis for
prevention. Diabetes Care., 1990; 13: 513–21.
3. WorldHealth Organization 2010. http://www.who.int/diabetes/facts/world figures/ en/. 4. Vincent Falanga, Wound healing and its impairment in the diabetic foot. Lancet., 2005;
366: 1736–43.
5. Boulton A, Vileikyte L, Ragnarson-Tennvall G, et al. The global burden of diabetic foot disease. Lancet, 2005; 366: 1719.
6. Victor Arana a,Yolanda Paz b, Angélica González c,Verna Méndez d, José D. Méndez e, Healing of diabetic foot ulcers in L-arginine-treated patients. Biomedicine & Pharmacotherapy., 2004; 58: 588–597
7. Diegelmann, R.F., Evans, M.C., 2004. Wound healing: an overview of acute, fibrotic and
delayed healing. Frontiers in Bioscience., 2004; 9: 283–289.
8. DiPietro, L.A., 1995. Wound healing: the role of the macrophage and other immune cells. Shock, 1995; 4: 233–240.
9. Park, H.J, Zhang, Y., Georgescu, S.P., Johnson, K.L., Kong, D., Galper, J.B. Human umbilical vein endothelial cells and human dermal microvascular endothelial cells offer new insights into the relationship between lipid metabolism and angiogenesis. Stem Cell Reviews., 2006; 2: 93–102.
10.Clark, R.A.. Fibrin and wound healing. Annals of NewYork Academy of Sciences., 2001; 936: 355–367.
11.Naguib, G., Al-Mashat, H., Desta, T., Graves, D.T., 2004. Diabetes prolongs the inflam- matory response to a bacterial stimulus through cytokine dysregulation. Journal of Investigative Dermatology., 2004; 123: 87–92
12.Goren, I., Muller, E., Pfeilschifter, J., Frank, S., 2006. Severely impaired insulin signal- ing in chronic wounds of diabetic ob/ob mice: a potential role of tumor necrosis factor-alpha. The American Journal of Pathology., 2006; 168: 765–777.
13.Hehenberger, K., Hansson, A. High glucose-induced growth factor resistance in human
fibroblasts can be reversed by antioxidants and protein kinase C- inhibitors. Cell Biochemistry and Function., 1997; 15: 197–201.
14.Diabetic delayed wound healing and the role of silver nanoparticles, Digest Journal of Nanomaterials and Biostructures., June 2008; 3(2): 49 – 54.
www.wjpr.net Vol 4, Issue 05, 2015.
2026 16.Romer J, Bugge TH, Pyke C, Lund LR, Flick MJ, Degen JL, et al. Impaired wound
healing in mice with a disrupted plasminogen gene. Nat Med., 1996; 2: 287–92.
17.Juhan-Vague I, Roul C, Alessi MC, Ardissone JP, Heim M, Vague P. Increased plasminogen activator inhibitor activity in non insulin dependent diabeticpatients– relationship with plasma insulin. Thromb Haemost., 1989; 61: 370–3
18.Definition of Diabetes, http://www.medterms.com/script/main/art.asp.
19.Diabetes MellitusAuthor: Ruchi Mathur, MD Medical Editor: William C. Shiel, http://www.medicinenet.com/diabetes_mellitus/article.
20.R.S. Satoshkar, S.D. Bhandarkar. A textbook of Pharmacology and Pharmacotherapeutics edition 6. Pg no.
21.Meislin HW, Guisto JA. Marx JA, ed. Rosen's Soft tissue infections Emergency
Medicine: Concepts and Clinical Practice. 6th ed. Philadelphia, PA: Mosby Elsevier; 2006:
22.Roger Walker, Cate Whittlesea, Nirmala N. Red Clinical pharmacy and therapeutics, revised 21st edition chap 135: 630.
23.Epidemiology and prevention of type 2 diabetes and the metabolic syndrome Jonathan E Shaw and Donald J Chisholm MJA., 2003; 179(7): 379-38Series.
24.Dunstan D, Zimmet P, Welborn T, et al. The rising prevalence of diabetes and impaired glucose tolerance: the Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care., 2002; 25: 829-834.
25.Zimmet P, Alberti K, Shaw J. Global and societal implications of the diabetes epidemic. Nature., 2001; 414: 782-787.
26.Carpenter MW, CoustanDR: Criteria for screening tests for gestational diabetes. Am J Obstet Gynecol., 1982; 144: 768–773.
27. Lederer R, Rand JS, Jonsson NN, Hughes IP, Morton JM. Frequency of feline diabetes
mellitus and breed predisposition in domestic cats in Australia. Vet J Dec20 2007. Pathophysiology of diabetes mellitus-algorithm - Caninsulin. American Diabetes
Association: Continuous subcutaneous insulin infusion Position Statement.Diabetes Care 27 (Suppl. 1): S110, 2004 American Diabetes Association: Resource guide 2004.Diabetes Forecast(January):23–RG81, 2004.
www.wjpr.net Vol 4, Issue 05, 2015.
2027 29.Daniel J Moore, Justin M Gregory, Yaa A Kumah-Crystal, et al Mitigating micro- and macro-vascular complications of diabetes beginning in adolescence., November 2009, Volume 2009: 5 Pages 1015 – 1031.
30.Stephanie C Wu et al, Foot ulcers in the diabetic patient, prevention and treatment, Vasc Health Risk Manag, 2007; 3(1): 65-76.
31.Wound and Skin Care Clinical Guidelines April 2007 Chapter 8: Acute Wounds Ramsey SD, Newton K, Blough D, McCulloch DK, Sandhu N, Reiber GE, et al. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care., Mar 1999; 22(3): 382-7.
32.Wound Infection Signs And Preventive Measures. Retrieved on 2010-01- 27.
33.Božidar Vujičić, Tamara Turk, Željka Crnčević-Orlić, Gordana Đorđević and Sanjin Rački 2012 Vujičić et al., licensee InTech.
34.Josephine M. Forbes and Mark E. Cooper, MECHANISMS OF DIABETIC COMPLICATIONS, Physical Rev 93: 137–188, 2013; doi:10.1152/physrev.00045.2011. 35.N. Murugesan , C. Snehalatha , R. Shobhana , G. Roglic , A. Ramachandran,* Awareness
about diabetes and its complications in the general and diabetic population in a city in southern India Diabetes Research and Clinical Practice on., 2007; 77: 433–437.
36.SARAH WILD, MB BCHIR, PHD : GOJKA ROGLIC, MD: ANDERS GREEN, MD, PHD, DR MED SCI : RICHARD SICREE, MBBS, MPH: HILARY KING, MD, DSC: global prevalence of Diabetes in diabetic Care published in., 2004; 27: 1047–1053. 37.Phillip Kantharidis, Bo Wang, Rosemarie M. Carew, and Hui Yao Lan Awareness
Diabetes Complications: The MicroRNA Perspective 1832 DIABETES, VOL. 60, JULY 2011.
38.SUNDARARAMAN SWAMINATHAN, MUHAMMAD G. ALAM, MD, MPH, VIVIAN A. FONSECA, and MD, SUDHIR V. SHAH, MD The role of iron in diabetes and its complications DIABETES CARE, VOLUME 30, NUMBER 7, JULY 2007. 39.George L. King J Periodontol, The role of inflammatory cytokines in diabetes and its
complications, Volume 79 • Number 8 (Suppl.)
40.Mi Young Lee, Dong Seop Choi, Moon Kyu Lee, Hyoung Woo Lee, use of Acarbose and Voglibose in J Korean Med Sci., 2014 Jan; 29(1): 90-97.
www.wjpr.net Vol 4, Issue 05, 2015.
2028 42.P.A. Bakhtiani a, J.ElYoussef a, A.K. Duell a,D.L. Branigan a, P.G. Jacobs b,M.R. Lasarev c, J.R., Factors affecting the success of glucagon delivered during an automated closed-loop system in type 1 diabetes, Journal of Diabetes and Its Complications, 2015; 29: 93–98.
43. Paul Zimmet, K. G. M. M. Alberti, & Jonathan Shaw Global and societal implications of the diabetes epidemic, NATURE | VOL 414 | 13 DECEMBER., 2001.
44.Carol Rees Parrish, R.D., M.S., Cynthia Kupper, Laurie A. Higgins, Combining Diabetes and Gluten-Free Dietary Management Guidelines, THE CELIAC DIET, 2006; 10(101): 56-59.
45.Ron C. Gaba, MD, Raquel Garcia-Roca, MD, and Jose Oberholzer, MD, Pancreatic Islet Cell Transplantation An Update for Interventional Radiologists journal SIR, 2012 J Vasc