Does Lidocaine Gel Alleviate the Pain of Bladder Catheterization in
Young Children? A Randomized, Controlled Trial
Maureen Vaughan, MD*; Elizabeth A. Paton, RN, MSN, CS, NP-C*; Andrew Bush, PhD‡; and Jay Pershad, MD*
ABSTRACT. Objective. Bladder catheterization (BC) is a commonly performed, painful procedure in the pe-diatric emergency department (ED). A survey demon-strated that analgesia is infrequently used for several brief painful procedures, including BC, in pediatric pa-tients. In this study, we evaluated the use of 2% lidocaine gel to alleviate the pain associated with BC in young children (<2 years) in the ED.
Methods. We conducted a randomized, double-blind, placebo-controlled trial comparing pain scores during bladder catheterization with 2% lidocaine gel versus nonanesthetic lubricant. We used a previously validated scale for measuring brief procedure-related pain in pre-verbal children (Face Legs Arms Cry Consolability Pain Scale [FLACC]). A total of 115 patients were recruited; 56 patients were randomized to the control group, and 59 were randomized to the lidocaine group. Lubricant was applied to both the genital mucosa and the catheter. Pain measurements were recorded at 3 time intervals: before insertion of the catheter, during catheterization, and after catheterization. Interobserver reliability had been previ-ously established in an observational pilot study.
Results. The difference in mean FLACC scores be-tween the control (7.55ⴞ2.56) and study groups (7.37ⴞ 2.87) during catheterization was not statistically signifi-cant. The change in FLACC from time 1 (preprocedure) to time 2 (during procedure) was statistically significant in both groups, suggesting that bladder catheterization is a painful procedure.
Conclusions. Altering the standard practice of use of nonanesthetic lubricant with 2% lidocaine gel as lubri-cant during bladder catheterization in young children may not be helpful in alleviating the pain associated with the procedure. Pediatrics 2005;116:917–920; pain management, Lidocaine gel, bladder catheterization, FLACC.
ABBREVIATIONS. ED, emergency department; BC, bladder cath-eterization; FLACC, Face, Legs, Arms, Cry, Consolability Pain Scale.
M
any brief yet painful procedures are per-formed on children in the emergency de-partment (ED) and other areas of the hos-pital every day. A survey of PICUs and NICUs suggested that analgesia is infrequently used for sev-eral procedures, including venipuncture (2%), intra-venous cannulation (10%), suprapubic bladder aspi-ration (8%), and urinary bladder catheterization (BC; 2%).1We also conducted an informal telephonic andelectronic survey of pediatric providers both within the United States and in other countries. The use of anesthetic gel as lubricant during BC for routine diagnostic urine sampling is an infrequent practice and not part of the standard of care in most institu-tions. There are a few dedicated pediatric facilities in the Midwest where 2% lidocaine gel is being used to facilitate pediatric urologic procedures, including BC.2In pediatric centers in the United Kingdom and
Australia, lignocaine gel was being used to facilitate voiding cystourethrograms in the radiology suite.
BC is a commonly performed painful procedure in the pediatric ED. Children experience a moderate amount of pain and distress during this procedure.3,4
Because bag specimens are subject to external con-tamination and yield higher rates of false-positive urine cultures, it is customary to obtain diagnostic urine samples via BC.5 This is especially so in the
preverbal or less verbal child, who may not be toilet trained. Any measure undertaken to alleviate the pain or anxiety of BC would be helpful.
Topical lidocaine, as a component in several prep-arations, is commonly used to reduce the pain as-sociated with repair of mucosal lacerations.6,7 In
prospective studies among adult patients who un-derwent elective urologic procedures, topical lido-caine applied to the genital mucosa was an effective analgesic, with a rapid onset of action, averaging 2.7 minutes.8There is paucity of data in pediatrics on the
effectiveness of lidocaine during BC.2In a
prospec-tive trial, conducted in the pediatric urology clinic, of 20 children who were between the ages of 4 and 11 years and were scheduled to have a urethral catheter inserted for a cystograms, patients were randomized to receive sterile chlorhexidine jelly or 2% lidocaine gel as lubricant. Self-rated pain scores and observer-rated behavioral distress were significantly lower in the lidocaine group than in the placebo group.2We
are not aware of any previous studies that have evaluated the effect of topical lidocaine in reducing
From the *Department of Pediatrics, Division of Emergency Medicine, and ‡Department of Preventive Medicine, University of Tennessee Health Sci-ences Center, Le Bonheur Children’s Medical Center, Memphis, Tennessee. Accepted for publication Jan 18, 2005.
doi:10.1542/peds.2005-0103 No conflict of interest declared.
Reprint requests to (J.P.) Division of Pediatric Emergency Medicine, Le Bonheur Children’s Medical Center, 50 N Dunlap St, Memphis, TN 38103. E-mail: [email protected]
the pain experienced during BC in the preverbal pediatric population.
The current standard of care during BC in our ED is to use nonanesthetic lubricating gel. The purpose of our study was to evaluate the effectiveness of 2% lidocaine gel in alleviating the pain and discomfort of BC in young children.
METHODS
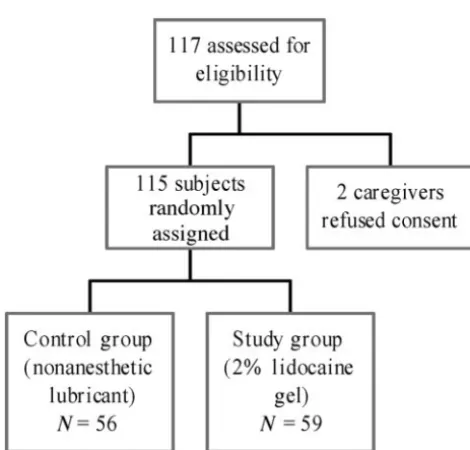
We conducted a randomized, double-blind, placebo-controlled trial over 7 months (July 2003 to January 2004), comparing 2% lidocaine gel with conventional nonanesthetic lubricant (Lubri-gel; Major Pharmaceuticals, Livonia, MI) during BC in children who were younger than 2 years. A total of 115 patients were recruited from a convenience sample of patients who underwent a diagnostic BC in our ED (Fig 1).
The study was set in an urban tertiary care pediatric facility with an annual ED census of 75 000. Our institutional review board approved the study. We excluded patients with an allergy to lidocaine, those with an altered mental status, unstable patients with polytrauma, and toilet-trained children.
One of the 2 investigators (M.V. or B.P.) recruited patients and obtained informed consent from parents. Patients were random-ized using a computer-generated randomization table into 1 of 2 groups. The randomization sequence was maintained in a sealed envelope in our pharmacy department. The lubricant (2% lido-caine gel or nonanesthetic lubricant gel) was provided in num-bered, colorless, 3-mL syringes. Patients were recruited sequen-tially in numeric order. BC was performed using sterile precautions as per standard nursing protocol. Approximately 1 to 2 mL of gel was applied to the genital mucosa for 2 to 3 minutes before catheterization. The remainder of the gel was used as lubricant on the catheter itself. Sterile preparation with povidone iodine (Betadine) solution was performed before catheter inser-tion. Sterility was maintained at all times with care taken to ensure that the tip of the syringe did not come in contact with either the genitals or the catheter.
Procedure-related pain was measured using the Face, Legs, Activity, Cry, Consolability Pain Scale (FLACC).9This is a
previ-ously validated scale for measurement of brief procedural pain in preverbal and cognitively impaired children.10–13FLACC records
the occurrence of 5 behaviors during the medical procedure. The intensity of the behaviors are rated on a scale from 0 to 2 in which 2 indicates maximal anxiety or pain (Table 1). The maximum and minimum possible scores are 10 and 0, respectively. A score ofⱕ2 is generally considered to indicate absence of pain behavior.14
Scores were recorded at 3 intervals. Time 1 was when the patient was placed in lithotomy position during sterile
prepara-tion phase, after gel had been applied to the genital mucosa but before catheter insertion. Time 2 was during insertion of the catheter. Time 3 was 3 to 5 minutes after the procedure, when the patient was in the caregiver’s arms (Table 2). We had initially conducted a prospective observational pilot study of 57 observa-tions on 19 consecutive eligible patients to help to identify the degree of change in the FLACC that may be considered significant and to distinguish preprocedure anxiety-related behaviors from procedural pain. Interobserver reliability of the FLACC during BC was also measured. The mean FLACC scores during the 3 mea-surement phases were 5.9 (⫾3.5), 8.8 (⫾1.6), and 1.6 (⫾1.9), re-spectively. Using repeated measurement analysis of variance, the difference in mean score obtained between times 1 and 2 was statistically significant (P⫽.0001). Interrater reliability, intraclass coefficient (2,1) was high (95% confidence interval: 0.93– 0.99 dur-ing time 1, 0.95– 0.99 durdur-ing time 2, and 0.92– 0.99 at time 3).15
Our null hypothesis was that there was no difference in the mean FLACC scores during the catheterization phase (time 2) between the control and study groups. A priori sample size of 112 was based on the anticipated effect size of 1 point on the FLACC between the 2 groups, at an␣of .05 and power of 90%.
RESULTS
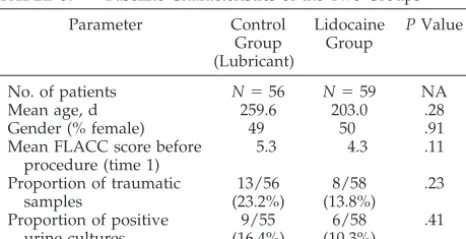
The 2 groups were similar with respect to age, gender, preprocedure pain scores, number of posi-tive urine cultures, and traumatic urine samples (Ta-ble 3). A positive urine culture was defined as 1 or 2 differentiated organisms isolated on culture at a con-centration of 103 or greater colony-forming units/
mL. A traumatic BC was defined as ⬎5 red cells/ high-power field on microscopic examination. The Wilcoxon rank sum test was used to compare scores obtained on the FLACC. The difference in the mean scores between the control and study groups during the procedure was not statistically significant (Table 4).
Using the Wilcoxon signed rank test, the change in the score on the FLACC from time 1 (preprocedure) to time 2 (during procedure) was determined to be statistically significant in both groups (Table 5). This was also consistent with results obtained in our pilot study, suggesting that BC is a painful procedure. Moreover, pain-related behaviors might be distin-guished from non–pain-related (preprocedure anxi-ety) behaviors using the FLACC (Fig 2).
DISCUSSION
Our results suggest that altering the standard prac-tice of using lidocaine gel instead of nonanesthetic lubricant during BC in young children may not be helpful in alleviating the pain during the procedure. However, BC seems to be a painful procedure. Non– pain-related behaviors could be distinguished from procedure-related pain using the FLACC. We are not aware of any previous data addressing the measure-ment of pain during BC in young children⬍2 years of age.
There are several limitations to our study. Our study population was a convenience sample of pa-tients, and potentially eligible patients were not en-rolled. We have no reason to suspect that patients in the ED at times when the investigators were not available would have been different from the study population. Moreover, the 2 study groups were sim-ilar in age, gender, preprocedure pain scores, pro-portion of traumatic urine samples, and positive urine cultures.
Fig 1. Study flow diagram.
Another limitation was that we had nursing per-sonnel of varying experience performing the BC. Be-cause standard nursing protocols for BC are followed at our institution, we do not believe that this would have confounded our results. In addition, there was no difference in the incidence of traumatic catheter-izations or false-positive urine cultures between the 2 groups.
For ensuring maximal effectiveness of analgesia in boys, instilling lidocaine into the penile urethra may have been more effective. This was not usual nursing policy at our institution. Moreover, the added dis-comfort to the patient would have confounded our scores. Although waiting longer than 2 to 3 minutes may have enhanced the analgesic effect of
lido-caine gel, we had to weigh this against holding the young child in lithotomy position after application of the lidocaine gel to the periurethral area to prevent the gel from being displaced from the perineum.
It may be argued that for ensuring accurate mea-surement of time from application of the lubricant to catheterization, a video recording of the entire pro-cedure with independent review of pain behaviors would have been ideal. However, given the anatomic area of the body involved, we had anticipated diffi-culty in obtaining caregiver consent to conduct the study.
There exists the potential for lidocaine toxicity in the doses used for BC in young infants. Before selec-tion of the dose in our protocol, we reviewed the literature on systemic toxicity from topical applica-tion of lidocaine. On the basis of results from studies performed in adult and pediatric patients using top-ical (mucosal) application of lidocaine-based prepa-rations, it was apparent that measured serum lido-caine levels were well below the toxic range.16–20
This was also true when lidocaine was applied to the inflamed mucosa of pediatric bone marrow trans-plant patients with oral mucositis.18Moreover, in an
adult urologic study, instillation of 400 mg of intra-vesical lidocaine for ⬎60 minutes produced serum levels that were 30 times less than the toxic range.17
This is explained by the relatively resistant nature of the transitional epithelium of the genital tract to sys-temic absorption of lidocaine. We selected a volume of 1 to 2 mL of 2% lidocaine gel to permit adequate lubrication and analgesia during catheter insertion. The total dose of lidocaine per kilogram of body weight would be necessary to keep in mind, espe-cially in a young infant or in patients with an in-flamed mucosa or delayed hepatic clearance.
We evaluated 115 patients in our study. On the basis of prestudy estimates, this sample size was large enough to exclude the possibility of a type II error. Although it is possible that smaller differences between the lidocaine and control groups would have become apparent with a larger sample size, it is unlikely that these differences would have been clin-ically meaningful. Also, these differences may not be extrapolated to the non-ED setting.
TABLE 1. FLACC: Behavioral Scale for Rating Pain-Related Behavior in Children
Item Behavior Score
Face Smile or no particular expression 0
Occasional grimace or frown, withdrawn, disinterested 1
Frequent to constant quivering chin, clenched jaw 2
Legs Normal position or relaxed 0
Uneasy, restless, tense 1
Kicking or legs drawn up 2
Activity Lying quietly, normal position, moves easily 0
Squirming, shifting back and forth, tense 1
Arched, rigid, or jerking 2
Cry No cry (awake or asleep) 0
Moans or whimpers, occasional complaint 1
Crying steadily, screams or sobs, frequent complaints 2
Consolability Content, relaxed 0
Reassured by occasional touching, hugging, talking to 1
Difficult to console or comfort 2
TABLE 2. Procedure
Child placed in lithotomy position
Application of lidocaine or nonanesthetic gel
Child remains in supine position but allowed to relax legs Wait time of 2–3 min
Placed in lithotomy position and sterile perineal preparation performed (time 1)
Insertion of catheter (time 2)
Child cleansed and returned to caregiver Wait 3–5 minutes after procedure (time 3)
TABLE 3. Baseline Characteristics of the Two Groups
Parameter Control Group (Lubricant) Lidocaine Group PValue
No. of patients N⫽56 N⫽59 NA
Mean age, d 259.6 203.0 .28
Gender (% female) 49 50 .91
Mean FLACC score before procedure (time 1)
5.3 4.3 .11
Proportion of traumatic samples 13/56 (23.2%) 8/58 (13.8%) .23
Proportion of positive urine cultures 9/55 (16.4%) 6/58 (10.3%) .41
TABLE 4. Comparison of Means and 95% Confidence Inter-vals Around the Mean, Using the FLACC During BC (Time 2) and After the Procedure (Time 3)
Group Control Lidocaine PValue
CONCLUSION
BC in young children is a painful procedure. The pain experienced can be assessed objectively using the FLACC. Substituting lidocaine gel for conven-tional nonanesthetic lubricant during BC may not be helpful in alleviating the procedure pain and discom-fort.
ACKNOWLEDGMENTS
This study was supported by a Le Bonheur Children’s Medical Center “Small Grant.”
We thank the nursing staff of our ED without whom this work would not have been possible.
REFERENCES
1. Bauchne H, May A, Coates E. Use of analgesic agents for invasive medical procedures in pediatric and neonatal intensive care units.J Pe-diatr.1992;121:647– 649
2. Gerard LL, Cooper CS, Duethman KS, Gordley BM, Kleiber CM. Effec-tiveness of lidocaine lubricant for discomfort during pediatric urethral catheterization.J Urol.2003;170:564 –567
3. Merritt KA, Ornstein PA, Spicker B. Children’s memory for a salient medical procedure: implications for testimony.Pediatrics.1994;94:17–23 4. Elder JS, Longenecker R. Premedication with oral midazolam for void-ing cystourethrography in children: safety and efficacy.AJR Am J Roent-genol.1995;164:1229 –1232
5. Al-Orifi F,McGillivray D, Tange S, Kramer MS. Urine culture from bag specimens in young children: are the risks too high?J Pediatr.2000;137: 221–226
6. Smith GA, Strausbaugh SD, Harbeck-Weber C, Cohen DM, Shields BJ, Powers JD. Tetracaine-lidocaine-phenylephrine topical anesthesia com-pared with lidocaine infiltration during repair of mucous membrane lacerations in children.Clin Pediatr (Phila).1998;37:405– 412
7. Pode D, Zylber-Katz E, Shapiro A. Intravesical lidocaine: topical anes-thesia for bladder mucosal biopsies.J Urol.1992;148:795–796 8. van der Burght M, Schonemann NK, Laursen JK, Arendt-Nielsen L,
Bjerring P. Onset and duration of hypoalgesia following application of
lidocaine spray on genital mucosa.Acta Obstet Gynecol Scand.1994;73: 809 – 811
9. Stevens B. Composite measures of pain. In: Finley GA, McGrath PJ, eds.
Measurement of Pain in Infants and Children: Progress in Pain Research and Management. Seattle, WA: IASP Press; 1996:161–178
10. Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S.The FLACC: a behavioral scale for scoring postoperative pain in young children. Pe-diatr Nurs.1997;23:293–297
11. Merkel S, Voepel-Lewis T, Malviya S. Pain assessment in infants and young children: the FLACC scale.Am J Nurs.2002;102:55–58 12. Voepel-Lewis T, Merkel S, Tait AR, Trzcinka A, Malviya S.The
reliabil-ity and validreliabil-ity of the Face, Legs, Activreliabil-ity, Cry, Consolabilreliabil-ity observa-tional tool as a measure of pain in children with cognitive impairment.
Anesth Analg.2002;95:1224 –1229
13. Willis MH, Merkel SI, Voepel-Lewis T, Malviya S. FLACC Behavioral Pain Assessment Scale: a comparison with the child’s self-report.Pediatr Nurs.2003;29:195–198
14. Suraseranivongse S, Santawat U, Kraiprasit K, Petcharatana S, Prakka-modom S, Muntraporn N. Cross-validation of a composite pain scale for preschool children within 24 hours of surgery.Br J Anaesth.2001;87: 400 – 405
15. Vaughan MC, Paton E, Bush A, Pershad J. Measuring Pain During Bladder Catheterization in Young Children. Presented at the American Academy of Pediatrics National Conference & Exhibition; October 31–November 5, 2003; New Orleans, LA
16. Leopold A, Wilson S, Weaver JS, Moursi AM. Pharmacokinetics of lidocaine delivered from a transmucosal patch in children.Anesth Prog.
2002;49:82– 87
17. Birch BR, Miller RA. Absorption characteristics of lignocaine following intravesical instillation.Scand J Urol Nephrol.1994;28:359 –364 18. Elad S, Cohen G, Zylber-Katz E, et al. Systemic absorption of lidocaine
after topical application for the treatment of oral mucositis in bone marrow transplantation patients.J Oral Pathol Med.1999;28:170 –172 19. Vickers ER, Marzbani N, Gerzina TM, McLean C, Punnia-Moorthy A,
Mather L. Pharmacokinetics of EMLA cream 5% application to oral mucosa.Anesth Prog.1997;44:32–37
20. Ameer B, Burlingame MB, Harman EM. Systemic absorption of topical lidocaine in elderly and young adults undergoing bronchoscopy. Phar-macotherapy.1989;9:74 – 81
TABLE 5. Comparison of Mean Change in Scores From Time 1 to Time 2 and from Time 2 to Time 3 in the Two Groups
Control Lidocaine
⌬Time (2–1) 2.25⫾3.22 (median⫽1; IQR⫽4;P⬍.01) 3.06⫾3.1 (median⫽2; IQR⫽5;P⬍.01)
⌬Time (3–2) ⫺4.96⫾2.61 (median⫽ ⫺5; IQR⫽4;P⬍.01) ⫺5.34⫾2.6 (median⫽ ⫺5; IQR⫽3;P⬍.01) IQR indicates interquartile range.
Fig 2. Means of pain values versus time by treat-ment group. y axis, pain score using FLACC (range: 0 –10);xaxis, times 1, 2, and 3 represent-ing preprocedure, durrepresent-ing BC, and after proce-dure.
DOI: 10.1542/peds.2005-0103
2005;116;917
Pediatrics
Maureen Vaughan, Elizabeth A. Paton, Andrew Bush and Jay Pershad
Children? A Randomized, Controlled Trial
Does Lidocaine Gel Alleviate the Pain of Bladder Catheterization in Young
Services
Updated Information &
http://pediatrics.aappublications.org/content/116/4/917 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/116/4/917#BIBL This article cites 18 articles, 1 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2005-0103
2005;116;917
Pediatrics
Maureen Vaughan, Elizabeth A. Paton, Andrew Bush and Jay Pershad
Children? A Randomized, Controlled Trial
Does Lidocaine Gel Alleviate the Pain of Bladder Catheterization in Young
http://pediatrics.aappublications.org/content/116/4/917
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2005 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news