Efficacy of Atomoxetine Versus Placebo in School-Age Girls With
Attention-Deficit/Hyperactivity Disorder
Joseph Biederman, MD*; John H. Heiligenstein, MD‡; Douglas E. Faries, PhD‡; Nora Galil, MD§; Ralf Dittmann, MD, PhD储; Graham J. Emslie, MD¶; Christopher J. Kratochvil, MD#; Harry F. Laws, MD‡;
Kory J. Schuh, PhD‡; and the Atomoxetine ADHD Study Group
ABSTRACT. Objective. The efficacy of atomoxetine was assessed in school-age girls with attention-deficit/ hyperactivity disorder (ADHD). Atomoxetine is a potent inhibitor of the presynaptic norepinephrine transporter with minimal affinity for other noradrenergic receptors or for other neurotransmitter transporters or receptors.
Methods. A total of 291 children who were 7 to 13 years of age and metDiagnostic and Statistical Manual of Mental Disorders, Fourth Editioncriteria for ADHD par-ticipated in 1 of 2 combined, double-blind, placebo-con-trolled, multisite, identical clinical trials. This intent-to-treat subset analysis examined the effects of atomoxetine versus placebo in 51 girls who were randomized to ato-moxetine (nⴝ30) or placebo (nⴝ21) for 9 weeks. ADHD symptoms were assessed using parent- and investigator-rated scales.
Results. Atomoxetine was superior to placebo on the following measures: the Attention-Deficit Hyperactivity Disorder Rating Scale-IV-Parent Version: Investigator Administered and Scored Total Score; the Inattentive and Hyperactive/Impulsive subscales of the Attention-Deficit Hyperactivity Disorder Rating Scale-IV-Parent Version: Investigator Administered and Scored Total Score; the ADHD Index subscale of the Conners’ Parent Rating Scale-Revised: Short Form; and the Clinical Global Im-pressions of Severity of ADHD. Statistically significant efficacy was seen 1 week after randomization and re-mained so for the duration of the study. One patient from each of the atomoxetine and placebo groups discontin-ued the study as a result of an adverse event.
Conclusion. Atomoxetine was found to be effective and well tolerated for the treatment of ADHD in school-age girls.Pediatrics2002;110(6). URL: http://www.pediatrics. org/cgi/content/full/110/6/e75; atomoxetine, ADHD, school-age, girls, nonstimulant.
ABBREVIATIONS. ADHD, attention-deficit/hyperactivity disor-der;DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; ADHD RS, Attention-Deficit Hyperactivity Disor-der Rating Scale-IV-Parent Version: Investigator Administered
and Scored Total Score; SD, standard deviation; CPRS-R, Conners’ Parent Rating Scale-Revised: Short Form; CGI-ADHD-S, Clinical Global Impressions of Severity of ADHD.
A
ttention-deficit/hyperactivity disorder (ADHD) is an early-onset childhood disorder that is estimated to occur in 3% to 7% of school-age children.1Its pathophysiology seems to involve the interaction of norepinephrine, epinephrine, and do-pamine in modulation of attention and impulsivity.2 ADHD is frequently associated with impaired aca-demic and social functioning and persists into adult-hood in a sizable number of affected youths.3Literature on the efficacy of pharmacologic treat-ment in school-age children with ADHD has focused almost exclusively on boys. There is a paucity of data reporting findings of the pharmacologic treatment of ADHD in school-age girls, most likely because many more boys with ADHD are referred for treatment. TheDiagnostic and Statistical Manual of Mental Disor-ders, Fourth Edition (DSM-IV) estimated that boys with ADHD outnumber girls by as much as 9:1.1In contrast, community-based studies have found the ratio of boys to girls with ADHD to be as low as 2.5:1,4 suggesting that school-age girls with ADHD are less likely to be diagnosed properly and receive adequate treatment.5Although the reasons for lack of studies in girls is not completely clear, Biederman et al,6 Gaub and Carlson,7 and Carlson et al8 sug-gested that lower levels of psychiatric problems, ag-gression, and related behaviors in girls as compared with boys may contribute to fewer treatment refer-rals of girls. Consistent with this hypothesis, New-corn et al9examined data from the National Institute of Mental Health Collaborative Multisite Multimodal Treatment Study of Children with ADHD10 and found that girls were less impaired than boys on most ADHD symptom ratings and were less impul-sive on a continuous performance test.
Other studies have not found significant gender differences for overall impairment, behavioral rat-ings, or psychological measures. Sharp et al,11 in a study that compared boys and girls with ADHD, found few differences in ratings of symptomatology, comorbid diagnoses, and psychological function. Likewise, in a study that compared 140 girls with ADHD and 122 normal girls, Biederman et al5found that the core ADHD symptoms observed in girls with ADHD are similar to those seen in boys with
From the *Massachusetts General Hospital, Boston, Massachusetts; ‡Lilly Research Laboratories, Indianapolis, Indiana; §Neuroscience Inc, Bethesda, Maryland;储Lilly Deutschland GmbH, Bad Homburg, and Psychosomatic Department, Children’s Hospital, University of Hamburg, Hamburg, Ger-many; ¶University of Texas Southwestern Medical Center, Dallas, Texas; and #University of Nebraska Medical Center, Omaha, Nebraska. Received for publication Apr 30, 2002; accepted Aug 14, 2002.
Atomoxetine was originally called tomoxetine. The name was changed to avoid any potential confusion with tamoxifen that might lead to errors in dispensing the drugs.
Reprint requests to (J.H.H.) Lilly Corporate Center, DC 2022, Indianapolis, IN 46285. E-mail: [email protected]
ADHD. However, the prevalence of both conduct disorder and oppositional defiant disorder in the girls with ADHD was half of those previously re-ported in boys with ADHD.12 Thus, lower rates of disruptive behaviors in girls may result in fewer clinic referrals, contributing to the lack of recognition of the disorder and hence a lower reported preva-lence of ADHD in girls.5
Currently, psychostimulants such as methylpheni-date and amphetamines are the standard pharmaco-therapies for the treatment of ADHD. However, there are significant limitations to treatment with psychostimulants, which are not effective or well tolerated in approximately 30% of school-age chil-dren with ADHD. Adverse effects such as insomnia, decreased appetite, and irritability may lead to dis-continuation or dosage limitations. The lack of ade-quate full-day treatment often results in recurrence of impairing symptoms at home and in the commu-nity. In addition, psychostimulants bear the addi-tional burden of being controlled substances, result-ing in concerns about abuse and diversion. For these reasons, there remains a need for safe, effective, and nonstimulant alternatives for the treatment of ADHD in children and adults.
Studies have shown that several nonstimulant compounds that affect noradrenergic and/or dopa-minergic pathways (eg, desipramine, bupropion) are somewhat effective in ADHD.13,14However, no non-stimulant is currently approved for use in children or adults with ADHD. Atomoxetine is a potent inhibi-tor of the presynaptic norepinephrine transporter with minimal affinity for other noradrenergic recep-tors or for other neurotransmitter transporters or receptors. It is being investigated for the treatment of pediatric and adult ADHD. Several recent reports have provided evidence that atomoxetine is superior to placebo in reducing symptoms of ADHD in chil-dren and adults.15,16
There is a paucity of data regarding the efficacy of medications for the treatment of ADHD in girls. The limited published literature suggests that psycho-stimulant treatment is equally effective in boys and girls with ADHD. Two studies found no gender differences in response to methylphenidate.17,18 Sharp et al11compared the efficacy of methylpheni-date and d-amphetamine in boys and girls with ADHD and found no differences in efficacy. The lack of adequately controlled, double-blind, placebo-con-trolled clinical trials in school-age girls represents a significant absence in information available for pa-tients, parents, and physicians. In an effort to address this void, we conducted a subset analysis from 2 identical, randomized, double-blind, placebo-con-trolled clinical trials, examining the effects of the nonstimulant atomoxetine versus placebo in school-age girls who received a diagnosis of ADHD. To our knowledge, this is 1 of the largest studies of treat-ment effects of medication in this population.
METHODS
Two identical, double-blind, placebo-controlled clinical trials were conducted simultaneously in the United States. Study 1 had 7 sites; study 2 had 10 sites. Patients, boys and girls, met diagnostic
criteria for ADHD based on the DSM-IV and as assessed by clinical interview and the Kiddie Schedule for Affective Disorders and Schizophrenia.19Patients had a score on the Attention-Deficit
Hyperactivity Disorder Rating Scale-IV-Parent Version: Investiga-tor Administered and Scored (ADHD RS)20at least 1.5 standard
deviations (SDs) above the age and gender norms for their diag-nostic subtype (primarily inattentive or primarily hyperactive/ impulsive) or the total score for the combined subtype. Patients had normal intelligence based on the Wechsler Intelligence Scale for Children, Third Edition.21 After the study was explained,
written informed consent was obtained from the child’s parent or legal guardian. These studies were approved by each of the in-vestigative sites’ institutional review boards and were conducted in accordance with the Declaration of Helsinki 1975, as revised in 1983.
Physical examinations, routine laboratory tests of blood and urine (including urine toxicology), and electrocardiograms were obtained from all patients during baseline. The following were exclusionary criteria: poor metabolism of the cytochrome P450 2D6 isoenzyme; weight⬍25 kg at the initial visit; a documented history of bipolar I or II disorder or history of psychosis; history of an organic brain disease or a seizure disorder; currently taking psychotropic medication; history of alcohol or drug abuse within the past 3 months; positive screening for drugs of abuse; or sig-nificant previous or current medical conditions (eg, human immu-nodeficiency virus positive, surgically corrected congenital heart defects, leukemia in remission).
Study Design
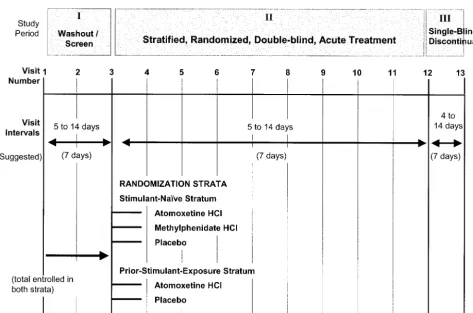
Figure 1 displays the design for each study. Visits 1 through 3 (study period 1) was a 2-week medication washout, screening, and assessment period; visits 3 through 12 (study period 2) was a 9-week, double-blind, acute treatment period; and visits 12 through 13 (study period 3) was a 1-week, single-blind study drug discontinuation period.
Before randomization, patients were divided into 2 groups on the basis of their previous psychostimulant treatment. Patients with no history of psychostimulant treatment (stimulant-naı¨ve stratum) were randomized to double-blind treatment with atom-oxetine, placebo, or methylphenidate. (The methylphenidate treat-ment arm was included in the stimulant-naı¨ve stratum to validate the study design in the event that atomoxetine failed to separate from placebo.) Patients who had received psychostimulant treat-ment (previous stimulant exposure stratum) were randomized to double-blind treatment with atomoxetine or placebo. Randomiza-tion was also stratified by investigaRandomiza-tional site. The randomizaRandomiza-tion schedules were generated by validated software and implemented in a blinded manner by using an interactive voice-response tele-phone system to dispense study medication.
The present report describes a subset intent-to-treat analysis that examined the effects of atomoxetine versus placebo in female patients. A total of 52 girls were randomized to either atomoxetine (n⫽ 31) or placebo (n ⫽ 21). In the stimulant-naı¨ve stratum, patients who were assigned to atomoxetine treatment received active drug before school and in the late afternoon/early evening, as well as a midday dose of placebo to preserve the blinding with the use of methylphenidate (the medication used to validate the study design). (Note: because of the small sample size of girls randomized to the methylphenidate treatment arm in the stimu-lant-naı¨ve stratum, we did not include them in the subset analysis reported in this article.) Patients in this stratum who were as-signed to placebo received study medication 3 times daily to maintain blinding. Patients in the previous stimulant exposure stratum were randomized to double-blind treatment with either atomoxetine or placebo, each administered before school and in the late afternoon/early evening. Study drug materials for all treatment groups were identical in appearance. The atomoxetine dose was titrated on the basis of clinical response on a milligram/ kilogram/day basis to a maximum daily dose of 2.0 mg/kg/d for atomoxetine (maximum allowable daily dose: 90 mg).
on an interview with the parent. The total score, which was the primary efficacy measure, was computed as the sum of the scores on each of the 18 items. In addition to the total score, scores were computed for inattention and hyperactivity/impulsivity subscales of the ADHD RS.
Secondary efficacy measures included the Conners’ Parent Rat-ing Scale-Revised: Short Form (CPRS-R),22which is a parent-rated
scale that assesses behaviors symptomatic of ADHD. It includes Oppositional, Cognitive Problems, Hyperactivity, and ADHD In-dex subscales. Another secondary efficacy measure was the Clin-ical Global Impressions of ADHD Severity (CGI-ADHD-S),23
which is a single-item rating of the clinician’s assessment of the severity of ADHD symptoms in relation to the clinician’s total experience with ADHD patients. Severity is rated on a 7-point scale (1⫽normal, not at all ill; 7⫽among the most extremely ill patients).
Statistical Analysis
All statistical tests were performed using a 2-tailed, .05 signif-icance level using an intent-to-treat principle. Treatment differ-ences in baseline patient characteristics were assessed using an analysis of variance model or Fisher exact test. For continuous measures, such as the ADHD RS, the CPRS-R, and the CGI-ADHD-S scale scores, change from baseline to endpoint of the double-blind treatment period was computed for all patients who had a baseline and at least 1 postbaseline measurement using a last observation carried forward approach. Treatment differences between atomoxetine and placebo in mean change from baseline to endpoint scores were assessed using an analysis of variance model with terms for baseline, gender, investigator, treatment, treatment-by-gender, and previous stimulant exposure strata. The primary efficacy analysis was the treatment comparison in mean change from baseline to endpoint ADHD RS total scores for ato-moxetine and placebo.
The ADHD RS scores over time were also assessed using a repeated measures mixed model. The model included terms for treatment, investigator, strata, visit, and treatment-by-visit inter-action, whereas the covariance matrix selection was based on Akaike’s Information Criteria. Treatment differences in
percent-ages of unsolicited treatment-emergent adverse events were as-sessed using the Fisher exact test.
RESULTS
A total of 52 girls were randomized for treatment (atomoxetine:n ⫽ 31; placebo: n ⫽ 21) across the 2 studies. A total of 51 patients who had a baseline and at least 1 postbaseline measurement using a last ob-servation carried forward were included in the sta-tistical analyses. Efficacy data were not available for 1 girl in the atomoxetine group, who discontinued the study because of a personal conflict. There were no significant differences between the treatment groups with respect to baseline demographics and severity of illness scores (Table 1). The most common comorbid diagnoses were oppositional defiant disor-der (38.5%) and phobias (13.5%). At baseline (com-bined treatment groups), female mean ADHD RS Total T-score was 88.9, which was 3.9 SD above the age/gender norm. (For comparison, the mean T-score in boys was 77.2, or 2.7 SD, above the age/ gender norm.) Of interest, 201 boys were random-ized to treatment with atomoxetine (n ⫽98) or pla-cebo (n⫽ 103) in the 2 studies.
Atomoxetine was superior to placebo on the pri-mary outcome measure (mean change from baseline to endpoint on the ADHD RS Total score; Fig 2). Atomoxetine-treated school-age girls experienced a statistically significantly greater decrease in their ADHD RS Total Score compared with placebo-treated school-age girls (15.8 vs 5.8, respectively;P⫽
Inattentive and Hyperactive/Impulsive subscales of the ADHD RS. Atomoxetine-treated patients re-ported a decrease on the Inattentive subscale relative to placebo-treated patients (8.8 vs 3.4, respectively;
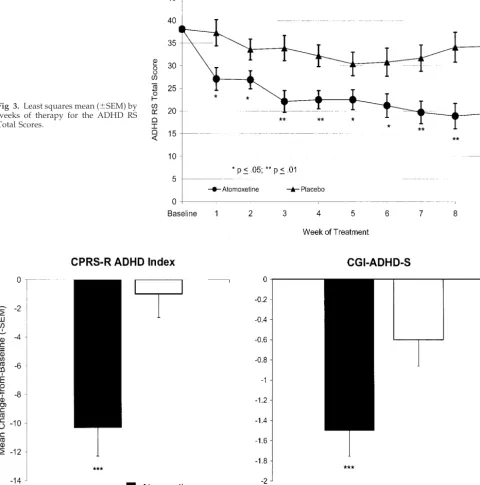
P ⫽ .001) and on the Hyperactive/Impulsive sub-scale (7.0 vs 2.3, respectively; P ⫽ .006; Fig 2). A visit-wise analysis of the ADHD RS Total Score com-paring atomoxetine with placebo found that atomox-etine-treated patients experienced significant efficacy that was evident at the first assessment 1 week after randomization (P⬍ .05) and persisted for the dura-tion of the study (Fig 3).
Atomoxetine was also superior to placebo on the parent-rated CPRS-R ADHD Index. Parents of atom-oxetine-treated patients reported a greater decrease in CPRS-R ADHD Index scores compared with par-ents of placebo-treated patipar-ents (10.3 vs 1.0, respec-tively; P ⬍ .001; Fig 4). In addition, a statistically significant decrease was observed on the CGI-ADHD-S for the atomoxetine group compared with the placebo group (1.5 vs 0.6, respectively;P⬍.001; Fig 4).
Atomoxetine was well tolerated in this population of school-age girls. The most frequently reported adverse events reported by atomoxetine-treated
pa-tients were abdominal pain (29%), rhinitis (26%), and headache (26%). However, there were no statistically significant differences between the treatment groups in the percentage of adverse events reported (Table 2). Furthermore, only 1 patient from each of the atomoxetine and placebo groups discontinued as a result of an adverse event (chest pain and somno-lence, respectively).
DISCUSSION
The results reported here represent 1 of the largest studies of medication effects in school-age girls with ADHD. An efficacy analysis of 51 school-age girls who met DSM-IVdiagnostic criteria for ADHD en-rolled in 2 identical, randomized, double-blind, pla-cebo-controlled studies demonstrated that atomox-etine (n ⫽ 30) was superior to placebo (n ⫽ 21) in reducing the severity of ADHD symptoms. Com-pared with placebo, atomoxetine significantly re-duced the ADHD RS Total Score, the Inattentive and Hyperactive/Impulsive subscales of the ADHD RS, the ADHD Index score of the CPRS-R, and the CGI-ADHD-S. When the data from the ADHD RS Total Score were examined using a visit-wise analysis, ato-moxetine produced statistically significant efficacy at Fig 2. Mean change from baseline to
endpoint scores (⫺standard error of the mean [SEM]) for the ADHD RS Total Score and Inattentive and Hy-peractive/Impulsive subscales for the atomoxetine and placebo treatment groups.
TABLE 1. Baseline Demographics and Illness Characteristics
Demographic Atomoxetine
(n⫽31)
Placebo (n⫽21)
PValue
Age (mean in y [SD]) 9.7 (1.6) 9.6 (1.5) .970
Weight (mean in kg [SD]) 38.3 (11.4) 39.7 (12.1) .450
Height (mean in cm [SD]) 138.6 (10.7) 138.6 (9.9) .635 Diagnostic subtypes (n[%])
Inattentive 6 (19.4%) 5 (23.8%) .739
Hyperactive/impulsive 0 (0.0%) 0 (0.0%) 1.000
Combined 25 (80.6%) 16 (76.2%) .739
WISC full-scale IQ (mean [SD]) 104.1 (15.7) 106.9 (16.5) .373 ADHD RS Total score (mean [SD]) 37.6 (9.5) 39.0 (8.1) .292 ADHD RS Inattentive subscale (mean [SD]) 20.8 (4.2) 22.4 (3.6) .069 ADHD RS Hyperactive/Impulsive subscale (mean [SD]) 16.8 (7.3) 16.5 (6.7) .820 CPRS-R ADHD index (mean [SD]) 27.4 (5.6) 26.2 (6.6) .889
CGI-ADHD-S (mean [SD]) 4.7 (0.8) 5.0 (0.8) .467
the first week after randomization that continued for the remainder of the study. These data demonstrat-ing significant efficacy for atomoxetine in school-age girls with ADHD extend data from studies that have shown that atomoxetine is efficacious in boys and girls as well as in men and women with ADHD15,16,24(Spencer et al, unpublished data). In ad-dition to demonstrating significant differences on investigator-scored measures, atomoxetine resulted in a significant decrease on a well-validated parent-age rating scale, the CPRS-R. The finding of efficacy on separate parent- and clinician-scored measures strengthens the significance of these results.
Overall, these data provide evidence that
atomox-etine can significantly reduce the severity of symp-toms in school-age girls with ADHD. Our findings clearly indicate that school-age girls with ADHD responded robustly to treatment with atomoxetine. Pediatricians, child psychiatrists, primary care phy-sicians, and other health care professionals should be mindful of the possible diagnosis of ADHD in girls who present with symptoms of inattentiveness, dis-organization, distractibility, and failure to finish tasks. Because girls are less likely to have comorbid externalizing disorders (oppositional defiant disor-der and conduct disordisor-der) than their male counter-parts, they are less likely to be identified and re-ferred. Studies have suggested that many boys who Fig 3. Least squares mean (⫾SEM) by
weeks of therapy for the ADHD RS Total Scores.
receive a diagnosis of ADHD are referred for evalu-ation because of disruptive disorders.7Others have noted that gender differences seen with children with ADHD are not as pronounced among adults with ADHD, most likely because adults can self-refer.25The present study indicates that atomoxetine can be used to treat girls with ADHD successfully. Early diagnosis and treatment of both boys and girls with ADHD is important to reduce the burden of illness in all patients.
The analysis reported here also provides addi-tional information about the tolerability of atomox-etine by reporting the adverse events and reasons for discontinuation in these school-age girls. There were no significant differences in treatment-emergent ad-verse events between girls who were treated with atomoxetine and those on placebo. The largest dif-ference was with vomiting. Among the atomoxetine-treated patients 19% (6 of the 31 patients) reported vomiting, whereas none of the girls on placebo re-ported this adverse event. However, this difference was not statistically significant, and no atomoxetine-treated patients discontinued treatment as a result of vomiting. Only 1 patient from each of the atomox-etine and placebo groups discontinued treatment as a result of an adverse event (chest pain and somno-lence, respectively). The small sample size of school-age girls in this analysis limits the interpretability of the adverse event analysis.
A limitation of these studies was the lack of teach-er-rated assessments of efficacy as a study objective. Although data were collected from teachers when available, an analysis of teacher data was neither a primary nor a secondary objective of this study. A study requiring data from teachers would have lim-ited the conduct of the study to the middle months of a school year and the populations to be studied to those children with 1 teacher. Considering that ato-moxetine treatment provides day-long coverage be-yond school hours, carefully conducted interviews with parents by trained clinicians can provide ade-quate information regarding school-related behavior
and performance observable in the evening and dur-ing weekends. Future studies, however, should as-sess the impact of atomoxetine on teacher ratings of school behavior and performance.
Despite these considerations, the data presented here provide additional evidence of the efficacy, safety, and tolerability of atomoxetine, a promising nonstimulant treatment for ADHD. Atomoxetine sig-nificantly decreased ADHD signs and symptoms in girls with ADHD and may offer an alternative to stimulants in the treatment of this disorder. The data reported from this subset analysis of 2 identical pla-cebo-controlled clinical trials address an important void in what is known about the treatment of school-age girls with ADHD.
ACKNOWLEDGMENTS This research was funded by Eli Lilly and Company. The Atomoxetine Study Group includes Paul Ambrosini, MD; Stan L. Block, MD; Joan Busner, PhD; Charles D. Casat, MD; C. Keith Conners, PhD; Daniel F. Connor, MD; David Dunn, MD; Stuart Kaplan, MD; Christopher McDougle, MD; Jeffrey H. New-corn, MD; F. Randy Sallee, MD, PhD; Keith Saylor, PhD; Thomas Spencer, MD; Mark Stein, PhD; Karen Dineen Wagner, MD, PhD; and Scott West, MD.
Drs Ambrosini, Biederman, Block, Busner, Casat, Conners, Connor, Dunn, Kratochvil, McDougle, Newcorn, Sallee, Saylor, Spencer, Stein, Wagner, and West have functioned as paid con-sultants and/or investigators for studies sponsored by Eli Lilly and Company. Drs. Dittmann, Heiligenstein, Faries, Laws, and Schuh are employees and shareholders of Eli Lilly and Company. We thank Nancy J. Trapp, Michele Y. Hill, and Fang Wan for contributions to the preparation of this manuscript.
REFERENCES
1. American Psychiatric Association.Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR.Washington, DC: American Psychiatric Association; 2000
2. Pliszka SR, McCracken JT, Maas JW. Catecholamines in attention-deficit hyperactivity disorder: current perspectives.J Am Acad Child Adolesc Psychiatry.1996;35:264 –272
3. Hechtman L. Assessment and diagnosis of attention-deficit/ hyperactivity disorder. Child Adolesc Psychiatr Clin N Am. 2000;9: 481– 498
4. Szatmari P. The epidemiology of attention-deficit hyperactivity disor-der.Child Adolesc Psychiatr Clin N Am.1992;1:361–371
5. Biederman J, Faraone SV, Mick E, et al. Clinical correlates of ADHD in females: findings from a large group of girls ascertained from pediatric and psychiatric referral sources.J Am Acad Child Adolesc Psychiatry.
1999;38:966 –975
6. Biederman J, Mick E, Faraone SV, et al. Influence of gender on attention deficit hyperactivity disorder in children referred to a psychiatric clinic.
Am J Psychiatry.2002;159:36 – 42
7. Gaub M, Carlson CL. Gender differences in ADHD: a meta-analysis and critical review.J Am Acad Child Adolesc Psychiatry.1997;36:1036 –1045 8. Carlson CL, Tamm L, Gaub M. Gender differences in children with
ADHD, ODD, and co-occurring ADHD/ODD identified in a school population.J Am Acad Child Adolesc Psychiatry.1997;36:1706 –1714 9. Newcorn JH, Halperin JM, Jensen PS, et al. Symptom profiles in
chil-dren with ADHD: effects of comorbidity and gender.J Am Acad Child Adolesc Psychiatry.2001;40:137–146
10. MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder.Arch Gen Psychiatry.1999;56:1073–1086
11. Sharp WS, Walter JM, Marsh WL, et al. ADHD in girls: clinical compa-rability of a research sample.J Am Acad Child Adolesc Psychiatry.1999; 38:40 – 47
12. Biederman J, Newcorn J, Sprich S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders.Am J Psychiatry.1991;148:564 –577
13. Wilens TE, Biederman J, Abrantes AM, Spencer TJ. A naturalistic as-sessment of protriptyline for attention-deficit hyperactivity disorder.
TABLE 2. Treatment-Emergent Adverse Events Reported by Patients Receiving Atomoxetine or Placebo*
Event Atomoxetine
(n⫽31) (%)
Placebo (n⫽21) (%)
Rhinitis 25.8 38.1
Abdominal pain 29.0 14.3
Headache 25.8 14.3
Pharyngitis 19.4 19.0
Decreased appetite 19.4 19.0
Vomiting 19.4 0.0
Cough increased 16.1 4.8
Nervousness 6.5 14.3
Somnolence 6.5 14.3
Nausea 6.5 14.3
Emotional lability 3.2 14.3
Fever 9.7 4.8
Insomnia 3.2 9.5
Diarrhea 3.2 4.8
Dizziness 3.2 4.8
J Am Acad Child Adolesc Psychiatry.1996;35:1485–1490
14. Wender PH, Reimherr FW. Bupropion treatment of attention-deficit hyperactivity disorder in adults.Am J Psychiatry.1990;147:1018 –1020 15. Michelson D, Faries DE, Wernicke J, et al. Atomoxetine in the treatment
of children and adolescents with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled, dose-response study. Pedi-atrics.2001;108(5). Available at: www.pediatrics.org/cgi/content/full/ 108/5/e83
16. Spencer TJ, Biederman J, Wilens TE, et al. Effectiveness and tolerability of tomoxetine in adults with attention deficit hyperactivity disorder.
Am J Psychiatry.1998;155:693– 695
17. Barkley RA. Hyperactive girls and boys: stimulant drug effects on mother-child interactions.J Child Psychol Psychiatry.1989;30:379 –390 18. Pelham WE, Jr, Walker JL, Sturges J, Hoza J. Comparative effects of
methylphenidate on ADD girls and ADD boys.J Am Acad Child Adolesc Psychiatry.1989;28:773–776
19. Kaufman J, Birmaher B, Brent D, Rao U, Ryan N.Kiddie-Sads-Present and Lifetime Version (K-SADS-PL). Version 1.0 of October 1996 ed.
Pitts-burgh, PA: Department of Psychiatry, University of Pittsburgh School of Medicine; 1996
20. DuPaul GJ, Power TJ, Anastopoulos AD, Reid R.ADHD Rating Scale-IV: Checklists, Norms, and Clinical Interpretations.New York, NY: The Guil-ford Press; 1998
21. Wechsler D.Wechsler Intelligence Scale for Children (WISC-III). 3rd ed. San Antonio, TX: The Psychological Corporation, Harcourt Brace and Company; 1991
22. Conners CK, Sitarenios G, Parker JD, Epstein JN. The revised Conners’ Parent Rating Scale (CPRS-R): factor structure, reliability, and criterion validity.J Abnorm Child Psychol.1998;26:257–268
23. Guy W.ECDEU Assessment Manual for Psychopharmacology, Revised.
Bethesda, MD: US Department of Health, Education, and Welfare; 1976 24. Spencer T, Biederman J, Heiligenstein J, et al. An open-label, dose-ranging study of atomoxetine in children with attention deficit hyper-activity disorder.J Child Adolesc Psychopharmacol.2001;11:251–265 25. Faraone SV, Biederman J, Spencer T, et al.
DOI: 10.1542/peds.110.6.e75
2002;110;e75
Pediatrics
Schuh
Dittmann, Graham J. Emslie, Christopher J. Kratochvil, Harry F. Laws and Kory J.
Joseph Biederman, John H. Heiligenstein, Douglas E. Faries, Nora Galil, Ralf
Attention-Deficit/Hyperactivity Disorder
Efficacy of Atomoxetine Versus Placebo in School-Age Girls With
Services
Updated Information &
http://pediatrics.aappublications.org/content/110/6/e75
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/110/6/e75#BIBL
This article cites 19 articles, 0 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/therapeutics_sub
Therapeutics
http://www.aappublications.org/cgi/collection/pharmacology_sub
Pharmacology
activity_disorder_adhd_sub
http://www.aappublications.org/cgi/collection/attention-deficit:hyper
Attention-Deficit/Hyperactivity Disorder (ADHD)
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior
Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.110.6.e75
2002;110;e75
Pediatrics
Schuh
Dittmann, Graham J. Emslie, Christopher J. Kratochvil, Harry F. Laws and Kory J.
Joseph Biederman, John H. Heiligenstein, Douglas E. Faries, Nora Galil, Ralf
Attention-Deficit/Hyperactivity Disorder
Efficacy of Atomoxetine Versus Placebo in School-Age Girls With
http://pediatrics.aappublications.org/content/110/6/e75
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
![Fig 2. Mean change from baseline toendpoint scores (�standard error ofthe mean [SEM]) for the ADHD RSTotal Score and Inattentive and Hy-peractive/Impulsive subscales for theatomoxetine and placebo treatmentgroups.](https://thumb-us.123doks.com/thumbv2/123dok_us/9504705.1479433/4.603.201.536.213.433/toendpoint-standard-inattentive-peractive-impulsive-subscales-theatomoxetine-treatmentgroups.webp)