Off-Label Use of Inhaled Nitric Oxide
After Release of NIH Consensus
Statement
Marc A. Ellsworth, MDa, Malinda N. Harris, MDa, William A. Carey, MDa, Alan R. Spitzer, MDb, Reese H. Clark, MDb
abstract
BACKGROUND:Inhaled nitric oxide (iNO) therapy is an off-label medication in infants,34 weeks’ gestational age. In 2011, the National Institutes of Health released a statement discouraging routine iNO use in premature infants. The objective of this study was to describe utilization patterns of iNO in American NICUs in the years surrounding the release of the National Institutes of Health statement. We hypothesized that iNO prescription rates in premature infants have remained unchanged since 2011.
METHODS:The Pediatrix Medical Group Clinical Data Warehouse was queried for the years 2009–2013 to describefirst exposure iNO use among all admitted neonates stratified by gestational age.
RESULTS:Between 2009 and 2013, the rate of iNO utilization in 23- to 29-week neonates increased from 5.03% to 6.19%, a relative increase of 23% (confidence interval: 8%–40%; P= .003). Of all neonates who received iNO therapy in 2013, nearly half were,34 weeks’ gestation, with these infants accounting for more than half of allfirst exposure iNO days each year of the study period.
CONCLUSIONS:The rates of off-label iNO use in preterm infants continue to rise despite evidence revealing no clear benefit in this population. This pattern of iNO prescription is not benign and comes with economic consequences.
WHAT’S KNOWN ON THIS SUBJECT:Off-label prescription of inhaled nitric oxide (iNO) to neonates,34 weeks’gestation has increased during the past decade. In early 2011, the National Institutes of Health determined that the available evidence did not support iNO use in this population.
WHAT THIS STUDY ADDS:Use of iNO among neonates,34 weeks’gestation has increased since 2011, entirely from greater use in extremely preterm neonates. Off-label
prescription of this drug now accounts for nearly half of all iNO use in American NICUs.
aDivision of Neonatal Medicine, Mayo Clinic, Rochester, Minnesota; andbCenter for Research, Education and Quality, Pediatrix Medical Group, Sunrise, Florida
Drs Ellsworth, Harris, and Carey conceptualized the study, interpreted the data, and drafted the manuscript; Dr Spitzer conceptualized and designed the study, acquired, analyzed, and interpreted the data, and critically reviewed and revised the manuscript; Dr Clark conceptualized and designed the study, acquired, analyzed, and interpreted the data, drafted the manuscript, and critically reviewed and revised the manuscript; and all authors approved thefinal manuscript for submission.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-3290
DOI:10.1542/peds.2014-3290 Accepted for publication Jan 16, 2015
Address correspondence to Marc A. Ellsworth, MD, Division of Neonatal Medicine, Mayo Clinic, 200 1st St SW, Rochester, MN 55905. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
In 1999, inhaled nitric oxide (iNO) was approved for treatment of hypoxic respiratory failure in term and near-term neonates. Given its efficacy and safety in this population,1–4iNO utilization increased during the following decade, most notably among neonates,34 weeks’gestational age.5 This marked rise in off-label use occurred at the same time that multiple randomized clinical trials failed to demonstrate clear benefit in this high-risk preterm population,6–16 a collective result that has been borne out in subsequent systematic
reviews.17–19Beyond the absence of evidence of benefit, an additional concern is that off-label prescription of iNO to preterm neonates contributes substantially to the cost of health care delivery in the NICU.10,20
As iNO use in the preterm population continued to rise,5,21the National Institutes of Health (NIH) and the American Academy of Pediatrics assembled content experts to develop consensus-based guidance for practicing neonatologists. The resulting NIH statement22and American Academy of Pediatrics clinical report23indicated that available evidence did not support the routine use of iNO in preterm infants, though rare clinical situations and new management strategies did merit further study. After issuance of the NIH statement in early 2011, the Neonatal Research Network (NRN) reported decreased use of iNO among neonates,29 weeks’gestation.24 Despite this overall decline, the iNO utilization rates of some NRN centers were much higher than previously published national averages.5,21
We conducted the current study to test our hypothesis that the rate at which iNO is prescribed off-label to preterm neonates has not changed significantly in the years after the NIH consensus statement.
METHODS
Study Design
We performed a retrospective cohort study by using a deidentified data set
that is approved by the Western Institutional Review Board (IRB). The study was also approved by the Greenville Memorial Hospital IRB (Greenville, SC) and considered exempt by the Mayo Clinic IRB (Rochester, MN).
Study Population
Neonates were included in our study sample if they required admission to a Pediatrix Medical Group (PMG) NICU and were discharged between January 1, 2009, and December 31, 2013. Neonates who died in the delivery room or those who were not admitted for neonatal intensive care (eg, comfort care) were not included in the analysis.
Data Set
PMG provides intensive care services in 310 hospitals throughout the United States and Puerto Rico. The physicians and nurse practitioners who provide care to neonates in PMG NICUs use a proprietary software system to generate clinical admission, progress, and discharge notes. These local data are consolidated within the PMG Clinical Data Warehouse (CDW), deidentified, and made compliant with Health Insurance Portability and Accountability Act of 1996
regulations. Data are also configured into tables that can be joined and queried for quality improvement and research.25–27
Data Analysis
We queried specific CDW tables to perform our analysis, namely patients, admissions, diagnoses, medications, and respiratory support. Data on estimated gestational age (EGA) represented the best estimates from both obstetrical data and neonatal examinationfindings. We identified all patients who received iNO by searching the medications and respiratory support tables for the term“nitric oxide.”For each patient, we estimated the duration of thefirst course of iNO therapy by subtracting the age at which iNO wasfirst
initiated from the age at which it was discontinued (excluding subsequent courses of iNO therapy). The total number of iNO days was calculated by summing these values for each year.
Patients were categorized by EGA (23–29 weeks, 30–33 weeks, and $34 weeks) and differences in their demographic characteristics were analyzed by year (Table 1). Continuous variables (eg, EGA and birth weight) were evaluated with analysis of variance and post hoc analysis to identify specific subgroup differences. Categorical variables (eg, race and gender) were evaluated with 2-tailedx2tests. Nonparametric data were assessed with Kruskal-Wallis analysis of variance. We used the linear trend test and the Cochran-Armitage trend test to evaluate time-related changes. All statistical analyses were performed by using JMP 11 (SAS Institute, Inc, Cary, NC).
RESULTS
There were a total of 420 571 infants admitted to PMG NICUs from 2009 to 2013. Of these, 5676 (1.3%) were exposed to iNO during their hospitalization. Aside from an increase in the median birth weight of infants treated in 2011 (P= .01), demographic characteristics did not vary from year to year among those receiving iNO therapy (Table 1).
Among all neonates,34 weeks admitted to level III or IV PMG NICUs in 2013, iNO utilization rates were inversely proportional to gestational age (Fig 2). For example, 13.9% of all 23- to 24-week infants were treated with iNO, compared with 0.6% of 33-week neonates. Of all neonates who received iNO therapy in 2013, nearly half (46%; Fig 3) were,34 weeks’gestation and thus
received this drug off-label. Because only 1.3% of iNO-exposed patients were treated at level II NICUs, data for these patients were not included in the above analyses.
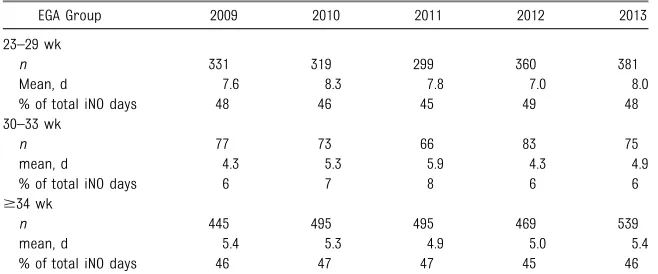
Specifics regarding the age at initiation for all neonates and duration of use (first course) for those with complete data are displayed in Tables 2 and 3, respectively. There were no
significant differences in either pattern of use within gestational age cohorts from 2009 to 2013. Infants ,34 weeks’gestation accounted for more than half of all iNO days each year of the study period.
DISCUSSION
We demonstrate that off-label prescription of iNO to preterm neonates has not declined in the years after the NIH statement discouraging routine use in this population.22Similar to NRN-affiliated clinicians,24we detected a small decrement in iNO use in 2011 among premature infants, though this change was not statistically
significant. By extending our analysis through 2013, we were able to determine that the overall rate of off-label iNO use among all gestational age subgroups persisted at its baseline level and the rate increased among neonates,30 weeks’ gestation. Between 2009 and 2013, for the 79 434 infants 23 to 29 weeks cared for at the 703 hospitals in the United States participating in the
TABLE 1 Distribution of iNO Use in PMG NICUs
Discharge Year P
2009 2010 2011 2012 2013
Total patients in CDW,n 79 883 82 778 85 149 85 994 86 767
iNO-treated patients,n(%) 1049 (1.3) 1120 (1.4) 1085 (1.3) 1159 (1.3) 1263 (1.5) .2
EGA, median (10th–90th) 35 (24–40) 35 (24–40) 36 (24–40) 34 (24–40) 34 (24–40) .6
EGA group,n(%), wka .2
23–29 392 (37) 397 (35) 366 (34) 441 (38) 476 (38) —
30–33 99 (9) 97 (9) 86 (8) 107 (9) 106 (8) —
$34 556 (53) 621 (55) 630 (58) 602 (52) 674 (53) —
Birth weight, median (10th–90th) 2.27 (0.62–3.71) 2.42 (0.60–3.80) 2.59 (0.62–3.75) 2.20 (0.59–3.79) 2.27 (0.60–3.78) .01
Boy,n(%) 614 (59) 666 (59) 638 (59) 684 (59) 721 (57) .4
Race/ethnicity,n(%)a .1
White 504 (48) 548 (49) 498 (46) 560 (48) 631 (50) —
Hispanic 223 (21) 251 (22) 261 (24) 227 (20) 224 (18) —
African American 211 (20) 221 (20) 222 (20) 263 (23) 258 (20) —
Asian 29 (3) 31 (3) 20 (2) 30 (3) 32 (3) —
American/Alaska Native 15 (1) 16 (1) 10 (1) 10 (1) 19 (2) —
Pacific Islander 3 (0) 3 (0) 5 (0) 6 (1) 11 (1) —
Other 64 (6) 50 (4) 69 (6) 63 (5) 88 (7) —
Cesarean delivery,n(%) 704 (67) 772 (69) 731 (67) 768 (66) 858 (68) .9
Outborn,n(%) 419 (40) 445 (40) 404 (37) 416 (36) 456 (36) .4
Disposition,n(%)a .7
Alive 586 (56) 604 (54) 604 (56) 634 (55) 713 (56) —
Died 231 (22) 246 (22) 213 (20) 264 (23) 261 (21) —
Transfer 232 (22) 270 (24) 268 (25) 261 (23) 289 (23) —
aBased on 2-tailed x2 testing evaluating the group.
FIGURE 1
Vermont Oxford Network, the rate of iNO utilization increased from 6.7% to 6.9% (unpublished data provided by the Vermont Oxford Network).
iNO use within PMG has accelerated most rapidly among extremely preterm neonates, a subgroup that now accounts for nearly half of all
iNO use in the NICU despite the potential for morbidities in this population.11,28Given increased iNO utilization in higher-acuity units,24it may be that iNO is directed at more critically ill neonates for which evidence of benefit and safety of use is most limited.6–16The observation that neonatologists would
increasingly prescribe iNO in a manner contrary to clinical evidence and expert opinion22,23 is fascinating and provocative.
We suspect that off-label iNO utilization is driven by the idea that iNO promotes increased survival. Despite no clear evidence that there is improved survival in iNO-exposed premature infants, the immediate physiologic effect of iNO is well described, with an increase in oxygen saturation being readily apparent in many infants who are exposed to iNO.6,29,30We speculate that this physiologic effect likely leads many neonatologists to attribute the survival of iNO-exposed neonates to iNO therapy, when in fact a number of other factors could have led to that infant’s outcome. We acknowledge that it is possible that iNO may be therapeutic in the premature neonate, but clearly its role has not been delineated. For example, there may be a role for use in infants with
premature rupture of membranes, oligohydramnios, and pulmonary hypoplasia, but currently there are no prospective studies in this
population.31Perhaps the history of iNO eventually will resemble that of another 1-time controversial therapy, extracorporeal membrane
oxygenation. Once regarded as unsafe and founded on suboptimal clinical evidence,32,33extracorporeal membrane oxygenation is now regarded as lifesaving therapy with a clear role for utilization in select groups of neonates.34
Until that time, we must consider the increased costs that the use of iNO therapy contributes to caring for critically ill neonates. Among the 456
FIGURE 2
Percentage of infants treated with iNO at PMG (level III or IV) NICUs stratified by gestational age in 2013.
FIGURE 3
Distribution of total iNO use by gestational age in PMG (level III or IV) NICUs in 2013.
TABLE 2 Age at Initiation of First Course of Therapy
EGA Group DOL iNO Started, d 2009 2010 2011 2012 2013
23–29 wk 0–7 227 (58) 208 (52) 200 (55) 252 (57) 261 (55)
8–28 104 (27) 117 (29) 97 (27) 96 (22) 130 (27)
.28 61 (16) 72 (18) 69 (19) 93 (21) 85 (18)
30–33 wk 0–7 87 (88) 80 (82) 71 (83) 91 (85) 90 (85)
8–28 5 (5) 6 (6) 5 (6) 7 (7) 8 (8)
.28 7 (7) 11 (11) 10 (12) 9 (8) 8 (8)
$34 wk 0–7 532 (96) 588 (95) 597 (95) 565 (94) 641 (95)
8–28 20 (4) 22 (4) 16 (3) 26 (4) 20 (3)
.28 4 (1) 11 (2) 17 (3) 11 (2) 13 (2)
neonates,34 weeks’gestation with completefirst exposure duration of use data in PMG NICUs in 2013, iNO was used for a total of 3409 patient days. Given the estimated median per day cost of iNO therapy ($5753),35 this off-label prescription of iNO may have generated a cost to payers of $19.6 million in 2013. The most recent vital statistics report indicates that∼135 000 infants were born at ,34 weeks’gestation in 2012.36If these infants were treated at the same rate and average duration as the above PMG cohort (2.63%, 7.48 days per treated patient), the estimated total cost to US health care would be
∼$153 million for off-label use. The accuracy of this estimate is uncertain, however, given that some hospitals pay for hourly usage of iNO, whereas others pay an up-front cost for
anticipated use over a given period of time.
The strength of this study relates to the quality of the data housed within the CDW. This database includes demographic and clinical information about more than 420 000 subjects hospitalized in PMG NICUs during the study period. Thus, our cohort represents a large sample of the total population of neonates admitted to NICUs throughout the country. Currently our data
collection techniques do not permit us to understand why iNO therapy was used. Specifically, we cannot know the primary reasons clinicians initiated treatment with iNO
(eg, bronchopulmonary dysplasia prevention,“rescue”therapy in respiratory failure, pulmonary hypertension, and pulmonary
hypoplasia). However, it may be possible to infer different
therapeutic groupings based on the timing of initiation of therapy. We chose not to address safety and efficacy concerns in this study, because it would have been challenging to draw meaningful inferences from retrospective analyses of a highly selected population of ventilated infants whose mortality rate suggested that they were critically ill. Only carefully designed prospective studies will answer which subset of premature infants might benefit from treatment with iNO.
CONCLUSIONS
The rates of off-label iNO use in PMG NICUs continue to rise despite clinical evidence and expert opinion suggesting no clear benefit in preterm neonates. This pattern of iNO prescription is not benign and comes with economic consequences. Despite evidence suggesting that iNO is a safe therapy in premature neonates, there is insufficient efficacy data to recommend continued use.
ACKNOWLEDGMENT
We thank the Vermont Oxford Network for providing unpublished data for inclusion in the article.
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose. FUNDING:No external funding.
POTENTIAL CONFLICT OF INTEREST:Dr Spitzer’s and Dr Clark’s employer Pediatrix Medical Group, and the Neo Conference, received unrestricted educational grants for the support of continuous medical education from the company that sells inhaled nitric oxide (Ikaria); and Drs Ellsworth, Harris, and Carey have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER:A companion to this article can be found on page 754, and online at www.pediatrics.org/cgi/doi/10.1542/peds.2015-0144.
REFERENCES
1. Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure.N Engl J Med. 1997;336(9):597–604
2. Clark RH, Kueser TJ, Walker MW, et al; Clinical Inhaled Nitric Oxide Research Group. Low-dose nitric oxide therapy for
persistent pulmonary hypertension of the newborn.N Engl J Med. 2000;342(7): 469–474
3. Finer NN, Barrington KJ. Nitric oxide for respiratory failure in infants born at or near term.Cochrane Database Syst Rev. 2006; (4):CD000399
4. Roberts JD Jr, Fineman JR, Morin FC III, et al; The Inhaled Nitric Oxide Study Group. Inhaled nitric oxide and persistent pulmonary hypertension of the newborn. N Engl J Med. 1997;336(9):605–610
5. Clark RH, Ursprung RL, Walker MW, Ellsbury DL, Spitzer AR. The changing
TABLE 3 Duration of iNO Use Per Patient
EGA Group 2009 2010 2011 2012 2013
23–29 wk
n 331 319 299 360 381
Mean, d 7.6 8.3 7.8 7.0 8.0
% of total iNO days 48 46 45 49 48
30–33 wk
n 77 73 66 83 75
mean, d 4.3 5.3 5.9 4.3 4.9
% of total iNO days 6 7 8 6 6
$34 wk
n 445 495 495 469 539
mean, d 5.4 5.3 4.9 5.0 5.4
% of total iNO days 46 47 47 45 46
pattern of inhaled nitric oxide use in the neonatal intensive care unit.J Perinatol. 2010;30(12):800–804
6. Subhedar NV, Shaw NJ. Changes in oxygenation and pulmonary
haemodynamics in preterm infants treated with inhaled nitric oxide.Arch Dis Child Fetal Neonatal Ed. 1997;77(3):F191–F197
7. Kinsella JP, Walsh WF, Bose CL, et al. Inhaled nitric oxide in premature neonates with severe hypoxaemic respiratory failure: a randomised controlled trial. Lancet. 1999;354(9184):1061–1065
8. Srisuparp P, Heitschmidt M, Schreiber MD. Inhaled nitric oxide therapy in premature infants with mild to moderate respiratory distress syndrome.J Med Assoc Thai. 2002;85(suppl 2):S469–S478
9. Schreiber MD, Gin-Mestan K, Marks JD, Huo D, Lee G, Srisuparp P. Inhaled nitric oxide in premature infants with the respiratory distress syndrome.N Engl J Med. 2003;349(22):2099–2107
10. Field D, Elbourne D, Truesdale A, et al; INNOVO Trial Collaborating Group. Neonatal Ventilation With Inhaled Nitric Oxide Versus Ventilatory Support Without Inhaled Nitric Oxide for Preterm Infants With Severe Respiratory Failure: the INNOVO multicentre randomised controlled trial (ISRCTN 17821339). Pediatrics. 2005;115(4):926–936
11. Van Meurs KP, Wright LL, Ehrenkranz RA, et al; Preemie Inhaled Nitric Oxide Study. Inhaled nitric oxide for premature infants with severe respiratory failure.N Engl J Med. 2005;353(1):13–22
12. Hascoet JM, Fresson J, Claris O, et al. The safety and efficacy of nitric oxide therapy in premature infants.J Pediatr. 2005; 146(3):318–323
13. Dani C, Bertini G, Pezzati M, Filippi L, Cecchi A, Rubaltelli FF. Inhaled nitric oxide in very preterm infants with severe respiratory distress syndrome.Acta Paediatr. 2006;95(9):1116–1123
14. Kinsella JP, Cutter GR, Walsh WF, et al. Early inhaled nitric oxide therapy in premature newborns with respiratory failure.N Engl J Med. 2006;355(4):354–364
15. Ballard RA, Truog WE, Cnaan A, et al; NO CLD Study Group. Inhaled nitric oxide in preterm infants undergoing mechanical ventilation. N Engl J Med. 2006;355(4):343–353
16. Mercier JC, Hummler H, Durrmeyer X, et al; EUNO Study Group. Inhaled nitric
oxide for prevention of bronchopulmonary dysplasia in premature babies (EUNO): a randomised controlled trial.Lancet. 2010;376(9738):346–354
17. Askie LM, Ballard RA, Cutter GR, et al; Meta-analysis of Preterm Patients on Inhaled Nitric Oxide Collaboration. Inhaled nitric oxide in preterm infants: an individual-patient data meta-analysis of randomized trials.Pediatrics. 2011; 128(4):729–739
18. Barrington KJ, Finer N. Inhaled nitric oxide for respiratory failure in preterm infants.Cochrane Database Syst Rev. 2010; (12):CD000509
19. Donohue PK, Gilmore MM, Cristofalo E, et al. Inhaled nitric oxide in preterm infants: a systematic review.Pediatrics. 2011;127(2). Available at: www.pediatrics. org/cgi/content/full/127/2/e414
20. Watson RS, Clermont G, Kinsella JP, et al; Prolonged Outcomes After Nitric Oxide Investigators. Clinical and economic effects of iNO in premature newborns with respiratory failure at 1 year. Pediatrics. 2009;124(5):1333–1343
21. Padula MA, Grover TR, Brozanski B, et al. Therapeutic interventions and short-term outcomes for infants with severe bronchopulmonary dysplasia born at
,32 weeks’gestation.J Perinatol. 2013; 33(11):877–881
22. Cole FS, Alleyne C, Barks JD, et al. NIH Consensus Development Conference statement: inhaled nitric-oxide therapy for premature infants.Pediatrics. 2011; 127(2):363–369
23. Kumar P; Committee on Fetus and Newborn; American Academy of Pediatrics. Use of inhaled nitric oxide in preterm infants.Pediatrics. 2014;133(1):164–170
24. Truog WE, Nelin LD, Das A, et al; NICHD Neonatal Research Network. Inhaled nitric oxide usage in preterm infants in the NICHD neonatal research network: inter-site variation and propensity evaluation. J Perinatol. 2014;34(11):842–846
25. Spitzer AR, Ellsbury DL, Handler D, Clark RH. The Pediatrix BabySteps Data Warehouse and the Pediatrix QualitySteps improvement project system—tools for“meaningful use”in continuous quality improvement.Clin Perinatol. 2010;37(1):49–70
26. Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Reported medication use
in the neonatal intensive care unit: data from a large national data set. Pediatrics. 2006;117(6):1979–1987
27. Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Empiric use of ampicillin and cefotaxime, compared with ampicillin and gentamicin, for neonates at risk for sepsis is associated with an increased risk of neonatal death. Pediatrics. 2006;117(1):67–74
28. Hintz SR, Van Meurs KP, Perritt R, et al Neurodevelopmental outcomes of premature infants with severe respiratory failure enrolled in
a randomized controlled trial of inhaled nitric oxide.J Pediatr. 2007;151(1):16–22
29. Skimming JW, Bender KA, Hutchison AA, Drummond WH. Nitric oxide inhalation in infants with respiratory distress syndrome.J Pediatr. 1997;130(2):225–230
30. Van Meurs KP, Rhine WD, Asselin JM, Durand DJ; Preemie NO Collaborative Group. Response of premature infants with severe respiratory failure to inhaled nitric oxide.Pediatr Pulmonol. 1997;24(5):319–323
31. Chock VY, Van Meurs KP, Hintz SR, et al; NICHD Neonatal Research Network. Inhaled nitric oxide for preterm premature rupture of membranes, oligohydramnios, and pulmonary hypoplasia.Am J Perinatol. 2009;26(4):317–322
32. Paneth N, Wallenstein S. Extracorporeal membrane oxygenation and the play the winner rule.Pediatrics. 1985;76(4): 622–623
33. Elliott SJ. Neonatal extracorporeal membrane oxygenation: how not to assess novel technologies.Lancet. 1991; 337(8739):476–478
34. Carey WA, Colby CE. Extracorporeal membrane oxygenation for the treatment of neonatal respiratory failure.Semin Cardiothorac Vasc Anesth. 2009;13(3):192–197
35. Campbell BT, Herbst KW, Briden KE, Neff S, Ruscher KA, Hagadorn JI. Inhaled nitric oxide use in neonates with congenital diaphragmatic hernia.Pediatrics. 2014; 134(2). Available at: www.pediatrics.org/ cgi/content/full/134/2/e420
DOI: 10.1542/peds.2014-3290 originally published online March 9, 2015;
2015;135;643
Pediatrics
H. Clark
Marc A. Ellsworth, Malinda N. Harris, William A. Carey, Alan R. Spitzer and Reese
Statement
Off-Label Use of Inhaled Nitric Oxide After Release of NIH Consensus
Services
Updated Information &
http://pediatrics.aappublications.org/content/135/4/643 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/135/4/643#BIBL This article cites 35 articles, 11 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2014-3290 originally published online March 9, 2015;
2015;135;643
Pediatrics
H. Clark
Marc A. Ellsworth, Malinda N. Harris, William A. Carey, Alan R. Spitzer and Reese
Statement
Off-Label Use of Inhaled Nitric Oxide After Release of NIH Consensus
http://pediatrics.aappublications.org/content/135/4/643
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.