Christopher S.J. Tran, BSc, Faculty of Medicine, University of Toronto
Joyce Nyhof-Young, MSc, PhD, Cancer Survivorship Program, Princess Margaret Hospital and Department of Radiation
Oncology, University of Toronto
Gayathri Embuldeniya, MA, CPhil, PhD, Division of Rheumatology, Department of Medicine, Sunnybrook Health Sciences Centre
1BVMB7FJOPU.)4D%JWJTJPOPG3IFVNBUPMPHZ%FQBSUNFOUPG.FEJDJOF4VOOZCSPPL)FBMUI4DJFODFT$FOUSF
Phedias Diamandis, PhD, Faculty of Medicine, University of Toronto
Lopamudra Das, BSc, Faculty of Medicine, University of Toronto
Romy Cho, BHSc, Faculty of Medicine, University of Toronto
Mary J. Bell, MD, MSc, FRCPC, Division of Rheumatology, Department of Medicine, Sunnybrook Health Sciences Centre and
Division of Rheumatology, Department of Medicine, Faculty of Medicine, University of Toronto
Abstract
This study aims to identify the informational,
emo-tional, and appraisal support needs of individuals
with inflammatory arthritis (IA) from the
perspec-tives of patients, family and friends, and health care
providers (HCPs). Desirable characteristics of a
peer-to-peer mentoring program as an adjunct to clinical
care for people with early IA (EIA) were also
ascer-tained. Semi-structured interviews were performed
with a purposive sample of patients with IA (n= 15),
family members and friends (n= 6), and HCPs (n=
9) involved in the care of IA. Interview data were
analyzed using NVivo 8. Descriptive themes were
identified through constant comparative analysis.
Individuals with IA prefer a variety of information
sources, and informational needs evolve over time.
Family and friends suggested that an emotional
sup-port network was valuable to help cope with and
learn about IA. The idea of peer-to-peer
mentor-ing as a form of support was well received, as peers
were perceived to be able to provide informational,
appraisal and emotional support. Although HCPs
cautioned that peers should acknowledge the limits
of their knowledge, they too suggested that peers
could help reinforce informational support
provid-ed by HCPs. Disease stage and personal qualities
were important considerations for a peer support
program. Peer support was a well-received approach
for helping individuals with EIA cope with concerns
brought by their new diagnosis and to meet their
in-formation and support needs. These results suggest
that peer mentoring, if context-driven and sensitive
to individual needs, could be valuable in helping
individuals with EIA to manage their condition.
De-velopment of an EIA-specific peer support
interven-tion is underway.
Corresponding Author: Mary J Bell, MD, MSc, FRCPC Division of Rheumatology
Department of Medicine, University of Toronto Sunnybrook Health Sciences Centre
2075 Bayview Avenue Toronto, Ontario M4N 3M5 Email: [email protected]
Introduction
I
nflammatory arthritis (IA) is a leading cause of functional
disability and chronic pain, and the burden of illness is
pro-jected to increase.
1-3The disease course and symptoms are
often unpredictable, making management difficult.
4Primary
care providers are underprepared to take on the management
of a chronic condition, and the number of musculoskeletal
specialists in Canada is decreasing.
5-7Unfortunately, delays to
rheumatologic care are common, as individuals with IA and
their health care providers (HCPs) both fail to recognize early
disease,
8-10leading to poor health outcomes.
11-13While interprofessional health care is important,
educat-ing IA patients with the knowledge and skills to help them to
manage their condition can improve patient health outcomes
and reduce healthcare burden, such as visits to emergency
de-partments.
14In fact, patient education in self-management has
been identified as an arthritis best-practice and a key clinical
practice guideline.
15-18Peer support models have been successfully implemented
for improved management of various health issues.
19-21A
peer is defined as a person who shares common
characteris-tics with an individual, such that the peer is able to relate to
and empathize with that person on a level that is not possible
by a non-peer.
22Peer support encompasses emotional,
ap-praisal and informational support provided by an individual
(or group) having personal experience of a specific behaviour
or stressor and characteristics similar to the population being
supported.
23Emotional support includes expressions of caring,
empathy, and reassurance. Appraisal support involves
affirma-tion of one’s feelings and behaviours, encouraging persistence
for resolving problems, and reassurance that frustrations can
be handled. Informational support involves providing advice,
suggestions and facts relevant to an individual’s particular
chal-lenges. All three types of support are based on experiential
knowledge rather than formal training.
23Peers have the
po-tential to influence health outcomes of other patients by
ad-dressing feelings of isolation, promoting positive outlook and
motivation, and providing information about behaviours that
encourage health and well-being.
23While peer support has helped individuals with various
chronic diseases to manage their conditions,
19-21it is not well
researched in the IA population. Peer support is particularly
relevant to members of the early IA (EIA) population who
of-ten express frustration due to work impairment and persisof-tent
pain.
24In particular, early emphasis on social support may
de-crease long-term functional disability in patients with EIA.
25As
such, peer support can play a vital role as an adjunct to clinical
care for IA by improving self-efficacy, self-management, social
support, health-related quality of life, coping-efficacy,
adher-ence to pharmacological therapy, and by decreasing anxiety
and disease activity among EIA patients.
This paper reports the results of an exploration of the needs
of individuals with IA, their friends and families, and HCPs to
assess patients’ educational and support needs and determine
the acceptability of a peer support intervention in the EIA
pop-ulation. This is the first phase of the development of a peer
support intervention for individuals with EIA.
Participants and Method
Recruitment
Individuals with IA receiving outpatient care from the
Divi-sion of Rheumatology at Sunnybrook Health Science Centre
(SHSC), Toronto, Canada, and their family and friends were
invited to participate by information letter distributed
dur-ing clinical hours and through The Arthritis Society. Family
and friends were also recruited by recommendation from
in-dividuals with IA. HCPs known to the principal investigator
(MB) were approached though personal contact, email or
telephone. A purposive sampling strategy ensured diversity in
disease duration and social demographics. Ethics approval was
received from SHSC Research Ethics Board.
Patient Disease Management
1. Tell me about the things you do to care for or manage your arthritis.
2. Tell me about the time when you received your diagnosis. What was your reaction?
Patient Decision-Making
8IFOZPVIBWFBRVFTUJPOBCPVUIPXUPDBSFGPSZPVSBSUISJUJTPSZPVIBWFBEFDJTJPOUPNBLFXIFSFEPZPVHPPSXIBUEPZPVEPUPmOEUIFBOTXFS or make the decision? What information sources do you use?
8IBUBSFZPVSQSFGFSSFENFUIPETGPSMFBSOJOH 8IBUBSFZPVSQSFGFSSFENFUIPETGPSHFUUJOHBOTXFSTUPZPVSRVFTUJPOTPSNBLJOHEFDJTJPOT (e.g., reading, information sessions, one-on-one vs. group; with health professional, with peers)
5. Some decisions we make are relatively minor and can be made quickly with very little thought (e.g., “Will I have cereal or toast for breakfast?”). Other decisions are much more difficult to make, such as whether or not to take medications or go to a physical therapist to help care for our arthritis. When you have a difficult decision to make what do you do? What are the steps you would take?
)PXFGGFDUJWFBSFUIFTFTUSBUFHJFTGPSNBOBHJOHZPVSBSUISJUJT 7. What would make it easier for you to make these difficult decisions?
Informational Needs
8. Thinking back to the time when you were diagnosed with arthritis, what kind of information did you need or would you have like to have received? What did you want to know about?
"TUJNFXFOUPOIPXEJEZPVSJOGPSNBUJPOOFFETDIBOHF
Emotional Needs
)PXJNQPSUBOUJTFNPUJPOBMTVQQPSUUPZPVGPSIFMQJOHZPVUPNBLFEFDJTJPOT
Appraisal Needs
11. How important is it to get feedback on these decisions?
Opinions on Peer Support
12. One strategy that can be used to help people make decisions is peer support. A peer is a person who shares common characteristics (e.g., age, sex, disease status) with the individual or group of interest. The ‘peer’ is able to relate to, and empathize with the person on a level that a non-peer would not be able to.
a. What is your opinion of this approach as a way to help you make decisions to help you manage your disease? How would you feel about having a peer as a decision coach to help you make decisions related to managing your condition?
b. What do you think the role of this peer could be? c. What are important qualities of a peer?
d. Would you prefer one-on-one or in a group setting? e. How often would you prefer to meet?
Other Comments
%PZPVIBWFBOZNPSFDPNNFOUTUIBUZPVXPVMEMJLFUPTIBSFXJUIVT
Inclusion Criteria
Patient participants required a formal diagnosis of IA.
‘Fam-ily members’ were first-degree relatives, partners, and friends
of an individual with IA; friends were included if they played a
substantial care-giving role. HCPs were physicians, nurses,
oc-cupational therapists, physiotherapists, and social workers for
individuals diagnosed with IA. All participants were 18 years or
older and able to understand and converse in English.
Interviews
Audiotaped interviews lasting 30 to 60 minutes, were
con-ducted face with patients and family, and either
face-to-face or by telephone with HCPs. Family were interviewed
sepa-rately from the patient with IA. A semi-structured interview
guide (Figure 1) was developed based on a literature review
of patient education in arthritis, previous studies of peer
sup-port needs in arthritis patients, and research team experiences.
Patients, family members, and friends were asked about their
own support needs and learning preferences. HCPs were asked
to assess their patients’ support needs. All participants were
asked about peer support suitability as a management strategy.
Interviews with patients, family and friends took place at a
private room at SHSC. HCPs were interviewed at various
clini-cal locations in Toronto. Interviewers wrote field notes
describ-ing each session (e.g., nonverbal communication and their
impressions about the interview) in order to inform future
in-terviews and data analysis.
Analysis
Interviews were transcribed verbatim, uploaded into NVivo
8
26and coded immediately after each interview to inform the
conduct and content of later interviews. The interview guide
was iteratively reviewed and updated accordingly. Content was
coded into descriptive categories using a constant comparative
method
27and then grouped into descriptive themes
28repre-senting the content of all interviews. Analyst triangulation was
used to establish themes, combining the experience and
per-spectives of a cultural anthropology (GE) and medicine (CT,
LD, RC, PD). Categories and themes from coded transcripts
of the interviews were analysed and refined, until consensus
was reached about the emergent themes in the perceptions,
attitudes and experiences of participants.
29-30Results
Interview participants consisted of individuals with IA
(n=15), their family members and friend (n=6) and HCPs
(n=9). A detailed breakdown of their characteristics is in
Ta-ble 1. Four prominent themes emerged across all interviews:
initial reactions upon hearing the diagnosis of IA, challenges
of living with IA, sources of support to address challenges
(in-formational, emotional, appraisal support), and thoughts on a
peer support intervention as an adjunct to EIA management.
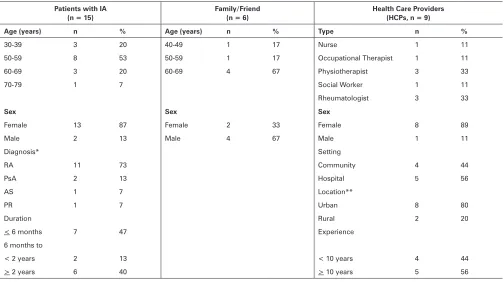
Table 1. Participant Characteristics
Patients with IA (n = 15)
Family/Friend (n = 6)
Health Care Providers (HCPs, n = 9)
Age (years) n % Age (years) n % Type n %
1 17 Nurse 1 11
8 1 17 Occupational Therapist 1 11 Physiotherapist 1 7 Social Worker 1 11 Rheumatologist
Sex Sex Sex
Female 87 Female 2 Female 8 Male 2 Male Male 1 11 Diagnosis* Setting
RA 11 Community
PsA 2 Hospital 5
AS 1 7 Location**
PR 1 7 Urban 8
Duration Rural 2
<NPOUIT 7 Experience NPOUITUP
Initial Reactions to Diagnosis
Patients’ reactions to receiving a diagnosis ranged from
re-lief and acceptance to shock, fear, disbere-lief, and denial. Several
patients were “glad” to learn their diagnosis, as they had had
unexplained symptoms for some time: “I was glad to get a
diag-nosis, to know what was going on and happy to know that there
was medication available” (Patient 108). HCPs also
acknowl-edged that patients may initially experience relief upon
hear-ing their diagnosis: “They are relieved to at least know what
they’ve got…” (HCP 406) Many other participants,
particular-ly HCPs, reported a sense of shock and denial at diagnosis on
the part of patients with IA: “I think sometimes people will start
the medications and then they’ll quickly discontinue them
be-cause they’re scared of them and they want the arthritis to just
go away. They just want to pretend that that isn’t really what’s
happening for them.” (HCP 403)
Challenges
All participants reported a host of challenges, including
delayed diagnosis, disease characteristics such as individuality,
unpredictability and invisibility, and the lifestyle changes the
condition brought in its wake.
Delayed Diagnosis
The importance of an early diagnosis for IA management
was endorsed by more than half of all participants. Participants
thought an earlier diagnosis could have helped with treatment
decisions, improved coping and condition management, and
reduced frustration:
“I guess people couldn’t answer the questions because they
didn’t know exactly what was happening until you run your
tests… But that period [of waiting before being diagnosed]
for the patient is excruciating, because you feel totally
help-less. You feel frustrated.” (Husband 303) More than one-third
of patients felt that their doctors made insufficient time for
them and that appointments were difficult to get. Initial
con-sults with a rheumatologist required wait times up to of three
months, often leading to lengthy periods before final
diagno-sis:
“I sort of dealt with it on my own for about six weeks... Then
I went to my family doc, and then we went through the process
of blood work with him. Then the referral, and then it took
six weeks to get into a doctor, a rheumatologist. So it really did
take probably three months before I was able to see a
rheuma-tologist.” (Patient 201)
Disease Individuality and Unpredictability
Several participants commented that IA can be quite
di-verse in presentation and treatment response, compounding
potential delays: “For a long time I really didn’t know what was
wrong, and I was getting different information. My clinical
pic-ture is really sort of not a classic rheumatoid arthritis picpic-ture.”
(Patient 201) A patient can also be symptom-free for long
pe-riods before sudden pain comes on without warning: “There
have been times where weeks and weeks and weeks, maybe
months have gone by, and then she could have a flare-up”
(Husband 304). HCPs acknowledged that treatment response
can be similarly unpredictable: “It varies from person to person
… you think [a patient] is going to respond one way, but they
do not.” (HCP 407)
Lifestyle Changes
Daily living, work, independence, finances, pregnancy and
personal relationships were all affected by IA. For example, a
lack of access to transportation results in increased reliance on
others for travel to appointments. In response, many patients
incorporated lifestyle changes to manage their condition, such
as an improved diet or doing more or different exercises: “I
am changing the way I’m eating … like I’m eating more salads,
watching my coffee intake and taking more honey, green tea,
and things like that.” (Patient 102)
Pacing and relying on others were suggested as useful
strate-gies to adjust to the demands of living with IA: “They really
need to learn that concept of pacing. If you’re going to exert
yourself to the limit, a good chance is you’re going to be flat
out for a while in a flare” (HCP 403); “You just plan differently
than what you planned before. Today, instead of doing the
whole house, you do one room at a time…” (Patient 203)
These lifestyle changes often led to a subtle change in
iden-tity for individuals with IA, as they learned to relate to
them-selves and others in new ways,
“Now I know that I need professional help, and I’m more
courageous to ask for help. Like I would just ask my son, can
you take me to emergency or can you take me to the doctor?
Or I ask my husband, can you take me to the doctor? I don’t
feel well. So it changed the person that I was.” (Patient 200)
Needs
Post-diagnosis informational, emotional, and appraisal
sup-port were frequently cited as key needs across all three
inter-view groups. For example, many patients and family members
wanted a range of information about potential causes and
out-comes of IA to aid in decision-making and ultimately coping
with the condition. Health care providers were key resources
in this information-gathering process:
“They’ll [patients] ask me, “Why did I get this disease?” We’ll
try to address [the causes] in a very layman’s way. We talk about
why this happened and things that they can control, meaning
if it’s being overweight or whatever it may be, and things that
they can’t control. We talk about what are conservative options
for treatment, what are some of the pharmacotherapy options
for treatment. And, then in my context, for surgical options for
treatment and the patients are always given a choice.” (HCP
401)
may impact on my daily living in the future.” (Patient 201)
Pa-tients and HCPs also noted a change in information needs over
time, in keeping with the course of the disease. One patient
explained, “I feel a lot better, so my immediate needs around
pain management are gone. I think my needs now are more
around prevention and how to prevent a relapse, how to stay
healthy so that I can continue to work for a long time and have
a healthy life.” (Patient 201)
Another noted, “As the disease changes, the questions
change too … as the disease becomes more serious, they ask
whether they can still work or whether they can still do certain
activities. If the disease gets better, they say, ‘Oh, should I now
resume activities, or can I now pursue a different career?’ ”
(HCP 408)
Emotional Support
Emotional support was also considered a key requirement
following diagnosis, especially by family and friends: “My
hus-band has helped me… He’s quite a pillar of support right now
because he sees what’s happening.” (Patient 100)
“I think we all have to recognise that an inflammatory
condi-tion is not just going on in their joints. It’s going on in their
minds. It’s going on in their relationships… There’s a huge
amount of emotional turmoil in people with a diagnosis of a
chronic inflammatory condition, and I just think they need
on-going psychosocial support and recognition.” (HCP 402)
At least three patients acknowledged that their emotional
needs were not being met. They felt unable to discuss their
condition with those closest to them in fear of worrying them
unnecessarily or due to perceived lack of empathy and interest:
“I don’t get any [emotional support] from anybody because
I don’t discuss it…. Nobody wants to hear about it.” (Patient
107); “I really downplay it at work … They’re not very
empa-thetic with people who have something wrong with them.”
(Pa-tient 202)
Appraisal Support
While not many participants explicitly alluded to appraisal
support, it was evident that HCPs, family members and friends
were sources of this type of support: “It is important…my son is
a doctor and my friend. My daughter, my husband, we’re all in
it together.” (Patient 101)
Peer Support
The concept of peer support was well-received by patients,
family and friends: “I think a peer can be really helpful in terms
of working through all of those emotions and the questions…”
(Patient 201). In contrast, HCPs had a more diverse range of
views on peer support. On the positive side, at least half of
HCPs viewed peer support as a complementary source of
infor-mation to what they already provided their patients:
“I think peers … would be very helpful when they talk about
coping mechanisms. So if people are having functional
limita-tions, or they are having difficulty with their activities of daily
living, then having other people to talk to about how they
man-aged that…I think that’s very good.” (HCP 405)
Only limited factual informational support provision was
recommended by HCPs, due to concerns about information
accuracy. Many HCPs mentioned that peers should take on a
role that is “within boundaries”, that is explicitly based on
ex-periential knowledge: “Certainly they could be compassionate
in listening … but I don’t think in a medical environment you
want to be fostering information that the medical environment
knows…is not helpful to the patient. So I think there have to
be some boundaries in that.” (HCP 406)
Other HCPs concerns included potential for burnout of
peer mentors and a sometimes negative atmosphere within
peer support groups: “One of the things that is sometimes
poorly controlled in a support group, is that it really becomes
a complaint circle, and everybody goes out of there feeling
depleted instead of encouraged.” (HCP 402) Despite
limita-tions, HCPs acknowledged the potentially positive impact of
well-trained peers on individuals with IA. Participants across all
groups approved the idea of a peer support intervention: “Peer
support is extremely important… And, you know, very often
people who are hesitant will believe someone else with the
dis-ease before they’ll believe one of the professionals.” (HCP 404)
Role of the Peer
Roles relating to the provision of informational, emotional,
and appraisal support are discussed below:
Informational Support: About one-third of participants
identified experiential information provision as a key peer
mentor role. Desirable information included experiences
deal-ing with challenges, treatment decisions, and strategies
regard-ing lifestyle changes. As one patient explained: “Someone who
has been there for a long time can talk about what they used
to do, how much the new stuff is helping them, everything that
has been successful for them, what hasn’t been successful.”
(Pa-tient 104)
Emotional Support: The provision of emotional support by
a peer included building self-esteem and alleviating fear and
anxiety associated with a diagnosis of IA. Some participants
also saw an opportunity for friendships and mentoring
rela-tionships to develop within the peer-to-peer relationship: “You
can discuss what’s going to happen, what may happen or what
has happened and give that person hope or encouragement.
And I think it alleviates some of the fear that they may
experi-ence …” (Friend 300)
Appraisal Support: At least two participants viewed appraisal
support as a component of emotional support: “Just
confirma-tion that you are making a good decision.” (Patient 104)
Desirable Peer Characteristics: These included compassion,
empathy and being knowledgeable, experienced, supportive,
understanding, and sensitive to participants’ need for privacy.
An effective peer provides direct support, is a good listener,
and “has some knowledge… somebody who would be able
to empathize with the situation….They would have to have a
broad knowledge of what’s out there.” (Patient 103)
Discussion and Conclusions
Interven-tions that address coping and maintaining function can help
improve patients’ health outcomes and reduce reliance on
emergency departments.
14-15Participants identified a number of challenges associated
with diagnosis, such as delayed diagnosis, diversity of disease
presentation, disease unpredictability and invisibility, and
nec-essary lifestyle changes. Factors that may contribute to these
experiences include shortages and geographic variation in
availability of specialists,
31as well as deficiencies in primary care
management of arthritis (i.e., inappropriate referral, general
practitioners’ lack of confidence in doing musculoskeletal
ex-amination).
32-36All three groups interviewed identified a need for
infor-mational, emotional, and appraisal support post-diagnosis.
Support interventions addressing a range of outcomes (e.g.,
health status, self-efficacy, health care use, health behaviours,
perceptions of good heath, bonding with others) are described
in the literature.
37-41In our study, HCPs were frequently cited
as a good source of informational support, but many
partici-pants felt that HCPs did not or could not fully meet their
infor-mational support needs. While all participants saw family and
friends as a source of necessary emotional support after a
diag-nosis of IA, several patients noted that their emotional needs
were not being met by their existing social network. While
ap-praisal support was sought from HCPs, and family and friends,
the degree to which such needs are met is unclear, as appraisal
support was not often explicitly articulated by participants.
This may be because some participants viewed emotional and
appraisal support as synonymous.
Given a stated inability of HCPs to fully address the support
needs of individuals with IA within the HCP-patient
relation-ship, all three groups of study participants thought a peer
sup-port program would be a potentially appropriate and desirable
way to bridge the gap between patients’ needs and existing
sup-port. Peer support models have also been suggested in the
lit-erature as a potentially low-cost, flexible means to supplement
formal healthcare supports provide benefits for both recipients
and peer support providers.
42All groups viewed peer mentors
as a potential way to provide timely informational support
through shared experiences, as well as emotional and appraisal
support, for example by providing feedback on decisions.
Pa-tients and their friends and families were enthusiastic about
the prospect of support from a peer who could empathize
with individual experiences. HCPs also saw value in the use of
peer mentors to provide the emotional and appraisal support,
but were cautious, emphasizing the need for role boundaries.
The subtle disjuncture between HCPs’ attitudes to peer
sup-port compared to those of patients and families points to the
need to design initiatives that are respectful of HCPs’ concerns,
while meeting and advocating for patient needs and not
re-producing the paradigm of medical dominance. For example,
despite potential to empower patients, the Expert Patients
Pro-gramme in the United Kingdom has been criticized for
per-petuating the traditional medical support model and failing to
reach those in most need.
43Our data indicate that the needs of individuals with IA are
not being met by existing social and healthcare relationships
and their self-management may suffer as a result. Doull
et al
.
22argue that a peer with a similar chronic disease is uniquely able
to empathize with an individual’s health situation. A peer
men-tor may, therefore, be seen as a means to bridge support gaps
and enable IA patients to better manage their condition. Based
on our findings, and given the successful use of peer support
models to address other health issues,
19-21peer support is
pro-posed as an appropriate method to address unmet needs of
individuals with IA.
Participants identified desirable peer mentor characteristics
such as empathy, knowledge and understanding and noted
that peer support must be context-driven and tailored to meet
individual needs and life circumstances. Attributes such as
class, gender, and ethnicity must be considered when matching
peers to patients. Research on peer support and chronic
dis-ease suggests compatibility and perceptions of similarity (i.e.,
same age range, stage of life, life circumstances between peers)
are important.
44-47Sharing the same disease experience may
not be enough to establish common ground between peers.
46Other studies suggest benefits accrue that do not appear to be
dependent on participant similarity or shared diagnosis
48and
that variations (e.g. disease, level of knowledge) in a program
may be a strength.
49Nonetheless, our study suggests a peer
sup-port program sensitive to diverse needs may be an effective
ad-junct to clinical care and may help persons with EIA to better
manage their condition.
Limitations include the single-centre structure and the
fact that research took place within the context of a universal
health care system, such that experiences may be specific to
these settings. Also, this needs assessment focused solely on IA,
and findings may not be applicable to other chronic disease
populations. While results may not be generalizable to the
larger IA population or other chronic disease populations, this
study provides added value to existing research on peer
sup-port in chronic disease by addressing a relatively unexplored
topic of peer support in individuals with EIA. These findings
are informing the development of a new peer support
inter-vention tailored to the EIA population. We are optimistic that
early peer support will reduce the burden that IA places on
the healthcare system by assisting individuals with EIA to better
manage their condition.
Acknowledgements
We the authors would like to thank the research team:
Jo-anna Sale, Joan Sargeant, Peter Tugwell, Sydney Brooks, Susan
Ross, Ruth Tonon, Dawn Richards, Jennifer Boyle, Kerry
Knick-le, Nicky Britten, Sharron Sandhu, Emma Bell, Laure Perrier,
Fiona Webster, Mary Cox-Dublanski. We would also like to
ac-knowledge the important role of the research participants.
References
1. Perruccio AV, Power JD, Badley EM. Revisiting arthritis prevalence pro-jections--it’s more than just the aging of the population. J Rheumatol 2006;33:1856-62.
2. Kvien TK. Epidemiology and burden of illness of rheumatoid arthritis. Pharmacoeconomics. 2004;22(2 Suppl):1-12.
3. Ward MM, Leigh JP, Fries JF. Progression of functional disability in patients with rheumatoid arthritis. Associations with rheumatology subspecialty care. Arch Intern Med 1993;153:2229-37.
5. Power JD, Perruccio AV, Badley EM. Ambulatory Physician Care for Muscu-loskeletal Disorders in Canada. J Rheumatol 2006;33:133-9.
6. Beaulieu M, Choquette D, Rahme E, Bessette L, Carrier R. CURATA: A patient health management program for the treatment of osteoarthritis in Québec: an integrated approach to improving the appropriate utili-zation of anti-inflammatory/analgesic medications. Am J Manag Care 2004;10:569-75.
7. Glazier RH, Badley EM, Wright JG, Coyte PC, Williams JI, Harvey B, et al. Patient and provider factors related to comprehensive arthritis care in a community setting in Ontario, Canada. J Rheumatol 2003;30:1846-50. 8. Hernandez-Garcia C, Vargas E, Abasolo L, Lajas C, Bellajdell B, Morado
IC, et al. Lag time between onset of symptoms and access to rheumatology care and DMARD therapy in a cohort of patients with rheumatoid arthritis. J Rheumatol 2000;27:2323-8.
9. Irvine S, Munro R, Porter D. Early referral, diagnosis, and treatment of rheumatoid arthritis: evidence for changing medical practice. Ann Rheum Dis 1999;58:510-3.
10. Suter LG, Fraenkel L, Holmboe ES. What factors account for referral delays for patients with suspected rheumatoid arthritis? Arthritis Rheum 2006;55:300-5.
11. Anderson JJ, Wells G, Verhoeven AC, Felson DT. Factors predicting re-sponse to treatment in rheumatoid arthritis: the importance of disease du-ration. Arthritis Rheum 2000;43:22-9.
12. Mottonen T, Hannonen P, Korpela M, Nissila M, Kautiainen H, Ilonen J, et al. Delay to institution of therapy and induction of remission using sin-gle-drug or combination-disease-modifying antirheumatic drug therapy in early rheumatoid arthritis. Arthritis Rheum 2002;46:894-8.
13. Wiles NJ, Lunt M, Barrett EM, Bukhari M, Silman AJ, Symmons DP, et al. Reduced disability at five years with early treatment of inflammatory poly-arthritis: results from a large observational cohort, using propensity models to adjust for disease severity. Arthritis Rheum 2001;44:1033-42.
14. Lorig KR, Ritter P, Stewart AL, Sobel DS, Brown BW Jr, Bandura A, et al. Chronic Disease Self-Management Program: 2-Year Health Status and Health Care Utilization Outcomes. Med Care 2001;39:1217-23.
15. Combe B, Landewe R , Lukas C, Bolosiu HD, Breedveld F, Dougados M, et al. EULAR recommendations for the management of early arthritis: report of a task force of the European Standing Committee for Interna-tional Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis. 2007;66:34-45.
16. Holbrook AM. Ontario treatment guidelines for osteoarthritis, rheumatoid arthritis, and acute musculoskeletal injury. Toronto: Queen’s Printer of On-tario; 2000.
17. Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW, Dieppe P, et al. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2003;62:1145-55.
18. Keysor JJ, DeVellis BM, DeFriese GH, DeVellis RF, Jordan JM, Konrad TR, et al. Critical review of arthritis self-management strategy use. Arthritis Rheum 2003;49:724-731.
19. Malchodi CS, Oncken C, Dornelas EA, Caramanica L, Gregonis E, Curry SL. The effects of peer counseling on smoking cessation and reduction. Obstet Gynecol 2003;101:504-10.
20. Morisky DE, Ang A, Coly A, Tiglao TV. A model HIV/AIDS risk reduc-tion programme in the Philippines: a comprehensive community-based approach through participatory action research. Health Promot Int 2004;19:69-76.
21. Keyserling TC, Samuel-Hodge CD, Ammerman AS, Ainsworth BE, Hen-riquez-Roldan CF, Elasy TA, et al. A randomized trial of an intervention to improve self-care behaviors of African-American women with type 2 diabe-tes: impact on physical activity. Diabetes Care 2002;25:1576-83.
22. Doull M, O’Connor AM, Robinson V, Tugwell P, Wells GA. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2005;3:CD005352. DOI: 10.100214651858.CD005352.
23. Dennis CL. Peer support within a health care context: A concept analysis. Int J Nurs Stud 2003;40:321–32.
24. Scott DL, Smith C, Kingsley G. What are the consequences of early rheumatoid arthritis for the individual? Best Pract Res Clin Rheumatol. 2005;19:117-36.
25. Evers AW, Kraaimaat FW, Geenen R, Jacobs JW, Bijlsma JW. Pain coping and
social support as predictors of long-term functional disability and pain in early rheumatoid arthritis. Behav Res Ther 2003;41:1295-310.
26. NVivo qualitative data analysis software; QSR International Pty Ltd. Version 8, 2008.
27. Strauss A, Corbin J. Basics of qualitative research: Techniques and proce-dures for developing grounded theory, 3rd ed. Thousand Oaks: Sage Pub-lications, 2008.
28. Boyatzis RE. Transforming qualitative information: thematic analysis and code development. Thousand Oaks, California: Sage; 1998. 200 p. 29. Kuzel A. Sampling in qualitative inquiry. In: Crabtree B Miller W, eds.
Doing Qualitative Research. 2nd ed. Thousand Oaks, California: Sage; 1999;33–45.
30. Mays N, Pope C. Rigour and qualitative research. BMJ. 1995;311:109-12. 31. Health Canada. Arthritis in Canada: An Ongoing Challenge. Ottawa,
On-tario, Health Canada 2003.
32. Glazier RH, Dalby DM, Badley EM, Hawker GA, Bell MJ, Buchbinder R. Determinants of physician confidence in the primary care management of musculoskeletal disorders. J Rheumatol 1996;23:351-6.
33. Glazier RH, Dalby DM, Badley EM, Hawker GA, Bell MJ, Buchbinder R, et al. Management of the early and late presentations of rheumatoid arthritis: A survey of Ontario primary care physicians. CMAJ 1996;155:679-87. 34. Glazier RH, Dalby DM, Badley EM, Hawker GA, Bell MJ, Buchbinder R, et
al. Management of common musculoskeletal problems: A survey of On-tario primary care physicians. CMAJ 1998;158:1037-40.
35. Lillicrap MS, Byrne E, Speed CA. Musculoskeletal assessment of general medical in-patients--joints still crying out for attention. Rheumatology (Ox-ford) 2003;42:951-4.
36. Speed CA, Crisp AJ. Referrals to hospital-based rheumatology and ortho-paedic services: Seeking direction. Rheumatology (Oxford) 2005;44:469-71.
37. Campbell HS, Phaneuf MR, Deane K. Cancer peer support programs—do they work? Patient Educ Counsel 2004;55:3-15.
38. Coward DD, Kahn DL. Transcending breast cancer: making meaning from diagnosis and treatment. J.Holist.Nurs 2005;23:264-286
39. Foster G, Taylor SJC, Eldridge S, Ramsay J, Griffiths CJ. Self-management education programmes by lay leaders for people with chronic conditions. Cochrane Database Syst Rev 2007;4:CD005108. DOI: 10.1002/14651858. CD005108.pub2.
40. Lorig KR, Ritter PL, Dost A, Plant K, Plaurent DD, McNeil I. The Expert Patients Programme online, a 1-year study of an internet-based self-man-agement programme for people with long-term conditions. Chronic Illn 2008;4:247-56.
41. Riemsma RP, Kirwan JR, Taal E, Rasker JJ. Patient education for adults with rheumatoid arthritis. Cochrane Database Syst Rev 2003;2:CD003688. DOI: 10.1002/14651858.CD003688.
42. Heisler M. Overview of peer support models to improve diabetes self-man-agement and clinical outcomes. Diabetes Spectrum 2007;20:214-21. 43. Wilson PM, Kendall S, Brooks F. The Expert Patients Programme: A
para-dox of patient empowerment and medical dominance. Health Soc Care Community 2007;15:426-38.
44. Carlsson C, Nilbert M, Nilsson K. Supporter or obstructer; experiences from contact person activities among Swedish women with breast cancer. BMC Health Serv Res 2005;5:9.
45. Horton R, Peterson MG, Powell S, Engelhard E, Paget SA. Users evalu-ate LupusLine, a telephone peer counseling service. Arthritis Care Res 1997;10:257-63.
46. Stewart M, Davidson K, Meade D, Hirth A, Weld-Viscount P. Group support for couples coping with a cardiac condition. J Adv Nurs 2001;33:190-9. 47. Sutton LB, Erlen JA. Effects of mutual dyad support on quality of life in
women with breast cancer. Cancer Nurs 2006;29:488-98.
48. Barlow JH, Bancroft GV, Turner AP. Volunteer, lay tutors’ experiences of the Chronic Disease Self-Management Course: Being valued and adding value. Health Educ Res 2005;20:128-36.