Estimation of Optimal CPR Chest Compression Depth
in Children by Using Computer Tomography
WHAT’S KNOWN ON THIS SUBJECT: Specific evidence for target chest compression depth parameters in children are not known or published, and thus therapeutic targets for pediatric chest compressions are based on extrapolation and extension from adults, animal models, and consensus interpretation of the literature.
WHAT THIS STUDY ADDS: We characterized chest depths of children by using chest computed tomography. These data were used to understand further the maximum absolute and maximum relative depths of chest compressions and could lead to improved guidelines for chest compressions in children.
abstract
OBJECTIVE:Pediatric consensus-driven cardiopulmonary resuscita-tion guidelines target chest compression (CC) depths of one third to one half anterior-posterior (AP) chest depth. Estimates for this target as assessed by computed tomography (CT) measurements of internal and external AP chest dimensions could direct future pediatric cardio-pulmonary resuscitation guidelines.
METHODS:A total of 280 consecutive chest CT scans in permuted blocks of 20 for each of 14 age divisions between 0 and 8 years were reconstructed and analyzed. External and internal AP depths were measured at midsternum, and residual chest depth was calculated at simulated one-third and one-half AP compressions.
RESULTS:After a simulated compression calculation, one-half exter-nal AP depth CC would result in residual interexter-nal depth of⬍10 mm for 94% (263 of 280) of children 3 months to 8 years. For a one-third external AP CC, only 0.4% (1 of 280) of children 3 months to 8 years had a calculated residual internal chest depth⬍10 mm.
CONCLUSIONS:By using CT reconstruction estimates of chest dimen-sions across the developmental spectrum from 0 to 8 years of age, we demonstrated that a simulated CC targeting approximately one-third external AP chest depth seems radiographically appropriate for chil-dren aged 3 months to 8 years, whereas simulated CC targeting ap-proximately one-half external AP chest depth seems radiographically to be too deep, resulting in residual internal chest depth of⬍10 mm for most patients of this age.Pediatrics2009;124:e69–e74
CONTRIBUTORS:Matthew S. Braga, MD,aTroy E. Dominguez,
MD,bAvrum N. Pollock, MD,cDana Niles, MS,bAndrew Meyer,
MD,dHelge Myklebust, PhD,eJon Nysaether, PhD,eand Vinay
Nadkarni, MDb
aDivision of Pediatric Critical Care Medicine,
Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire; Departments ofbAnesthesiology and Critical Care Medicine, cRadiology, anddNeonatology, Children’s Hospital of
Philadelphia, Philadelphia, Pennsylvania;eDepartment of
Research and Development, Laerdal Medical AS, Stavanger, Norway
KEY WORDS
chest films, pediatrics, pediatric advance life support, resuscitation
ABBREVIATIONS
CC— chest compression AHA—American Heart Association ERC—European Resuscitation Council
ILCOR—International Liaison Committee on Resuscitation CPR— cardiopulmonary resuscitation
CT— computed tomography AP—antero-posterior
The views expressed in the manuscript are of the authors and are not meant to represent the position of the American Heart Association or the International Liaison Committee on Resuscitation.
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0153
doi:10.1542/peds.2009-0153
Accepted for publication Feb 24, 2009
Address correspondence to Matthew Braga, MD, Pediatric Critical Care, Children’s Hospital at Dartmouth, Dartmouth-Hitchcock Medical Center, One Medical Center Dr, Lebanon, NH 03756-0001. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
low. Donoghue et al1reported only 4% neurologically intact survival overall out-of-hospital. In-hospital, ⬃17% of children survive and 13% of adults sur-vive neurologically intact.2Survival to return of spontaneous circulation, hospital admission, and hospital dis-charge has been associated with qual-ity of chest compressions (CCs) in adults, in particular adequate depth of compression.3Current adult CC guide-lines specify that a CC depth target of 38 to 51 mm corresponds to⬃16% to 21% relative depth of the adult chest.4 Real-time directive and corrective feedback can improve adherence to these guidelines and resuscitation outcomes.5 The American Heart As-sociation (AHA), European Resuscita-tion Council (ERC), and InternaResuscita-tional Liaison Committee on Resuscitation (ILCOR) guidelines and treatment rec-ommendations were created by con-sensus, and the relative depth of CC was estimated grossly and without ev-idence of internal and external chest depths. Specific evidence for target depth of CC parameters in children are not known or published; thus, thera-peutic targets for pediatric CCs are based on extrapolation and extension from adults, animal models, and con-sensus interpretation of the literature. AHA pediatric cardiopulmonary resus-citation (CPR) guidelines 2000 stated that CCs provide circulation as a result of changes in intrathoracic pressures and/or direct compression of the heart. In Guidelines 2000, the recommended target of compression depth for chil-dren is approximately one third to one half the depth of the chest (1.0 –1.5 in).6 In Guidelines 2005, no new research data that support specific CC depth targets were presented. The previous recommendation of a target depth of 1.0 to 1.5 in has been removed. For chil-dren 1 to 8 years of age, the AHA rec-ommends “approximately one third to
“approximately one third of the depth of the chest,”7and ILCOR recommends “approximately one third the anterior-posterior diameter of the chest.”8
The purpose of this study was to char-acterize the internal and external chest depths of children of various ages between the ages of 0 to 8 years by using chest computed tomography (CT) technology. These data can then be used to understand further the maximum absolute and maximum rel-ative depths of CCs that can be per-formed on children and to provide evidence-based guidance for CPR feed-back devices in the future. The evi-dence from this study could emphasize the lack of data to support current pe-diatric CC guidelines and begin to question the safety and efficacy of these current guidelines. Our second-ary objective was to calculate and esti-mate residual internal chest depths if simulated external CCs of one-half, one-third, and one-fifth external an-tero-posterior (AP) chest depth were delivered. We hypothesized that CT re-construction estimates of chest di-mensions across the developmental spectrum from 0 to 8 years would dem-onstrate that simulated CC targeting approximately one-third external AP CC depth seems appropriate for chil-dren 3 months to 8 years.
METHODS
General Schema of Study Design and Subject Enrollment
This study was a retrospective study approved by the institutional review board at the Children’s Hospital of Philadelphia. All pediatric chest CT scans previously performed by the ra-diology department at the Children’s Hospital of Philadelphia were consid-ered eligible except for patients with severe scoliosis or obvious major chest wall deformities (pectus excavatum/
scans that were available were re-viewed and analyzed for each age group: ⬍3 months, 3 months to ⬍6 months, 6 months to ⬍9 months, 9 months to⬍12 months, 12 months to
⬍15 months, 15 months to ⬍18 months, 18 months to ⬍21 months, 21 months to ⬍2 years, 2 years to
⬍3 years, 3 years to⬍4 years, 4 years to⬍5 years, 5 years to ⬍6 years, 6 years to ⬍7 years, and 7 years to
⬍8 years. By using CT reconstruction, individual chest depths were mea-sured and residual internal depth re-sulting from several simulated CC depths was calculated. Measurements were assessed by using objective mea-surement scales and were supervised and confirmed by an attending radiol-ogist expert in pediatric chest CT.
We next examined the percentages of patients who would have⬍10 mm of residual chest depth during a simu-lated one-half external AP chest depth compression. Our investigative team prospectively selected 10-mm residual chest depth as a cutoff by consensus, because we believed that⬍10 mm re-sidual chest depth would still have the potential to injure the intrathoracic structures and may not actually be achievable because of the presence of the thickness of the myocardium.
Sample Size and Power
From pilot studies of children, the co-efficient of variation for measuments of chest depth have been re-ported to be⬃10% to 13%.9Given this known variability, a sample of 20 pa-tients in each age group was chosen to limit the calculated 95% confidence interval for measurements in each group to⬍0.5 cm in infants and up and
years into 14 age groups, thereby giv-ing a total number of 280 CT scans to review.
Analysis
Internal and external chest depth mea-surements were performed as demon-strated in Fig 1. By using an axial slice at the midsternal level below the level of the intermammary line and in the typical location where CCs are deliv-ered, we calculated the external chest depth by measuring a line drawn per-pendicularly from the skin anteriorly to the skin posteriorly. In addition, we calculated the internal depth available by measuring a line drawn perpendic-ularly from the posterior midsternum to the anterior vertebral body. The depth of a proposed CC was calculated for one half (50%), one third (33%), and one fifth (20%) the measured ex-ternal chest depth. Residual inex-ternal chest depth after simulated CC was calculated as the internal chest depth from chest CT scan minus the depth of the proposed CC (assuming that the full depth of the CC would be transmit-ted to the internal structures).
Graphic representation of the range of internal and external chest depth measured across age groups was displayed by using box and whisker
plots. We performed multiple regres-sion to assess the association between changes in measurements with age and gender. We calculated the pro-portion of patients with measured re-sidual chest depths of ⬍0-mm and
⬍10-mm residual chest depth across age groups for both the calculated compression depths and adult recom-mendations (38 –51 mm). A value of 0 mm would indicate that no remaining internal chest depth would available during the simulated CC, and a nega-tive value would suggest that it would be impossible to compress to that par-ticular target depth because of there not being enough available internal chest depth to accommodate the CC. A positive value would reflect the re-maining available internal chest depth after a simulated CC.
RESULTS
Figure 2 displays the internal and ex-ternal chest depths by age. The pre-dicted internal AP depth was found to be y (mm) ⫽ 51.7 ⫹ 0.38 * age (months)⫹3.4 * male (yes⫽1, no⫽ 0) (R2⫽0.69,P⬍.001).
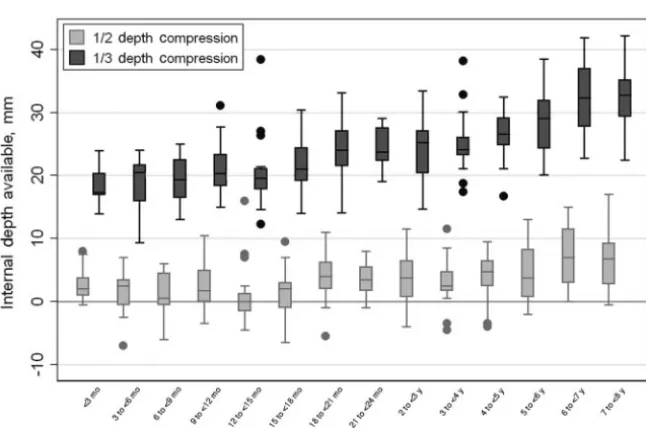
Figure 3 displays residual internal chest depth during simulated one-third and one-half AP external chest depth compressions. As with the
mea-sured internal chest depths, the resid-ual internal chest depth measure-ments available for compression also increased with age (P⬍.001 for both one-half and one-third external chest depth compressions).
Figure 4 displays the percentage of pa-tients in each age group with⬍0 mm and⬍10 mm of residual internal chest depth during a one-half AP external chest depth compression. For one-half external AP CC, 94% (263 of 280) of chil-dren aged 3 months to 8 years had a calculated residual internal chest depth⬍10 mm. For one-third external AP CC, only 0.4% (1 of 280) of children aged 3 months to 8 years had a calcu-lated residual internal chest depth
⬍10 mm.
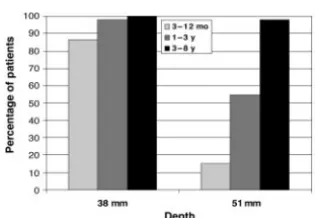
Figure 5 displays residual internal chest depth during a simulated one-fifth (20%) chest depth compression. Figure 6 displays the percentage of pe-diatric patients with⬎10 mm of resid-ual internal chest depth during the current adult recommended 38-mm (1.5 in) and 51-mm (2 in) simulated CC.
DISCUSSION
This is one of the first studies to at-tempt to evaluate and challenge objec-tively the current pediatric CC depth recommendations. The current AHA, ERC, and ILCOR recommendations are extrapolated from adult data and are consensus based. This study suggests that the current recommendations of one-third to one-half external AP chest depth are not ideal and may not be at-tainable or safe for all children. With a one-half chest depth compression, 25% of patients in the 3- to 12-month group would theoretically have no re-sidual internal depth. This suggests that during a one-half AP CC, there would be no room for the intrathoracic structures, including the heart and great vessels. This may actually be im-possible to achieve but if achievable could potentially be harmful to the FIGURE 1
CT scan demonstrating axial image at the midsternal level and method for calculating external and internal chest depth.
structures being compressed. This is also the case for 21% of 1- to 3-year-olds and 8% of 3- to 8-year-old children.
The percentages of patients who would have⬍10 mm of residual chest depth during a simulated one-half ex-ternal AP chest depth compression are displayed in Fig 4. These results sug-gest that during a one-half external AP
CC, 98% of 3- to 12-month-olds would have⬍10 mm of residual chest depth; 96% of 1- to 3-year-olds and 88% of 3- to 8-year-olds would also have⬍10 mm of residual chest depth during a one-half AP CC. As mentioned in the meth-ods, we prospectively selected 10-mm residual chest depth as a cutoff by con-sensus, because we believed that
⬍10-mm residual chest depth would still have the potential to injure the in-trathoracic structures and may actu-ally not be achievable because of the presence of the thickness of the myo-cardium. We believed that this was a very conservative estimate of “over-compression.” Because 10 mm of re-sidual chest depth still may not be enough to accommodate the intratho-racic structures, these results provide more impressive data suggesting that a one-half external AP chest depth compression may not be achievable or safe for young children.
For completeness, we further calcu-lated and compared our findings with current adult CC depth recommenda-tions. Pickard et al10found that the ex-ternal compression depth target for adults, 38 to 51 mm, corresponds to
⬃16% to 20% relative depth of com-pression for male adults and 17% to 21% for female adults. The residual in-ternal chest depth during a simulated 20% external AP CC (Fig 5) suggests that all pediatric patients would have
⬎20 mm of residual internal depth (100%⬎10 mm, as well). We then mea-sured the residual internal depth dur-ing the current adult recommended CC of 38 mm and 51 mm (Fig 6). During a 38-mm simulated CC, 86% of 3- to 12-month-olds, 98% of 1- to 3-year-olds, and 100% of 3- to 8-year-olds would have⬎10 mm of residual chest depth. During a 51-mm simulated CC, 15% of FIGURE 2
Box-and-whisker plot of internal and external chest depth by age. The predicted internal AP chest depth was found to be y (mm)⫽51.7⫹0.38 * age (months)⫹3.4 * male (yes⫽1, no⫽0) (R2⫽0.69,
P⬍.001).
FIGURE 3
Box-and-whisker plot of calculated residual internal chest depth by age during one-half and one-third external AP chest depth compression.
⬍
3- to 12-month-olds, 55% of 1- to 3-year-olds, and 98% of 3- to 8-year-olds would have⬎10 mm of residual chest depth. These findings suggest that for 3- to 8-year-olds, the current adult recom-mendations of 38 to 51 mm might be a safe alternative to the current pediat-ric recommendations. For the 3-month to 3-year-old, a 51-mm CC seems to be too deep, but a 38-mm CC would poten-tially be a safe alternative.
We believe that this study will have a positive impact on the current field of pediatric resuscitation by providing radiographic evidence for CC depth recommendations that are
approxi-mately one third the external AP depth of the pediatric chest. With the grow-ing field of CPR real-time-assist and feedback technologies, it has become more important than ever to ensure that the current goal CC depths are both safe and attainable in the pediat-ric population, because these recom-mendations are anticipated to be pro-grammed into the CPR feedback technologies. Thus, the information ob-tained from this study begins to ques-tion the current CC depth guidelines and provide a basis for additional re-search into these recommendations.
Target parameters for delivery of CCs should generally apply to the wide range and spectrum of chest wall characteristics of patients across the pediatric spectrum. Thus, therapeutic targets for feedback and quality assur-ance of pediatric CCs should focus on the delivery of adequately deep and fast compressions, with efforts to pro-mote full release according to current consensus treatment recommenda-tions and guidelines.
Our study is a retrospective, an obser-vational, and a single-center study and
thus is limited by the patient selection, which includes a variety of children who underwent chest CT scans at the Children’s Hospital of Philadelphia. Al-though we did have strict exclusion cri-teria for those with chest wall deformi-ties, we did not describe in detail patients who were included. The in-cluded patients did have a variety of prescan diagnoses ranging from pneu-monia and tumors to congenital ab-normalities. This patient selection may not be identical to patients who re-quire CCs and eliminates those with severe thoracic deformity. In our anal-ysis, we also assumed that the exter-nal diameter of the chest does not change as a result of the compres-sions. This could happen if the chest collapses or if the position of the chest in the release phase is modified by the compressions (eg, as a result of lean-ing). The major limitation to this study is that measurements were performed in 2 dimensions and without any hemo-dynamic information supporting ideal CC depth. On the basis of this study, additional specific volumetric analysis of the chest cavity and that of the heart both before and during a CC is war-ranted. With the advancing field of di-agnostic radiology, measuring static and dynamic volumes of the chest cav-ities and heart is becoming more prac-tical. A final limitation is that we did not account for potential soft tissue com-pressibility during our calculated ex-ternal CCs when we performed our cal-culations. We assumed that all of the one-third or one-half external AP chest depth compressions would be trans-lated to the internal chest depth. Some patients may have more or less soft tissue around the sternum and back that would have absorbed some of the CC and could have caused an overesti-mation of the actual CC depth trans-lated to the internal chest depth. We believe this to be a very small amount of compressibility.
FIGURE 5
Box-and-whisker plot of calculated residual internal chest depth during a 20% external AP CC by age.
FIGURE 6
Percentage of patients with⬎10-mm residual internal chest depth during a 38-mm (1.5 in) and 51-mm (2 in) AP CC.
chest dimensions across the develop-mental spectrum from 0 to 8 years of age, we demonstrated that simulated CC targeting approximately one-third external AP chest depth seems appro-priate for the majority of children aged 3 months to 8 years. Simulated CC tar-geting approximately one-half external AP chest depth may be too deep, result-ing in residual internal chest depth of
⬍10 mm. Current consensus-recom-mended one-third to one-half external AP chest depth may not be feasible or desirable for all children who are younger than 8 years and might need
of a constant CC depth target of 38 mm would be expected to be adequate for
⬎98% of 1 to 8-year-old children, with
⬎10 mm of residual chest depth. This simulated CC study suggests that addi-tional studies should be conducted to confirm these findings with actual CC and with hemodynamic measures dur-ing real CPR.
ACKNOWLEDGMENTS
Dr Nadkarni receives unrestricted grant support from the Laerdal Foun-dation for Acute Care Medicine; Medi-cal Education Technologies, Inc; Agency
Nadkarni has served as the Chair-man of the Emergency Cardiovascular Care Committee of the American Heart Association and is the current co-chairman of ILCOR.
We thank the Center for Simulation, Advanced Education, and Innovation at the Children’s Hospital of Philadelphia; Center for Resuscitation Science at the University of Pennsylvania School of Medicine; and Kristy Arbogast, PhD, Matthew Maltese, MS, Robert A. Berg, MD, Stephanie Tuttle, MBA, Naoki Shimizu, MD, Mark Helfaer, MD, and Akira Nishisaki, MD.
REFERENCES
1. Donoghue AJ, Nadkarni V, Berg RA, et al. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge.Ann Emerg Med.2005;46(6):512–522
2. Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults.JAMA.2006;295(1):50 –57
3. Edelson DP, Abella BS, Kramer-Johansen J, et al. Effects of compression depth and pre-shock pauses predict defibrillation failure during cardiac arrest.Resuscitation.2006;71(2):137–145 4. ECC Committee, Subcommittees and Task Forces of the American Heart Association. 2005
Amer-ican Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovas-cular care.Circulation.2005;112(24 suppl):IV1–IV203
5. Kramer-Johansen, Myklebust H, Wik L, et al. Quality of out-of-hospital cardiopulmonary resusci-tation with real time automated feedback: a prospective interventional study.Resuscitation.
2006;71(3):283–292
6. American Heart Association in collaboration with International Liaison Committee on Resuscita-tion. Guidelines 2000 for cardiopulmonary resuscitation and emergency cardiovascular care.
Circulation.2000;102(8 suppl):I1–I384
7. Biarent D, Bingham R, Richmond S, et al. European Resuscitation Council guidelines for resusci-tation 2005: section 6 —paediatric life support.Resuscitation.2005;67(suppl 1):S97–S133 8. International Liaison Committee on Resuscitation. 2005 international consensus on
cardiopulmo-nary resuscitation and emergency cardiovascular care science with treatment recommenda-tions.Circulation.2005;112(8)[suppl 1]:III-73–III-90
9. Pedersen IM, Hermans JJ, Molenbroek JF. Measurement of the Sternum for Better Cardiopulmo-nary Resuscitation. Abstract presented at the Nordic Ergonomics Society conference; October 1–3, 2007; Lysekil, Sweden
DOI: 10.1542/peds.2009-0153
2009;124;e69
Pediatrics
Meyer, Helge Myklebust, Jon Nysaether and Vinay Nadkarni
Matthew S. Braga, Troy E. Dominguez, Avrum N. Pollock, Dana Niles, Andrew
Computer Tomography
Estimation of Optimal CPR Chest Compression Depth in Children by Using
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/1/e69
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/1/e69#BIBL
This article cites 9 articles, 1 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/radiology_sub
Radiology
sub
http://www.aappublications.org/cgi/collection/emergency_medicine_
Emergency Medicine following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2009-0153
2009;124;e69
Pediatrics
Meyer, Helge Myklebust, Jon Nysaether and Vinay Nadkarni
Matthew S. Braga, Troy E. Dominguez, Avrum N. Pollock, Dana Niles, Andrew
http://pediatrics.aappublications.org/content/124/1/e69
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.