Comparison of Minitrampoline– and Full-Sized Trampoline–Related
Injuries in the United States, 1990 –2002
Brenda J. Shields, MS*; Soledad A. Fernandez, PhD‡; and Gary A. Smith, MD, DrPH*§
ABSTRACT. Objective. To compare mini- and full-sized trampoline–related injuries in the United States.
Methods. A retrospective analysis of data was con-ducted for all ages from the National Electronic Injury Surveillance System (NEISS) of the US Consumer Prod-uct Safety Commission from 1990 to 2002. We compared 137 minitrampoline-related injuries with 143 full-sized trampoline–related injuries, randomly selected from all full-sized trampoline–related injuries reported to the NEISS during the study period.
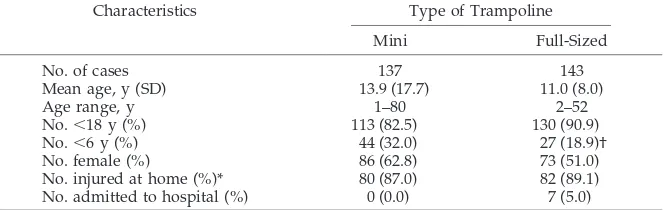
Results. Patients ranged in age from 1 to 80 years (mean [SD]: 13.9 [17.7]) and 2 to 52 years (mean [SD]: 11.0 [8.0]) for mini- and full-sized trampoline–related injuries, respectively. Most patients were younger than 18 years (82% mini, 91% full-sized). Thirty-two percent of minitrampoline- and 19% of full-sized trampoline– related injuries were to children who were younger than 6 years; girls predominated (63% mini, 51% full-sized). Children who were younger than 6 years were more likely to be injured on a minitrampoline than on a full-sized trampoline, when compared with 6- to 17-year-olds (odds ratio [OR]: 2.43; 95% confidence interval [CI]: 1.33– 4.47). The majority of injuries occurred at home (87% mini, 89% full-sized). All patients who were injured on a minitrampoline were treated and released, whereas 5% of patients who were injured on a full-sized trampoline were admitted to the hospital. On minitrampolines, chil-dren who were younger than 6 years were at risk for head lacerations (OR: 4.98; 95% CI: 1.71–16.03), and chil-dren who were 6 to 17 years were at risk for lower extremity strains or sprains (OR: 6.26; 95% CI: 1.35–59.14). Children who were 6 to 17 years and injured on a full-sized trampoline were at risk for lower extremity strains or sprains (OR: 4.85; 95% CI: 1.09 – 44.93). Lower extremity strains or sprains were the most common injury sus-tained by adults (18 years and older; 33% mini, 15% full-sized).
Conclusions. Injury patterns were similar for mini-and full-sized trampolines, although minitrampoline–re-lated injuries were less likely to require admission to the hospital and more commonly resulted in head lacerations among children who were younger than 6 years. Risk for injury could not be determined because of the lack of
data regarding duration of exposure to risk. We therefore conclude that the use of full-sized trampolines by chil-dren should follow the policy recommendations of the American Academy of Pediatrics. Trampolines, includ-ing minitrampolines, should be regarded as traininclud-ing de-vices and not as toys. Until more data are available re-garding exposure to risk, we caution against the use of the minitrampoline as a play device by children in the home, which is where most minitrampoline-related inju-ries occur. Pediatrics 2005;116:96–103; trampoline, mini-trampoline, injury.
ABBREVIATIONS. AAP, American Academy of Pediatrics; CPSC, United States Consumer Product Safety Commission; ED, emer-gency department; NEISS, National Electronic Injury Surveillance System; OR, odds ratio; CI, confidence interval.
G
eorge Nissen was inspired to invent the “bouncing table,” later renamed the trampo-line, in 1937 after watching tightrope walkers and trapeze artists perform twists, spins, and somer-saults into safety nets at the circus.1As trampoline use increased in popularity, so did the frequency of associated injuries. The first trampoline-related injuries were reported in 1956 by Zimmer-man2and in 1960 by Ellis et al.3Spinal cord injuries are the main severe injury associated with trampo-lines.4–7 Most of these injuries involve the cervical spine and result in quadriplegia.4–7The minitrampo-line is also associated with risk for spinal cord injury, most notably from poorly executed somersaults.8,9 By the late 1990s, despite the recommendation of the American Academy of Pediatrics (AAP) that tram-polines not be used in home or recreational settings, recreational trampoline-related injuries reached “ep-idemic proportions,” as reported by Furnival et al.10 Almost all of the trampolines associated with these injuries were at private homes, usually in back-yards.10–13Most of the injuries occurred on full-sized trampolines.11Relatively few studies have focused exclusively on trampoline-related injuries in the pediatric popula-tion,13–20 and even fewer have described minitram-poline-related injuries.14,21,22 Therefore, the goal of our study was to describe and compare mini- and full-sized trampoline–related injuries among chil-dren and adults in the United States. More specific, we aimed to (1) compare the types of injuries asso-ciated with minitrampolines with those assoasso-ciated with full-sized trampolines, (2) compare trampoline-related injuries sustained by children (⬍18 years) with those sustained by adults (18 years and older)
From the *Center for Injury Research and Policy, Columbus Children’s Research Institute, Children’s Hospital, Columbus, Ohio; ‡Center for Bio-statistics, Ohio State University, Columbus, Ohio; and §Department of Pediatrics, Ohio State University College of Medicine and Public Health, Columbus, Ohio.
Accepted for publication Oct 14, 2004. doi:10.1542/peds.2004-1326
No conflict of interest declared.
for both types of trampolines, and (3) compare tram-poline-related injuries sustained by children younger than 6 years with those sustained by children 6 to 17 years for both types of trampolines.
METHODS
The US Consumer Product Safety Commission (CPSC) moni-tors consumer product–related injuries that are treated in US hospital emergency departments (EDs) through the National Elec-tronic Injury Surveillance System (NEISS). The NEISS was estab-lished in 1972 with revisions made in its sampling frame in 1978, 1990, and 1997. The NEISS obtains data from a probability sample of 98 hospitals selected from the population of all hospitals with EDs in the United States and its territories.23Projections of injuries that occur nationally are made from this probability sample. Data regarding injuries associated with consumer products and recre-ational activities are collected on a daily basis via computer from each participating hospital. The NEISS has been shown to be highly sensitive and accurate in identifying consumer product– related injury cases.24–27
Data were obtained from the CPSC regarding trampoline-re-lated injuries (product code 1233) reported through the NEISS during the 13-year period 1990 through 2002. Through review of the comment fields for each case, cases were divided into 2 cate-gories: minitrampoline-related and full-sized trampoline–related injuries. A minitrampoline was identified in the comment fields as a minitramp, small tramp, jogging tramp, or exercise tramp. Dur-ing the 13-year study period, 137 minitrampoline-related injuries and 22 997 full-sized trampoline–related injuries were reported to the NEISS. These injuries represent an estimated 5400 minitram-poline-related and 915 500 full-sized trampoline–related injuries nationally. Because of the relatively small number of minitrampo-line-related injury cases, we chose not to weight these cases to make national projections regarding these injuries during data analysis. The minitrampoline cases were compared with a sample of full-sized trampoline cases. Eleven full-sized trampoline–re-lated injury cases were randomly selected from each of the 13 years of the study period (totaln⫽143) in the following manner. All full-sized trampoline–related injury cases were grouped by year of injury. Within each of the 13 years, each case was assigned an identification number, ranging from 1 to the total number of cases for that year. GraphPad Quickcalcs, a random-number gen-erator program,28was used to select randomly 11 case identifica-tion numbers from each of the 13 years. This allowed us to obtain similar sample sizes for the 2 groups while controlling for year of injury.
To evaluate whether the random sample was representative of all full-sized trampoline–related injury cases reported to the NEISS during the study period, we compared values of the major variables to be analyzed (age, gender, body part injured, type of injury, location where the injury event occurred, and disposition from the ED) between the 2 groups using2 anal-yses, with and without Yates correction, and Studentttest. No statistically significant differences were found for any of the vari-ables. The same comparisons were made between the random sample of full-sized trampoline–related injuries and the national projections for all full-sized trampoline–related injuries calculated using the NEISS sample weights. In this comparison, the only significant difference found was the percentage of trampoline-related injuries that occurred at school: 4.3% for the random sample versus 1.2% for all estimated full-sized trampoline–related injuries that occurred in the United States during the study period. It was concluded that the random sample was representative of all full-sized trampoline–related injury cases reported to the NEISS during the 13-year study period.
The type of injury was grouped into 5 categories during study analyses: (1) soft tissue injury (contusion, abrasion, and hema-toma), (2) fracture/dislocation, (3) laceration, (4) strain/sprain, and (5) other (concussion, crushing injury, internal organ injury, and avulsion). Likewise, the body part injured was grouped into 5 categories during study analyses: (1) head (head, face, mouth, and ear), (2) neck, (3) trunk (shoulder, upper trunk, and lower trunk), (4) lower extremity (knee, lower leg, upper leg, ankle, foot, and toe), and (5) upper extremity (elbow, lower arm, upper arm, wrist, hand, and finger). Patients were categorized into 2 main age groups for data analyses: children (younger than 18 years) and
adults (18 years or older). Because the CPSC11recommends that children younger than 6 years not use trampolines, we further divided children into 2 subgroups for analyses: children younger than 6 years and 6- to 17-year-olds.
Data were analyzed using EpiInfo software.29Continuous data were tested for normality using the Kolmogorov-Smirnov test. Bartlett test was used to assess homogeneity of variances. Statis-tical analyses included2analysis, with and without Yates cor-rection, Fisher’s exact 2-tailed test, and the Mann-WhitneyUtest. The level of significance for all statistical tests was␣⫽.05. The computation of odds ratio (OR) with an exact 95% confidence interval (CI)30was also performed.
RESULTS Sample Description
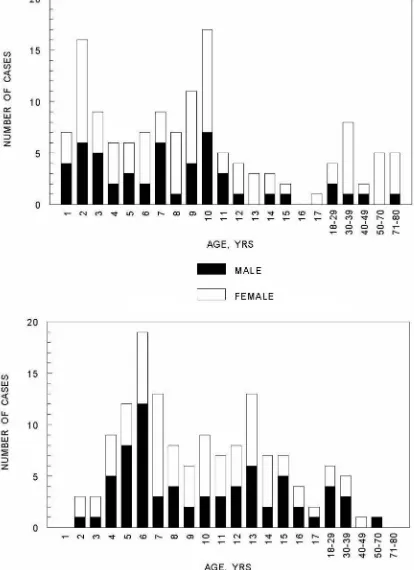
A total of 137 minitrampoline-related injury cases were reported to the NEISS from 1990 through 2002. These patients ranged in age from 1 to 80 years (mean [SD]: 13.9 [17.7] years). A total of 113 (82.5%) patients were younger than 18 years, and 44 (32%) were younger than 6 years. Females predominated (n
⫽ 86 [62.8%]; Fig 1).
A total of 143 full-sized trampoline–related injury cases, randomly selected from all full-sized trampo-line–related injury cases, were reported to the NEISS from 1990 through 2002. These patients ranged in age from 2 to 52 years (mean [SD]: 11.0 [8.0] years). Of these patients, 130 (90.9%) were younger than 18 years and 27 (18.9%) were younger than 6 years. Females accounted for slightly more than half of the cases (n ⫽73 [51.0%]; Fig 1).
There were no statistically significant differences between the minitrampoline and full-sized trampo-line groups with respect to gender, age, or number of patients who were younger than 18 years. However, a significantly greater number of children who were younger than 6 years were injured on a minitrampo-line (OR: 2.43; 95% CI: 1.33– 4.47; P ⬍ .01) when compared with 6- to 17-year-olds.
The annual number of minitrampoline-related in-juries during the 13-year period ranged from 6 to 18 (mean [SD]: 10.5 [3.8]), with peak numbers in 1991 (n⫽16), 1995 (n⫽15), and 2000 (n⫽18). There was no secular trend in the number of minitrampoline-related injuries during the study period. For full-sized trampolines, the number of cases was fixed at 11 per year by our sampling method. Overall, there were more injuries for both types of trampolines during the months of April through October, with the mode in May. Although not statistically signifi-cant, there was a greater number of minitrampoline-related injuries than full-sized trampoline–minitrampoline-related in-juries from November through February.
There was no significant difference between the 2 types of trampolines with respect to the location where the injury event occurred. Most (87.0%) mini-trampoline-related injuries occurred at home, 6.5% occurred at a place of recreation or sports, 5.4% oc-curred at school, and the remaining 1.1% ococ-curred on other public property. Likewise, 89.1% of full-sized trampoline–related injuries occurred at home, 4.3% occurred at a place of recreation or sports, 3.3% oc-curred at school, and the other 3.3% ococ-curred on other public property.
time of injury. Deleting these cases from the analyses did not alter the results of the study. Therefore, they were included in all analyses. The mechanisms of injury for these 18 cases were that the trampoline was dropped or fell onto the patient (n ⫽ 7), the patient unintentionally fell from another object onto the trampoline (n ⫽ 3), the patient was underneath
Body Part Injured
The lower extremity (43.8%) was the most com-mon body region injured on minitrampolines, fol-lowed by the head (24.8%), upper extremity (18.2%), trunk (10.2%), and neck (2.9%). The lower extremity (42.0%) was also the most common body region in-jured on full-sized trampolines, followed by the up-per extremity (25.2%), head (14.0%), trunk (10.5%), and neck (8.4%).
There was no significant difference between chil-dren and adults with respect to body part injured on full-sized trampolines. On minitrampolines, children (younger than 18 years) were more likely to sustain a head injury (OR: 9.39; 95% CI: 1.40 – 402.47;P⫽.01), whereas adults (18 years and older) were more likely to sustain a lower extremity injury (OR: 3.11; 95% CI: 1.14 –9.14;P⫽.02; Fig 2).
There was no significant difference in body part injured on full-sized trampolines between children who were younger than 6 years and those who were 6 to 17 years of age. However, on minitrampolines, children who were younger than 6 years were more likely to sustain a head injury (OR: 7.82; 95% CI: 2.94 –22.58;P⬍.01), whereas children who were 6 to 17 years of age were more likely to sustain a lower extremity injury (OR: 3.95; 95% CI: 1.57–10.82; P ⬍
.01; Fig 2). Important results are summarized in Tables 2 and 3.
Type of Injury
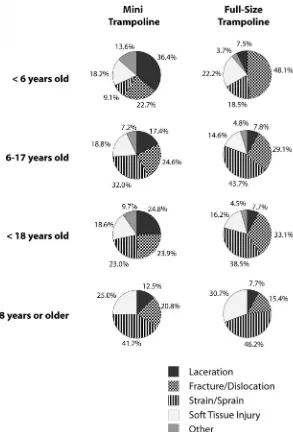
There was a significant difference between type of injury sustained on minitrampolines compared with full-sized trampolines (P ⬍ .01). While performing analyses separately for each type of trampoline, there was no significant difference between children and adults with respect to type of injury (Fig 3); however, children who were younger than 6 years were more likely to sustain a laceration on a minitrampoline when compared with 6- to 17-year-olds (OR: 2.69; 95% CI: 1.04 –7.18;P⫽.04). Children who were 6 to 17 years of age were more likely to sustain a strain or sprain on both minitrampolines (OR: 4.62; 95% CI: 1.40 –20.00;P⬍ .01) and full-sized trampolines (OR: 3.38; 95% CI: 1.13–12.34;P⫽.02) than children who were younger than 6 years (Fig 3). Important results are summarized in Tables 2 and 3.
Most Common Injuries (Body Part and Injury Type Combined)
The most common types of injuries sustained on minitrampolines for children (younger than 18 years) were head lacerations (20.3%) and for adults (18 years and older) were lower extremity strains or sprains (33.3%). Children who were younger than 6 years were most at risk for sustaining a head lacer-ation (OR: 4.98; 95% CI: 1.71–16.03; P ⬍ .01), while children who were 6 to 17 years of age were most at risk for sustaining a lower extremity strain or sprain (OR: 6.26; 95% CI: 1.35–59.14;P⫽ .01).
On full-sized trampolines, lower extremity strains or sprains were most common for both children (23.8%) and adults (15.4%). Furthermore, children who were younger than 6 years more frequently sustained lower extremity fractures or dislocations, whereas children who were 6 to 17 years of age were more at risk for lower extremity strains or sprains (OR: 4.85; 95% CI: 1.09 – 44.93; P ⫽ .03). Important results are summarized in Tables 2 and 3.
Mechanism of Injury
From the comments in the narrative portion of the NEISS database, we determined that the patient was more likely to be actively using the trampoline at the time of injury when a full-sized trampoline was in-volved (99.3% [142 of 143]) than when a minitram-poline was involved (87.6% [120 of 137]; OR: 19.97; 95% CI: 3.04 – 846.49;P⬍ .01). Only 1 (0.7%) patient was not actively using the full-sized trampoline at the time of injury, compared with 17 (12.4%) patients for the minitrampoline.
The majority of injuries were caused by a fall onto or off of the trampoline (48.8% [64 of 131] mini, 48.9% [65 of 133] full-sized). Patients who were using a minitrampoline were more likely to be injured by running into or falling/tripping over the trampoline (17.6% [23 of 131]) than those who were using a full-sized trampoline (3.0% [4 of 133]; OR: 6.82; 95% CI: 2.24 –27.98;P⬍ .01). Some of these injuries may have occurred while mounting or dismounting the minitrampoline. Patients who were using a full-sized trampoline were more likely to be injured while jumping on the trampoline or performing a stunt (35.3% [47 of 133]) than those who were using a TABLE 1. Comparison of Minitrampoline and Full-Sized Trampoline Study Populations
With Respect to Age, Gender, Location of Injury Event, and Hospital Admission
Characteristics Type of Trampoline
Mini Full-Sized
No. of cases 137 143
Mean age, y (SD) 13.9 (17.7) 11.0 (8.0)
Age range, y 1–80 2–52
No.⬍18 y (%) 113 (82.5) 130 (90.9)
No.⬍6 y (%) 44 (32.0) 27 (18.9)†
No. female (%) 86 (62.8) 73 (51.0)
No. injured at home (%)* 80 (87.0) 82 (89.1)
No. admitted to hospital (%) 0 (0.0) 7 (5.0)
* Location of injury event was not documented for 45 minitrampoline and 51 full-sized trampoline cases.
minitrampoline (20.6% [27 of 131]; OR: 2.10; 95% CI: 1.17–3.82; P ⫽ .01). Other mechanisms of injury in-cluded colliding with another person on the trampo-line and twisting an extremity on the trampotrampo-line.
Hospital Admissions
All patients who were injured on a minitrampoline were treated and released from the ED. Seven (5%) of the patients who were injured on a full-sized tram-Fig 2. Percentage of children (younger than 18
years) and adults (18 years and older) with poline-related injuries according to type of tram-poline and body part injured.
TABLE 2. Comparison of Child and Adult Trampoline-Related Injuries According to Type of Trampoline and Person’s Age and According to Body Part Injured, Type of Injury, and Most Common Injuries
Minitrampoline Full-Sized Trampoline
Age Group, y P* OR 95% CI Age Group, y P*
⬍18,n(%) ⱖ18,n(%) ⬍18,n(%) ⱖ18,n(%) Body part injured
Head 33 (29.2) 1 (4.2) .01 9.39 1.40–402.47 20 (15.4) 0 (0.0) NA
Lower extremity 44 (38.9) 16 (66.7) .02 3.11 1.14–9.14 55 (42.3) 5 (38.5) NS Type of injury
Laceration 28 (24.8) 3 (12.5) NS 10 (7.7) 1 (7.7) NS
Strain/sprain 26 (23.0) 10 (41.7) NS 50 (38.5) 6 (46.2) NS
Most common injuries
Head laceration 23 (20.3) 1 (4.2) NS 9 (6.9) 0 (0.0) NA
Lower extremity strain/sprain 18 (15.9) 8 (33.3) NS 31 (23.8) 2 (15.4) NS
Lower extremity fracture/dislocation 9 (8.0) 2 (8.3) NS 17 (13.1) 0 (0.0) NA
NS indicates not significant; NA, not available.
poline were admitted to the hospital. Six of the 7 had fractures; 5 of the 6 fractures were to the upper extremity, and the other was a fracture of the cervical spine. The seventh patient had a concussion. Six of
the admitted patients ranged in age from 3 to 13 years, and the seventh was 34 years of age. The 34-year-old sustained the cervical spine fracture. Four of the patients were female, and 3 were male. TABLE 3. Comparison of Trampoline-Related Injuries to Children According to Type of Trampoline and Children’s Age and According to Body Part Injured, Type of Injury, and Most Common Injuries
Minitrampoline Full-Sized Trampoline
Age Group, y P* OR 95% CI Age Group, y P* OR 95% CI
⬍6,
n(%)
6–17,
n(%) ⬍
6,
n(%)
6–17,
n(%)
Body part injured
Head 24 (54.5) 9 (13.0) ⬍.01 7.82 2.94–22.58 4 (14.8) 16 (15.5) NS Lower extremity 9 (20.4) 35 (50.7) ⬍.01 3.95 1.57–10.82 11 (40.7) 44 (42.7) NS Type of injury
Laceration 16 (36.4) 12 (17.4) .04 2.69 1.04–7.18 2 (7.4) 8 (7.8) NS
Strain/sprain 4 (9.1) 22 (31.9) ⬍.01 4.62 1.40–20.00 5 (18.5) 45 (43.7) .02 3.38 1.13–12.34 Most common injuries
Head laceration 16 (36.4) 7 (10.1) ⬍.01 4.98 1.71–16.03 2 (7.4) 7 (6.8) NS
Lower extremity strain/sprain 2 (4.5) 16 (23.2) .01 6.26 1.35–59.14 2 (7.4) 29 (28.2) .03 4.85 1.09–44.93 Lower extremity fracture/dislocation 3 (6.8) 6 (8.7) NS 7 (25.9) 10 (9.7) NS
NS indicates not significant.
* The2test with Yates correction was used for all statistical analyses.
DISCUSSION
Minitrampoline-related injuries more commonly resulted in head lacerations among children who were younger than 6 years. Smith13 also found that younger children are more likely to sustain head, neck, and facial injuries, with head lacerations being more common among children who are younger than 6 years. The higher center of gravity of young children may make them more prone to fall head-first, and the immature strength and coordination of their arms leave them less able to protect themselves in a fall, thus resulting in an increased rate of head injury for these children.
Previous studies have demonstrated that most full-sized trampoline–related injuries to children oc-cur on the body of the trampoline, including falls onto the mat, collisions with other trampolinists, and flips or complex maneuvers on the mat.2,10,19In our study, patients who were using a minitrampoline were significantly more likely to be injured by run-ning into or falling/tripping over the trampoline, whereas patients who were using a full-sized tram-poline were significantly more likely to be injured while jumping on the trampoline or performing a stunt. For both types of trampoline, approximately half (49%) of injuries were caused by a fall onto or off of the trampoline.
Use of a trampoline by multiple people simulta-neously occurred in 77% of the cases reported by Woodward et al14and 83% of the cases reported in the CPSC trampoline fact sheet.11 Such group use would be expected to be more common for full-sized trampolines than for minitrampolines, because the larger mat size of a full-sized trampoline allows more room for use by multiple individuals. However, we were unable to compare group use between full-sized and minitrampolines in our study because of incomplete documentation of group use in the free-text comments reported in the NEISS database. Black and Amadeo19found no correlation between the se-verity of the injury and the number of jumpers on the trampoline. Injuries associated with group use in-volved the youngest person of the group in 50% of cases with ages known for all trampolinists.14 In addition to being bumped or bounced off the tram-poline by others, a smaller child may be injured by the elastic recoil of the mat generated by a larger person or group of people.14 The force of this recoil can result in fractures of the lower extremity,16 as well as other types of injury.
Extremity injuries, both lower and upper, have been identified as the most common trampoline-re-lated injury in recent years.10,12,13,19,20,31Other inves-tigators have identified a decrease in the occurrence of fractures and dislocations with increasing age and an increase in soft tissue injuries and lower extremity strains or sprains with increasing age of the trampo-linist.13,32Likewise, in this study, the lower extremity was the most common body region injured for both types of trampoline. Lower extremity strains or sprains were more common for children who were 6 to 17 years of age and for adults. In addition, chil-dren who were younger than 6 years more
fre-quently sustained lower extremity fractures or dislo-cations on full-sized trampolines than older children. Esposito33noted a rapid increase in the use of the trampoline as a backyard recreational activity during the past 10 years. Consistent with this observation, most mini- and full-sized trampoline–related injuries occurred at home in our study population. Others have reported similar findings,10–13,20,31and a change from what was previously an indoor, school-related, athletic endeavor, to a warm-weather, after school, leisure activity involving younger children at home is apparent.14
Attempts at somersaulting, both backward and forward, are the most dangerous maneuvers on the trampoline3and have resulted in the largest number of serious injuries,7,9 especially acute injury to the cervical spinal cord.3–6The majority of known cases of quadriplegia associated with both mini- and full-sized trampolines resulted from improper execution of a somersault.8,34 One cervical spine fracture oc-curred in our study, but data were unavailable re-garding this patient’s functional outcome.
Hospital admission rates for trampoline-related in-juries reported by other investigators ranged from 1.9% to 23%.10,13,14,20,31,32In comparison, 5% of full-sized trampoline–related injuries and none of the minitrampoline-related injuries in our study re-quired admission to the hospital. The lack of admis-sions for minitrampoline-related injuries may be partly attributable to a higher proportion of injury mechanisms with lower kinetic energy involved, such as running into or falling/tripping over the trampoline.
Problems associated with recreational use of tram-polines, especially at home and in backyards, are a lack of professional instruction, trained spotters, and supervision; potential degradation of the trampoline from being outdoors and unprotected from the weather; and not properly positioning the trampo-line away from other objects, such as trees and fences. In addition, trampoline owners usually do not lock away the trampoline when it is not in use and do not secure minitrampolines to the floor or other stationary structure, as is recommended.9
Smith and Shields20 reported that knowledge of injury risks associated with trampolines was not an effective deterrent to trampoline use; neither could adult supervision be relied on to decrease trampo-line-related injuries. They found that 73% of parents indicated that they had been aware of the potential dangers of trampolines before their child was in-jured, 10% reported that their child had been injured previously on a trampoline, 54.8% of children con-tinued to use a trampoline after the injury event, and adult supervision was present at the time of injury in 56% of cases.
inadequate to prevent trampoline-related injuries. They recommended that children not use backyard trampolines, and the sale of trampolines for private recreational use should be halted. This is in agree-ment with the policy position of the AAP. However, these recommendations are based on data regarding injuries that are almost entirely associated with the use of full-sized trampolines in residential back-yards. Is the risk for injury similar for minitrampo-lines, and should these same recommendations be applied to minitrampolines? The findings of our study provide a response to these questions. Injury patterns were similar for mini- and full-sized tram-polines, although minitrampoline-related injuries were less likely to require admission to the hospital and more commonly resulted in head lacerations among children who were younger than 6 years. Risk for injury could not be determined because of the lack of data regarding duration of exposure to risk. We therefore conclude that the use of full-sized tram-polines by children should follow the policy recom-mendations of the AAP. Trampolines, including minitrampolines, should be regarded as training de-vices and not as toys. Until more data are available regarding exposure to risk, we recommend against the use of the minitrampoline as a play device by children in the home, which is where most minitram-poline-related injuries occur.
This study has several limitations. NEISS data may not be representative of trampoline-related injuries that are treated in settings outside of EDs or injuries that do not receive medical attention. The incidence of trampoline-related injuries per hour of exposure cannot be determined from our data. Therefore, the risk for injury on minitrampolines versus full-sized trampolines cannot be determined. Although inci-dence rates are important in clarifying the influence of risk factors and calculating relative risks and ORs, the frequency and the relative proportion of cases provide useful measures for a comparative under-standing of these sources of injury. Another limita-tion of this study was lack of documentalimita-tion of the circumstances of injury in many cases. The small number of adults in our study precluded statistical analyses for some comparisons. Furthermore, small sample size resulted in a wide 95% CI for some ORs, when comparisons were made between children and adults. Large variability in the data may also have contributed to wide CIs.
REFERENCES
1. Wulffson DL. Trampoline. In:The Kid Who Invented the Trampoline. New York, NY: Dutton Children’s Books; 2001:99 –101
2. Zimmerman HM. Accident experience with trampolines.Res Q.1956; 27:452– 455
3. Ellis WG, Green D, Holzaepfel NR, Sahs AL. The trampoline and serious neurological injuries. A report of five cases.JAMA.1960;174: 1673–1676
4. Kravitz H. Problems with the trampoline: I. Too many cases of perma-nent paralysis.Pediatr Ann.1978;7:728 –729
5. Torg JS. Trampoline-induced quadriplegia. Clin Sports Med. 1987;6: 73– 85
6. Rapp GF, Nicely PG. Trampoline injuries.Am J Sports Med. 1978;6: 269 –271
7. Meredith MM. Don’t sell your trampoline. J Phys Educ Rec Dance.
1981;52:82– 83
8. American Alliance for Health, Physical Education, and Recreation. The use of trampolines and minitramps in physical education.J Phys Educ Rec Dance.1978;49:14
9. National Association for Sport and Physical Education. The Use of Trampolines and Mini Tramps in Physical Education. A Position Paper of the Middle and Secondary School Physical Education Council and The National Association for Sport and Physical Education. Reston, VA: National Asso-ciation for Sport and Physical Education; 2002
10. Furnival RA, Street KA, Schunk JE. Too many pediatric trampoline injuries.Pediatrics.1999;103(5). Available at: www.pediatrics.org/cgi/ content/full/103/5/e57
11. US Consumer Product Safety Commission.Fact Sheet 85: Trampolines. Washington, DC: US Consumer Product Safety Commission; 1976 12. Chalmers DJ, Hume PA, Wilson BD. Trampolines in New Zealand: a
decade of injuries.Br J Sports Med.1994;28:234 –238
13. Smith GA. Injuries to children in the United States related to trampo-lines, 1990 –1995: a national epidemic.Pediatrics.1998;101:406 – 412 14. Woodward GA, Furnival R, Schunk JE. Trampolines revisited: a review
of 114 pediatric recreational trampoline injuries. Pediatrics. 1992;89: 849 – 854
15. Hammer A, Schwartzbach AL, Paulev PE. Some risk factors in trampo-lining illustrated by six serious injuries.Br J Sports Med.1982;16:27–32 16. Boyer RS, Jaffe RB, Nixon GW, Condon VR. Trampoline fracture of the
proximal tibia in children.AJR Am J Roentgenol.1986;146:83– 85 17. Olsen PA. Injuries in children associated with trampoline-like air
cush-ions.J Pediatr Orthop.1988;8:458 – 460
18. Clare PE. Trampoline injuries to the lower extremity. Two case reports.
Am J Sports Med.1978;6:141–142
19. Black GB, Amadeo R. Orthopedic injuries associated with backyard trampoline use in children.Can J Surg.2003;46:199 –201
20. Smith GA, Shields BJ. Trampoline-related injuries to children. Arch Pediatr Adolesc Med.1998;152:694 – 699
21. Torg JS, Das M. Trampoline-related quadriplegia: review of the litera-ture and reflections on the American Academy of Pediatrics’ position statement.Pediatrics.1984;74:804 – 812
22. Torg JS, Das M. Trampoline and minitrampoline injuries to the cervical spine.Clin Sports Med.1985;4:45– 60
23. Kessler E, Schroeder T.The NEISS Sample (Design and Implementation). Washington, DC: US Consumer Product Safety Commission; 1999 24. Hopkins RS. Consumer product-related injuries in Athens, Ohio,
1980 –1985: assessment of emergency room-based surveillance.Am J Prev Med.1989;5:104 –112
25. Annest JL, Mercy JA, Gibson DR, Ryan GW. National estimates of nonfatal firearm-related injuries: beyond the tip of the iceberg.JAMA.
1995;273:1749 –1754
26. Davis Y, Annest JL, Powell KE, Mercy JA. An evaluation of the National Electronic Injury Surveillance System for use in monitoring nonfatal firearm injuries and obtaining national estimates.J Saf Res.1996;27: 83–91
27. McNeill AM, Annest JL. The ongoing hazard of BB and pellet gun-related injuries in the United States.Ann Emerg Med.1995;26:187–194 28. GraphPad Software Inc. GraphPad Quickcalcs. Random numbers.
GraphPad Software Inc; 2002. Available at: www.graphpad.com/ quickcalcs/randomn2.cfm. Accessed May 12, 2005
29. Dean AG, Dean JA, Burton AH, Dicker RC. Epi Info, Version 5.01b: A Word Processing, Database, and Statistics Program for Epidemiology on Microcomputers. Stone Mountain, GA: USD, Inc; 1990
30. LogXact [computer software]. Version 4.0. Cambridge, MA: Cytel Soft-ware Corporation; 1999
31. Canadian Hospitals Injury Reporting and Prevention Program (CHIRPP). Injuries associated with trampolines. CHIRPP database, summary data for 1998, all ages. Health Canada; 2000. Available at: www.hc-sc.gc.ca/pphb-dgspsp/injury-bles/chirpp/injrep-rapbles/ trmpln㛭e.html. Accessed May 12, 2005
32. Larson BJ, Davis JW. Trampoline-related injuries.J Bone Joint Surg Am.
1995;77:1174 –1178
33. Esposito PW. Trampoline injuries.Clin Orthop.2003;409:43–52 34. Rapp GF II. Safety suggestions for trampoline use.Pediatr Ann.1978;7:
730 –731
35. Silver JR, Silver DD, Godfrey JJ. Trampolining injuries of the spine.
Injury.1986;17:117–124
DOI: 10.1542/peds.2004-1326
2005;116;96
Pediatrics
Brenda J. Shields, Soledad A. Fernandez and Gary A. Smith
2002
−
the United States, 1990
Comparison of Minitrampoline- and Full-Sized Trampoline-Related Injuries in
Services
Updated Information &
http://pediatrics.aappublications.org/content/116/1/96
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/116/1/96#BIBL
This article cites 26 articles, 5 of which you can access for free at:
Subspecialty Collections
chnology_sub
http://www.aappublications.org/cgi/collection/health_information_te Health Information Technology
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2004-1326
2005;116;96
Pediatrics
Brenda J. Shields, Soledad A. Fernandez and Gary A. Smith
2002
−
the United States, 1990
Comparison of Minitrampoline- and Full-Sized Trampoline-Related Injuries in
http://pediatrics.aappublications.org/content/116/1/96
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.