on
Making
a Difference
Morris Green, MD
From the Department of Pediatrics, the Indiana University School of Medicine and the James Whitcomb Riley Hospital for Children, Indianapolis, Indiana
A question being much discussed today, here and
elsewhere, is how to be helpful to all children and their families, especially those who are highly vu!-nerable and at special risk. It is a question that also intrigued Abraham Jacobi, a vigorous advocate for
children and a vocal opponent of practices and
conditions he viewed as inimical to their best inter-ests.
Now, as in Jacobi’s day, the privileged status that
society confers on the professions carries implicitly, and increasingly explicitly, the charge that they remain responsive to the needs of the times. In the
case of pediatricians, there is the expectation that
we will do whatever is in our individual or collective power to help children and their families master
the rapid changes and risks that confront them
today. Pediatricians are being challenged increas-ingly to become involved in social as well as biomed-ical issues and to promote healthy adaptation as well as growth and development.
PEDIATRICS AND ADAPTATION
These remarks on the potential role of pediatri-cians in promoting adaptation to developmental,
social, educational, and psychosocial issues call for
an extension of their traditional role in helping
children and parents cope with biomedical
prob-lems.”2 As exemplified in Table 1, such adaptation
may be biomedical or psychosocial and prospective, concurrent, or rehabilitative. For successful
adap-tation to occur, the child or adolescent must
ad-vance from the “Risk” box in Figure 1 to the one
Received for publication Jun 13, 1990; accepted Oct 3, 1990
Presented, in part, on the occasion of the Abraham Jacobi Award, American Academy of Pediatrics Spring session, Seattle,
Washington, May 1, 1990.
Reprint requests to (M. G.) 702 Barnhill Drive, Indianapolis, Indiana 46202-5225.
PEDIATRICS (ISSN 0031 4005). Copyright © 1991 by the American Academy of Pediatrics.
labeled “Mastery.” Those who end in the box
la-beled “Maladaptation” are life’s losers, penalized
by symptoms, poor functioning, and unhappy
fam-ilies.
Table 2 is a list of groups of children, adolescents, and families currently at risk in our society.3’4 Those who confront a cluster of risks are in double,
triple, or even quadruple jeopardy.5 For example, a
child with a learning disorder may be poor, have epilepsy, live with a depressed mother in a single-parent household, and receive inadequate remedial education.
The outcome of the process of adaptation is vec-tored by the quantity and quality of protective and mediating factors available to contain an
individ-ual’s vulnerabilities.6’7 Table 3 is a list of some of
the protective factors which contribute to resiliency or “invulnerability.” One may predict confidently that a child or adolescent blessed with most of these
traits will do very well indeed; those who have few
such traits in the face of multiple vulnerabilities are destined by and large to have suboptimal or even tragic outcomes.
I have begun to develop an office screening
in-strument to identify such protective factors or
strengths as well as vulnerabilities as part of the
assessment of a child or adolescent when seen for health supervision or for a psychosocial, educa-tional, developmental, or biomedical disorder. The presently available behavioral screening checklists, which focus predominantly on problems and
symp-toms, are not very useful in transforming early
intervention approaches from deficit-based models
to those that also build on present or potential
strengths. Sharing with parents and children an
accounting of their strengths as determined by such a screening assessment will help to validate their
sense of efficacy and to promote the
physician-patient alliance. Parents are more likely to listen
Fig 1. Flowsheet for adaptation.
TABLE 1. Adaptation of Children and Parents
I. To biologic stressors A. Prospective
Immunization
Exercise-induced bronchospasm B. Concurrent
Antibiotics for meningitis
Insulin, fluids, and electrolytes for diabetes
C. Rehabilitative Birth defects Head injury
II. To psychosocial stressors
A. Prospective
Adoption
Hospitalization/surgery
B. Concurrent
Birth of an infant with a handicap
Death Divorce
C. Rehabilitative School avoidance Conversion disorder
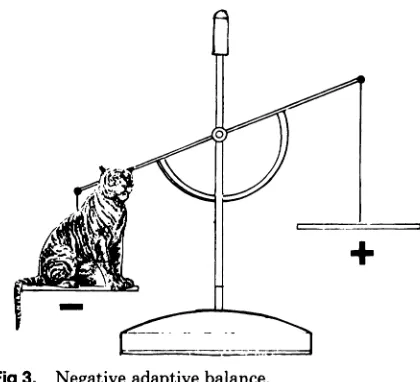
The pediatrician’s role in promoting adaptation
includes, first, assessing the balance between the
patient’s protective factors and vulnerabilities and,
second, helping him or her develop additional
strengths. This is shown diagrammatically in
Fig-ure 2 as a balance with the patient’s protective factors or strengths loading the scale pan on the
right and their vulnerabilities loading the one on
the left. When this adaptive balance is in
equilib-nium or tilted to the right, the physician’s interven-tions need to be only minimal, eg, anticipatory guidance or suggestions for concurrent adaptation to relatively minor problems.
When, however, the balance is weighted toward
the left, the pediatrician can explore with the
fam-ily, child, or adolescent how they might develop additional strengths, ie, build up weights on the
right. This alternative kind of psychosocial, devel-opmental, and educational “weight” training may include, for example, developing social skills in a 10-year-old girl who is shy, encouraging a father to
spend more time with his underachieving son, tu-toning for a child having trouble with mathematics,
or referring a depressed mother for psychiatric help.
Gradually shifting the balance to the right in this
fashion may be a powerful intervention. Only a few
“grams” may be added to the scale pan as a result
of a visit, but just the right word at the right time
from a trusted pediatrician, the reinforcement that comes with a physician’s transmitted confidence
that the patient can do it, thoughtful suggestions
that might be tried, and access to other appropriate
professionals may make a large difference even
when the problems manifested by the patient
mi-tially seem overwhelming and intractable. In this
fashion, on occasion and seemingly magically, one
may transform a tiger of a problem (Fig 3) to a
pussy cat (Fig 4)! This is a highly gratifying
expe-rience for a clinician and a life boost for the child. In the hands of a skilled and thoughtful
pediatri-cian and with adequate community resources, this
recombinant process of splicing new adaptational and coping skills into a patient’s or family’s reper-toire is highly effective. It represents, in its own
way, a kind of recombinant biology that can be
applied practically by the practitioner in everyday practice. In addition to the help provided by the individual pediatrician, high-risk groups weighted
with multiple vulnerabilities need medical care that
is linked to organized and responsive nursing, social
work, and home visiting services.
TABLE 2. Children and Adolescents Potentially at
Risk
. Children living in poverty (20%)
. Single parent families (22%)
. Children with chronic illness or handicap
. Pregnant adolescents
. Abused and neglected children
. Children of divorce (1 million/y)
. Children in foster care (250 000)
. Adolescents in detention (>250 000)
. Children of alcoholic, emotionally ill, or otherwise
dys-functional parents . Risk-taking adolescents
. Adolescents who abuse alcohol and drugs
. Drug-exposed infants (375 000/y)
. Children exposed to environmental hazards . Absence of prenatal care (1 of 4 pregnant women) . Low birth weight infants
. Infants and children with acquired immunodeficiency
syndrome
I Emotionally ill children and youth (estimated to range from 11% to 19%)
. School drop-outs; illiterate children
. Children who have unemployable parents;
unemploya-ble adolescents
. Those with no health insurance coverage (up to 12 million children and adolescents)
+
TABLE 3. Selected Protective Factors Which Contribute to Resiliency. Temperament or disposition characterized by a positive mood and flexibility
. A supportive social network and positive role models: parents, relatives, teachers, and other significant adults and peers
. The feeling that one is loved and valued by parents and other significant persons
. Social skills; one or more close friends; ability to mobilize social supports; ability to ask for help with comfort
. Parents who allow age-appropriate autonomy
. Availability of parents at times of failure; to buffer and protect the child against excessive stress
. Ability to define and persist in achieving goals
S Sense of belonging to and active participation in a valued group S Physical fitness, endurance, and vigor
. Normal intelligence and good health
. Strong personal sense of competence based on achievements, successes, special interests, or talents
. A view of the world as coherent and controllable . Opportunities for mastery of new challenges
. Expectation of personal success . Positive perception of events
. Belief in ability to modify one’s behavior constructively
. Recognition of one’s effort and achievement by parents and others
. Ability to form trusting relationships
S A sense of responsibility for one’s own health
. Ability to enjoy life and to have had some joyful experiences
. Family warmth, cohesion, support, communication, and mutuality
. Ability to express feelings
. High self-esteem and constructive assessment of personal capacities
. A sense of efficacy; the belief that one knows what to do and can do it
. Access to educational, vocational, and social opportunities
. Presence of a positive value system
Fig 2. Adaptive balance.
j
Fig 3. Negative adaptive balance.
PEDIATRIC COMORBIDITY AND SHARED
ETIOLOGY
Comorbidity, a term more traditionally
consid-ered in relation to the multiple disorders of the elderly or to psychiatry, is equally applicable to pediatric patients, especially when psychosocial,
family, and community morbidity is included. The
high prevalence of comorbidity in those who live in poverty, for example, needs to be reflected in their diagnostic assessments. That they are not included
customarily is attributable to lack of an adequate
pediatric nosology for family, community, and
so-cia! disease and to the absence of a tradition of
complementing the internal with the external
as-pects of medicine.
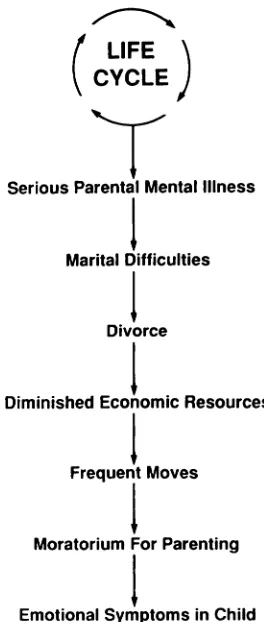
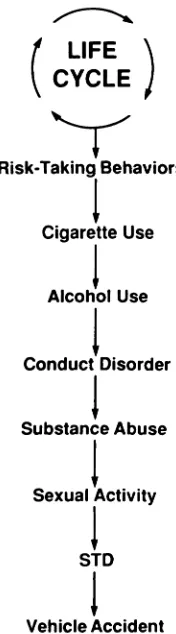
There is also increased recognition that many maladaptive symptoms and disorders emerge from common root causes. Such intertwined etiologies are at least additive but more often multiplicative.
These interrelationships may be shown graphically
in the form of a “life cycle” as shown in Figure 5
and with side chains as shown in Figures 6, 7, and
8.
0
- _
Fig 4. Positive adaptive balance.
Marital Difficulties
Family Stressors
Lack of Values
‘I Lack Social Supports
Negative Peer Influences
Poverty Dysfunctional
, Family
Family
Violence/Abuse Poor Schools
t
Fig 5. Life cycle.
Poor
Parent-child Relationship
simplified fashion, in vivo, they would look more like the spider web shown in Figure 9. Enmeshed, suspended in time and space, feeling helpless and hopeless, such patients and families are unable to
extricate themselves without intensive
interven-tion. Interrupting these dysfunctional and devel-opmentally regressive life cycles is a daunting task.
It is difficult to change familiar life patterns; new
support networks may not be adopted quickly; and
social transplants simply may not take.
THE
ADAPTATION
OF THE
COMMUNITY
PRACTITIONER
Adaptation at the community pediatric practice
level is an emerging frontier in pediatric education,
care, and research. What can pediatricians do to
make a difference at this relatively new cutting
edge? How can the pediatric office serve more ef-fectively as a community-based parent and child
resource center? How can we help break the
dys-functional chain reactions that threaten the future of many of the nation’s children?
Responses to these questions include the
follow-ing:
I
LIFEt
CYCLESerious Parental Mental Illness
Divorce
Diminished Economic Resources
Frequent Moves
1
Moratorium For ParentingI
Emotional Symptoms in Child
Fig 6. Life cycle: side chain associated with parental mental illness.
S The staging of primary ambulatory care into
three levels of service rather than only the one
implied by the term “primary care” is a concept
whose time has come.8 To convey its complexity adequately, general pediatric care should be staged into Levels I, II, and III. In addition, these stages should be reflected in levels of
reimburse-ment.
Analogous to the traditional division of
hospi-tal-based practice into primary, secondary, and
tertiary care, the three hierarchal levels of
am-bulatory care shown in Figure 10 are defined by
the time required for a specific service; the train-ing, experience, and competence needed to
pro-vide the care; the complexity of the problem; and whether the pediatrician works alone or as a
member of a team. The time allotted by
practi-tioners to these three levels of care will depend on their special competencies, the needs of the
population they serve, and organization of their practice.
These levels apply to health supervision
serv-ices as well as to the diagnosis and management
of problems. Whereas a well-organized, low-risk
family may need only Level I health supervision,
I
LIFE ‘CYCLE
Fig 9. Spider web.
The Hospital The Community
Fig 10. Staging of pediatric health care.
STD
Vehicle Accident
Fig 7. Life cycle: side chain associated with risk-taking behaviors.
p
LIFE‘ CYCLE
ADD/Hyperactivity
Learning Disability
I
Poor Peer RelationshipDepression
I
Conduct Disorder
I
School Drop-out
I
Ethnic Prejudice
I
Unemployment
Fig 8. Life cycle: side chain associated with ADD (at-tention deficit disorder).
Risk-Taking Behaviors
1
Cigarette Use
Alcohol Use
I
Conduct DisorderSubstance Abuse
1
Sexual ActivityLevel II or III services.9 Levels I, II, and III apply to personal, one-to-one care, the predominant
daily work of the pediatrician. Community or
level “C” care, an increasingly full-time, part-time, or voluntary role of the pediatrician, is
concerned with the health of populations of
chil-dren. This includes improvement of access, the
coordination of care, and the establishment of community resources responsive to identified
needs. Just as hospital-based supporting services are essential to care for children with serious
biomedical illnesses, community-based resources
are required for the care of patients with Level II and III developmental, educational, and/or psy-chobiologic problems.
. Seeing more of these problems in their current
practices, many practitioners wish to augment their psychotherapeutic skills. A number of ex-cellent books, tapes, articles, continuing medical
education courses, and minifellowships on the
psychologic and developmental aspects of
pedi-atrics help meet this need; however, in my view,
such competencies is through continuing
partic-ipation in what I have termed Collaborative
Of-flee Rounds groups. A group that consists of seven
to eight pediatric practitioners, a pediatrician
interested in developmental psychobiology, a
child psychiatrist, and a child psychologist meet
regularly approximately every 2 weeks to discuss
the treatment of patients currently being seen in
the practice of one of the pediatricians. Several
Collaborative Office Rounds groups have been
funded recently by the Bureau of Maternal and
Child Health, and I would encourage this
ap-proach as an effective continuing pediatric
edu-cational strategy for the American Academy of
Pediatrics.
. For practitioners to provide an increased amount
of Level II and III care, reimbursement for
cog-nitive services must be available. The lack of
adequate payment is a major impediment to
in-elusion of such care. A positive change would lie
in the proposed adoption of a resource-based
relative value system for reimbursement of
med-ical care. For populations at special risk, funding
also should be provided for social work, nursing,
and home visitor services.
C The pediatric practitioner has experience with
some types of pediatric morbidity that for a
num-ben of reasons are not experienced or discussed
during residency training. In front-line settings,
the initial complaints, their duration, and patient
expectations often differ from those in teaching
hospitals with their nonrepresentative patient
populations. In addition, the practitioner gains
the long-term view of a child, family, or problem
made possible by continuity of care. Such rich
case experience and naturalistic observations
need to be added to the cumulative knowledge
base of pediatrics. Transmission of that
knowl-edge to others may be achieved either by the
individual practitioner publishing reports based
on his or her individual experiences or through
collaboration, as in the Pediatric Research in
Office Settings program of the American
Acad-emy of Pediatrics.
C In addition to one-to-one health supervision
vis-its, some practitioners schedule group sessions
for parents with children in the first 2 years of
life. There is also a growing emphasis on parent
education through newsletters, handouts,
audi-otapes, and videotapes.
. Self-administered and automated screening
as-sessments are being explored along with
corn-puter-generated reports, including focused health
education advice. Based on an individual
assess-ment of a parent on child’s questions, presenting complaints, and family protective
factors/vulner-abilities, a current and periodically revised
Per-sonal Health Plan, analogous to the Individual
Education Plan, may be computer-generated.
This process would include an individualized
printout of specific advice, anticipatory guidance,
and a listing of family strengths.’#{176} Where
mdi-cated, the printout would also highlight one or
more specific objectives to be accomplished by
the child, adolescent, or parent before the next
visit. Personal Health Plans would be especially
important for children and families with
long-term disorders. Such Personal Health Plans
would document for health services researchers
and third party payers the content of pediatric
care currently being delivered in various settings.
. Pediatric participation in planning, consultation,
or direct service in community settings such as
schools, child care centers, and public health
de-partments is an established tradition. ln the care
of individual patients many pediatricians now
work collabonatively with social workers and
psy-chologists in their offices or in other sites, but
continued effort is needed throughout the country
for the further development of community-based
diagnostic and treatment resources to
comple-ment and supplement those available to the
prac-titioner.
. Coordination of services, especially when various
elements of a Personal Health Cane package are
given in many sites by multiple professionals, is
an appropriate role for the pediatric office serving as the child’s medical home. For highly vulnerable
families and groups, the organization of care must
integrate medical with other health and human
services. Whereas some sophisticated and
resili-ent parents successfully traverse the maze of
community or regional services, those who are
less resourceful or assertive become lost or
de-Spain of the dead ends, barriers, and Service gaps
they confront. The practitioner may elect to be
the case coordinator or may delegate that role to
another person in the office or community.
. Because community ecology and resources play
such an important role in child health, it is
ap-propniate in 1990 for Departments of Pediatrics
to establish Sections of Community Pediatrics,
as some have already. Progressive departments
will, I believe, add to their residency programs
more of the content and skills needed for
pedia-tnicians to work in community as well as hospital
settings.” In those educational rotations,
pedi-atnic practitioners will be the teachers, and
pedi-atnic offices on community child health centers
will be the training venues. In the future,
accred-itation of pediatric residencies may require this
. Not all the changes in our society have been
regressive or hazardous for the development of
children. Progressive advances include Public
Law 94-142, the Education for the Handicapped
Act, and Public Law 99-457, the Amendment to
the Act for intervention programs for 0- to
3-year-olds; the concern expressed by business and
government leaders about child and adolescent
health, development, and education; the presence
of several coordinated, comprehensive
commu-nity systems for children, adolescents, and
fami-lies; the growth in home care and
community-based services for children with special needs; the American Academy of Pediatrics initiative to gain
increased access to health services through health
insurance for all children and pregnant women;
the growth of school-based health clinics; and the
improved education of pediatric residents in the
psychosocial and developmental aspects of child
health.’2”
. Continued responsiveness and renewal in pedi-atnic education and practice and in public policy for children at state and national levels would be facilitated considerably by the establishment of
one or two National Academic Centers for
Corn-munity Pediatrics. I would also hope that
Corn-munity Pediatric Interdisciplinary Program
Grants would be made available to promote a
productive collaboration between departments of
pediatrics and departments and schools of
behav-ioral and social science, nursing, education,
man-agement, public health, business, and
govern-ment.
. Finally, we must augment actively our individual
and joint community, state, and national
advo-cacy for child and adolescent health.
Eric Erickson concluded his 1973 Jefferson
Lee-tures with the valediction, “Take Care.”4 He
fur-ther expressed the hope that those two words would
“come to mean more. . . than we should be careful,
or take care of ourselves.” These remarks outline
some of our present opportunities to meet
Enick-son’s challenge. ln so doing, we can make a
sub-stantial difference in the lives of children.
REFERENCES
1. Green M. Pediatric education and the care of the person.
Pediatrics. 1986;78:431-437
2. Cohen F, Lazarus RS. Coping and adaptation in health and illness. In: Handbook of Health, Health Care, and the Health Professions. New York: The Free Press; 1983
3. Alpert JJ, Weitzman M. An overview of childhood mortality and morbidity. In: Green M, Haggerty RJ, eds. Ambulatory
Pediatrics. Philadelphia: W. B. Saunders Co; 1990:4-9
4. Starfield B, Katz H, et a!. Morbidity in childhood: a longi-tudinal view. N Engl J Med. 1984;310:824
5. Garmezy H, Rutter M. Acute reactions to stress. In: Child
Psychiatry: Modern Approaches. 2nd ed. Oxford: Blackwell
Scientific Publications; 1985
6. Dugan TF, Coles R, eds. The Child in Our Time: Studies in the Development of Resiliency. New York: Brunner/Mazel; 1989
7. Masten AS, Garmezy AS. Risk, vulnerability, and protective factors in developmental psychopathology. Adv Clin Child Psychol. 1985;8:1
8. Green M. Coming of age in general pediatrics. Pediatrics. 1983;72:275-282
9. Green M. Behavioral and developmental components of child health promotion: How can they be accomplished?
Pediatr Rev. 1986;8:133-141
10. Elias MJ. Long-term social adaptation. In: Green M, Hag-gerty RJ, eds. Ambulatory Pediatrics. Philadelphia: W. B. Saunders Co; 1990:64-68
11. Green M. Building a model in educating pediatricians to
provide access to primary care. Proceedings of a conference
on Educating Pediatricians to Provide Ascess to Primary
Care, Easton, Maryland, June 6-8, 1989. Supported by the Bureau of Maternal and Child Health, US Department of
Health and Human Services. 1989:27-32
12. The First Sixty Months and Bringing Down the Barriers.
National Governor’s Association, 444 North Capitol Street, Washington, DC 20001
13. Schorr LB. Within Our Reach: Breaking the Cycle of Disad-vantage. New York: Doubleday/Anchor Books; 1988