Page 1
Introduction
No single stakeholder can create public health interventions on a scale sufficient to combat the enormity of the HIV/AIDS crisis. Uncontrolled spread of HIV has reduced life expectancy by more than 10 years in some sub-Saharan African countries and today accounts for nearly 20% of all deaths and disability-adjusted life-years (DALYs) lost in the region.1 Thus, reliance on public-private partnerships is critical to addressing the multiple and diverse health needs of AIDS endemic countries.
In many ways, South Africa2 is the regional epicenter of the pandemic, with an adult population HIV infection rate that is second only to Botswana’s. In framing its own response to AIDS in South Africa, Pfizer3 realized it could not act without the direct sponsorship of the government. Initiating a plan to contribute to improved AIDS treatment was only the first – and arguably least important – step. Actually making it work to deliver a useful public health outcome required the active involvement not only of the government, but of health professionals, community leaders, NGOs, and the patient population as well. Pfizer’s deep community ties, based on a 50-year record as a local investor and employer, proved critical in making its outreach successful.
This brief review of the Pfizer partnership with the Ministry of Health to distribute free Diflucan® (fluconazole) demonstrates that product donations can serve as an effective response to AIDS if it is coupled with efforts to build drug distribution and professional health care capacity to treat patients. Equally important is that the Programme has forged a new set of productive working relationships between stakeholders who came to the project with different backgrounds and perspectives as well as a frankly disparate set of objectives. A “decision tree” illustrating how we built those relationships into the heart of the Programme each step of the way is provided as a guide to other companies exploring the launch of similar partnerships. These questions reach beyond Pfizer and can be used as a general guide to product donation decision making.
Our case study concludes with a few lessons learned in providing medicines not only to South Africa but also to the 10 other African countries now participating in the Diflucan Partnership Programme.4 As Pfizer continues to search for new treatments and vaccines, increasing access to existing medicines now through targeted donations – including training and infrastructure support – is the most practical way for the health community to address the problem of ill health among the poorest of the poor.
1Inter Press Service - Monday, November 30,1998. “HEALTH-SOUTH AFRICA: AIDS Threatens Human Development Gains”. "The spread of HIV and AIDS in South Africa is fuelled by the apartheid legacy of the migrant labour system, the accompanying spread of sexually transmitted diseases and the subordinate status of women," says the report sponsored by the United Nations Development Programme (UNDP) and UNAIDS.
2
South Africa is the wealthiest country in Africa, spending about $237 per capita on healthcare on a total population of 43 million. Between 1992 and 1999, however, the Rand halved in value against the US dollar. Nearly 40% of the population lives in Kwazulu-Natal and Gauteng, two districts with the highest AIDS rates (World Health Organization, World Health Report, 2002, p. 81).
3
Pfizer Inc discovers, develops, manufactures and markets leading prescription medicines for humans and animals, as well as many of the world’s best known consumer products. Pfizer is the largest research-based pharmaceutical company in the world, with sales in over 150 countries. It has a long tradition of commitment to community that dates back to the Company’s
beginnings in Brooklyn. Commitment to community remains one of Pfizer’s core values. Over the past several years, Pfizer organizations around the world have stepped up their activities in this area.
4
Page 2
Programme Specifics
Launched in December 2000, the Diflucan Partnership Programme (DPP) focuses on treating the two major opportunistic infections frequently experienced by AIDS patients while providing critical training and public health infrastructure to ensure effective levels of compliance. Initially, the agreement with the South African Ministry of Health was to assess the program in two years to determine areas for improvement. In less than two years, the Programme has reached over 90% of the targeted state hospitals in South Africa, trained more than 8000 health care providers in the treatment of opportunistic fungal infections, and dispensed more than one million tablets to AIDS patients. While a cure for AIDS is still unattainable, the partnership has already improved the quality of life for many thousands of patients. Based on the initial success in reaching patients, the South African partnership has now been expanded without dollar or time limits.
Programme Goals and Performance Metrics
In April 2001, after a year-long negotiation process, Pfizer and the South African government treated its first patient with Diflucan. The two infections treated, Cryptococcal meningitis (CM) and Oesophageal candidiasis (OC), are estimated to occur in 10-40% of patients with advanced AIDS. Treatment for these two conditions is palliative; patients who cannot swallow often deteriorate rapidly from malnutrition and those with fungal brain infections often die if not treated immediately.
Pfizer carefully considers the feasibility and impact of donation programs prior to embarking on them (See Appendix). Pfizer’s overarching goals are clear:
1. Build on established country programs with minimal interruption of existing services;
2. Underscore the long-term need for developing medically responsible treatment and prevention ;
3. Continue to improve and expand global partnerships to help fight the AIDS epidemic around the
world, consistent with Pfizer’s values.
However, Pfizer cannot and will not implement programs without partners who offer other public health and operational components. Most of the effectiveness of a public health intervention comes from collaborative efforts to build the local infrastructure and capacity so that products can make their way to those who need them. Building effective partnerships to facilitate this is hard, long-term work. Further, effective partnerships require diverse ideas, complementary resources and trust.5,6,7,8
For example,the memorandum of understanding between the Ministry of Health and Pfizer took several
months to negotiate. Each partner needed to review its expected roles and responsibilities, and develop trust in the intentions and abilities of the other. For the Ministry, this was the first time it would engage directly in a co-administered program with a private R&D-based pharmaceutical company. There was no clear precedent to be tapped in embarking on this partnership. However, the front-end investment of time
5 T.K. Das and Bing-Sheng Teng (Jan 1, 2000). A Resource-Based Theory of Strategic Alliances. From Journal of Management. Page(s): 29
6
J. Austin (2000). The Collaboration Challenge: How Nonprofits and Businesses Succeed Through Strategic Alliances. San Francisco: Jossey-Bass Publishers.
7 Public-Private Partnerships for Public Health. (2002). Editor, Michael R. Reich. Harvard University Press.
8 T.K. Das and Bing-Sheng Teng (Mar 1, 2001). Trust, Control, and Risk in Strategic Alliances: An Integrated Framework [*]. From Organization Studies. Page(s): 28
Page 3
and discussion resulted in a much stronger program than would have been the case had there been no such scrutiny.
The components of the Diflucan Partnership Programme include:
Pfizer
1 . Donate Diflucan (fluconazole) indicated for the treatment of HIV/AIDS patients with either
Cryptococcal meningitis (CM) and/or Oesophageal candidiasis (OC);
2. Register Diflucan for donation, in accordance with the country’s requirements
3. Provide patient and healthcare professional education and training materials for the proper use of Diflucan;
4. Send stock with at least 12 months of dating;
5. Pay for shipping up to the port of entry into the country.
The South African government
1. Take title to the donated Diflucan upon delivery to the country;
2. Allow the product to enter the country free of government taxes, levies or charges.
3. Assist with customs clearance and ensure that the donated product is stored, distributed, dispensed and used in accordance with approved processes, and classify the product as a controlled substance (for additional security from theft);
4. Ensure the attendance of targeted health care workers at training Programmes;
5. Ensure that the product is provided free of charge to eligible patients enrolled in the Programme; 6. Vigorously attempt to prevent, detect and prosecute diversion of donated Diflucan, and report on
product diversion in accordance with the procedures established;
7. Establish a Ministerial Working Group to oversee the operation and scale-up of the Programme.
The Need for Infrastructure
In a recent article in the New York Times, President Bill Clinton points out the dilemma of supplying complex medicines to health care systems that are ill-prepared to use them effectively:
“too many countries are still in denial about the scope of the problem and what has to be done about it; many countries lack the nationwide health infrastructure to treat such a disease; most countries don’t have enough health-care personnel to run a complicated treatment program..” 9
Building capacity and infrastructure are long-term prospects. Yet multiple sectors of society can take critical steps now to move gradually toward better health care systems. For example, Pfizer has provided a grant to the International Association of Physicians for AIDS Care (IAPAC) to conduct training sessions in every country where the DPP is operating. The training includes physicians, nurses, pharmacists and other allied health professionals and specifically addresses each component of care: clinical diagnosis and treatment, inventory control and reporting.
9
Page 4
Another part of the solution lies in donating medicines targeted to reach those patients who cannot afford medicines at any price. Sadly, this is a large portion of the developing world.10 Often, critical segments of the supply chain for drugs do not function. Many dysfunctions are often manageable, however, sidestepping them over the long-term is often more costly than addressing and fixing what is broken. In South Africa for instance, Pfizer continues to work directly with the Ministerial Working Group to audit the system and share the reports.
Often, a regional approach can strengthen capacity across several countries at once. For example, Pfizer has provided funding and donated its engineers to build a regional Infectious Disease Institute to be located in Kampala, Uganda. This new facility will train up to 80 physicians from the region each year in HIV/AIDS care and treat about 50,000 patients per year. The center came about through Pfizer’s relationships with the Academic Alliance for AIDS Care and Prevention, the San Francisco AIDS Foundation, Pangaea Global, Makerere University, The AIDS Support Organization (TASO), the Infectious Diseases Society of America, among others. Thus, while public-private partnerships often involve primary parties at the country level, global initiatives typically require multiple resources, creating some overlap.
Outcomes
Pfizer’s donation of Diflucan is offered without dollar or time limits.11 Initially in 2001, distribution reached approximately 80 of the targeted facilities. One year later, through joint efforts within the Ministry of Health and from Pfizer, they show the following results:
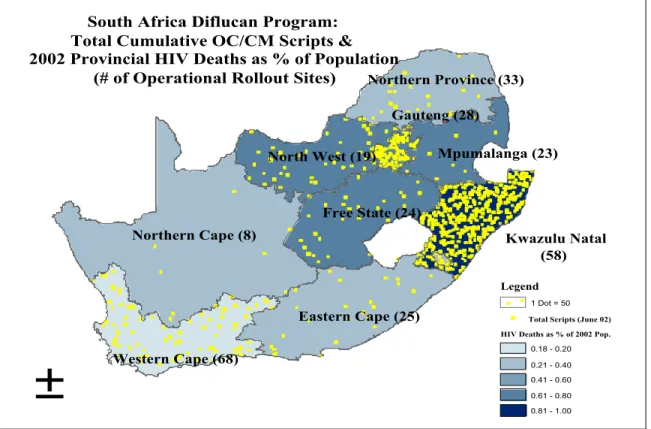
• Nearly 300 facilities are participating in all 9 provinces with emphasis on Kwazulu-Natal, where the HIV deaths as a percentage of the 2002 population is highest (Figure 1).
• Through IAPAC, over 8,000 health care professionals have been trained in South Africa who are
now refreshed on how to diagnose and treat opportunistic fungal infections. Provider morale has improved now that they can actually treat their patients for fungal infections.
• Providers have dispensed over one million tablets to patients who are not able to afford the
purchase of medicines, and those patients will have this drug supply available as long as they need it.
• The Ministry of Health created a Ministerial Working Group that meets periodically to discuss
program challenges. Pfizer is part of that group. The caution initially exhibited by these strategic partners has grown into coordinated and communicative action.
• Pfizer has broadened their HIV/AIDS partnerships globally to include international institutions such as the Center for Disease Control, charitable partners such as Interchurch Medical Assistance, other faith-based organizations, training professionals and logistics consultants, to name a few.
10 United Nations. http://unstats.un.org/unsd/mi/mi_results.asp?row_id=580, accessed 12/04/2002.
11 Although the partnership does not have dollar or time estimates, Pfizer has estimated the total cost of its current partnership commitments to be US$ 103 million. (1) Pfizer donated or pledged to donate product valued at approximately US$ 100 million (wholesale price) to provide over 2 million treatments to HIV/AIDS patients for either cryptococcal meningitis or oesophageal candidiasis. (2) Pfizer trained 9,000+ health care professionals in the treatment of opportunistic fungal infections. The cost of completed and planned training in 12 countries is approximately US$ 2 million. (3) Pfizer’s administrative support of the program is approximately US$ 1 million. This includes professional staff, consultants, outside services, production of educational materials and brochures, shipping services, audit and assessment.
Page 5
• Pfizer now supports the DPP in 11 countries and extends their offer without dollar or time limits to the Least Developed Countries most in need.
Figure 1. South Africa map of the Diflucan Partnership Programme overlaid on the Provincial HIV deaths reported as a percentage of the 2002 population.12
Lessons Learned
The collaboration between Pfizer and the South African government leads to one critical conclusion: the partners were able to mount an effective long-term program because of the initial environment of trust and open communication that occurred prior to the product being introduced into the system. Clearly, addressing public health problems in less developed countries is not a simple matter of sending a shipment of medicines to the country, whether the product is free, discounted or not. The more we view donation efforts as accretive rather than destructive to market-led answers to providing access to health care, the more these partnerships will seed the pathway for other initiatives, fostering a model of trust and cooperation necessary to achieve an ultimate solution to the global AIDS crisis.
Based on our direct experience in negotiating public-private partnerships, we suggest that eight principles must be set as pre-conditions for going forward in forging a successful bond. These are:
12
Source: Pfizer Inc and MRC in South Africa, 2002. Prepared by Miriam Pfisterer.
±
Gauteng (28) Kwazulu Natal (58) Eastern Cape (25) Northern Cape (8) Western Cape (68) Northern Province (33) Free State (24) Mpumalanga (23) North West (19) Legend 1 Dot = 50 update.TOT_SCRIPT HIV_Deaths 0.18 - 0.20 0.21 - 0.40 0.41 - 0.60 0.61 - 0.80 0.81 - 1.00South Africa Diflucan Program: Total Cumulative OC/CM Scripts & 2002 Provincial HIV Deaths as % of Population
(# of Operational Rollout Sites)
Total Scripts (June 02) HIV Deaths as % of 2002 Pop.
Page 6
1. Establish an agreement between the principle responsible parties in advance and discuss how those
strategies will be practically implemented, including contingency plans for incidences such as theft and establishment of working national or regional task forces with participation from reliable staff;
2. Give each party equity so they have more than altruistic reasons to care about the outcome of the
program;
3. Publicize the program so that professionals and the general public are aware of the parameters of what is offered;
4. Provide training to health care professionals to reinforce knowledge of treatment regimens and ensure that medicine is properly dispensed;
5. Holding periodic meetings among partners to modify programmes or address issues is critical to
continuing trust, assignment of accountability and prevention of major dysfunction;
6. Line managers must be frequently informed to maintain interest and share the vision that senior
officials or executives who set up these programmes intend;
7. Resources from both partners must be set aside to form complementary partnerships, address problems and act upon identified gaps in logistics;
8. Detailed reporting, both on a descriptive and analytical level, is critical to measuring successes and capturing problems.
Page 7
APPENDIX I —Pfizer s Product Donations Decision Tree
Is there both a market failure and a public health crisis?
No action.
Can we uniquely address the problem? Can we afford the program? No action.
Are we invited by the country (MoH, President)?
Make offer via letter.
Are systems in place to absorb product? Are risks acceptable? (requires monitoring, auditing and consultation with Ministry)
1. Solidify plan for assessment. Is the problem insurmountable? 2. Estimate product needs based on
epidemiology and access structures. 3. Refine program costs, establish and request budget.
No action. Assess what contribution partners will make to the strategic alliance to fix problem. Are they willing to commit resources?
Defer program until problems are fixed.
Is the program reaching facilities and patients?
(requires accurate reporting on dispensing forms and prescription pads)
- Continue gathering proxy measures - Work with the MoH to determine/investigate for process & outcome assessment. problem.
- Obtain feedback from the field - Take action as necessary (decide jointly with (through NGO & government contacts, partners).
and site visits) - Report to senior management how issue was
- Report to senior management. addressed with next steps. - Share reports with partners.
No Yes Yes No Yes No No No Yes Yes Yes Yes No No
Page 8
APPENDIX II — Pfizer Diflucan Partnership Timeline
Country Type of Partnership (Government or NGO) Program Launch (Signing of Memorandum of Understanding with Pfizer) Number of health workers trained to provide HIV/AIDS-related care*
South Africa Government December 1, 2000 9,036
Uganda Government February 8, 2002 65
Swaziland Government February 11, 2002 60
Botswana Government February 13, 2002 151
Namibia Government February 21, 2002 65
Lesotho Government February 27, 2002 99
Malawi Government June 25, 2002 90
Tanzania Government August 20, 2002 50
Rwanda Government September 17, 2002 35
Mozambique Government September 20, 2002
Ghana NGO – Family
Health International
Trainings planned for 2003
Haiti NGO – Partners in
Health
Trainings planned for 2003 * As of December 2002