The n e w e n g l a n d j o u r n a l of m e d i c i n e
c l i n i c a l p r a c t i c e
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines,
when they exist. The article ends with the authors’ clinical recommendations.
Small Abdominal Aortic Aneurysms
Janet T. Powell, M.D., Ph.D., and Roger M. Greenhalgh, M.D.From the University Hospitals of Coventry and Warwickshire, National Health Service Trust, Coventry, United Kingdom (J.T.P.); and the Department of Vascular Surgery, Imperial College at Charing Cross, London (R.M.G.). Address reprint requests to Dr. Powell at the University Hospitals of Cov-entry and Warwickshire, NHS Trust, Clifford Bridge Rd., Coventry CV2 2DX, United King-dom, or at [email protected]. N Engl J Med 2003;348:1895-901.
Copyright © 2003 Massachusetts Medical Society.
A 68-year-old man with a 50-year history of smoking presented with amaurosis fugax and was found to have an incidental infrarenal aortic dilatation, with a maximal diam-eter of 3.2 cm. After five years of routine follow-up, the aortic diamdiam-eter has increased to 4.8 cm. What is the appropriate follow-up for and management of this case?
In the absence of symptoms related to an aneurysm, the threat that the aneurysm will rupture is the major consideration. Only 10 to 15 percent of patients survive the rupture of an abdominal aortic aneurysm; a minority reach the hospital alive, and of these, only about half survive the emergency surgical repair.1 But overall, few patients with
aneu-rysms die from a ruptured aneurysm; most (approximately 66 percent) will die from another cardiovascular cause.
Ultrasonographic screening studies show that about 5 percent of men older than 65 years of age have an occult small aneurysm (3 to 6 cm in diameter).2 The risk of rupture
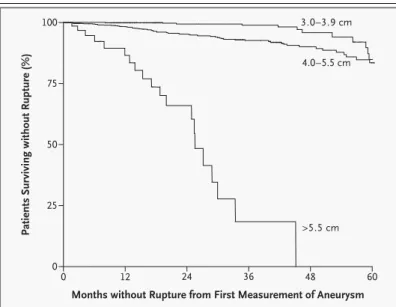
of small aneurysms is low, but the natural history of an untreated aneurysm is one of con-tinued expansion.3 When the diameter of the aneurysm exceeds 5.5 cm, the risk of
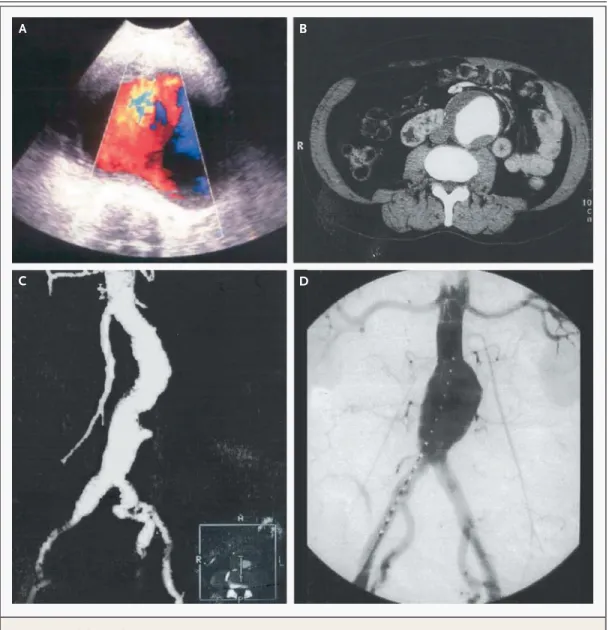
rup-ture increases markedly (Fig. 1), and all vascular surgeons would recommend repair of aneurysms larger than 6 cm, provided that the patient was fit for surgery.4 Aneurysms
this large (Fig. 2) account for less than 10 percent of aneurysms detected by screening.5
What recommendations should be made for those with smaller aneurysms? e p i d e m i o l o g y
The prevalence of abdominal aortic aneurysms among men is about three times that among women, and women younger than 55 years of age rarely have such aneurysms. The age-related increase in the diameter of the infrarenal aorta in men (median diameter, 1.75 cm at 25 years of age and 2.25 cm at 55 years of age) is more marked than that in women.6 After 55 years of age, the median diameter remains constant, but the
distri-bution becomes skewed toward larger diameters: 6 percent of men have an aortic diam-eter of more than 2.9 cm by 65 years of age.6 Thereafter, the prevalence of aneurysms (as
indicated by an aortic diameter of 3 cm or larger) among men increases by about 6 per-cent per decade. Clinically relevant aneurysms (at least 4 cm in diameter) are found in about 1 percent of men 55 to 64 years of age, and the prevalence increases by 2 to 4 per-cent per decade thereafter.6,7
Smoking is the strongest independent risk factor7: 90 percent of patients with
aneu-rysms have smoked. As compared with persons who have never smoked, the incidence of aneurysm is increased by a factor of six among those who have smoked for more than 40 years and by a factor of seven among those who have smoked more than 20 cig-arettes per day.8 After smoking cessation, the risk of development of an aneurysm
declines each year by approximately 1/
30 of the original risk.8
The n e w e n g l a n d j o u r n a l of m e d i c i n e
p a t h o g e n e s i s
Atherosclerosis has been considered to be a cause of abdominal aortic aneurysms, since studies show a positive relation between aneurysm and other car-diovascular disease and related markers, ranging from a history of previous carotid or coronary artery disease to the measured ankle–brachial pressure in-dex.9,10 Selective screening for aneurysms in
pa-tients with intermittent claudication nearly doubles the yield of screening in the general population, whereas screening of cohorts of patients with hyper-lipidemia or hypertension often does not.11
Screen-ing of siblScreen-ings (older than 50 years of age) of pa-tients with aneurysms revealed an occult aneurysm (3.3 to 6.5 cm) in 29 percent of brothers and 6 per-cent of sisters.12
Abdominal aortic aneurysm is a familial disor-der, possibly genetic (polygenic) in origin.13
Mono-genic disorders associated with an increased risk of aortic aneurysm — including the fibrillin-1 defect (Marfan’s syndrome) and abnormal type III procol-lagen (Ehlers–Danlos syndrome type IV) — are rare. Proteolysis and inflammation are the biologic mech-anisms driving the expansion of aneurysms.14
Evi-dence from studies in mice and humans indicates that metalloproteases have an important role in the formation of aneurysms, particularly the mac-rophage-associated enzyme MMP-9.15 Currently,
there is no strong evidence linking variation in pro-tease or propro-tease-inhibitor genes with the likelihood of the development of an aneurysm, but a debate has started over whether functional gene polymor-phisms can predict the outcome.16 Patients with an
aortic aneurysm who had an interleukin-6 genotype associated with high plasma interleukin-6 concen-trations had three-year overall mortality that was twice that among patients without this genotype.17
The 4G/5G polymorphism in the plasminogen-acti-vator inhibitor type 1 (PAI-1) gene promoter alters plasma PAI-1 levels and hence fibrinolysis. Patients with the PAI-1 5G5G genotype, which is associated with the lowest plasma PAI-1 levels in vivo, had low-er oplow-erative mortality aftlow-er elective aneurysm repair than patients with other PAI-1 genotypes (0 percent vs. 8 percent).18
s u r g i c a l i n t e r v e n t i o n
Two large randomized trials have addressed the is-sue of whether elective surgical repair of small ab-dominal aortic aneurysms saves lives. Patients with asymptomatic aneurysms (diameter, 4.0 to 5.5 cm) were randomly assigned to either early elective (open) surgery or a period of surveillance for rapid expansion and the development of symptoms, with a protocol recommending surgery when the diam-eter exceeded 5.5 cm. The United Kingdom Small Aneurysm Trial, in which ultrasonographic surveil-lance was used, showed that the cumulative 6-year survival rate was 64 percent in both treatment groups, the risk of aneurysm rupture was 1 percent per year, and the 30-day operative mortality among patients who underwent elective repair was 5.6 per-cent.19,20 The Aneurysm Detection and
Manage-ment (ADAM) Veterans Affairs Cooperative Study, in which surveillance was primarily conducted by computed tomography (CT), showed a six-year cu-mulative survival rate of 74 percent in each treatment group, rates of rupture of 0.6 percent per year, and operative mortality of 2.7 percent.21 The absolute
differences between the two trials probably relate to the different populations studied. The United King-dom trial included a substantial proportion of wom-en (17 percwom-ent). Patiwom-ents in the ADAM study cohort were more fit, with better lung and renal function and more favorable lipid profiles.22 Both studies
demonstrated that elective surgery for small aneu-rysms does not improve six-year survival.
Longer-term follow-up, to 9 years, in patients in
s t r a t e g i e s a n d e v i d e n c e
Figure 1. Risk of Rupture of Aneurysm According to the First Measured Aortic Diameter.
The analysis is based on information from 1792 men and 465 women with ab-dominal aortic aneurysms.
Patients Surviving without Rupture (%)
Months without Rupture from First Measurement of Aneurysm 100 75 50 25 0 0 12 24 36 48 60 3.0–3.9 cm >5.5 cm 4.0–5.5 cm
c l i n i c a l p r a c t i c e
the United Kingdom trial showed no significant dif-ference in the mean survival between the surgery group and the surveillance group (6.7 years and 6.5 years, respectively).22 However, there was a
margin-al late benefit in overmargin-all survivmargin-al in the surgery group (P=0.05). This is not a finding that supports a change in practice, since the results were largely at-tributable to changes in lifestyle, including smoking cessation prompted by surgery.23 The higher costs
of treatment associated with a policy of early sur-gery22 reinforce the preference for
ultrasonograph-ic surveillance for men with small aneurysms, particularly in places where there is tax-funded health care.
The results of both trials may inform decisions about the timing of surgery, since about three quar-ters of the patients in the surveillance group eventu-ally underwent surgery. Neither trial provided clear evidence that the 30-day mortality from elective sur-gery increased with age. Biologic age, as reflected by measures of lung, cardiac, and renal function, ap-pears to be more important.1,20,24 There is no
ro-Figure 2. An Abdominal Aortic Aneurysm.
Panel A is a duplex ultrasonographic image, with the central sector showing the color flow. Panel B is a planar computed tomographic (CT) image, Panel C a CT angiographic image, and Panel D a fluoroscopic image obtained during endovas-cular repair.
A B
The n e w e n g l a n d j o u r n a l of m e d i c i n e
bust, prospectively validated method for selecting patients who have low operative risk. Although al-most half the early deaths that occur after elective aneurysm repair are attributed to cardiac causes, preoperative cardiac testing may not identify those patients who are at the highest risk.25 Instead,
pa-tients with poor lung and renal function have the highest risk of death after elective open surgical repair1,20,24-26: for patients with a serum creatinine
concentration of more than 1.2 mg per deciliter (104 µmol per liter) and a forced expiratory volume in one second of less than 2.0 liters, the risk of death could exceed 10 percent. Preoperative physiothera-py should be recommended, since it improves out-come after major abdominal surgery.27 Even with
low operative mortality, the ADAM study failed to show a survival benefit associated with a policy of early surgery.
In men, surgery can safely be delayed until the aneurysm exceeds 5.5 cm in diameter, because the risk of rupture is low. The risk of rupture is negligi-ble for aneurysms with a diameter of less than 4 cm, but the risk increases with increasing diameter (Fig. 1). However, the risk of rupture is four times as high among women as among men.22 The fact that
an-eurysms rupture at smaller diameters in women may simply reflect the tendency for the normal di-ameter of the aorta to be smaller in women than in men, with a fixed diameter representing a greater dilatation as a proportion of the original diameter.6
For women, the threshold diameter of 5.5 cm for aneurysm repair is probably too high, but trial data do not permit the specification of a lower threshold. s m o k i n g c e s s a t i o n a n d m e d i c a l t h e r a p y The therapeutic goal is to prevent small aneurysms from reaching a size at which the risk of rupture is high. Data from population screening show wide variability in the rates of expansion of aneurysms, but growth appears to be exponential. One study re-ported growth rates of 2.0, 3.4, and 6.4 mm per year for aneurysms that began at 3.0 to 3.9 cm, 4.0 to 4.9 cm, and 5.0 to 5.9 cm, respectively.3 Effective
medical therapy must reduce the rate of expansion by more than 50 percent in order to keep a 4-cm an-eurysm from reaching the 5.5-cm threshold within five years.
Smoking, the only consistent risk factor for ex-pansion of aneurysms, increases the growth rate by 20 to 25 percent.3,8,28-30 Data from 1743 patients
followed prospectively showed that aneurysms ex-panded significantly more rapidly (by a mean of 0.29
cm per year) in current smokers than in former smokers (mean, 0.25 cm per year). Blood pressure and cholesterol levels did not predict the rate of ex-pansion, and the rate was slower in patients with diabetes than in those without diabetes.30 The risk
of rupture and the risk of death due to rupture are higher among current smokers than among former smokers and patients who never smoked — by as much as a factor of 14 for smokers of hand-rolled cigarettes.1,31
There is a dearth of information about the treat-ment of hypertension and hyperlipidemia in patients with aneurysms and conflicting evidence about how these and other cardiovascular risk factors relate to the progression of disease.32,33 Propranolol does
not reduce the growth rate of small aneurysms and impairs quality of life.34 Statins have both
lipid-low-ering and antiinflammatory actions, but none of the trials of statins have evaluated aortic diameter. Antioxidant vitamin supplementation (with alpha-tocopherol, beta carotene, or both) does not reduce the incidence of aneurysm or rupture.35
Doxycy-cline, an antibiotic that is effective against Chlamyd-ia pneumonChlamyd-iae and an inhibitor of metalloproteases, awaits evaluation in a large randomized trial assess-ing its efficacy in slowassess-ing the expansion of aneu-rysms.36 The results of a small trial suggest that a
short course of roxithromycin reduces expansion for 12 months,37 but more data are needed. For
pa-tients with aneurysms, modification of cardiovascu-lar risk factors is more likely to prolong life in ways other than by slowing the expansion of aneurysms. s c r e e n i n g a n d s u r v e i l l a n c e
Abdominal aortic aneurysms are not always asymp-tomatic, and tenderness on aortic palpation, back pain, abdominal pain, and intermittent claudication can all be aneurysm-related symptoms. Abdominal palpation has neither the sensitivity nor the specific-ity of ultrasonography in screening for aneurysm.38
Evidence from two studies suggests that one-time ultrasonographic screening of men, at the age of 65 years, is sufficient to identify nearly all those who are at risk.39,40 Twelve years after screening, no subject
with an initial aortic diameter of less than 2.6 cm had had aneurysm repair or rupture, and all survivors had an aortic diameter of less than 4 cm.39 Recently,
a trial involving 67,800 men in the United Kingdom demonstrated that screening halves the rate of an-eurysm-related death within four years but does not reduce overall mortality and does reduce quality of life (principally patients’ perceptions of their own
c l i n i c a l p r a c t i c e
health).41 Without a medical therapy that limits the
growth of aneurysms, population-screening pro-grams may not be cost effective.42
Screening and surveillance programs must be rigorous and have stringent quality control. Ultra-sonographic monitoring of previously diagnosed aneurysms is reliable, safe, noninvasive, and rela-tively inexpensive.42 There has been no formal
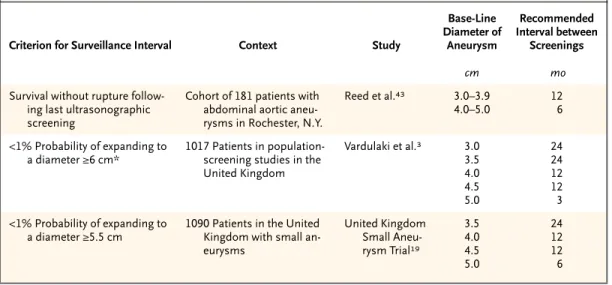
eval-uation of the benefits of screening persons with a history of smoking or a family history of aneurysms. Evidence concerning the appropriate interval be-tween screenings comes from the analysis of the previous diameter of the aneurysm, the rate of growth, and rates of rupture (Table 1). If women were considered for surgery when their aneurysms reached a diameter of 5 cm, screening intervals of 12 months could be recommended for aneurysms with diameters of 3.0 to 4.4 cm, and intervals of 6 months for aneurysms with diameters of 4.5 to 5.5 cm. On this basis, approximately 5 percent of pa-tients would be considered for surgery at each sur-veillance visit.
e n d o v a s c u l a r r e p a i r
Conventional open repair of aneurysms with re-placement with a Dacron (polyester) graft is a major surgical procedure. The expectation that endovas-cular repair, first described in 1985,44 poses less
op-erative risk than conventional repair remains
un-proved. Endovascular repair requires radiologic and surgical skills. Under local or general anesthesia, a stent–graft system is introduced through the fem-oral artery, and either self-expanding or balloon-expanding stents are used to trap a Dacron prosthe-sis, with the proximal end precisely below the lower renal artery. The common devices are bifurcated and modular and incorporate stents in the wall to facil-itate distal iliac fixation. Some devices use hooks and barbs to secure better fixation and prevent de-vice migration.
“Endoleaks” — leaks from fabric tears or be-tween modular systems that permit continued per-fusion and expansion of the aneurysmal sac — can lead to rupture. In 2001, the Food and Drug Admin-istration issued a public health notification follow-ing reports of adverse events related to the integrity of devices and vascular damage that occurred with two approved products, and these products were withdrawn from the market. In 2002, the Medical Devices Agency of the United Kingdom issued sim-ilar alerts about three additional devices. To assess problems in the future, close surveillance of devices used for endovascular repair of aneurysms is recom-mended, usually with repeated CT scanning one and three months after repair and annually thereafter. The effect of increased exposure to radiation from CT surveillance is unknown. Although ultrasonog-raphy is useful in the measurement of the diameter of the sac, endoleaks (which complicate 10 to 20 percent of repairs) are often missed; magnetic
res-a r e res-a s o f u n c e r t res-a i n t y
* In the case of an aneurysm with a diameter of 5.0 cm, the 1 percent threshold was exceeded. Table 1. Recommended Intervals for Surveillance for Small Aneurysms.
Criterion for Surveillance Interval Context Study
Base-Line Diameter of Aneurysm Recommended Interval between Screenings cm mo
Survival without rupture follow-ing last ultrasonographic screening
Cohort of 181 patients with abdominal aortic aneu-rysms in Rochester, N.Y.
Reed et al.43 3.0–3.9 4.0–5.0 12 6 <1% Probability of expanding to a diameter ≥6 cm* 1017 Patients in population- screening studies in the United Kingdom Vardulaki et al.3 3.0 3.5 4.0 4.5 5.0 24 24 12 12 3 <1% Probability of expanding to a diameter ≥5.5 cm
1090 Patients in the United Kingdom with small an-eurysms United Kingdom Small Aneu-rysm Trial19 3.5 4.0 4.5 5.0 24 12 12 6
The n e w e n g l a n d j o u r n a l of m e d i c i n e
onance imaging takes longer, is more expensive, and cannot be used for stainless-steel–based de-vices.45,46
There is, at present, no evidence that the risk of rupture of an aneurysm is reduced after endovascu-lar repair; the reported risk of rupture is 1 percent per year47 — similar to that for patients who have
not undergone surgery and are followed in surveil-lance programs.19,21 The majority of reports on
en-dovascular repair have thus far been from single-center, nonrandomized studies.48 Such studies are
subject to bias and exclude patients who are con-sidered to be poor candidates for endovascular re-pair, usually because the neck of the aneurysm is unsuitable for the fixation of a graft (although in-creasing experience and technological advances should improve the generalizability of this proce-dure). Randomized trials comparing open surgical repair with endovascular repair are under way. p a t i e n t s ’ p r e f e r e n c e s a n d t i m i n g o f s u r g e r y
Patients’ preferences for treatment, including the potential timing of any corrective procedure, should be considered. The awareness that one may have to undergo major surgery in the future may impair one’s quality of life. In the United Kingdom Small Aneurysm Trial,23 there were only small
differenc-es in the quality of life (as evaluated by a short qudifferenc-es- ques-tionnaire) at one year between those assigned to ear-ly surgery and those assigned to ultrasonographic surveillance. However, survivors of early elective sur-gery perceived their health to be better than did pa-tients in the surveillance group.23 Hospitalization
for surgery may promote smoking cessation, with associated improvements in health and survival.22
The potential for medical therapy to slow or arrest the growth of an aneurysm could also influence the preferences of patients in the future.
There are no formal guidelines for the screening or management of small abdominal aortic aneurysms.
In the case of a patient with a small abdominal aor-tic aneurysm, such as the case described in the vi-gnette, the first step is to counsel the patient to stop smoking and to recommend nicotine replacement, bupropion, or both, as necessary. Hyperlipidemia and hypertension should be adequately treated, al-though there are no data to indicate that the expan-sion of aneurysms is slowed by such therapy. Be-cause data from two large trials did not indicate that early elective surgery improves survival, the patient should undergo regular surveillance, with repeated ultrasonographic screening at six-month intervals. The aneurysm is likely to reach 5.5 cm in diameter in about two years, during which time endovascular technology will most likely have improved further and medical therapy may be on the horizon. When the diameter of the aneurysm exceeds 5.5 cm, sur-gery (or possibly endovascular repair, depending on the results of ongoing clinical trials) would be ap-propriate, following assessment of lung, renal, and cardiac function.
g u i d e l i n e s
s u m m a r y a n d r e c o m m e n d a t i o n s
r e f e r e n c e s
1. Brown LC, Powell JT. Risk factors for aneurysm rupture in patients kept under ul-trasound surveillance. Ann Surg 1999;230: 289-96.
2. Scott RA, Ashton HA, Kay DN. Abdomi-nal aortic aneurysm in 4237 screened pa-tients: prevalence, development and man-agement over 6 years. Br J Surg 1991;78: 1122-5.
3. Vardulaki KA, Prevost TC, Walker NM, et al. Growth rates and risk of rupture of ab-dominal aortic aneurysms. Br J Surg 1998; 85:1674-80. [Erratum, Br J Surg 1999;86: 280.]
4. Powell JT, Greenhalgh RM, Ruckley CV, Fowkes FGR. Prologue to a surgical trial. Lancet 1993;342:1473-4.
5. Abdominal aortic aneurysms: report of a meeting of physicians and scientists,
Uni-versity College London Medical School. Lancet 1993;341:215-20.
6. Singh K, Bønaa KH, Jacobsen BK, Bjørk L, Solberg S. Prevalence of and risk factors for abdominal aortic aneurysms in a popula-tion-based study: the Tromso Study. Am J Epidemiol 2001;154:236-44.
7. Lederle FA, Johnson GR, Wilson SE, et al. Prevalence and associations of abdominal aortic aneurysm detected through screening. Ann Intern Med 1997;126:441-9.
8. Wilmink TBM, Quick CRG, Day NE. The association between cigarette smoking and abdominal aortic aneurysms. J Vasc Surg 1999;30:1099-105.
9. Pleumeekers HJ, Hoes AW, van der Does E, et al. Aneurysms of the abdominal aorta in older adults: the Rotterdam Study. Am J Epidemiol 1995;142:1291-9.
10.Alcorn HG, Wolfson SK Jr, Sutton-Tyrrell K, Kuller LH, O’Leary D. Risk factors for ab-dominal aortic aneurysms in older adults en-rolled in the Cardiovascular Health Study. Ar-terioscler Thromb Vasc Biol 1996;16:963-70.
11.Allardice JT, Allwright GJ, Wafula JM, Wyatt AP. High prevalence of abdominal aortic aneurysm in men with peripheral vas-cular disease: screening by ultrasonogra-phy. Br J Surg 1988;75:240-7.
12.Bengtsson H, Norrgard O, Angquist K-A, Ekberg O, Oberg L, Bergqvist D. Ultra-sonographic screening of the abdominal aor-ta among siblings of patients with abdominal aortic aneurysms. Br J Surg 1989;76:589-91.
13.Tilson MD. Aortic aneurysms and ath-erosclerosis. Circulation 1992;85:378-9.
14.Shah PK. Inflammation, metalloprotein-ases, and increased proteolysis: an emerging
c l i n i c a l p r a c t i c e
pathophysiological paradigm in aortic an-eurysm. Circulation 1997;96:2115-7.
15.Pyo R, Lee JK, Shipley JM, et al. Targeted gene disruption of matrix metalloprotein-ase-9 (gelatinase B) suppresses development of experimental abdominal aortic aneu-rysms. J Clin Invest 2000;105:1641-9.
16.Marian AJ. On genetics, inflammation, and abdominal aortic aneurysm: can single nucleotide polymorphisms predict the out-come? Circulation 2001;103:2222-4.
17.Jones KG, Brull DJ, Brown LC, et al. In-terleukin-6 (IL-6) and the prognosis of ab-dominal aortic aneurysms. Circulation 2001; 103:2260-5.
18.Jones KG, Powell JT, Brown LC, Green-halgh RM, Jormsjö S, Eriksson P. The influ-ence of 4G/5G polymorphism in the plas-minogen activator inhibitor-1 gene promoter on the incidence, growth and operative risk of abdominal aortic aneurysm. Eur J Vasc En-dovasc Surg 2002;23:421-5.
19.The UK Small Aneurysm Trial Partici-pants. Mortality results for randomised controlled trial of early elective surgery or ultrasonographic surveillance for small ab-dominal aortic aneurysms. Lancet 1998; 352:1649-55.
20.Brady AR, Fowkes FG, Greenhalgh RM, Powell JT, Ruckley CV, Thompson SG. Risk factors for postoperative death following elective surgical repair of abdominal aortic aneurysm: results from the UK Small Aneu-rysm Trial. Br J Surg 2000;87:742-9.
21.Lederle FA, Wilson SE, Johnson GR, et al. Immediate repair compared with surveil-lance of small abdominal aortic aneurysms. N Engl J Med 2002;346:1437-44.
22.The United Kingdom Small Aneurysm Trial Participants. Long-term outcomes of immediate repair compared with surveil-lance for small abdominal aortic aneurysms. N Engl J Med 2002;346:1445-52.
23.Idem. Health service costs and quality of
life for early elective surgery or ultrasono-graphic surveillance for small abdominal aortic aneurysms. Lancet 1998;352:1656-60.
24.Steyerberg EW, Kievit J, de Mol Van Ot-terloo JC, van Bockel JH, Eijkemans MJ, Habbema JD. Perioperative mortality of elec-tive abdominal aortic aneurysm surgery: a clinical prediction rule based on literature and individual patient data. Arch Intern Med 1995;155:1998-2004.
25.D’Angelo AJ, Puppala D, Farber A, Mur-phy AE, Faust GR, Cohen JR. Is preoperative cardiac evaluation for abdominal aortic an-eurysm repair necessary? J Vasc Surg 1997; 25:152-6.
26.Yasuhara H, Ishiguro T, Muto T. Factors affecting late survival after elective abdomi-nal aortic aneurysm repair. Br J Surg 1999; 86:1047-52.
27.Fagevik Olsen M, Hahn I, Nordgren S, Lonroth H, Lundholm K. Randomized con-trolled trial of prophylactic chest physio-therapy in major abdominal surgery. Br J Surg 1997;84:1535-8.
28.MacSweeney STR, Ellis M, Worrell PC, Greenhalgh RM, Powell JT. Smoking and growth rate of small abdominal aortic aneu-rysms. Lancet 1994;344:651-2.
29.Chang JB, Stein TA, Liu JP, Dunn ME. Risk factors associated with rapid growth of small abdominal aortic aneurysms. Surgery 1997;121:117-22.
30.Brady AR, Thompson SG, Greenhalgh RM, Powell JT. Cardiovascular risk factors and abdominal aortic aneurysm expansion: only smoking counts. Br J Surg 2003;90: 492-3. abstract.
31.Strachan DP. Predictors of death from aortic aneurysm among middle-aged men: the Whitehall Study. Br J Surg 1991;78:401-4.
32.Reed D, Reed C, Stemmermann G, Ha-yashi T. Are aortic aneurysms caused by ath-erosclerosis? Circulation 1992;85:205-11.
33.Lee AJ, Fowkes FG, Carson MN, Leng GC, Allan PL. Smoking, atherosclerosis, and risk of abdominal aortic aneurysm. Eur Heart J 1997;18:671-6.
34.Propranolol Aneurysm Trial Investiga-tors. Propranolol for small abdominal aortic aneurysms: results of a randomized trial. J Vasc Surg 2002;35:72-9.
35.Tornwall ME, Virtamo J, Haukka JK, Al-banes D, Huttunen JK. Alpha-tocopherol (vitamin E) and beta-carotene supplementa-tion do not affect the risk for large abdomi-nal aortic aneurysm in a controlled trial. Atherosclerosis 2001;157:167-73.
36.Baxter BT, Pearce WH, Waltke EA, et al. Prolonged administration of doxycycline in patients with small asymptomatic abdomi-nal aortic aneurysms: report of a prospective (Phase II) multicentre study. J Vasc Surg 2002;36:1-12.
37.Vammen S, Lindholt JS, Ostergaard L, Fasting H, Henneberg EW. Randomized double-blind controlled trial of roxithromy-cin for prevention of abdominal aortic aneu-rysm expansion. Br J Surg 2001;88:1066-72. [Erratum, Br J Surg 2002;89:120-1.]
38.Lederle FA, Walker JM, Reinke DB. Se-lective screening for abdominal aortic aneu-rysms with physical examination and ultra-sound. Arch Intern Med 1988;148:1753-6.
39.Crow P, Shaw E, Earnshaw JJ, Poskitt KR, Whyman MR, Heather BP. A single nor-mal ultrasonographic scan at age 65 years rules out significant aneurysm disease for life in men. Br J Surg 2001;88:941-4.
40.Scott RAP, Vardulaki KA, Walker NM, Day NE, Duffy SW, Ashton HA. The long-term benefits of a single scan for abdominal aortic aneurysm (AAA) at age 65. Eur J Vasc Endovasc Surg 2001;21:535-40.
41.Ashton HA, Buxton MJ, Day NE, et al. The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomised controlled trial. Lancet 2002; 360:1531-9.
42.Multicentre Aneurysm Screening Study Group. Multicentre aneurysm screening study (MASS): a cost effectiveness analysis for screening for abdominal aortic aneu-rysms based on four year results from a ran-domised controlled trial. BMJ 2002;325: 1135-8.
43.Reed WW, Hallett JW Jr, Damiano MA, Ballard DJ. Learning from the last ultra-sound: a population-based study of patients with abdominal aortic aneurysm. Arch In-tern Med 1997;157:2064-8.
44.Volodos’ NL, Shekhanin VE, Karpovich IP, Troian VI, Gur’ev IA. A self-fixing syn-thetic blood vessel endoprosthesis. Vestn Khir IM Grek 1986;137:123-5. (In Russian.)
45.Wolf YG, Johnson BL, Hill BB, Rubin GD, Fogarty TJ, Zarins CK. Duplex ultra-sound scanning versus computed tomo-graphic angiography postoperative evalua-tion of endovascular abdominal aortic aneurysm repair. J Vasc Surg 2000;32:1142-8.
46.McWilliams RG, Martin J, White D, et al. Detection of endoleak with enhanced ultra-sound imaging: comparison with biphasic computed tomography. J Endovasc Ther 2002;9:170-9.
47.Harris PL, Vallabhaneni SR, Desgranges P, Becquemin JP, van Marrewijk C, Laheij RJ. Incidence and risk factors of late rupture, conversion, and death after endovascular re-pair of infrarenal aortic aneurysms: the EUROSTAR experience. J Vasc Surg 2000; 32:739-49.
48.Teufelsbauer H, Prusa AM, Wolff K, et al. Endovascular stent grafting versus open surgical operation in patients with infrare-nal aortic aneurysms: a propensity score-adjusted analysis. Circulation 2002;106: 782-7.