Investigating the relationship between emotional intelligence and transformation leadership
in Nurse Managers
Katrina Perroud *
Deputy Director of Nursing at Lyndoch Warrnambool
Lyndoch, Warrnambool Inc., Hopkins Road, Warrnambool, Vic, 3280
Email: [ddon@lyndoch.org.au]
Katrina holds the position of Deputy Director of Nursing at Lyndoch Warrnambool Inc., which is the
largest provider of residential services in the South-West region of Victoria. In addition to the
organizations vast community services, Lyndoch provides accommodation for 85 high care residents and
112 people with low care needs. With over twenty years experience as a nurse Katrina has been fortunate
to develop expertise in the areas of education and management. After working as a clinical coordinator
and educator for nine years Katrina branched into Management by taking a post as a Nurse Manager.
Katrina has also managed a Hostel and held the position of Associate Director of Nursing at a large
sub-acute metropolitan hospital in Melbourne. Katrina has completed her Masters in Business Administrative
Management with her minor thesis focusing on Emotional Intelligence and Transformational Leadership
with plans to commence her PhD next year. Katrina has a keen interest in clinical risk management, staff
development and leadership in nursing.
Deb Stewart
School of Management, Victoria University, Melbourne, Australia
Email: deb.stewart@vu.edu.au
Profile:
Deb Stewart is a Senior Lecturer and Coordinator for the M.Bus. (Management) at Victoria
University. In 2004, Deb won the Vice Chancellor’s and Dean‘s Awards for Teaching Excellence and in
2005 was a finalist in the ANZAM and Pearson Education, Management Educator of the Year Award. She
is coordinator for Organisation Change Management, Work and Organisation Systems and Organisation
Analysis and Behaviour at the Masters level. Deb has a Masters and Grad.Dip. in Organisation
Behaviour (Swinburne) and is undertaking a PhD at the same university. She completed B.Arts and
Dip.Ed. (Monash University) and Grad.Dip.AdminStuds (Chisholm IT), She has presented conference
papers and published papers on quality management, the learning organisation, managing change, and
gender, leadership and power.
Preferred Stream:
Management Education and Development
ABSTRACT
In a world where organizations are faced with increasing challenges effective leadership becomes central
to success. Many studies on leadership have resulted in the belief that transformational leadership
behaviour is central to effective leadership and subsequent positive organizational outcomes. If we adopt
the philosophy that transformational leadership is the preferred behaviour of effective leaders, then what
predisposes an individual to behave in this way? There is growing evidence that that emotional
intelligence is a major catalyst in pre-empting transformational leadership behaviours.
This paper aims to explore emotional intelligence as the “concept of possibility” to ignite
transformational leader behaviour. This study seeks to explore whether there is a relationship between
emotional intelligence and transformational leadership in Nurse Managers. Little research to date on
leadership in healthcare has demonstrated a connection between emotional intelligence and
transformational leadership. In order to explore the relationship between these two constructs, self-report
and observation measures of emotional intelligence were employed in addition to superior and
subordinate rating of transformational leadership behaviour in nurse managers. Results from this study
suggest that emotional intelligence, as measured by the ability to monitor and manage emotions in oneself
and others, is positively related to transformational leadership behaviour and therefore may be a skill that
underpins this leadership style.
KEYWORDS
Leadership, attitudes, emotions, interpersonal behaviour, communication, power and influence.
PURPOSE
Organizational success can largely be attributed to how effective the core functions of the organization are
managed and led (Vance and Larson 2002). In today’s context, a leader’s capability has the power to
either positively or negatively influence individual and group performance and in turn is the success or
otherwise of the organization. Over recent years, a growing body of knowledge has emerged as leadership
researchers gather evidence to support transformational leadership as the preferred model for effecting
organisational success (Pillai and Williams 2004; Leban and Zulauf 2004; Sosik and Dworakivsky 1998).
As researchers embark on a journey of exploration in order to determine what predisposes an individual to
exhibit transformational leader behaviour, interest is being generated in a concept called emotional
intelligence (EI), with a strong indication that this construct could be a major catalyst to transformational
leadership in action (Ashkanasy and Daus 2002; Prati et al 2003; George 2000).
The overall aim of the research was to explore whether Nurse Managers who exhibit high levels of
emotional intelligence, (i.e. self-awareness, self-management, social awareness, and relationship
management) demonstrate greater transformational leadership behaviours (i.e. idealized influence,
inspirational motivation, intellectual stimulation, and individualized consideration) as opposed to Nurse
Managers who exhibit low levels of emotional intelligence.
This research is intended to assist in establishing some clarity regarding the connection between emotional
intelligence and transformational leadership and to help guide future research on the interrelatedness
between these two constructs and their impact in organizations. The study was conducted at a large
metropolitan hospital in Melbourne, Victoria, Australia, which employs approximately 3500 staff and
treats more than one quarter of a million patients annually. This health service provides a comprehensive
range of specialist medical and surgical services and accommodates six directorates comprising of 42
clinical units
.
Support for the research project being conducted at the hospital was obtained through the
organization’s Ethics Committee.
DESIGN / METHODOLOGY
The focus of the study is not to determine whether the tools used within this research project are reliably
constructed, although the researcher acknowledges future research in this area would be valuable
.
Given
the chosen theoretical framework and nature of the research, a combined qualitative and
quantitative research methodology was employed
Qualitative Methodology
The qualitative approach was deemed appropriate in order to study leadership in action whilst Nurse
Managers interacted with their staff during a formal unit based meeting.
Observation
Observational technique formed the core basis of the qualitative method employed. Overt observation was
carried out as a means to assess the degree to which Nurse Managers employed emotional intelligence
skills whilst facilitating a leadership activity (unit staff meeting). A structured tool (
Emotional
Intelligence Behavioural Competency Assessment - EIBCA)
was devised to capture those observed
behaviours of the Nurse Manager as observed during their facilitation of a unit staff meeting. Whilst Nurse
Managers were scored under each of the sub-scales of the EIBCA depending on their response, examples
of naturally occurring behaviour were provided in order to justify the ratings applied by the researcher
(official observer) and provide meaning to those behavioural responses witnessed.
Quantitative Methodology
Quantitative research was carried out as means to determine how clinical nursing staff rated their Nurse
Managers leadership style. Questionnaire based organizational surveys (Leadership Behaviour
Questionnaire- LBQ) were used to elicit superior and subordinate perception of their Nurse Managers’
leadership styles A total of five Nurse Managers were sampled based on the depth and purpose of the
research.
Data Collection
Surveys Nursing Co-Directors and Clinical Nurses
Data was collected from each of the Nurse Manager’s superiors (Nursing Co-Directors), and subordinates
(Clinical Nurses) in order to elicit their perception of the leadership style of their Nurse Manager.
Respondents were asked to rate their Nurse Manager’s display of transformational leader behaviour in
regards to the four components, which make up this construct, through a self-administered questionnaire.
The Leadership Behaviour Questionnaire (LBQ)
measured the components of transformational
leadership, which include; intellectual stimulation, individualized consideration, inspirational motivation,
and idealized influence. The items of each scale required the rater to determine the degree to which each
Nurse Manager demonstrated leadership behaviours relevant to that scale by selecting responses on a
five-point likert scale ranging from 1= rarely or never, to 5= very frequently, if not always. The
Leadership
Behaviour Questionnaire (LBQ)
measurement tool was developed following a content analysis of the
literature on transformational leadership and review of The Multifactor Leadership Questionnaire (MLQ).
Other studies that have used the MLQ tool identified scale reliabilities as being high (Den Hartog et al
1997). Whilst the MLQ measures 37 items under the four components of transformational leadership, the
modified LBQ used in this study was reduced to 21 items.
Surveys Nurse Managers
The majority of emotional intelligence components were measured through observation, given that
self-management, social awareness, and relationship management are competencies that are behaviourally
anchored. However, self-awareness, which centres more on an individual’s internal state, was examined
by introspection in the form of a survey. The measurement tool titled
, Emotional Intelligence
Self-Awareness Questionnaire (EISAQ),
required Nurse Managers to indicate their level of agreement by
selecting responses on a five-point likert scale, from a suite of responses ranging from 1= Disagree
Strongly, to 5= Agree Strongly.
Competency Based Observation
A competency based approach to explore and measure emotional intelligence in the context of leadership
was selected. An observational method was chosen to capture an aspect of leadership in action and more
specifically to determine the degree to which each Nurse Manager displayed facets of emotional
intelligence during a team leader activity. The
Emotional Intelligence Behavioural Competency
Assessment (EIBCA)
was developed based on Goleman, Boyatzis and McKee’s (2002) Emotional
Intelligence Model (See Figure 2). The Emotional Intelligence Model has been refined from the original
five-dimension model created earlier by Goleman, with the result of ‘…an emotional intelligence model
that more clearly links specific clusters of competencies to the underlying brain dynamics that drive them’
(reference p 38). The authors believe that emotional competencies are built on the foundations of
emotional intelligence and that emotional competencies in turn form the cornerstone for effective
leadership. The EIBCA reflects 15 competencies as opposed to the 20 competencies of the ECI given that
self-awareness was not measured within this tool but assessed under a different framework of self-report
by participants.
Cronbach’s Alpha Co-efficient
For each of the three instruments used (Emotional Intelligence Self-Awareness Questionnaire -
EISAQ
,
Leadership Behaviour Questionnaire -
LBQ
and the Emotional Intelligence Behavioural Competency
Assessment –
EIBCA
) a Cronbach’s alpha co-efficient analysis was applied with the results confirming
that these survey instruments provided a good measure of the underlying constructs (Table 1).
The scales for each measurement tool used in this study have been itemized, with the number of
items being controlled to reduce fatigue and response pattern bias, but sufficient enough to
increase the validity and reliability of the measures. The choice of responses given to each item
has sufficient variance with measures giving choices of responses from one to five (1-5).Whilst
the decision not to utilize scientifically tested tools arose from funding constraints, the researcher
does acknowledge using a highly abbreviated form of other tools strictly for the purpose of this
research activity.
DATA ANALYSIS
Leadership Behaviour
Leadership Behaviour questionnaires completed by the Nurse Managers superior and subordinates were
analysed using SPSS version 11.0.
Multivariate Analysis Of Variance (MANOVA)
was used to perform
an analysis on several dependent variables simultaneously. As a follow-up an ANOVA was conducted to
determine whether there were any significant differences between the five Nurse Managers in relation to
the four components of transformational leadership. Subsequent
t-testing further explored the nature of
difference between each of the five Nurse Managers in terms of the four leadership styles, and thus
improved the quality of results.
Emotional Intelligence Self-Awareness
Analysis of the EISAQ was carried out by a scoring system. This self-report tool consisted of three scales
with various items listed (10 in total) under each of these categories, which were then rated on a five-point
Likert scale by participants. Scores were based on responses from the Likert scale ranging from 1= rarely
or never, to 5= very frequently, if not always.
Emotional Intelligence Behavioural Competency Assessment
The EIBCA rating was achieved by placing a numerical value under each of the items (behavioural
indicators) under the three components of emotional intelligence observed (self-management, social
awareness and relationship management) that indicated the degree to which the Nurse Manager displayed
that behaviour where appropriate. In instances where the behaviour was not applicable during the staff
meeting this was factored into the rating summary by subtracting the potential value from the overall
possible scores. The numerical values applied were: Displayed = 2; Partially Displayed =1; and Not
Displayed = 0.
Total Emotional Intelligence Score
Scores for total emotional intelligence (self-awareness, self-management, social awareness and
relationship management) were then achieved by averaging the total percentage for all four components of
emotional intelligence with a corresponding classification level of high, moderate or low total EI rating.
RESULTS
Nurse Manager Perception of Self-Awareness (Table 2)
Results arising from responses received by Nurse Managers following completion of a self-administered
questionnaire relating to the self-awareness component of emotional intelligence are outlined in Table 2.
Based on the total emotional intelligence score for self-awareness each participant rated themself as high
in emotional intelligence self-awareness. That is, they assessed their emotional intelligence within a range
from 80% for the highest assessment to 68% for the lowest self-assessment.
EI self-awareness was explored by eliciting the Nurse Manager’s perception of his/her ability to recognize
thoughts, feelings and moods. Given that this study was set in a highly visible social environment, the
need for the Nurse Manager’s awareness and expression of emotion and its subsequent effect on people is
of considerable significance in the context of their leadership role. Emotional self-awareness has been
described as the stepping-stone along the path to other EI competencies such as self-management, social
awareness and relationship-management. As Gardner and Stough (2002) strongly suggest, before a person
can grow and develop in the areas of self-management, social awareness and relationship-management
they have to first understand themselves and how they are perceived by others.
In the area of EI self-awareness a correlation was made with scores from the other components of
emotional intelligence relating to self-management, social awareness and relationship-management in all
Nurse Managers with the exception of participant number five. The Nurse Manager in question rated
themself as high in self-awareness (76%) but achieved a moderate rating from the EI behavioural
competency assessment (58%). One possible explanation for this may be that the Nurse Manager may
have an over-inflated view of themself or may not be aware of how they come across to others. Goleman
(1998c) draws on the differences between leaders who can realistically assess themselves with those who
are not so skilled in this area by stating ‘…while the arrogant, tuned-out leader protects him or herself
with blind spots, effective leaders know their strengths,
their limits, and their weaknesses’ (p 22
). The
same Nurse Manager also received the lowest results in terms of how staff rated their transformational
leadership
style (59%). These comparisons strengthen the argument that until a person can recognise their
feelings and thoughts and when and why they occur, they cannot exert control over their emotions so that
their behaviour has a positive influence and impact on others.
The other four participants who achieved a positive correlation between their EI self-awareness rating and
the competency assessment scores demonstrated greater psychological insight and self-concept which
indicates they were more in tune with how their display of emotion impacts on others. As Fuimano (2004)
states ‘…people who are emotionally intelligent make self-awareness a priority. They’re not afraid of their
feelings, but learn to use them as a barometer or an inner guidance system’ (p 10). In addition to a positive
match with all four EI components for participants one to four, this group also achieved a higher rating
from their clinical staff regarding their transformational leadership style as opposed to participant number
five.
Leading on from the notion that individuals who are more aware of their emotions and their impact on
others enhance their ability to manage others, such a skill may lead to exertion of greater influence over
teams due to the very nature of their emotional stature. Ashkanasy and Daus (2002) describe the effect
that one person’s emotion can have on another as infectious, stating ‘…people “catch’ or are ‘infected’ by
emotion from others, a result that has come to be known as emotional contagion’ (p 79). Of the five Nurse
Managers observed, two had this emotionally contagious effect on their followers. Whilst observing one
participant, the mood of the meeting was very serious with the Nurse Manager communicated information
at a rapid pace and staff tentatively listened with little opportunity for comment. When the Nurse Manager
suddenly made an amusing comment the atmosphere suddenly changed and the majority of the group
swiftly took on a mirror image of the Nurse Manager’s happy state. Similarly, the other participant was
directing the meeting in a very serious and formal fashion with the same tone being adopted by staff, but
when the Nurse Manager became more relaxed and actively invited input from the group, staff began to
freely engage in conversation. This observation supports Goleman’s (1998b) belief that people mirror the
behaviour of their leader, for example, if the leader displays calmness then followers are more likely to
adopt the same approach.
Emotional Intelligence Competencies at Work
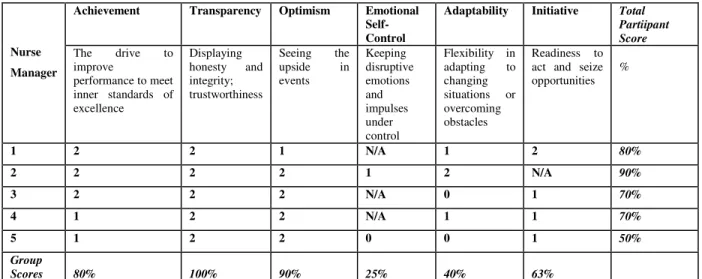
Self-Management (Table 3)
When observing EI competencies relating to self-management (Table 3), partial scores obtained for
achievement in two participants resulted from a demonstrated lack of conviction when addressing certain
standards of practice in order to meet excellence. A partial display of adaptability related to one
participant informing staff of a new assessment process soon to be introduced within the organization but
the Nurse Manager did not discuss the rationale behind the new tool or when and how it was to be
implemented. Another participant did not encourage change in practice regarding the assessment and
management of patient falls. Interestingly, of the two Nurse Managers who were confronted with
situations that warranted control of emotion, only one was partially able to demonstrate a sense of
emotional control over the situation (participant number two) whilst the other (participant number five)
scored a zero rating in relation to this skill. The zero rating from participant number five was a
consequence of their inability to manage the frustration and anxiety of their staff. The Nurse Manager
(number five) in this situation stated, in an abrupt tone to a staff member, “You are not letting me finish
what I was trying to say”. The atmosphere following this statement was subdued and staff did not
contribute further to the discussion. Bagshaw (2000) describes behaviour whereby the leader has a
negative impact on followers as emotionally unintelligent. Behaviours such as managers criticizing staff,
speaking to them in an undermining manner and threatening language falls well into this category.
Social Awareness (Table 4)
In relation to the empathy sub-scale of EI social awareness (Table 4), a low 40% group rating resulted
from a zero score from three of the five participants. Two of the three participants (numbers one and three)
had a tendency to rush through the meeting with little time to explore issues raised by staff, whilst
participant number five did not acknowledge staff comments on areas discussion areas at the meeting.
Participant number one also cut a staff member off whilst he was responding to a comment and interrupted
another staff member while they were in the middle of a sentence. In regards to acknowledging the
feelings of others, the low group percentile reflected the zero scores achieved by participants three and
five and a partial score from participant number one. For example, Participant number three, who scored a
zero rating, did not allow staff the opportunity to debrief over a critical incident that had occurred over the
weekend, especially when staff asked for reassurance on how they had managed the situation at the time.
The Nurse Manager casually stated that they had done the right thing but did not explore feelings of the
staff surrounding the event nor reinforce the strategies that were diligently employed by the staff during
managing the critical incident.
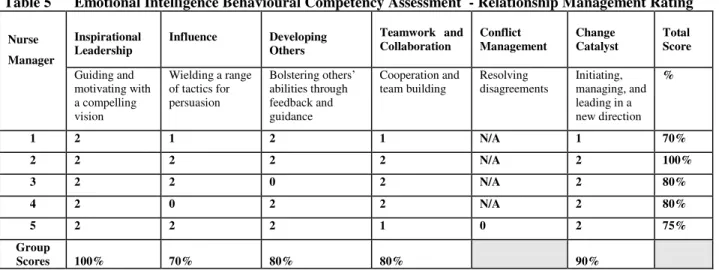
Relationship Management (Table 5)
With four of the five participants, the opportunity did not arise during the competency- based assessment
for these Nurse Managers to demonstrate how they would react in a conflict situation (Table 5). Nurse
Manager participant number five scored a zero rating as a consequence of their inability to successfully
resolve conflict in the staff meeting. The Nurse Manager appeared to become annoyed with staff as they
vented their feelings and viewed their reaction as a personal attack on her integrity rather than trying to
understand and articulate to the group how she perceived the staff to be feeling in regards to this issue.
The Nurse Manager may have achieved a more satisfactory outcome if she were able to feed back to the
staff how she perceived the group to be feeling. This acknowledgement would have then served as a basis
for team problem solving rather than the resultant team conflict. As Sy and Cote (2004) state
‘…emotionally intelligent individuals can repair unpleasant emotions and enhance pleasant emotions
when doing so is appropriate by employing strategies that alter these emotions’ (p 449). Other areas that
scored a partial rating related to the sub-scale of change catalyst, which resulted from the manner in which
participant number one responded to a staff member’s enquiry of progress regarding recruitment of a new
Nurse Manager to the unit. The Nurse Manager responded by stating “I’m not allowed to comment as they
don’t want me to discuss it with you”. In the area of teamwork and collaboration, partial ratings resulted
from participant number one asking the group a question then not allowing them to respond but rather
proceeding to answering her own question.
Overview of EI Behavioural Competency Scores (Table 6)
Four of the five participants achieved a high total EI competency score (Table 6). Nurse Manager five
achieved a moderate rating as compared to the other four participants. A marked discrepancy was noted
between one participant’s rating of self-awareness which was high at 76% and the score obtained from
observation of their other EI competencies such as self-management, social awareness and
relationship-management which resulted in a 58% combined skill demonstration in these areas.
Total Emotional Intelligence Score (Table 7)
All participants achieved a high total emotional intelligence score (Table 7), as a result of averaging
percentile scores in the areas of self-awareness, self-management, social awareness and
relationship-management.
Transformational Leadership - Supervisor and Subordinate Perceptions (Table 8)
Four of the five participants were rated by their superior and subordinates as demonstrating positive
transformational leadership behaviour (80.3% to 91.4%) with participant number five scoring only a
moderate rating in this area of 58.9% (See Table 8).
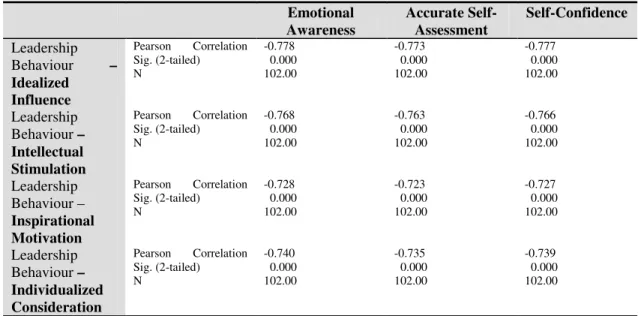
Relationship between Transformational Leadership and Emotional Intelligence (Table 9)
To assess whether Nurse Managers who exhibit high levels of emotional intelligence, demonstrate greater
transformational leadership behaviours as opposed to Nurse Managers who exhibit low levels of
emotional intelligence, a correlation analysis was undertaken of the 102 superior/subordinate assessments
of the five Nurse Managers in terms of their leadership style and their emotional awareness, accurate self
assessment and self confidence (Table 9).
The correlation analysis indicated that the three elements of emotional self-awareness strongly and
positively correlate with each other and whilst the other components of emotional intelligence
(self-management, social awareness and relationship management) are not as correlated they are still
represented as very strong (See Table 9).
Results indicate support of the predicted relationship between emotional intelligence and transformational
leadership (Table 10). A strong positive relationship between these two constructs was found in three of
the five participants, and a negative correlation from the other two participants.
LIMITATIONS
Whilst the findings of this study reveal a connection between emotional intelligence and transformational
leadership in Nurse Managers, the researcher acknowledges a number of limitations arising from the study
and hence cautions interpretation and generalization of the findings. Firstly, the sample size of Nurse
Managers is relatively small with only five Nurse Managers having participated in the study. Secondly,
the tools to measure both the construct of emotional intelligence and transformational leader behaviour
have not been empirically tested for their reliably and validity but rather have been adapted from the work
of others. Furthermore, the emotional intelligence competency based assessment was limited to only one
leadership activity of the Nurse Manager, for example, facilitating a staff meeting. Observing participants
on only one occasion may not reflect their true EI skills. Performance and ultimate display of emotional
intelligence may be altered from the person’s natural state because of nervousness or anxiety as a result of
being “watched” by an unfamiliar person. Whilst results from this study suggest that there is a positive
relationship between high-level emotional intelligence and transformational leadership, more rigorous
evidence would evolve by utilising empirically validated tools to test both the constructs of emotional
intelligence and transformational leadership. Also, a part of the research methodology was based on
self-report measures, which limit the basis upon which conclusions can be drawn. Thirdly, the study sample
was limited to Nurse Managers within a healthcare setting and as such was not representative of the
broader leadership population. Despite the above-mentioned limitations, results of this study indicate the
need for further research in this area.
FUTURE RESEARCH
Results of this study substantiate further research into the relationship between emotional intelligence and
transformational leadership given the potential benefits to leadership theory and practice and ultimately,
organizational success. More rigorous methodology would enhance any further study in this area, in
particular, using a similar design of self-report and other rating and observation of emotional intelligence
competencies spanning more than one leadership activity. Observation of several leadership activities
would allow greater scope and more accurate assessment of a participant’s true EI skills. Repeated
exposure to the researcher and process may justify discrepancies where a skill was not initially observed
but then later employed consistently due to the participant becoming more relaxed with the researcher and
less nervous about the procedure. Larger samples at an executive level from several major metropolitan
health services would also provide more in-depth information to enable assertions to be more clearly
validated. If the relationship between emotional intelligence and transformational leadership could be
strengthened by more empirically valid research the benefits to organizations in the key areas of
leadership recruitment and training may unfold. Dulewicz and Higgs (2003) highlight the importance of
more research in this area in the belief that it ‘…should help to determine the way in which emotional
intelligence is translated into effective senior-level leadership behaviours and will provide guidance on the
development of future leaders (p 208). Researchers and academics alike need to market emotional
intelligence as a core leadership competency. But to do this we need more evidence on how it can make a
positive difference. Health professionals need to start talking about emotional intelligence in everyday
practice so that people know what it means and in turn become more aware of their display of emotion and
its impact on others.
REFERENCES
Ashkanasy NM & Daus CS (2002) Emotion in the Workplace: The new challenge for managers, Academy
of Management Executiv 16(1):76-86.
Bagshaw M (2000) Emotional intelligence – training people to be affective so that they can be effective,
Industrial and Commercial Training 32 (2):61-65.
Dulewicz V & Higgs M (2003) Leadership at the Top: The Need for Emotional Intelligence in
Organizations, The International Journal of Organizational Analysis 11(3):193-210.
Fuimano J (2004) Raise your emotional intelligence, Nursing Management 35(7):10-12.
Gardner L & Stough C (2002) Examining the relationship between leadership and emotional intelligence
in senior level managers, Leadership & Organizational Development Journal 23(2):68-78.
George J (2000) Emotions and leadership: The role of emotional intelligence,
Human Relations 53(8):
1027-1055.
Goleman D (1998b) What Makes a Leader, Harvard Business Review November-December:93-102.
Goleman D (1998c) The Emotional Intelligence of Leaders, Leader to Leader Fall:20-26.
Goleman D, Boyatzis R & McKee A (2002) The New Leaders – Transforming the Art of leadership into
the Science of Results, 1
stedn, Little Brown, London.
Leban W & Zulauf C (2004) Linking emotional intelligence abilities and transformational leadership
styles, The Leadership & Organization Development Journal 25(7):554-564.
Pillai R & Williams EA (2004) Transformational leadership, self-efficacy, group cohesiveness,
commitment, and performance, Journal of Organizational Change Management 17 (2):144-159.
Prati LM, Douglas C, Ferris GR, Ammeter AP & Buckley MR (2003) Emotional Intelligence, Leadership
Effectiveness, and Team Outcomes, The International Journal of Organizational Analysis 11(1):21-40.
Sosik JJ & Dworakivsky AC (1998) Self-Concept Based Aspects of the Charismatic Leader: More Than
Meets the Eye, Leadership Quarterly 9(4) Winter:503-524.
Sy T & Cote S (2004) Emotional Intelligence: A key ability to succeed in the matrix organization, Journal
of Management Development 23(5):437-455.
Vance C & Larson E (2002) Leadership Research in Business and Health Care,
Journal of Nursing
Scholarship, Second Quarter:165-171.
Table 1 Cronbach’s Alpha Co-efficient
Instruments Alpha
ESAQ 0.9922
LBQ 0.9908
EIBCA 0.9913
Table 2 Emotional Intelligence - Self-Awareness Rating Score EI Score
Nurse
Manager High 66-100% Moderate 34-65% Low 0-33%
1 80%
2 78%
3 68%
4 86%
5 76%
Table 3 Emotional Intelligence Behavioural Competency Assessment - Self-Management Rating
Achievement Transparency Optimism Emotional
Self-Control
Adaptability Initiative Total
Partiipant Score Nurse Manager The drive to improve performance to meet inner standards of excellence Displaying honesty and integrity; trustworthiness Seeing the upside in events Keeping disruptive emotions and impulses under control Flexibility in adapting to changing situations or overcoming obstacles Readiness to act and seize opportunities % 1 2 2 1 N/A 1 2 80% 2 2 2 2 1 2 N/A 90% 3 2 2 2 N/A 0 1 70% 4 1 2 2 N/A 1 1 70% 5 1 2 2 0 0 1 50% Group Scores 80% 100% 90% 25% 40% 63%
Table 4 Emotional Intelligence Behavioural Competency Assessment - Social Awareness Rating
Empathy Organisational
Awareness Service Total Score
Nurse Manager
Listens to the views of others and communicates a genuine interest in concerns raised by staff
Acknowledges the feelings of others
Reading the currents, decision networks, and politics at the organizational level
Recognizing and meeting follower, client,
or customer needs % 1 0 1 1 2 50% 2 2 2 2 2 100% 3 0 0 2 2 50% 4 2 2 2 2 100% 5 0 0 2 2 50% Group Scores 40% 50% 90% 100%
Table 5 Emotional Intelligence Behavioural Competency Assessment - Relationship Management Rating Inspirational Leadership Influence Developing Others Teamwork and Collaboration Conflict Management Change Catalyst Total Score Nurse Manager Guiding and motivating with a compelling vision Wielding a range of tactics for persuasion Bolstering others’ abilities through feedback and guidance Cooperation and team building Resolving disagreements Initiating, managing, and leading in a new direction % 1 2 1 2 1 N/A 1 70% 2 2 2 2 2 N/A 2 100% 3 2 2 0 2 N/A 2 80% 4 2 0 2 2 N/A 2 80% 5 2 2 2 1 0 2 75% Group Scores 100% 70% 80% 80% 90%
Table 6 Emotional Intelligence Competencies
Emotional Intelligence Competencies Total EI Competency Score Nurse
Manager Self-Management Social Awareness Relationship Management High Moderate Low
1 80% 50% 70% 70%
2 90% 100% 100% 97%
3 70% 50% 80% 67%
4 70% 100% 80% 83%
5 50% 50% 75% 58%
Table 7 Total Emotional Intelligence Score (Self-rating and Behavioural Competency Assessments)
\
Table 8 Transformational Leadership Percentile Scores across the 5 Nurse Managers
Nurse Manager 1 2 3 4 5
LBQA Idealised Influence Processed 88.4% 87.8% 76.6% 88.2% 61.4%
LBQB Intellectual Stimulation Processed 88.4% 83.6% 82.2% 85% 59.2%
LBQC Inspirational Motivation Processed 92.6% 91.2% 82.2% 86% 57.%
LBQD Individualised Consideration Processed 87.4% 84.2% 80.2% 85.4% 58%
Total Transformational Leadership Scores 91.4% 86.7% 80.3% 86.2% 58.9%
Total EI Score
Self-Awareness, Self-Management, Social Awareness and Relationship Management
Participant
High 66-100% Moderate 34-65% Low 0-33%
1 75%
2 87.5%
3 67.5%
4 84.5%
Table 9 Self-Awareness Correlations Emotional Awareness Accurate Self-Assessment Self-Confidence Leadership Behaviour – Idealized Influence Pearson Correlation Sig. (2-tailed) N -0.778 0.000 102.00 -0.773 0.000 102.00 -0.777 0.000 102.00 Leadership Behaviour – Intellectual Stimulation Pearson Correlation Sig. (2-tailed) N -0.768 0.000 102.00 -0.763 0.000 102.00 -0.766 0.000 102.00 Leadership Behaviour – Inspirational Motivation Pearson Correlation Sig. (2-tailed) N -0.728 0.000 102.00 -0.723 0.000 102.00 -0.727 0.000 102.00 Leadership Behaviour – Individualized Consideration Pearson Correlation Sig. (2-tailed) N -0.740 0.000 102.00 -0.735 0.000 102.00 -0.739 0.000 102.00
Table 10 Comparison between Transformational Leadership and Emotional Intelligence Scores Transformational
Leadership Scores
Emotional Intelligence Scores Nurse
Manager Self-rating Competency Assessment Total EI Score
1 89% 80% 70% 75%
2 87% 78% 97% 88%
3 81% 68% 67% 68%
4 86% 86% 83% 85%