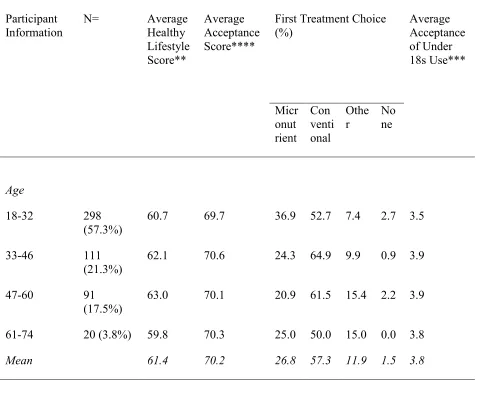
Acceptance Toward the use of Micronutrients as an Alternative Treatment for Mood Disorders
Full text
Figure
Related documents
When infant mortality declines there is a change in the epidemiologic pattern; namely, some groups of causes turn less important while some others become the leading causes of
VTT has been actively conducting R&D on gasification technologies for biomass and waste since the early 1980s. Working together with a Finnish SME, VTT developed a
William Catholic Church is a Eucharistic community; Glorifying God through prayer, sacraments and service; Creating oneness with God and neighbor;.. By generously sharing our
For example, Kaluszka (2005) uses the TVaR as a premium principle and Cai and Tan (2007) calculate the optimal retention for a stop loss reinsurance by considering the VaR and
Staggering types of treatment appointments versus scheduling the same type of appointment repeatedly will keep the dental team and their schedule flowing smoothly.. The
Step 4 CEMS Audit Performance Test: Using the same calibration equation derived for the initial calibration and Post-Calibration Performance Test, the CEMS Audit
• Each clinic visit information HEI Register • Cohorts by birth month • Summarizes clinical information by month, up to 18 months HEI Cohort Analysis (HCA) Tool • 9 and 18
Preface.. In February 2003, the National Research Council, in its Final Report “Diagnosis and Control of Johne’s Disease,” recommended that veterinarians be supplied with materials
