Development of Total Quality Management framework for
Libyan health care organisations
ABDELMOTLEB, Fakhureldein Abdusalam
Available from Sheffield Hallam University Research Archive (SHURA) at:
http://shura.shu.ac.uk/17146/
This document is the author deposited version. You are advised to consult the
publisher's version if you wish to cite from it.
Published version
ABDELMOTLEB, Fakhureldein Abdusalam (2008). Development of Total Quality
Management framework for Libyan health care organisations. Doctoral, Sheffield
Hallam University.
Copyright and re-use policy
See
http://shura.shu.ac.uk/information.html
S h e fflffd H a lla m U n iv e rs ity t < n g a n d IT S e rv ic e s A d s * n C e n tre C ity C a m p u s _ d S 1 1 W B
T W
1 0 1 9 0 6 2 7 0 3
S h e ffie ld H a lla m U n iv e rs ity L e a rn in g a n d IT S e rv ic e s A d s e tts C e n tre C ity C a m p u s
S h e ffie ld S I 1 W 8
D e v e l o p m e n t o f a T o t a l Q u a l i t y M a n a g e m e n t F r a m e w o r k f o r L i b y a n H e a l t h C a r e o r g a n i s a t i o n s
F a k h u r e l d e i n A b d u s a l a m A b d e l m o t l e b
A t h e s i s s u b m i t t e d i n p a r t i a l f u l f i l m e n t o f t h e r e q u i r e m e n t s o f S h e f f i e l d H a l l a m U n i v e r s i t y
f o r t h e d e g r e e o f D o c t o r o f P h i l o s o p h y
A c k n o w le d g e m e n ts
F irst and forem ost, m y thanks and gratitude go to G od for providing m e w ith the m eans
and perseverance to com plete this research. W ithout his help, none o f this or any other
accom plishm ent w ould have been possible.
I w ould also like to express m y sincere appreciation to P rof. S am eh S aad for guidance and
continual support. Y our guidance, support, and good nature w ere invaluable.
S pecial thanks go to m y w ife. W ithout her lim itless assistance and encouragem ent, this
thesis w ould not have been com pleted.
I w ould like also to thank m y m other; m y father, m y sisters and m y brothers, for their love,
support and for creating an environm ent that alw ays encouraged m e to learn.
T his thesis is dedicated to m y parents, m y w ife and m y children, your support w as an
N o m e n c la tu r e
T Q M : T otal Q uality M anagem ent
Q F D : Q uality F unction D eploym ent
JIT : Just In T im e
P D C A : P lan, D o, C heck and A ct
IS O : International O rganization for S tandardisation
W W H : S econd W orld W ar
M B N Q A : M alcolm B aldrige N ational Q uality A w ard
E Q A : E uropean Q uality A w ard
JQ A : Japan Q uality A w ard
S Q A : S ingapore Q uality A w ard
A H P : A nalytic H ierarchy P rocess
IR : Inconsistency R atio
S P SS : S tatistical P ackage for S ocial S ciences
A N O V A : A nalysis o f V ariance
L I: V ision
L 2: M ission
L 3: S trategy
L 4: C om m unication
L 5: E m pow erm ent
L 6: T rust
L 7: T eam developm ent
L E : L eadership E xcellence
L : L eadership
F C : F ocus on C ustom er
P M : P rocess and m easurem ent
C I: C ontinuous im provem ent
Q ID W : Q uality in D aily W ork
Q P : Q uality P lanning
Q C : Q uality C ontrol
Q I: Q uality Im provem ent
A P : A daptation and preparation
Q C *: Q uality C ircle
Q C T : Q uality C ircles T eam
IP C Q S : Identify the problem in the current quality system
C F : S elect the factors to be evaluated
M Q : M easuring the quality service
S A : S ensitivity analysis
P C D A : P lan-D o-C heck-A ct stage
A b str a c t
P rim ary h ealth care is th e first stag e fo r th e n ation al h ealth . A s su ch it is co n sid ered as th e first
stag e o f co m m u n icatio n b etw een th e citizen , fam ily an d th e so ciety . T h e m ain o b jectiv e fo r an y
p rim ary h ealth care is to m eet th e n eed o f th e in d iv id u al at h ig h q u ality , an d im p ro v e th e
p erfo rm an ce o f th e h ealth care sy stem . T h e q u ality h ere is w h at th e p atien t receiv es w ith reg ard to
ex cellen t an d safe m ed ical an d h ealth serv ices.
A cco rd ing to th e av ailab le literatu re an d b ased o n th e au th o r’s m an y v isits an d p relim in ary
in v estig atio n reg ard in g L ib y an h ealth care secto r in g en eral an d T rip o li h ealth care secto r in
p articu lar, itjja s b een p ro v en th at th e reality o f g o v ern m en t h o sp itals in L ib y a is th at: th ese
h o sp itals are facin g m an y p ro b lem s o p p o sin g th eir im p ro v em en t, co n tin u ity an d ab ility to co m p ete.
B ased o n a series o f co m p reh en siv e q u estio n n aires, th e w eak n ess in th e cu rren t sy stem are
id en tified , an d also fo u n d th at T o tal Q u ality M an ag em en t (T Q M ) w o u ld p ro v id e th e so lu tio n fo r
L ib y an H ealth care sy stem . T Q M is a w ay o f m an ag in g to im p ro v e th e effectiv en ess, efficien cy ,
flex ib ility , an d co m p etitiv en ess o f a b u sin ess as a w h o le. T h e literature illu strated th at th ere are
m an y m o d els an d fram ew o rk s in th e field o f T Q M . H o w ev er, th e q u ality g u ru s have never agreed
about a specific fiam ew ork o r im plem entation procedure. In ad d itio n , th ere is lack o f a g en eral m o d el in
h ealth care, an d th ere is n o clear ag reem en t as to th e w ay in w h ich T Q M sh o u ld b e im p lem en ted in
a h ealth care secto r. T herefore, th e fo cu s o f th is stu dy is to id en tify an ap p ro p riate T Q M fram ew o rk
fo r L ib y an Jiealth care, o rg an isatio n s an d b en ch m ark in g th em an d d istin g u ish th eir co m p etitiv e
ad v an tag e, in o rd er to ach iev e p erform an ce ex cellen ce.
A co m p reh en siv e literatu re rev iew related to T Q M is carried o u t to h av e a clear in sig h t in to th e
T Q M an d its ap p licatio n in h ealth serv ice, ^ q u estio nn aire su rv ey m eth o d is ad o p ted to g ath er th e
d ata an d in fo rm atio n , w h ich fo rm th e b asis fo r th e d ev elo p m en t o f th e p ro p o sed T Q M fram ew o rk .
S tatistical P ack ag e fo r th e S o cial S cien ces S P S S an d A n aly tical H ierarch y P ro cess A H P are
u tilised to an aly se th e co llected d ata an d v iew s fro m m an ag ers. an d em p lo y ees in th e o rg an isatio n s
u n d er in v estig atio n . In ad d itio n , in o rd er to ach iev e th e aim o f th is stu d y tw o m o d els are d ev elo p ed
an d T Q M fram ew o rk th at co v ers m o st asp ects o f T Q M startin g fro m to p m an ag em en t aw aren ess
u n til ev en p ro m o tin g co n tin u ou s im p ro v em en t is d ev elo p ed .
T h e v erificatio n an d v alid atio n p ro cess o f th e p ro p o sed T Q M fram ew o rk an d its im plem en tatio n
stag e im p lied th at th e p ro p o sed fram ew o rk facto rs an d stag es are im p ortan t fo r im p ro v in g th e
P u b lic a tio n s fr o m th e th e sis
S aad, S. M . and A bdelm otleb, F . A ., 2008, E valuation o f the leadership perform ance in
total quality m anagem ent. T he 18th International C onference on F lexible A utom ation and
Intelligent M anufacturing (F A IM 2008). 30 June - 2 July 2008, S kovde, S w eden.
S aad, S. M . and A bdelm otleb, F. A ., 2008, P erform ance E xcellence in H ealthcare
O rganisations. T he 18th International C onference on F lexible A utom ation and Intelligent
T a b le o f c o n te n ts
A cknow ledgem ents... i
N om enclature... ii
A bstract... ... iv
P ublications from the thesis...v
T able o f contents... vi
A ppendixes... ... xiv
L ist o f tables... xiv
L ist o f figures... ... ...xviii
C h a p te r o n e: In tr o d u c tio n 1.1. Introduction ... 2
1.2. A im s and objectives... 4
1.3. P roblem B ackground... 5
1.4. O verview o f the T hesis... :... 5
C h a p te r tw o : S tu d y in g a n d a n aly sin g th e c u r r e n t sta tu s 2.1. Introduction... ... ... ...11
2.2. O verview o f L ibyan H ealthcare... ...12
2.3. T he L ibyan policy in the field o f prim ary healthcare... ...14
2.3.1. T he policy o f healthcare sector ... 14
2.3.2. D ifficulties o f healthcare sector... ... 16
C h ap te r th ree:
U n d er sta n d in g T o ta l Q u a lity M a n a g em e n t
3.1. Introduction... ...19
3.2. T he concepts and definitions o f Q uality and T Q M ... ... 3.3. T Q M in H ospitals and H ealthcare... 24
3.4. C om parison betw een the traditional and m odern quality concepts... 27
3.5. T he im portance o f T Q M ... ... ...28
3.6. E vo lution o f T Q M ... 29
3.7. Q uality G urus... 31
3.7.1. E dw ard D em ing... 31
3.7.1.1. T he D em ing W heel (P D C A )... 33
3.7.2. Juran Joseph ... ,... ... ...34
3.7.3. P hilip C rosby... ...35
3:7.4. K aoru Ishikaw a... ... ... ... 35
3.8. S um m ary...:... ... 36
C h a p te r fo u r: T o ta l Q u a lity M a n a g e m e n t a n d its R e q u ir e m e n ts 4.1. Introduction... ... 38
4.2. F actors o f T Q M ...<... 38
4.2.1. L eadership ... 39
4.2.2. T raining and E ducation ... :...40
4.2.3. F ocus on custom er... 41
4.2.4. P rocess and m easurem ent... 41
4.2.5. C ontinuous im provem ent... 42
4.5. M odels o f T Q M ... ... ... 46
4.6. R equirem ents o f total quality m anagem ent im plem entation ... 49
4 .7 . T h e g a p s in th is a r e a ... ... 5 2 4.7. S um m ary... ... ... 54
C h a p te r five: R e se a r c h M e th o d o lo g y 5.1. Introduction... ... :... ;...57
5.2. U nderstanding research... 57
5.3. T ypes o f research ... ... ... ...57
5.3.1. P urpose o f the research ... ... ... ... ...59
5.3.1.1. E xploratory research... 59
5.3.1.2. D escriptive research... ... ...59
5.3.1.3. A nalytical research... ... ... ...59
5.3.1.4. P redictive research... ... ... ...59
5.3.2. P rocess o f the research ... ... 60
5.3.2.1. Q uantitative research and qualitative research... ...60
5.3.3. L ogic o f the research... :... 60
5.3.3.1. D eductive research and inductive research... ... 60
5.3.4. O utcom e o f the research ... ... ...61
5.3.4.1. A pplied research and B asic research... ...61
5.4. T he research M ethodologies... ... 66
5.5. T ypes o f research m ethodology ... ... ...67
5.5.1. S election o f m ethodology in this research... 67
5.5.1.1. Q uantitative and qualitative case studies... 68
5.6.1. S tudy sam ple... ... 69
5.6.2. D ata collection... 70
5.6.2.1. S econdary data... ■ ... 70
5.6.2.2. P rim ary data... ... ... ...71
5.6.2.2.1. Interview s... 71
5.6.2.2.1.1. F ocus-G roup Interview ... — .72
5.6.2.2.1.2. F ace-to-face Interview ... 73
5 .6 .2 .2 .1.3. P ilot study... 73
5.6.2.2.2. Q uestionnaire survey... ... 76
5.7. D ata analysis... ... 81
5.8. S um m ary... ... ... ...83
C h a p te r six : E v a lu a tio n o f th e le a d e r sh ip p e rfo rm a n ce in to ta l q u a lity m a n a g e m en t 6.1. Intro duction... ... '... ... 86
6.2. L eadership E xcellence o f S uccessful C hange... ... 86
6.3. T he proposed leadership perform ance m odel in (T Q M )... ... 87
6.3.1. C ulture change... ... 89
6.3.1.1. C om parison betw een m odem and traditional culture... ...91
6.3.1.2. R equirem ents o f changing the organisational culture... 92
6.3.2. L eadership factors... — .93
6.3.2.1. V ision... .93
6.3.2.2. M ission... 94
6.3.2.3. S trategy... 94
. 6.3.2.4. C om m unication... ... 94
6 3 .2 .6 . T rust... ... ... 95
6 3 .2 .7 . T eam developm ent... 95
6.4. R esearch M ethodology... ... 96
6.5. S election o f sam ple... 96
6.6. D ata C ollection... ...98'
6.7. D ata preparation for analysis purposes... 98
6.8. C haracteristics o f the research sam ple... ... ,... 99
6.8.1. T he gender... 99
6.8.2. T he age groups... 100
6.8.3. Q ualifications... ...102
6.8.4. M anagem ent L evel... ... 103
6.8.5. T ripoli H ealthcare O rganisations und er investigation...104
6.9. D escriptive S tatistics...106
6.10. A nalysis o f V ariance (A N O V A )... ... 107
6.11. C orrelation A nalysis... 110
6.12. R eliability A nalysis... ...;... :... 113
6.13. E valuation o f L eadership in T ripoli H ealthcare O rganisations... ...115
6.14. T he results and discussion... ... ....1 2 0 6.15. S um m ary... ...123
C h a p te r sev en : P e rfo r m a n c e E x c e lle n c e in H e a lth ca r e O r g a n isa tio n s 7.1. Introduction... 127
7.2. P erform ance E xcellence...128
7 3 . B enchm arking... ... ... •... 130
7.4.1. A nalytical H ierarchy P rocess (A H P)... ... ... 132
7.4.2. Justification for using A H P ... ... 135
7.5. T he proposed perform ance excellence m odel...137
7.5.1. S tructuring a hierarchy m odel for perform ance excellence ... 137
7.5.2. Im plem entation o f a hierarchy m odel o f T ripoli healthcare sector... 138
7.5.3. R esu lts and discussion... 141
7.6. S ensitivity A nalysis... ... ... 150
7.7. S um m ary... ... ...157
C h a p te r eig h t: F ra m e w o rk fo r th e im p le m e n ta tio n o f T Q M 8.1. Introduction... ... ... 159
8.2. O verview the organisational structure o f T ripoli healthcare secto r... ... 160
8.3. F ram ew ork for the im plem entation o f T Q M ... 163
8.4. T he stages o f the proposed T Q M ... ... 168
8.4.1. Q uality P lanning (Q P )... ....16 8 8.4.1.1. A daptation and preparation... 168
8.4.1.2. Q uality C ircle... 170
8.4.1.2.1. Q uality C ircles T eam in health sector... .174
8.4.1.3. Identify the problem in the current quality system ... ...176
8.4.1.4. S elect the factors to be evaluated... ... 176
8.4.2. Q uality C ontrol... 177
8.4.2.1. M easuring the quality service... 177
8.4.2.2. S ensitivity analysis... 178
8.4.4. Q uality Im provem ent... 179
8.4.4.1.1. T he planning stage... 179
8.4.4.1.2. T he do stage... ....1 8 0 8.4.4.1.3. T he check stage... ... ...181
8.4.4.1.4. T he action stage... ... 183
8.4.4.1 .5. C ontinuous im provem ent... 184
8.5. S um m ary ... 185
C h a p te r n in e: V e r ific a tio n I v a lid a tio n th e p r o p o se d T Q M fr a m e w o r k 9.1. Introduction... 188
9.2. D esign o f the proposed questionnaire... 188
9.3. S election o f sam ple... 189
9.3.1. P ilot stage... 189
9.3.2. D evelopm ent o f the final questionnaire... ... ... 189
9.4. D etails o f the proposed questionnaire... ..190
9.4.1. T he gender... ... *... ... 190
9.4.2. T he age groups... 191
9.4.3. Q ualifications... 193
9.4.4. M anagem ent L evel... 194
9.5.R esults, analysis and discussion... 196
9.5.1. R eliability A n aly sis... 196
9.5.1.1. R eliability A nalysis for the second section o f questionnaire... 196
9.5.1.2. R eliability A nalysis for the third section o f questionnaire... 199
9.5.1.3. R eliability A nalysis for the fourth section o f questionnaire... ... 202
9.5.2. S ection 2: D escriptive statistics o f the organisations situation ... 204
9.5.3.1. P riority w eights o f the proposed fram ew ork factors... 235
9.5.4.S ection 4 : D escriptive S tatistics o f the proposed fram ew ork stages... ....240
9.5.4.1. P riority w eights o f the proposed fram ew ork factors... 251
9.5.5. A nalysis o f V ariance (A N O V A ) o f the second section o f the questionnaire... 254
9.5.6. A nalysis o f V ariance (A N O V A ) o f the third section o f questionnaire... 259
9.5.7. A nalysis o f V ariance (A N O V A ) o f the fourth section o f the questionnaire... 260
9.5. S um m ary... 263
C h a p te r T en F in d in g s, C o n c lu sio n , lim ita tio n a n d r e co m m en d a tio n 10.1. Introduction... ... 265
10.2. T he m ain findings... ... ... ... 265
10.2.1. T he literature findings... ...265
10.2.2. T he survey findings... ... ... 266
10.2.2.1. T he first questionnaire findings... 266
10.2.2 .2. T he second questionnaire findings...268
10.2.2.3. T he third questionnaire findings... ... 271
10.2.2.3.1. P art I... :... ... 271
10.2.2.3.2. P art II... ... ... 272
10.2.2.3.2. P art m ... ... ... 272
10.3. C onclusion ... 273
10.4. T he R esearch L im itation... .:... ....;... 276
10.5. R esearch contributions... ... ... ... 276
10.6. R ecom m endation and F urther R esearch...,... ...278
A P P E N D IC E S
Q uestionnaires... 294
A ppendix O ne... ...294
A ppendix T w o... 298
A ppendix T hree... ... ... 316
L ist o f T a b les T able (3.1) C om parison betw een the traditional and m odem quality concept... ... 27
T able (3.2) Im portant events in the developm ent o f T Q M ... ... 29
T able (4.1) L ist o f quality factors and literature support... ... 45
T able (4.2) P rinciples and C ore concepts o f T Q M ... 47
T able (5.1) C lassification o f m ain types o f research... ...58
T able (5.2) F eatures o f the tw o m ain paradigm s... 67
T able (6.1) L ist o f leadership factors and literature support... 88
T able (6.2) C om parison betw een total quality m anagem ent and the traditional concept... ... ... ... 91
T able (6.3) R equirem ents o f changing the organisational culture... 93
T able (6.4) D istributed questionnaire and the response rate...97
T able (6.5a) D escriptive statistics for gender groups... ...99
T able (6.5b) T he gender grou ps o f respondents... 99
T able (6.6a) D escriptive statistics for age groups... ...101
T able (6.6b) T he age groups o f respondents... 101
T able (6.7a): D escriptive statistics for qualifications... 102
T able (6.7b) T he qualifications o f respondents... 102
T able (6.8a) D escriptive statistics for m anagem ent level... ...104
T able (6.8b) T he m anagem ent level o f respondents... 104
T able (6.9b): T ripoli H ealthcare O rganisations o f respondents...105
T able (6.10) D escriptive S tatistics o f L eadership factors... 106
T able (6.1 la) one-w ay A N O V A output D escriptive...108
T able (6.1 lb ) A N O V A output... ... ... 109
T able (6.12) O utput for the P earson C orrelation... ... 111
T able (6.13) Item S tatistics... 113
T able (6.14) Item -T otal S tatistics... 114
T able (6.15) S cale S tatistics... 114
T able (6.16) R eliability S tatistics... ,... ... 114
T able (6.17) E valuation o f L eadership in T ripoli H ealthcare O rganisations... 116
T able (6.18) M easuring (L E ) in T ripoli H ealthcare O rganisations... 117
T able (6.19) T he strengths and w eaknesses points o f leadership in T ripoli healthcare... 119
T able (7.1) Justification for using A H P w ith literature support... 135
T able (7.2) C om parison scale... 140
T able (7.3) P air-w ise com parison m atrix for T Q M factors... 141
T able (7.4) M ean respondents o f nine senior m anagers using M icrosoft E xcel...142
T able (7.5) priority details for decision hierarchy... ... 148
T able (8.1) com parison o f the A m erican quality gum s... 165
T able (8.2) Juran’s contributions expressed in his quality trilogy... ....166
T able (9.1a) D escriptive statistics for gender groups... ...190
T able (9.1b) T he gender groups o f respondents... ...190
T able (9.2a)D escriptive statistics for age groups... ...192
T able (9.2b) T he age groups o f respondents... 192
T able (9.3a) D escriptive statistics for qualifications... 193
T able (9.4a) D escriptive statistics for m anagem ent level... :... 195
T able (9.4b) T he m anagem ent level o f respondents... ... 195
T able (9.5) Item S tatistic... 196
T able (9.6) Item -T otal S tatistics... 197
T able (9.7) S cale S tatistics... 198
T able (9.8) R eliability S tatistics... ... ... 198
T able (9.9) Item S tatistics... ... 199
T able (9.10) Item -T otal S tatistics... ... ... ... ... 200
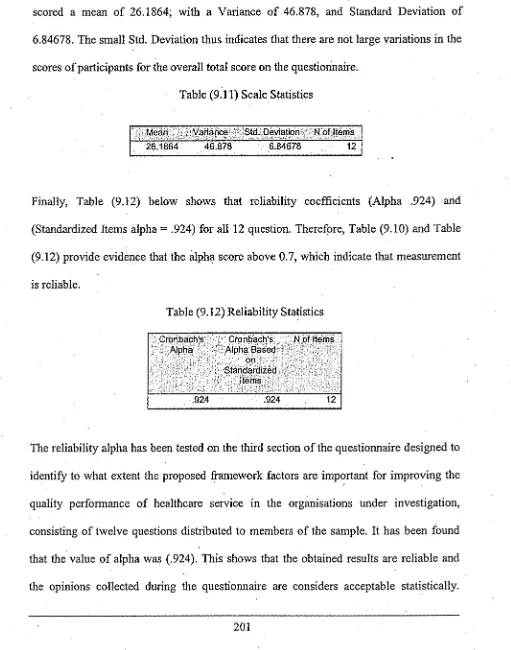
T able (9.11) S cale S tatistics.... ... ... 201
T able (9.12) R eliability S tatistics... ... 201
T able (9.13) Item S tatistics... 202
T able (9.14) Item -T otal S tatistics... 203
T able (9.15) S cale S tatistics... 203
T able (9.16) R eliability S tatistics... 204
T able (9.17) D escriptive S tatistics the organisations situation w ith regard to T Q M ... 205 .
T able (9.18) Q 1... ... ... ...205
T able (9.19) Q 2... 207
T able (9.20) Q 3... 208
T able (9.21) Q 4... ...210
T able (9.22) Q 5... ... 211
T able (9.23) Q 6... 212
T able (9.24) Q 7... ... :...213
T able (9.25) Q 8... ... ... 214
T able (9.26): Q 9... :... ... ’... 215
T able (9.28) Q ll... ,... ... 218
T able (9.29) Q 12... 219
T able (9.30) Q 13... ... ... ... '... 220
T able (9.31) D escriptive S tatistics o f proposed fram ew ork factors... ... 221
T able (9.32) V ision.... ... 222
T able (9.33) M ission... ,... ... 223
T able (9.34) S trategy... ... 224
T able (9.35) C om m unication ... ... ... 225
T able (9.36) E m pow erm ent... ... ... 226
T able (9.37) T rust... ... ... ... 227
T able (9.38) T eam developm ent...228
T able (9.39) L eadership ... 229
T able (9.40) T raining and E ducation... ... 230
T able (9.41) F ocus on C ustom er... :...232
T able (9.42) P rocesses and M easurem ent... 233
T able (9.43) C ontinuous Im provem ent... ... ...234
T able (9.44) R espondents opinion about the proposed fram ew ork facto rs... 236
T able (9.45) D escriptive S tatistics o f the proposed fram ew ork stages... ,... 240
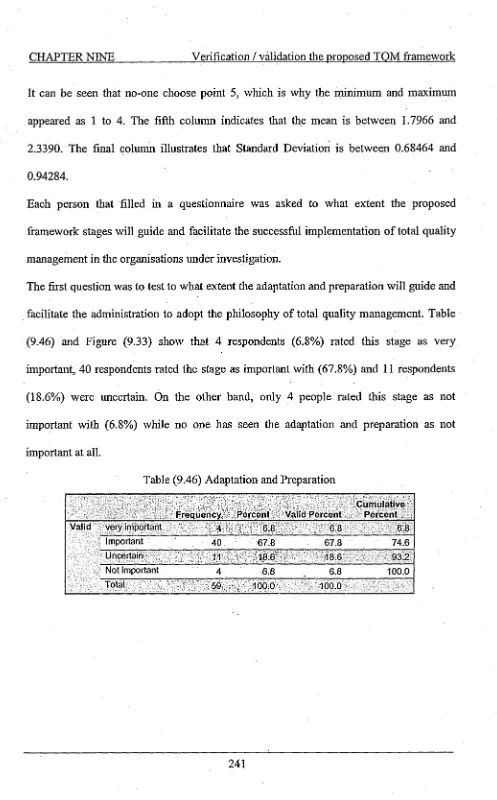
T able (9.46) A daptation and P reparation ... ...241
T able (9.47) Q uality C ircles T eam ... ...■ ...,.243
T able (9.48) Identify the problem in the current quality system ... 244
T able (9.49) S elect the factors to be evaluated... 245
T able (9.50) M easuring the quality service... 247
T able (9.51) sensitivity analysis... ... ... 248
T able (9.60) R espondents opinion about the proposed fram ew ork stages... 251
T able (9.61) A N O V A results... :... ...254
T able (9.62) M ultiple C om parisons... 255
T able (9.63) A N O V A results... 259
T able (9.64) A N O V A results... 261
T able (9.65) M ultiple C om parisons... ... :... 262
L ist o f F ig u r es F igure (3.1) T he D em ing W heel (P D C A )...33
F igure (4.1) C hin et al hierarchy m odel using the analytic hierarchy process (A H P )....48
F igure (5.1) T he research process... ... 65
F igure (5.2) T ypes o f qualitative interview s... 72
F igure (5.3) T ypes o f questionnaires... 78
F ig (6.1) T he proposed L eadership E xcellence M odel... ...89
F igure (6.2) T he response to the survey’s questionnaire ... ...98
F igure (6.3) P ie C hart show s the respondents gender groups...100
F igure (6.4) P ie C hart show s the respondents age groups... 101
F igure (6.5) P ie C hart show s the respondents qualifications... ...103
F igure (6.6) P ie C hart show s the respondents m anagem ent level... 104
F igure (6.7) P ie C hart show s the respondents T ripoli H ealthcare O rganisations... 106
F igure (6.8): L eadership E xcellence in L ibyan H ealthcare O rganisations... ..118
F igure (6.9): T he strengths and w eaknesses points o f leadership in T ripoli healthcare.. 119
F igure (7.1) T he proposed perform ance excellence A H P m odel o f T ripoli healthcare... 138
F igure (7.3) T he priority w eights o f the nine healthcare organisations w ith respect to
L eadership... ... ... 145
F igure (7.4) T he priority w eights o f the nine healthcare organisations w ith respect to
T raining and E ducation... ... 146
F igure (7.5) T he priority w eights o f the nine healthcare organisations w ith respect to
F ocus on C ustom er... ... ... 146
F igure (7.6) the priority w eights o f the nine healthcare organisations w ith respect to
P rocess and m easurem ent... ... 147
F igure (7.7) the priority w eights o f the nine healthcare organisations w ith respect to
C ontinuous im provem ent... 147
F igure (7.8) distributive sum m ary o f the evaluation results... ... ...148
F igure (7.9) perform ance sensitivity for perform ance excellence in T ripoli healthcare
organisations... -... 151
F igure (7.10) the dynam ic sensitivity for perform ance excellence in T ripoli healthcare
organisations (original situation)... ... ... 152
F igure (7.11) D ynam ic sen sitiv ity analysis - first situation... 155
F igure (7.12) D ynam ic sen sitiv ity analysis - second situation... 155
F igure (7.13) D ynam ic sen sitiv ity analysis - third situation... 156
F igure (7.14) D ynam ic sensitivity analysis - fourth situation... 156
F igu re (8.1) O rganisational structure o f T ripoli healthcare sector... 161
F igure (8.2) Q uality in D aily W ork (Q E D W )... ...167
F igure (8.3) T he proposed T Q M fram ew ork for L ibyan healthcare sector... 169
F igure (8.4) O rganisational structure o f T ripoli healthcare sector... 173
F igure (9.1) T he respondents gender groups... ...191
F igure (9.3) T he respondents qualifications... ... ... 194
F igure (9.4) T he respondents m anagem ent level... ... 195
F igure (9.5) T he respondent's agreem ent/disagreem ent o f Q l... 206
F igure (9.6) T he respondents agreem ent/disagreem ent o f Q 2... 207
F igure (9.7) T he respondents agreem ent/disagreem ent o f Q 3... ..209
F igure (9.8) T he respondents agreem ent/disagreem ent o f Q 4... ...210
F igure (9.9) T he respondents agreem ent/disagreem ent o f Q 5... 211
F igure (9.10) T he respondents agreem ent/disagreem ent o f Q 6... 212
F igure (9.11) T he respondents agreem ent/disagreem ent o f Q 7... .213
F igure (9.12) T he respondents agreem ent/disagreem ent o f Q 8... 214
F igure (9.13) T he respondents agreem ent/disagreem ent o f Q 9... 216
F igure (9.14) T he respondents agreem ent/disagreem ent o f Q 10... 217
F igure (9.15) T he respondents agreem ent/disagreem ent o f Q ll... 218
F igure (9.16) T he respondents agreem ent/disagreem ent o f Q 12... 219
F igure (9.17) T he respondents agreem ent/disagreem ent o f Q 13... 220
F igure (9.18) R espondents opinion about how im portant the “clear vision” as a factor for
im proving the q u ality... 222
F igure (9.19) R espondents opinion about m ission as an im portant factor... 223
F igure (9.20) R espondents opinion about strategy as an im portant factor... 224
F igure (9.21) R espondents opinion about com m unication as an im portant facto r...225
F igure (9.22) R espondents opinion about em pow erm ent as an im portant factor... 226
F igure (9.23) R espondents opinion about trust as an im portant factor... .227
F igure (9.24) R espondents opinion about team developm ent as an im portant factor.... 228
F igure (9.25) R espondents opinion about leadership as an im portant facto r... ... 229
F actor. .231
F igure (9.27) R espondents opinion about custom er focus as an im portant factor... 232
F igure (9.28) R espondents opinion about processes and m easurem ent as an im portant
facto r... ... ,... 233
F igure (9.29) R espondents opinion about continuous im provem ent as an im portant
F actor... ... ... ... ... 235
F igure (9.30) T op m anagem ent priority w eights o f the proposed fram ew ork factors.... 237
F igure (9.31) M iddle m anagem ent priority w eights o f the proposed fram ew ork factors.238
F igure (9.32) T he priority w eights o f the proposed fram ew ork factors... 239
F igure (9.33) R espondents opinion about adaptation and preparation stage... 242
F igure (9.34) R espondents opinion about Q uality C ircles T eam stag e... 243
F igure (9.35) R espondents opinion about identifying the problem in the current quality
system stage... ... ...244
F igure (9.36) R espondents opinion about select the factors to be evaluated stage... 246
F igure (9.37) R espondents opinion about m easuring the quality service stage ,... 247
F igure (9.38) R espondents opinion about sensitivity analysis stage... 248
F igure (9.39) R espondents opinion about P lan-D o-C heck-A ct (P D C A ) stag e... 250
F igure (9.40) T op m anagem ent priority w eights o f the proposed fram ew ork stages... 252
F igure (9.41) M iddle m anagem ent priority w eights o f the proposed fram ew ork stages.252
C H A P T E R O N E Introduction
C h a p te r o n e:
In tro d u ctio n
1 .1 . In tr o d u c tio n ... ,..«2
1 .2 . A im s a n d o b je c tiv e s... ... ...4
1 .3 . P ro b lem B a c k g r o u n d ... 5
1 .1 . In tro d u ctio n :
T otal Q uality M anagem ent (T Q M ) is a m anagem ent approach for an organisation centred
on quality, based on the participation o f all its m em bers and aim ed at m eeting custom er
expectations (S hort and R ahim , 1995). M oreover, im plem enting total quality program m e
requires positive, very visible and effective leadership from all levels o f m anagem ent
(K och, 1993). T here is now general recognition in L ibyan health care o f the need to have
in place form alized structures and program m es, w hich continually m onitor and evaluate
im provem ents. A ccording to E vans (2008) m anagers recognised that the "quality o f
m anagem ent" is as im portant as the "m anagem ent o f quality". H e also started
organisations to integrate the principles o f quality m anagem ent system ; the concept o f
total quality m anagem ent has becom e m ore popular. Q uality is the new m eaning o f the
organisation at the level o f perform ance excellence, rather than narrow or engineering
technical production based on discipline and perm eated every aspect o f running the
organisation.
T his research w ill focus on the changes taking place in quality system s in L ibya as part
o f a com prehensive and broad ranging reform program m e, aim ed at developing a health
system able to provide high quality health services to the L ibyan people. It also
encom passes an attem pt to specify the role o f leadership and hum an resources in w orking
out the features o f this system .
T he policy on prim ary healthcare is built on the principle o f providing health services for
everyone that has been approved by the G eneral C ongresses. A s for the national strategy
C H A P T E R O N E Introduction
750 centres for prim ary health care w ere available, along w ith 82 hospitals and m edical
centres. T w enty grouped clinics w ere prepare and supplied w ith m odem current m edical
equipm ents to cover defect in m edical and assisting m edical staff, according to
cooperation and integration agreem ents (T he L ibyan health populism com m ittee, 2004 ).
N ow adays, im proving the health services in developed countries is a m ission as reported
w idely in the new s. T his m ission is even m ore difficult to achieve in developing countries
due to the lim ited resources and social econom ic difficulties, this is one o f the m ain
barriers not only in the health services, but also in m any other public sectors. A ccording
to the available literature and based on m y m any visits and prelim inary investigation
about L ibyan healthcare sector in general and T ripoli healthcare sector in particular, it has
been proven that the reality o f governm ent hospitals in L ibya is that: these hospitals are
facing m any problem s opposing their im provem ent, continuity and ability o f com petition.
H ealth care is going through essential changes and the present health care clim ate
changes on a daily basis (R ad, 2005). F o r these reasons, w e should adopt the m odem
styles for confronting and conveying these challenges for L ibyan healthcare organisations
w hich need to im prove their perform ance in term s o f quality care, and reaching excellent
perform ance at all levels operation in each professional field w ithin the organisation, and
1 .2 . A im s a n d o b jectiv es:
T he aim o f this research is to develop an appropriate T Q M fram ew ork for achieving
perform ance excellence in L ibyan healthcare organisations and benchm arking them and
distinguish their com petitive advantage. T he proposed fram ew ork can be used for:
• D eveloping a new system to m easure perform ance, in L ibyan healthcare.
• C ontinuous im provem ent.
• Identifying a culture that strongly focuses on quality perform ance.
• H elping in developing and m odernising service perform ance m easures.
T he aim o f the research w ill be achieved through the follow ing objectives:
• R eview the current healthcare system in L ibya.
• R eview the literature com prehensively to identify and develop appropriate
research m ethod(s) in order to identify w eakness in the current system and help in
developing and justifying the proposed fram ew ork.
' • A ssess the current organisational culture in L ibyan healthcare in order to ensure
that the developed fram ew ork fits into the culture aspect. In other w o rd s,(ld en tig ^
... ' ' ■ ■
\the organisational culture that is required for im plem entation o f T Q M , and
com pare this w ith the situation that currently exists w ithin L ibyan healthcare.
• D evelop a T Q M fram ew ork that is appropriate for L ibyan healthcare, w hich w ill
support the developm ent o f m anagers and em ployees at different levels in the
organisation, and to identify the skills required to successfully im plem ent
changes.
• P rovide an im plem entation procedure.
C H A PT ER O N E Introduction
1 .3 . P r o b lem B a c k g ro u n d :
U ndoubtedly, quality is a dream and goal for everyone w orking w ithin health care
(Jackson, 2001). H ow ever, the reality o f governm ent hospitals in L ibya is that these
hospitals are facing m uch opposition to their im provem ent, continuity and ability o f
com petition. T he m ost im portant problem is the low level o f health service offered to
patients. T his situation created a clim ate o f m istrust betw een patients and these hospitals.
T his led to m any patients seeking m edical attention, how ever, although the governm ent
invested considerable am ounts o f m oney for buildings, tools, equipm ents and m edical
staff w ithin these hospitals and health centres, also, these hospitals have no ability to
com pete w ith m edical organisations abroad w hich, burdens the governm ent w ith m ore
losses. T here are also m any problem s relating m anagem ent, w orkforce and m edical
services beneficiaries.
1 .4 . O v e r v iew o f th e T h e sis:
T he thesis is organised into ten chapters as follow s:
• C hapter one: T his chapter illustrates the introduction about T otal Q uality
M anagem ent, the research aim s and objectives, problem background and the
justification o f using T Q M for confronting the challenges that face L ibyan
C H A P T E R O N E Introduction
• C hapter tw o: In this chapter an overview about L ibyan health care services is
established and data and inform ation about adopted policies, characteristics,
difficulties and quality system in the field o f healthcare are collected. T he
m ain deliverable o f this chapter is to provide a clear understanding o f the
L ibyan healthcare and identify L ibyan healthcare policies and problem s in the
current quality sy stem ..
• C hapter three: In this chapter som e com m on concepts and definitions o f
Q uality and T Q M is introduced. C lear understanding o f total quality
m anagem ent b y highlighting the im portant aspects and perspectives pertained
to im plem enting T Q M in hospitals and health care. In addition, the historic
evolution o f T Q M and its factors are review ed. T he m ain deliverable o f this
chapter is to present and docum ent on the intellectual and philosophical
fram es o f T Q M and perform ance m anagem ent in the public sector.
• C hapter four: T his chapter review o f the literature on quality m anagem ent in
order to clarify quality factors and literature support. S hort presentations o f
the m ost im portant T Q M factors that are generally accepted b y m any
researchers are discussed and presented, w hich are: L e a d ersh ip , T ra in in g a n d
E d u c a tio n , F o cu s o n c u sto m e r, P ro c ess a n d m e a su re m e n t a n d C o n tin u o u s
Im p ro v e m e n t. In addition, the different N ational Q uality A w ard, m odels and
C H A P T E R O N E Introduction
im plem entation process are illustrated. F inally, requirem ents o f total quality
m anagem ent im plem entation are discussed.
• C hapter five: T he m ain intention o f this chapter is to outline the com m on
types o f research available in literature and to discuss the research d esig n an d
m ethodology. T he chapter focuses on m ain m ethodologies that can be used in
business and m anagem ent research. T his chapter discusses also the research
approach and strategy, sam ple size, data collection m ethod, the data analysis,
and tests for validity and reliability process.
• C hapter six: T he m ain intention o f this chapter is to exam ine and discuss the
data collected during the survey. S even leadership factors are chosen from
vast literature review ed these factors w ere used for developing a self-
explanatory survey questionnaire (on a five-point L ikert scale ranging from
strongly agree to strongly disagree) to collect data from m anagers and
em ployees at different m anagem ent levels. T he m ain deliverables o f this
chapter are to identify the strengths and w eakness points o f leadership, w hich
help in creating the organisational culture that is required for im plem entation
o f T Q M . In addition, S tatistical analyses are perform ed using a statistical
package for social sciences (SP S S). M oreover, tests for validity and reliability
C H A P T E R O N E Introduction
• C hapter seven: T his chapter focuses on the identification o f the best practice
o f total quality m anagem ent (T Q M ) factors that allow organisations to seize
perform ance excellence and provide a benchm arking tool for the T Q M
factors. T his chapter considers five T Q M factors nam ely: L e a d e rsh ip ,
T ra in in g a n d E d u c a tio n , F o c u s o n c u sto m e r, P ro c e ss a n d m e a su re m e n t a n d
C o n tin u o u s Im p ro v e m e n t w hich form the basis for the developm ent o f a
m odel to m easure the perform ance excellence o f healthcare organisations.
A nalytical H ierarchy P rocess (A H P ) is used to im plem ent the proposed
perform ance excellence m odel, w hich is validated through questionnaires
w ithin healthcare organisations in the developing countries and in particular
L ibyan H ealthcare O rganisations.
• C hapter eight: the m ain aim o f this chapter is to provide a proposed T Q M
fram ew ork that is appropriate for L ibyan healthcare. In addition, provides an
im plem entation procedure for the proposed T Q M fram ew ork and the skills
required to successfully im plem ent changes. T he m ain deliverable o f this
chapter is a T Q M fram ew ork for achieving perform ance excellence in L ibyan
healthcare organisations and provides an im plem entation procedure.
• C hapter nine: T he m ain aim o f this chapter is to study and discuss the data
collected during the survey. T he survey designed in order to ^verify/validate
.the proposed T Q M fram ew ork and its im plem entation procedure,. A ll answ ers
■ C H A P T E R O N E Introduction
statistical analyses are perform ed using a statistical package for social
sciences (SP S S). M oreover, tests for validity and reliability are carried out.
• C hapter ten: this chapter is the final chapter, the findings, conclusion about
this research is provided, and som e recom m endations are presented. In
C H A P T E R T W O _____ __________________ S tudying and analysing the current status
C h a p te r tw o :
S tu d y in g a n d a n a ly sin g th e c u r re n t sta tu s
2 .1 . In tr o d u c tio n ... ... 1 1
2 .2 . O v er v ie w o f L ib y a n H e a lth c a r e... ... ...1 2
2 .3 . T h e L ib y a n p o lic y in th e field o f p r im a r y h e a lth ca r e... 1 4
2 .3 .1 . T h e p o lic y o f h e a lth ca r e se c to r ... :... ... 1 4
2 .3 .2 . D iffic u lties o f h e a lth c a r e se c to r... ... 1 6
2 .1 . In tro d u ctio n :
-Im proving health is the m ain justification for the existence o f any health system , in other
w ords, the ultim ate goal for any such system . T he quality program m es in the health field
exist, m uch the sam e as in the industrial sector. T he quality here is w hat the patient
receives w ith regard to excellent and safe m edical and health services, w hich is m eeting
custom er requirem ents (F uertes, 1999).
T otal quality is subm itted to the patient b y several various m edical and health
organisations. A ny m istake connected w ith the services or the existence o f any m edical
m istake b y those w ho belong to the m edical field, is som ething that cannot be tolerated if
total quality m anagem ent is to be achieved.
T here is no doubt that the benefits from quality program m es require m ore preparation,
arrangem ent and change w ithin the organisational culture to clarify their aim s, and as a
result m anagers should learn to be patient (B ardoel and S ohal, 1999). H ow ever, it m ay
not be easy for em ployees w ho are w orking in any sector to accept evaluation o f their
perform ance and their progress; this is so because evaluation entails self-criticism and
em ergence o f difficulties and m istakes and thus discussion o f the causes in order to find
the best possible w ays to overcom e. In this chapter an overview about L ibyan health care
services is established and data and inform ation about adopted policies, characteristics,
difficulties and quality system in the field o f healthcare are collected. T he m ain
deliverable o f this chapter is to provide clear understanding o f the L ibyan healthcare and
identify L ibyan healthcare policies and problem s in the current quality system .
2 .2 . O v er v iew o f L ib y a n H ea lth ca re:
L ibya has an estim ated population o f 5.5 m illion inhabitants and is one o f the largest
countries in A frica. It is located in N orth A frica; and covers approxim ately 1,770,000
square kilom etres. H ealth now adays in its scientific concept is p art o f the national
econom y and social developm ent in all its dim ensions. A new life started by the
beginning o f the L ibyan revolution in 1969, w hen people started to fight against diseases,
poverty, and illiteracy. F rom the beginning, the revolution gave consideration to the
health sector. H ealth utilities w ere established and m edicines and free treatm ent m ade
available for all, w hich led to the disappearance o f m any diseases and a better living
standard. W ithin a short period, infant deaths w ere m inim ized and diseases disappeared.
H ealth services expanded to include the disabled and elderly people all these steps w ere
reflected into a plan o f perm anent strategy, that health care is considered as a right
provided b y the com m unity to all citizens w ithout exception, w ith all necessary efforts to
achieve the best rates and dim ensions o f health services in quality treatm ent and
protective. F or this purpose in L ibya m ore than 750 centres for prim ary health care and
82 hospitals and m edical centres w ere available and 20 grouped clinics w ere prepared
and supplied w ith m odem , current m edical equipm ent to cover replace defective
equipm ent and to assist the m edical staff, according to cooperation and integration
agreem ents. A t the sam e tim e, faculties o f m edicine, dentists, and pharm acy w ere
established and health education institutions to graduate qualified national elem ents, to
replace the foreigners. A ll adm inistrative and regulative m eans w here taken to secure a
link betw een health services and other services o f concern, such as catering services,
areas to be provided w ith suitable health services. W ith continuous efforts health services
w ere im proving for the better, day-by-day (T he L ibyan health populism com m ittee,
2004).
P rim ary health care is the first stage for the national health. A s such it is considered as the
first stage o f com m unication betw een the citizen, fam ily and the society. T here is no
doubt that the prim ary healthcare is one o f the m ost im portant cares provided by the
country. In addition, it becom es highly im portant by the nations as peoples are considered
a w ealth bonanza. T he m ain objective for any prim ary healthcare is to m eet the need o f
the individual, and im prove the perform ance o f the system . T he prim ary health care is
now the standard to m easure the range or extent o f the success pertinent to the health
system s.
P rim ary and social healthcare adm inistration is one o f the m ost im portant adm inistrations
w ithin L ibyan health sector. A nd as a technical, controlling supervisory and specialist
adm inistration, it is assigned to laying out plans and program s, the nation al strategic goal
regarding the prim ary healthcare w hich is the landm ark for the health for all system in
L ibya and is approved under the general people's C om m ittee num ber (24) for 1424 on the
national strategy to provide healthcare for all people. T he prim ary healthcare includes the
follow ing:
-1) M otherhood and childhood section
2) H ealth inform ation and culture section.
3) E ndem ic diseases and vaccination section.
4) S chool health section. .
5) E nvironm ental, professional health section
6) S upervision and inspection section.
7) S tatistics, docum entation and studies section. (T he L ibyan health populism
com m ittee, 2004).
2 .3 . T h e L ib y a n p o lic y in th e field o f p r im a r y h ea lth ca re:
O n 25/01/2006 the researcher held an interview w ith the H ealthcare D irector in T ripoli
and highlighted the policy and difficulties in T ripoli prim ary healthcare.
T he follow ing sections provide a sum m ary o f the interview :
2 .3 .1 . T h e p o lic y o f h e a lth c a re secto r:
T he policy o f prim ary healthcare is built on the principle o f providing health for
everybody, w hich has been approved b y general congresses. A s for the national strategy
for prim ary health care, it constitutes the basis for the health system in L ibya, and has
been approved under resolution o f the general people's com m ittee num ber (24) 1424. T he
strategy has included the follow ing:
-1) T he health system in L ibya is considered as being based o n prim ary
healthcare.
2) T he strategy consist o f follow ing p rin cip
les:-- R esponsibility o f the society is to ensure basic health care for all.
- Justice in the distribution o f health resources.
- C onsideration o f healthcare as an investm ent process and representation o f
that process as part econom ic, social and environm ental developm ent.
- R esponsibility o f all health sectors to provide health service.
- U se o f suitable technology.
C H A P TE R T W O _______ ____________S tudying and analysing the current status
- L inking o f the citizen w ith the doctor in the prim ary care unit according to a
fam ily record system and a com m itm ent system to enable access to preventive
treatm ent and qualification services.
3) H ealth care services include the follow ing elem ents:
-G lobal elem ents:
- H ealth inform ation and culture.
- H ealth food and nutrition.
- S afe seated w ater and environm ental safety
and cleanliness.
- B aby and m other care.
- V accination.
- E ndem ic diseases avoidance.
- F irst aid.
- P rovision o f basic m edicines.
L ocal elem ents: - • '
S chool health.
- P sychology health.
- P rofessional (w ork - related) health.
- S ocial health and health related to senior citizens.
4) T he prim ary healthcare are consist o f three levels:
-- F irst level: w here prim ary healthcare services are provided.
S econd level: W here m ore com plicated problem s transferred from first level,
- T hird level: B y w hich coordination o f all parts o f the health system takes
place and w hich provides expertise, assessm ent and developm ent.
5) S trategy im plem entation: depends on the follow ing:
-- D evelopm ent o f health adm inistration, training o f its cadre, im provem ent o f
health inform ation system and m edical docum entation.
- F ocus on national w orkforce.
- M odernisation and m aintenance o f health facilities and taking care o f their
equipm ent and revolution o f the w hole process.
- Im provem ent o f supply channels.
- C ooperation w ith international, regional and A rab organisations.
- D evelopm ent o f financial resources.
T reatm ent facilities, private clinics and w hat com es under their field are considered as
channels providing m edical services for the strategy im plem entation.
C H A PT ER T W O ________________________ S tudying and analysing the current status
2 .3 .2 . D iffic u lties o f h e a lth ca r e secto r:
H ow ever, som e difficulties m ay occur w hich could .lead to reduce standards in service,
such as:
-- D efect to secure m edical needs w ere increase by inhabitant's grow th, and increase
o f foreigners in L ibya.
- P erm anent strategy (free o f cost) m edication .
- U nfair and unjust blockade im posed on L ibya and econom ic changes w hich m ay
- T he huge num ber o f functions not exposed to perm anent dim ension not m atching
services provided w hich constitute a burden on the balance.
- T he existing regulation and organisational structure, w hich w ere not able to m atch
these changes.
- A bsence o f training plans and qualification to m atch the fast developm ent in
diagnosis and m edication.
2 .4 . S u m m a ry :
In this chapter an overview about L ibyan health care services established and data and
inform ation about adopted policies, characteristics, difficulties and quality system in the
field o f healthcare are collected. In the next tw o chapters a com prehensive literature
review related to T otal Q uality M anagem ent (T Q M ) w ill be carried out to have a clear
insight into the T Q M and its application in health sendee. In addition, the historic
C H A P T E R T H R E E _________________ U nderstanding T otal Q uality M anagem ent
C h a p te r th ree:
U n d e rsta n d in g T o ta l Q u a lity M a n a g e m e n t
3 .1 . In tro d u c tio n ... ... 1 9
3 .2 . T h e c o n c e p ts a n d d e fin itio n s o f Q u a lity a n d T Q M ... ..1 9
3 .3 . T Q M in H o sp ita ls a n d H e a lth c a r e... ... 2 4
3 .4 . C o m p a r iso n b e tw e e n th e tra d itio n a l a n d m o d e rn q u a lity c o n c e p ts... 2 7
3 .5 . T h e im p o r ta n c e o f T Q M .... ... *... ...2 8
3 .6 . E v o lu tio n o f T Q M ... 2 9
3 .7 . Q u a lity G u ru s? ... 3 1
3 .7 .1 . E d w a r d D e m in g ... 3 1
3 .7 .1 .1 . T h e D e m in g W h e e l (P D C A )...3 3
3 .7 .2 . J u r a n J o se p h ... 3 4
3 .7 .3 . P h ilip C r o sb y ... 3 5
3 .7 .4 . K a o ru Ish ik a w a ... 3 5
3 .1 . In tr o d u c tio n :
T otal Q uality M anagem ent (T Q M ) is not a new approach in developed countries. T here is
how ever, som e experience o f its practices in several developing countries.
T he quality program m es have to be designed in a w ay to satisfy the custom ers’
requirem ents and according to possibilities available. T herefore, the T Q M program m es
should start to evaluate the case and to try to increase qualifications and abilities in a
clear, frank and easy m ethod to im plem ent. Q uality is not here only to solve our
problem s, but to clarify those problem s to find the incentive behind them and to
cooperate in the best w ay possible to find solutions for those problem s or im prove the
services (S hort & R ahim , 1995). In this chapter som e com m on concepts and definitions
o f Q uality and T Q M is introduced. C lear understanding o f total quality m anagem ent b y
highlighting the im portant aspects and perspectives pertained to im plem enting T Q M in
hospitals and health care. In addition, the historic evolution o f T Q M and its factors are
review ed. T he m ain deliverable o f this chapter is to present and docum ent on the
intellectual and philosophical fram es o f T Q M and perform ance m anagem ent in the public
sector.
3 .2 . T h e c o n c e p ts a n d d e fin itio n s o f Q u a lity a n d T Q M :
F irst o f all, before deciding to im plem ent changes in business, w e need to define quality.
If the custom er w ants quality, w hat does that m ean? T he answ er is not sim ple. Q uality
can be defined as the custom er’s expectations and requirem ents; quality contains
anything the custom er expects and requires, and is ever changing (H radesky, 1995).
indicated that quality is built into an organisation by being com petitive, rem oving
consternation, m anaging costs and b y caring. T hese four reasons illustrate w hy quality is
very im portant and w hy now is the tim e for m aking quality happen. H e indicated that
consternation is caused by increasingly large num bers o f em ployees spending m ore and
m ore o f their tim e doing w ork over again, because it w as not done from the first tim e.
O rganisations m ust care not only about its custom ers, but also about th e com m unity,
those living around it, their environm ent, and its com petitive position.
A ccording to E vans (2008) custom ers today are clever enough to know quality issues that
firm s face today and the organisation that doesn't listen to its custom ers is in for a
im polite developm ent, or, at w orst, a quick failure. T his is w hy an understanding o f
quality is still very im portant to every m em ber o f staff in every organisation. H e added
that Joseph Juran, one o f the quality gurus in the 1900s, indicated that historians w ould
define the tw entieth century as the century o f productivity and the tw enty-first century
should be designated the century o f quality.
T otal quality m anagem ent (T Q M ) has a long life. T he Japanese m oved in the direction o f
quality after the S econd W orld W ar and the U nited S tates in the m id-1980s w ith the
form ation o f the B aldrige A w ard in 1987. T he m ovem ent then expanded into to E urope
w ith the establishm ent o f the first E uropean F oundation for Q uality M anagem ent and the
E uropean Q uality A w ard in 1988 and 1989 respectively. S o T Q M has been around a long
tim e (W illiam s et al, 2004).
T rials o f defining T Q M led to several discussions and a large extent o f m isunderstanding
as w ell as a huge extent o f definitions. T here are several attem pts to define the T Q M ,
phenom enon that appears to have evolved over a period o f tim e (H aigh and M orris,
2001). S o there have been several definitions and each deals w ith certain aspects. Journal
o f O rganisation C hange o f M anagem ent contacted E dw ard D em ing before he died in
1993, it called on him to present the concept o f T Q M as being the producers o f this
concept, but he replied that he didn’t know w hat this concept m eant. D em ing pointed out
that this concept involved a lot o f m eaning for the researchers; that for each researcher in
this field his/her ow n term related w ith this concept, even if they are based on the
beneficiary ’s satisfaction (H egan, 1994). Q uality m anagem ent is a revolution because the
philosophy and test m ethods and tools to discover better w ays o f doing things, it could be
help public sector organisations to fulfil their responsibilities effectively and at a reduced
cost to the governm ent and taxpayers, also in the sam e a tim e im proving services
(O ’R ourke et al, 2001). R egardless o f the differences m ade b y such attem pts, there are
som e definitions that have appeared and found a place w ithin the adm inistrative m ind.
T he follow ing are am ong such definitions:
-T otal quality m anagem ent (-T Q M ) is a system o f activities directed at achieving satisfied
custom ers, em pow ered em ployees, higher profits, and low er cost (Juran and G ryna,
1993). T Q M is an approach involving m any processes that guarantee that this quality
subject m atter w ill im prove its effectiveness and com petitiveness, and ability to adapt to
new conditions (K och, 1993). A lso, S aunders and P reston (1994) illustrated that T Q M is
a system for m anagem ent, w hich focuses on im provem ent in the quality o f goods and
services provided to custom ers as the key to business success. Z airi (1994) introduced
som e definition o f T Q M w hich is; T Q M is essentially com plete set o f techniques, and
the benefit o f the end custom er. T Q M seeks to develop organisations through the creation
o f better planning and prioritise better design. It also aim ed at strengthening operations
and w eak S trong protection areas that give organisations edge over their com petitors
(through continuous im provem ent the com parison). In addition, it is about total quality
m anagem ent continuous process o f providing the best practices to ensure sustainability,
and positive com petitiveness. In a sense, it is about the m anagem ent o f change; it is then
lim itless and tim eless in its approach. L ikew ise, A rm strom g (1995) introduced T Q M as a
key business im provem ent strategy and the key m anagem ent m atter o f the future because
it is crucial for activity and com petitiveness. D ahlgaard et al (1998) used the definition o f
T Q M b y K anji w ho defined T Q M as the w ay o f life o f an organisation com m itted to
custom er satisfaction through continuous im provem ent. A lso, it w as defined b y O akland
(2000), as an entry o f activity im provem ent and w ork flexibility as a w hole and total
quality m anagem ent need a culture change and involving everyone at each level in an
organisation. P rajogo et al (2005) indicated that T Q M is a m anagem ent m odel, w hich
aim s to m eet custom er needs and expectations w ith an organisation through continuous
im provem ent o f quality o f goods and services and by m erging all functions and processes
inside an organisation. In addition, D em ing put the responsibility for the continuous
im provem ent o f products and services that m eet the needs o f custom ers and survive the
com petition directly to the D epartm ent (T um m ala et al, 1995). F uentes (1999) defined
T Q M as a system atic and participation approach to planning and im plem enting-a process
o f continual im provem ent in the organisation w hich focused on the satisfaction o f
custom ers’ expectations, identification o f problem s, and prom oting open decision m aking
im prove quality and decrease costs (O vretveit, 2000 ). M oreover, W illiam s et al (2004)
defined T Q M as a m anagem ent approach to ensure m utual cooperation am ong everyone
in the organisation and business processes related to the production o f products and
services that m eet needs and expectations o f custom ers. In addition, T oufeak (2004)
indicated that T Q M is a co-operative form or m odel to perform business, depending on
skills and capabilities o f personnel and m anagem ent staff for the aim o f continuity o f
quality and productivity im provem ent via em ploym ent o f w ork team s. T his definition
includes the three com ponents necessary for (T Q M ) success in any organisation:
M an agem ent by P articipation, C ontinuants Im provem ent and T eam w ork. O n the other
hand, there is another w ay to look at T Q M , w hich is to analyse the three w ords: total,
quality and m anagem ent. A ccording to K anji and L iu (2003), total m eans m ade up o f the
w hole, quality is a degree o f excellence a product or service provides, and m anagem ent
m eans act, art o f planning, organising, leading and controlling. L ikew ise, H aigh and
M orris, (2001) indicated that total m eans organisation w ide process involving everyone
from the m ailroom to the boardroom , quality m eans establishing quality goals for each
and every elem ent in the process o f product or service delivery, so as to m eet the needs o f
custom ers and their expectations from the outset and m anagem ent does not only m ean the
com m itm ent o f senior m anagem ent to the goals, but the quality o f senior m anagem ent in
the active pursuit o f them . In addition, R ad (2005) explained that T Q M aim ed to m eet
the needs o f custom ers to prevent poor quality, instead o f correcting problem s after they
happen. A lso put the continuous im provem ent understanding o f the im portance o f
perform ance m easurem ent to identify opportunities for im provem ent and elim inate
sources o f inefficiency and costs.
3 .3 . T Q M in H o sp ita ls a n d H e a lth c a r e :
H ealthcare is the fastest grow ing service in developed and developing countries alike.
W ith the rapid developm ent o f science and technology and globalisation, there are
increased requirem ents for high-technology m edical care. A ll countries should strive to
address the grow ing need for health facilities in term s o f hum an and m aterial resources
(D ey, 2006). H ospitals are being required to focus not only on good m edical cafe and the
technical facet o f the service, but on the functional facet o f care too, such as
com m unication betw een patients and staff. T his illustrates the im portance o f introducing
T Q M for the developm ent o f these hospitals until they find acceptance b y custom ers
(T om es and N g, 1995). In healthcare, there is also lack o f uniform definition o f quality
due to the m ixture o f professional groups and the inherent characteristics o f health
services. M oreover, understanding the expectations o f the custom er is not an easy task.
T he custom ers often do not really know w hat they w ant, or do not tell you directly w hat
they w ant (L im , 2000). D ey (2006) indicated that organisations require quality culture
that defines the issues and problem s in the dynam ic system , to propose solutions to these
issues and develop a fram ew ork to im plem ent these solutions. M oreover, S hort and
R ahim (1995) indicated that hospital adm inistrators should evaluate and m ake the
necessary adjustm ents to the structure and philosophy, politics and the adm inistration,
before introducing T Q M . E ven in ideal cases, a successful T Q M requires full
com m itm ent, and a lot o f tim e and energy. In the health sector, the recognition o f quality
m eans continuous im provem ent, im proved results, and providing better care for patients,
w ith the possibility to change the health o f all m edical, nursing and adm inistration staff
organisations should take im m ediate steps to ensure that they provide better care at low er
absolute costs. A lso, O 'R ourke et al (2001) illustrated that a quality fram ew ork in the
healthcare setting has been defined as one w hich gives the patient's full satisfaction, the
ability to im prove health care and acceptance o f patients and the com m unity. It w ill also
need to m eet consum er needs and expectations, develop the potential o f the resources
used in the process and the best level o f achievem ent. In short, K och (1993) sum m arised
T Q M in healthcare in the follow ing:
- P utting the patient first.
- B eing fully aw are o f patients’ expectations and needs.
- S atisfying patients and satisfying them first tim e.
- R ecognising the cost o f poor qu ality.
- S upporting and encouraging every m em ber o f staff in every healthcare
organisation.
- S upporting and encouraging staff to reach higher quality and cost effective
healthcare services.
- E ncouraging professionalism and expertise betw een all staff.
T herefore, the total quality m anagem ent has characteristics and m erits that m ake it higher
than the traditional quality m anagem ent, that it includes every individual and aim s to
serve the consum ers. G enerally, there are several points that can be form ed on total
quality m anagem ent:
1. Q uality can m ean different things to different people. T his leads to
different definitions (D ahlgaard et al, 1998).
2. T otal quality m anagem ent is a trip, not an arrival station; it is a
continuous, perm anent im provem ent.
3. T he goal o f total quality m anagem ent is to satisfy the custom er needs and
expectations.
4. T otal quality m anagem ent needs tim e to achieve its results. T he T Q M
literature suggests that success com es to organisations, w hich are ready for
a change in clim ate. T herefore, organisations should take tim e to diagnose
and identify w ays o f rem oving barriers o f T Q M (W eeks et al, 1995).
5. T Q M is not a fast m anagem ent fix; it is about changing the w ay things are
done w ithin the organisation’s lifetim e (K anji and A sher, 1996).
6. T Q M insures that m anagem ent adopts a strategic overview o f quality and
focuses on prevention, not discovery, o f problem s (O akland, 1998).
7 . C ontinuous im provem ent is everyone’s responsibility. •
In. short, according to Z airi (1994) the challenge for all o f us is possibly to create T Q M
w ork m ore effectively in any sector, to m ake sure that organisations optim ise its benefits,
to develop it as a philosophy o f new m anagem ent so that it can address future challenges,
to dissem inate ideas on a large scale, definitions, exam ples o f T Q M and its w orkings and
their integration into the education system s.
3.4. C o m p ariso n betw een th e trad itio n al an d m o d ern q u ality concepts:
In order that w e can com pare betw een the traditional and m odem view connected w ith
the quality, and the follow ing table (3.1) show s the com parison betw een the traditional
and m odem quality concept.
C H A P T E R T H R E E ____________ _________ U nderstanding T otal Q uality M anagem ent
T able (3.1) C om parison betw een the traditional and m odem quality concept (H aigh and
M orris, 2001 and S harara, 2000 ).
[ C o m p ariso n field ' ; .. [O ptim um quality lev el;.'.. .
T rad itio n al concept O ptim um quality level exists, so that the
custom ers do not pay for im provem ent o f quality after such optim um level.
/ M o d ern co n cep t . f ; N o t optim um level but . ; j
; im proving the quality is a' . \ s i continuousprocess. . ,,. i
i •' *
j K ey goals'for quality-,. • C onform ity for d